
Abstract
Background
Coronavirus disease 2019 (COVID-19) has become a global pandemic, affecting millions of people. However, clinical research on its neurological manifestations is thus far limited. In this study, we aimed to systematically collect and investigate the clinical manifestations and evidence of neurological involvement in COVID-19.
Methods
Three medical (Medline, Embase, and Scopus) and two preprints (BioRxiv and MedRxiv) databases were systematically searched for all published articles on neurological involvement in COVID-19 since the outbreak. All included studies were systematically reviewed, and selected clinical data were collected for meta-analysis via random-effects.
Results
A total of 41 articles were eligible and included in this review, showing a wide spectrum of neurological manifestations in COVID-19. The meta-analysis for unspecific neurological symptoms revealed that the most common manifestations were fatigue (33.2% [23.1–43.3]), anorexia (30.0% [23.2–36.9]), dyspnea/shortness of breath (26.9% [19.2–34.6]), and malaise (26.7% [13.3–40.1]). The common specific neurological symptoms included olfactory (35.7–85.6%) and gustatory (33.3–88.8%) disorders, especially in mild cases. Guillain–Barré syndrome and acute inflammation of the brain, spinal cord, and meninges were repeatedly reported after COVID-19. Laboratory, electrophysiological, radiological, and pathological evidence supported neurologic involvement of COVID-19.
Conclusions
Neurological manifestations are various and prevalent in COVID-19. Emerging clinical evidence suggests neurological involvement is an important aspect of the disease. The underlying mechanisms can include both direct invasion and maladaptive inflammatory responses. More studies should be conducted to explore the role of neurological manifestations in COVID-19 progression and to verify their underlying mechanisms.
Similar content being viewed by others


Introduction
In December 2019, numerous patients had been diagnosed with unexplained pneumonia in Wuhan, China, which quickly spread to the other regions of the world. The disease, which was named as coronavirus disease 2019 (COVID-19) by the World Health Organization (WHO), has now been confirmed to have originated from a severe acute respiratory syndrome (SARS)-like coronavirus (SARS-CoV-2). By May 3rd, 2020, the pandemic had affected more than 200 countries, with 3,349,786 cases having been confirmed as COVID-19, including 238,628 deaths (data from COVID-19 Situation Report-104 by the WHO). The disease in most patients is characterized by mild to medium fever, dry cough, chest distress or dyspnea, with interstitial pneumonia features on chest computed tomography (CT) scan [1, 2]. The main routes of transmission are respiratory droplets and close contact transmission. The average of the reproductive number of COVID-19 is 3.28, based on a summary of 12 related studies, which is much higher than SARS and Middle East respiratory syndrome (MERS) [3].
As knowledge of the SARS-CoV-2 virus has accumulated, most researchers have agreed that COVID-19 is not just a respiratory disease and that it could affect other systems in human. There have recently been increasing studies on the neurological involvement of COVID-19, which could be associated with more severe symptoms and higher mortality. However, there has been no comprehensive review regarding on this topic until now. Here in this systematic review with meta-analysis, we collected and analyzed the clinical manifestations and evidence of neurological involvement in this disease.
Methods
Search strategy and study selection
This study was approved by the Ethics Committee of the Tongji Medical College, Huazhong University of Science and Technology, and the written consent was exempted because it was a secondary analysis of the published studies. In this systematic review and meta-analysis, we searched the English literature that demonstrated clinical manifestations and that provided evidence of neurological manifestations in COVID-19, according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (PRISMA Checklist in Supplement materials). Given the novelty of the field, the search was conducted up to May 3rd, 2020, in two preprint databases (bioRxiv and medRxiv) and three popular medical databases (PubMed, Embase and Scopus). A combination of keywords related to COVID-19, neurological manifestations, neurological diseases and specific symptoms were used with Boolean operators for more efficient literature retrieval (search strategy in Supplement materials).
Eligibility criteria
The studies on clinical manifestations and evidence regarding neurological manifestations after COVID-19 were collected using Endnote X9 software (Clarivate Analytics), and the duplicates were removed accordingly. Case reports, case series, correspondence with relevant clinical data, and retrospective and cross-sectional studies were included for further analysis and review. The exclusion criteria included (1) clinical observation with no related neurological symptoms and a lack of related data; (2) the studies focused on a specific population (e.g., infants, children, patients with cancer, pregnant women); (3) repeated research on the same cohort of patients; and (4) other types of study (e.g., reviews, book chapters). All selected publications were comprehensively reviewed by two independent investigators to ensure their eligibility for inclusion in the review. If any disagreement occurred about eligibility of the literature, it was resolved by consensus after thoroughly discussing the publication with a third investigator.
Inclusion criteria, data extraction and quality evaluation for meta-analysis
Given that the articles reporting specific neurological symptoms (e.g., dysgeusia, agnosia) were limited, only articles that reported unspecific neurological symptoms (e.g., headache, weakness, respiratory failure) in patients with COVID-19 were selected for further meta-analysis. The quality assessment tool for case series studies designed by the National Institutes of Health (NIH) was applied to evaluate the included studies in the meta-analysis. For each item, we scored 1 point for “yes” and 0 points for “no,” “not available,” “not reported,” and “cannot determine.” The total score from all nine criteria (0–9) was generated accordingly to gauge the overall quality of the study.
Statistical analysis
Stata (version 15.1) was used to perform a meta-analysis of single arm studies. The combined prevalence and 95% confidence interval were calculated using the random-effects model. Egger’s test was performed to assess publication bias in all literature, and P < 0.05 was considered statistically significant. Subgroup analysis was done to discuss the heterogeneity of the meta-analysis.
Results
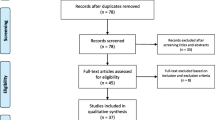
After a primary search, a total of 440 publications were retrieved, including 73 from Pubmed, 133 from Embase, 163 from Scopus, and 71 from medRxiv and bioRxiv. Among these, 142 were duplicates and were removed accordingly. We evaluated the eligibility of the remaining 298 papers according to title, abstract, article type, and full-texts (Fig. 1). The 11 papers from other resource (e.g., references list of existing papers) were added. Ultimately, 41 studies were included for systematic review and meta-analysis, including 20 studies on unspecific neurological manifestations [1, 2, 4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21], 20 studies on the specific neurological symptoms [22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41], and 1 reporting both types of symptoms [42].

Study selection and characteristics
Unspecific neurological symptoms associated with COVID-19 and meta-analysis
From a clinical aspect and the reported symptoms, headache, myalgia, fatigue, nausea, vomiting, confusion, anorexia, dizziness, malaise, dyspnea/shortness of breath were regarded as unspecific symptoms and were included in the subsequent meta-analysis.
Twenty-one eligible papers that reported unspecific neurological symptoms are summarized in Table 1, among which 19 (90.5%) were retrospective case series with one retrospective cohort (4.8%) and 1 prospective case series (4.8%). Nineteen studies (90.5%) enrolled patients from China, with the other two from Korea and India, respectively. There were 7 (33.3%) multicenter studies and 12 (57.1%) reports from a single institute. The number of enrolled patients ranged from 13 to 1099, and the sex ratio varied from 0.69 to 3.33 (male/female). The quality assessment for the literature is detailed in Supplement Table S1.
We then meta-analyzed the prevalence of the nine unspecific neurologic COVID-19 manifestations in 3837 patients. For the common neurological manifestations (the number of the studies > 10 and total cases > 1500), fatigue (33.2% [23.1–43.3]) and dyspnea/shortness of breath (26.9% [19.2–34.6]) were the most prevalent symptoms, followed by myalgia (16.0% [12.3–19.8]), headache (9.2% [7.2–11.2]), and nausea/vomiting (5.1% [3.3–6.8]). Among the neurological manifestations that were reported sporadically (the number of the studies < 10 and total cases < 1500), the most common symptoms were anorexia (30.0% [23.2–36.9]), malaise (26.7% [13.3–40.1]), dizziness (10.0% [5.9–14.2]), and confusion (5.2% [− 1.7 to 12.2]), in descending order (Fig. 2). Significant publication bias was not observed in the common neurological manifestations including headache, myalgia, fatigue, nausea/vomiting, and dyspnea/shortness of breath (Fig. 2, all p > 0.05 by Egger’s test).

Meta-analysis of the prevalence of unspecific neurologic manifestations in COVID-19
Substantial heterogeneity was observed in most symptoms within subgroups (Fig. 2 and Supplement Tables S2–5). In the subgroup analysis, dyspnea/shortness of breath was more prevalent in the studies performed in Wuhan, on elder patients (median or mean age > 47 years), with higher M/F ratio (M/F ratio > 1.38), and higher percentage of severe cases (> 15%) (p < 0.05). In addition, fatigue was more frequent in the severe cases and studies in Wuhan (p < 0.05), and younger patients tended to experience more headaches. No other potential sources of heterogeneity of these five unspecific neurological manifestations were identified.
Specific neurological symptoms associated with COVID-19
We retrieved 21 studies regarding the specific neurological symptoms and diseases after COVID-19 (summarized in Table 2), among which 6 (28.6%) studies were case series and the rest (71.4%) were cases reports. In the six cases series, two studies focused on a relatively wide spectrum of neurological manifestations (e.g., central nervous system [CNS], peripheral nervous system [PNS], neuromuscular disorders) [36, 42], with the other four focused on olfactory and gustatory dysfunction [23, 24, 29, 37]. In the 15 case reports, 5 were associated with Guillain–Barré syndrome [31,32,33,34,35], 5 focused on neurological inflammation (e.g., myelitis, encephalitis, meningitis) [22, 26, 28, 30, 39, 41], 2 on cerebrovascular diseases [27, 38], and the rest on specific neurological symptoms [25, 40].
Laboratory, electrophysiological, radiological, and pathological evidence of neurological manifestations after COVID-19
Eleven papers that demonstrated laboratory, electrophysiological, radiological, and pathological changes after COVID-19 were distilled from the summarized literature, including seven on the examination of cerebrospinal fluid [30, 32, 34,35,36, 39, 41], three on electroencephalogram [36, 39, 41], two on nerve conduction [32, 34], six on magnetic resonance imaging (MRI) scans [26, 27, 30, 32, 36, 40], two on CT images [27, 40], and one post-mortem examination [25] (summarized in Table 3).
Discussion
To our knowledge, this is the first systematic review with meta-analysis of more than 41 studies involving approximately 4700 patients that provides a comprehensive view of neurological manifestations in COVID-19. In comparison with previous review and proposal on the topic, both clinical manifestations and related evidence were demonstrated to investigate multifaceted mechanisms underlying neurological involvement in COVID-19.
After the primary exploration, the neurological manifestations in COVID-19 were found to mainly fall into three categories: (1) neurological diseases comorbid with COVID-19, in which neurological symptoms occur prior to the infection that also make patients themselves susceptible to COVID-19 due to frequent exposure in medical facilities and suboptimal health status (e.g., cerebrovascular diseases, neural trauma); (2) unspecific neurological manifestations, which can be caused by systematic responses and partially by the neuroinvasive behavior of the infection (e.g., headache, myalgia, fatigue); (3) specific neurological symptoms and diseases that were due to neurological involvement in COVID-19 (e.g., encephalitis, myelitis, seizures). This review mainly focused on the last two categories of COVID-19 neurological manifestations.
Unspecific neurological manifestations in COVID-19
Unspecific neurological manifestations are various and insidious in COVID-19. It has been reported that unspecific neurological manifestations occurred in the early onset of the infection and could serve as the primary and only symptom when COVID-19 patients were admitted to the hospital [32]. Neurologic manifestations were also more prevalent in the patients with severe disease, which increased the risk of transmission and could lead to death if not handled properly and effectively [42]. However, there is a wide symptomatic spectrum of neurological manifestations in COVID-19, and it is easy to misdiagnose them during the epidemic due to the respiratory nature of the virus. After a systematic exploration of the literature, we found that the headache, myalgia, fatigue, nausea/vomiting, confusion, anorexia, dizziness, malaise, and dyspnea/shortness of breath were reported as unspecific neurological symptoms. Among them, the dominant clinical manifestations were fatigue, dyspnea/shortness of breath, anorexia, and malaise, which affected approximately one-third of patients with COVID-19.
Whether dyspnea/shortness of breath is a neurological symptom is still a matter of debate. Recently, several patients with dyspnea in an intense care unit (ICU) subjectively described that active and conscious breath was needed to maintain a normal breathing rhythm [43]. As we know, angiotensin-converting enzyme 2 (ACE2), an important SARS-CoV-2 receptor, is found to be expressed in the cardiorespiratory center of the medulla together with other brain regions [44, 45]. Given the high similarity among coronaviruses and the fact that other coronaviruses (e.g., SARS-CoV, MERS-CoV) could invade the nervous system [46], it is reasonable to speculate that SARS-CoV-2 virus might play a role in the dyspnea/shortness of breath via affecting the respiratory center of the medulla, especially in those patients with rapid disease progression but without severe respiratory symptoms. Thus, dyspnea/shortness of breath was included as one of the neurological manifestations in this review, and we observed that it was one of most prevalent neurological symptoms in COVID-19 infection. However, further clinical and experimental studies should be performed to differentiate the exact cause of dyspnea and to explore its potential association with neurological involvement.
Specific neurological manifestations and diseases associated with COVID-19
In this review, we found six case series focused on the specific neurological manifestations, including CNS-related symptoms (e.g., impaired consciousness, acute cerebrovascular disease, corticospinal tract signs, ataxia, and seizure), PNS-related symptoms (e.g., taste impairment, smell impairment, vision impairment, and nerve pain), and musculoskeletal injury [23, 24, 29, 36, 37, 42]. Interestingly, olfactory dysfunction and gustatory disorders were observed 30–80% in patients with mild COVID-19. Recently, Fodoulian et al. and Brann et al. had reported that ACE2 and SARS-CoV-2 entry genes were expressed by sustentacular cells in the human olfactory neuroepithelium [47, 48]. In addition, bilateral inflammatory response in the olfactory clefts was observed in a patient with COVID-19 with sudden olfactory loss but without nasal obstruction by MRI and CT scans, which suggests the virus might affect olfactory function via direct invasion of the olfactory neuroepithelium [40]. However, we lack definitive evidence regarding the potential association between the PNS symptoms and the risk of CNS infection.
Regarding the neurological diseases, we found that aseptic neuroinflammation appeared to be related to COVID-19, including Guillain–Barré syndrome, Miller Fisher syndrome, myelitis, meningitis, and encephalitis [22, 30, 32, 34, 35, 39]. Notably the polymerase chain reaction (PCR) tests of cerebrospinal fluid (CSF) were negative in all cases. The mechanism for the neuroinflammation in the patients with COVID-19 is unclear. However, in a recent report on a rare condition (hemorrhagic necrotizing encephalopathy) in COVID-19, the author inferred that the breakdown of the blood–brain barrier (BBB) by cytokine storm could be the primary cause of disseminated brain necrosis and hemorrhage in this case [27]. Together with the increase in protein levels and immunoglobulin in CSF, we suspect that both the cytokine storm secondary to the systematic infection and the overactivation of the immune system might play a role in this process.
Evidence for neurological involvement of COVID-19
Currently, our knowledge regarding on neurological involvement of COVID-19 is still limited. The definitive evidence for the invasive behavior of COVID-19 in CNS is mainly from two neuropathological reports. Paniz-Mondolfi et al. had reported the presence of SARS-CoV-2 in brain tissue from post-mortem examination of a COVID-19 patient by employing a transmission electron microscope. Viral particles of approximately 80–110 nm, which were pleomorphic and spherical with distinct stalk-like projections and perfectly matched the structural features of SARS-CoV-2, were spotted in the frontal lobe section of the brain [25]. Notably, these viral particles were found to be located not only in the cytoplasmic vacuoles of neuronal cells but also in the small vesicles of endothelium cells, which suggested this direct neuroinvasive behavior via hematogenous pathways might be a leading cause for rapid progression of neurological symptoms [25]. In consistence with this finding, SARS-CoV-2 was also detected in CSF via PCR examinations in a male patient suffering from consciousness disturbance and transient generalized seizures, with typical meningitis and encephalitis characteristics shown on the MRI [30]. Interestingly, this case presented negative PCR result in nasopharyngeal swab at the time point, which indicated that CNS invasion might happen in the early phase of COVID-19 [30]. However, several similar studies had reported negative findings in the CSF examination, which suggests that direct neuroinvasion of SARS-CoV-2 is not a universal phenomenon for COVID-19 [32, 34]. But the interpretation of these negative results should be cautious due to the limitation of PCR examinations, which is currently the most prevalent test for viral detection. Its low sensitivity in CSF specimen may lead to repeated negative findings. Thus, more investigations are needed to further confirm this direct invasive behavior.
The adjuvant evidence for neurological involvement in COVID-19 includes CSF examination, electrophysiology, and radiological findings. The characteristic change in CSF after COVID-19 is the slight increase in cell counts and protein levels, especially immunoglobulins, which suggests its inflammatory or infective status [30, 32, 34,35,36, 39]. For electrophysiology, two cases presented unspecific alterations, another patient exhibited focal seizure in electroencephalogram [36, 39], and the rest showed delayed nerve conduction, attenuation of action potential amplitude, and absent F-Waves, which are associated with the damage to myelin and axons in Guillain–Barré Syndrome [32, 34]. In the radiological examination, MRI and CT scans had been commonly adopted to search for clues for neurological disorders after COVID-19, such as inflammation and cerebrovascular dysfunction, which suggest the direct invasion of SARS-CoV-2. In the patients diagnosed with encephalitis, myelitis, meningitis, and Guillain–Barré Syndrome, enhancement of lesion sites in meninges, brain, spinal cord, and nerve roots was detectable in MRI and correlated with individual clinical manifestations [30, 32, 36]. Poyiadji et al. reported a unique case of acute hemorrhagic necrotizing encephalopathy associated with COVID-19 and the patient presented bilaterally hemorrhagic lesions within multiple brain regions, which implied that the breakdown of the BBB might serve as an explanation of COVID-19-associated cerebrovascular diseases [27]. In addition, perfusion abnormalities appeared to be prevalent (100%) in the patients with COVID-19 with severe neurological symptoms and were not only found in the patients with cerebrovascular disorders [36].
Potential mechanism underlying the neurological manifestation in COVID-19
From the limited studies on the neurological involvement of COVID-19, SARS-CoV-2 could impair the nervous system via two potential pathways: (1) direct invasion of neural tissue and (2) maladaptive inflammatory responses (Fig. 3).

The potential mechanism underlying the neurological manifestation in COVID-19. Based on the current evidence, there are two routes for the neurological involvement of COVID-19. (1) SARS-CoV-2 could direct infect nervous system via hematogenous and neural retrograde pathways; (2) SARS-CoV-2 overactivates the immune system, and secondary cytokines storm and immunoglobins impair the nervous system
In terms of direct invasion, SARS-CoV-2 could affect the CNS mainly through the hematogenous and the neuronal retrograde routes. First, ACE2 was found to be enriched in the endothelium cells of the CNS. Thus, viruses might invade nervous systems by infecting the endothelial cells of the BBB and the blood–CSF barrier in the choroid plexus. This hypothesis was strongly supported by the study conducted by Paniz-Mondolfi et al. [25]. The authors captured the viral particles using a cytoplasmic vacuole at the endothelial neural cell interface in a transmission electron microscope, which suggests that SARS-CoV-2 could bind to vascular endothelium, penetrate the BBB, and invade nervous tissues through hematogenous pathways. However, some researchers believe that the hematogenous route is not the only pathway, and that the neuronal retrograde transmission serves as another potential mechanism. In this route, SARS-CoV-2 might first invade peripheral nerve terminals and infect the CNS retrogradely. Previous animal studies on SARS-CoV and OC43-CoV had suggested the virus could enter the brain by disruption of the nasal epithelium and lead to subsequent neuronal dissemination when administered intranasally [46] [49]. Due to the high similarity among SARS-CoV, SARS-CoV-2, and OC43-CoV, it is likely that this same route also works in COVID-19. Notably, anosmia and dysgeusia were reported recently to be prevalent among patients with COVID-19 despite a lack of upper respiratory symptoms [23, 37]. In addition, ACE2 and other entry genes of SARS-CoV-2 are found to be highly expressed by sustentacular and non-neuronal cells in the human olfactory neuroepithelium [47, 48]. However, definitive evidence for this transmission route is lacking, and more solid pathological and experimental investigations should be conducted to validate this pathway.
Maladaptive inflammatory responses can also contribute to the neurological manifestations of COVID-19, especially in those patients in whom no virus RNA is detected in CSF. In the early phase of COVID-19, the increased secretion of inflammatory cytokines (e.g., IL-1β, IFN-γ, TNF-α, IL-4, IL-10) was a signature feature caused by rapid viral replication and secondary cellular injury. In addition, higher plasma levels of these inflammatory cytokines were observed in the ICU patients, which suggests that a cytokine storm presented in the severe patients [12]. This cytokine storm could induce various neurological symptoms and was previously reported to be able to disrupt the BBB and induce neuroinflammation in the sepsis [27, 50, 51]. In addition, the neutralizing antibodies (anti-S protein lgG), which are assumed to clear the virus and promote the recovery, can also cause severe secondary injury by altering inflammatory responses. In a previous study on SARS-CoV, anti-S protein lgG was found to facilitate severe tissue injury in other organs, such as the lung [52, 53]. In a recent case series of neurologic features in severe SARS-CoV-2 infection, oligoclonal bands and elevated IgG were detected in the CSF, which suggests that the activation of the immune system might be a double-edged sword [36].
Limitations
This systematic review with meta-analysis has several limitations. First, in the meta-analysis of the unspecific manifestations we included all the related symptoms, some of which were not classical neurological presentations. Neurological involvement could contribute partially to these symptoms, and an overall analysis may exaggerate its role in COVID-19. Second, in the systematic review, most of the included papers on clinical characteristics were of retrospective design and were performed in China, which could introduce potential bias. Third, the studies on specific neurological symptoms and diseases were mostly case reports and were limited. Fourth, during the outbreak of COVID-19, the influx of numerous COVID-19 patients made advanced neuroimaging, CSF tests, electrophysiological tests, and pathological examinations impractical due to high risk of cross-infection, which limited the evidence of neurological involvement. Fifth, this study was conducted during an ongoing outbreak. Many related studies have not yet been published, which could influence the results. The potential mechanism underlying the neurological manifestation in COVID-19 will be updated along with emerging evidence.
Conclusions
The neurological manifestations are various and prevalent in COVID-19, but are usually underestimated. Emerging clinical evidence suggests that neurological involvement is an important aspect of the disease. The multifaceted mechanisms are involved in its neurological impact, which includes both direct invasion and maladaptive inflammatory response. Nevertheless, more clinical and experimental research should be conducted to further explore the role of neurological manifestations on the disease progression and its underlying mechanism.
Availability of data and material
Most of analyzed data were included in this manuscript and supplemental materials. The relevant data can also be obtained with the request from any qualified investigator for purposes of replicating procedures and results.
References
Xu YH, Dong JH, An WM, Lv XY, Yin XP, Zhang JZ, Dong L, Ma X, Zhang HJ, Gao BL (2020) Clinical and computed tomographic imaging features of novel coronavirus pneumonia caused by SARS-CoV-2. J Infect 80(4):394–400. https://doi.org/10.1016/j.jinf.2020.02.017
Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, Wang B, Xiang H, Cheng Z, Xiong Y, Zhao Y, Li Y, Wang X, Peng Z (2020) Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan. China Jama. https://doi.org/10.1001/jama.2020.1585
Liu Y, Gayle AA, Wilder-Smith A, Rocklöv J (2020) The reproductive number of COVID-19 is higher compared to SARS coronavirus. J Travel Med. https://doi.org/10.1093/jtm/taaa021
Tian S, Hu N, Lou J, Chen K, Kang X, Xiang Z, Chen H, Wang D, Liu N, Liu D, Chen G, Zhang Y, Li D, Li J, Lian H, Niu S, Zhang L, Zhang J (2020) Characteristics of COVID-19 infection in Beijing. J Infect 80(4):401–406. https://doi.org/10.1016/j.jinf.2020.02.018
Gupta N, Agrawal S, Ish P, Mishra S, Gaind R, Usha G, Singh B, Sen MK, Covid Working Group SH (2020) Clinical and epidemiologic profile of the initial COVID-19 patients at a tertiary care centre in India. Monaldi Arch Chest Dis. https://doi.org/10.4081/monaldi.2020.1294
Yang W, Cao Q, Qin L, Wang X, Cheng Z, Pan A, Dai J, Sun Q, Zhao F, Qu J, Yan F (2020) Clinical characteristics and imaging manifestations of the 2019 novel coronavirus disease (COVID-19): a multi-center study in Wenzhou city, Zhejiang, China. J Infect 80(4):388–393. https://doi.org/10.1016/j.jinf.2020.02.016
Chen T, Wu D, Chen H, Yan W, Yang D, Chen G, Ma K, Xu D, Yu H, Wang H, Wang T, Guo W, Chen J, Ding C, Zhang X, Huang J, Han M, Li S, Luo X, Zhao J, Ning Q (2020) Clinical characteristics of 113 deceased patients with coronavirus disease 2019: retrospective study. BMJ 368:m1091. https://doi.org/10.1136/bmj.m1091
Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He JX, Liu L, Shan H, Lei CL, Hui DSC, Du B, Li LJ, Zeng G, Yuen KY, Chen RC, Tang CL, Wang T, Chen PY, Xiang J, Li SY, Wang JL, Liang ZJ, Peng YX, Wei L, Liu Y, Hu YH, Peng P, Wang JM, Liu JY, Chen Z, Li G, Zheng ZJ, Qiu SQ, Luo J, Ye CJ, Zhu SY, Zhong NS (2020) Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med 382(18):1708–1720. https://doi.org/10.1056/NEJMoa2002032
Liu K, Fang YY, Deng Y, Liu W, Wang MF, Ma JP, Xiao W, Wang YN, Zhong MH, Li CH, Li GC, Liu HG (2020) Clinical characteristics of novel coronavirus cases in tertiary hospitals in Hubei Province. Chin Med J (Engl) 133(9):1025–1031. https://doi.org/10.1097/cm9.0000000000000744
Yang X, Yu Y, Xu J, Shu H, Xia J, Liu H, Wu Y, Zhang L, Yu Z, Fang M, Yu T, Wang Y, Pan S, Zou X, Yuan S, Shang Y (2020) Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet Respir Med 8(5):475–481. https://doi.org/10.1016/s2213-2600(20)30079-5
Zhang G, Hu C, Luo L, Fang F, Chen Y, Li J, Peng Z, Pan H (2020) Clinical features and short-term outcomes of 221 patients with COVID-19 in Wuhan, China. J Clin Virol 127:104364. https://doi.org/10.1016/j.jcv.2020.104364
Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, Zhang L, Fan G, Xu J, Gu X, Cheng Z, Yu T, Xia J, Wei Y, Wu W, Xie X, Yin W, Li H, Liu M, Xiao Y, Gao H, Guo L, Xie J, Wang G, Jiang R, Gao Z, Jin Q, Wang J, Cao B (2020) Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 395(10223):497–506. https://doi.org/10.1016/S0140-6736%2820%2930183-5
Xu XW, Wu XX, Jiang XG, Xu KJ, Ying LJ, Ma CL, Li SB, Wang HY, Zhang S, Gao HN, Sheng JF, Cai HL, Qiu YQ, Li LJ (2020) Clinical findings in a group of patients infected with the 2019 novel coronavirus (SARS-Cov-2) outside of Wuhan, China: retrospective case series. BMJ 368:m606. https://doi.org/10.1136/bmj.m606
Covid-19 National Emergency Response Center E, Case Management Team KCfDC, Prevention (2020) Early epidemiological and clinical characteristics of 28 cases of coronavirus disease in South Korea. Osong Public Health Res Perspect 11(1):8–14. https://doi.org/10.24171/j.phrp.2020.11.1.03
Qian GQ, Yang NB, Ding F, Ma AHY, Wang ZY, Shen YF, Shi CW, Lian X, Chu JG, Chen L, Wang ZY, Ren DW, Li GX, Chen XQ, Shen HJ, Chen XM (2020) Epidemiologic and clinical characteristics of 91 hospitalized patients with COVID-19 in Zhejiang, China: a retrospective, multi-centre case series. Qjm Epub. https://doi.org/10.1093/qjmed/hcaa089
Chang D, Lin M, Wei L, Xie L, Zhu G, Dela Cruz CS, Sharma L (2020) Epidemiologic and clinical characteristics of novel coronavirus infections involving 13 patients outside Wuhan, China. JAMA 323(11):1092–1093. https://doi.org/10.1001/jama.2020.1623
Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y, Qiu Y, Wang J, Liu Y, Wei Y, Xia J, Yu T, Zhang X, Zhang L (2020) Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet 395(10223):507–513. https://doi.org/10.1016/S0140-6736%2820%2930211-7
Zhang X, Cai H, Hu J, Lian J, Gu J, Zhang S, Ye C, Lu Y, Jin C, Yu G, Jia H, Zhang Y, Sheng J, Li L, Yang Y (2020) Epidemiological, clinical characteristics of cases of SARS-CoV-2 infection with abnormal imaging findings. Int J Infect Dis 94:81–87. https://doi.org/10.1016/j.ijid.2020.03.040
Xu X, Yu C, Qu J, Zhang L, Jiang S, Huang D, Chen B, Zhang Z, Guan W, Ling Z, Jiang R, Hu T, Ding Y, Lin L, Gan Q, Luo L, Tang X, Liu J (2020) Imaging and clinical features of patients with 2019 novel coronavirus SARS-CoV-2. Eur J Nucl Med Mol Imaging 47(5):1275–1280. https://doi.org/10.1007/s00259-020-04735-9
Fan H, Zhang L, Huang B, Zhu M, Zhou Y, Yu W, Zhu L, Cheng S, Tao X, Zhang H, Chen J (2020) Retrospective analysis of clinical features in 101 death cases with COVID-19. medRxiv. https://doi.org/10.1101/2020.03.09.20033068
Leung KS-S, Ng TT-L, Wu AK-L, Yau MC-Y, Lao H-Y, Choi M-P, Tam KK-G, Lee L-K, Wong BK-C, Ho AY-M, Yip K-T, Lung K-C, Liu RW-T, Tso EY-K, Leung W-S, Chan M-C, Ng Y-Y, Sin K-M, Fung KS-C, Chau SK-Y, To W-K, Que T-L, Shum DH-K, Yip SP, Yam W-C, Siu GKH (2020) A territory-wide study of early COVID-19 outbreak in Hong Kong community: a clinical, epidemiological and phylogenomic investigation. medRxiv. https://doi.org/10.1101/2020.03.30.20045740
Zhao K, Huang J, Dai D, Feng Y, Liu L, Nie S (2020) Acute myelitis after SARS-CoV-2 infection: a case report. medRxiv. https://doi.org/10.1101/2020.03.16.20035105
Levinson R, Elbaz M, Ben-Ami R, Shasha D, Levinson T, Choshen G, Petrov K, Gadoth A, Paran Y (2020) Anosmia and dysgeusia in patients with mild SARS-CoV-2 infection. medRxiv. https://doi.org/10.1101/2020.04.11.20055483
Yan CH, Faraji F, Prajapati DP, Boone CE, DeConde AS (2020) Association of chemosensory dysfunction and Covid-19 in patients presenting with influenza-like symptoms. Int Forum Allergy Rhinol. https://doi.org/10.1002/alr.22579
Paniz-Mondolfi A, Bryce C, Grimes Z, Gordon RE, Reidy J, Lednicky J, Sordillo EM, Fowkes M (2020) Central nervous system involvement by severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2). J Med Virol. https://doi.org/10.1002/jmv.25915
Zhang T, Rodricks MB, Hirsh E (2020) COVID-19-Associated acute disseminated encephalomyelitis: a case report. medRxiv. https://doi.org/10.1101/2020.04.16.20068148
Poyiadji NA-O, Shahin GA-O, Noujaim DA-O, Stone MA-O, Patel SA-O, Griffith BA-O (2020) COVID-19-associated acute hemorrhagic necrotizing encephalopathy: CT and MRI features. Radiology. https://doi.org/10.1148/radiol.2020201187
Ye M, Ren Y, Lv T (2020) Encephalitis as a clinical manifestation of COVID-19. Brain Behav Immun Epub. https://doi.org/10.1016/j.bbi.2020.04.017
Klopfenstein T, Kadiane-Oussou NJ, Toko L, Royer PY, Lepiller Q, Gendrin V, Zayet S (2020) Features of anosmia in COVID-19. Medecine et Maladies Infectieuses. https://doi.org/10.1016/j.medmal.2020.04.006
Moriguchi T, Harii N, Goto J, Harada D, Sugawara H, Takamino J, Ueno M, Sakata H, Kondo K, Myose N, Nakao A, Takeda M, Haro H, Inoue O, Suzuki-Inoue K, Kubokawa K, Ogihara S, Sasaki T, Kinouchi H, Kojin H, Ito M, Onishi H, Shimizu T, Sasaki Y, Enomoto N, Ishihara H, Furuya S, Yamamoto T, Shimada S (2020) A first case of meningitis/encephalitis associated with SARS-Coronavirus-2. Int J Infect Dis 94:55–58. https://doi.org/10.1016/j.ijid.2020.03.062
Sedaghat Z, Karimi N (2020) Guillain Barre syndrome associated with COVID-19 infection: a case report. J Clin Neurosci. https://doi.org/10.1016/j.jocn.2020.04.062
Toscano G, Palmerini F, Ravaglia S, Ruiz L, Invernizzi P, Cuzzoni MG, Franciotta D, Baldanti F, Daturi R, Postorino P, Cavallini A, Micieli G (2020) Guillain-Barré syndrome associated with SARS-CoV-2. N Engl J Med Epub. https://doi.org/10.1056/NEJMc2009191
Virani A, Rabold E, Hanson T, Haag A, Elrufay R, Cheema T, Balaan M, Bhanot N (2020) Guillain-Barré Syndrome associated with SARS-CoV-2 infection. IDCases. https://doi.org/10.1016/j.idcr.2020.e00771
Zhao H, Shen D, Zhou H, Liu J, Chen S (2020) Guillain-Barré syndrome associated with SARS-CoV-2 infection: causality or coincidence? Lancet Neurol 19:383–384. https://doi.org/10.1016/s1474-4422(20)30109-5
Gutiérrez-Ortiz C, Méndez A, Rodrigo-Rey S, San Pedro-Murillo E, Bermejo-Guerrero L, Gordo-Mañas R, de Aragón-Gómez F, Benito-León J (2020) Miller Fisher syndrome and polyneuritis cranialis in COVID-19. Neurology. https://doi.org/10.1212/wnl.0000000000009619
Helms J, Kremer S, Merdji H, Clere-Jehl R, Schenck M, Kummerlen C, Collange O, Boulay C, Fafi-Kremer S, Ohana M, Anheim M, Meziani F (2020) Neurologic features in severe SARS-CoV-2 infection. N Engl J Med Epub. https://doi.org/10.1056/NEJMc2008597
Lechien JR, Chiesa-Estomba CM, De Siati DR, Horoi M, Le Bon SD, Rodriguez A, Dequanter D, Blecic S, El Afia F, Distinguin L, Chekkoury-Idrissi Y, Hans S, Delgado IL, Calvo-Henriquez C, Lavigne P, Falanga C, Barillari MR, Cammaroto G, Khalife M, Leich P, Souchay C, Rossi C, Journe F, Hsieh J, Edjlali M, Carlier R, Ris L, Lovato A, De Filippis C, Coppee F, Fakhry N, Ayad T, Saussez S (2020) Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (COVID-19): a multicenter European study. Eur Arch Otorhinolaryngol. https://doi.org/10.1007/s00405-020-05965-1
Al Saiegh F, Ghosh R, Leibold A, Avery MB, Schmidt RF, Theofanis T, Mouchtouris N, Philipp L, Peiper SC, Wang ZX, Rincon F, Tjoumakaris SI, Jabbour P, Rosenwasser RH, Gooch MR (2020) Status of SARS-CoV-2 in cerebrospinal fluid of patients with COVID-19 and stroke. J Neurol Neurosurg Psychiatry. https://doi.org/10.1136/jnnp-2020-323522
Pilotto A, Odolini S, Masciocchi S, Comelli A, Volonghi I, Gazzina S, Nocivelli S, Pezzini A, Foca E, Caruso A, Leonardi M, Pasolini MP, Gasparotti R, Castelli F, Padovani A (2020) Steroid-responsive severe encephalopathy in SARS-CoV-2 infection. medRxiv. https://doi.org/10.1101/2020.04.12.20062646
Eliezer M, Hautefort C, Hamel AL, Verillaud B, Herman P, Houdart E, Eloit C (2020) Sudden and complete olfactory loss function as a possible symptom of COVID-19. JAMA Otolaryngol Head Neck Surg. https://doi.org/10.1001/jamaoto.2020.0832
Bernard-Valnet R, Pizzarotti B, Anichini A, Demars Y, Russo E, Schmidhauser M, Cerruti-Sola J, Rossetti AO, Du Pasquier R (2020) Two patients with acute meningo-encephalitis concomitant to SARS-CoV-2 infection. medRxiv. https://doi.org/10.1101/2020.04.17.20060251
Mao L, Jin H, Wang M, Hu Y, Chen S, He Q, Chang J, Hong C, Zhou Y, Wang D, Miao X, Li Y, Hu B (2020) Neurologic manifestations of hospitalized patients with coronavirus disease 2019 in Wuhan, China. JAMA Neurol. https://doi.org/10.1001/jamaneurol.2020.1127
Li YC, Bai WZ, Hashikawa T (2020) The neuroinvasive potential of SARS-CoV2 may play a role in the respiratory failure of COVID-19 patients. J Med Virol. https://doi.org/10.1002/jmv.25728
Deng Y, Tan X, Li ML, Wang WZ, Wang YK (2019) Angiotensin-converting enzyme 2 in the rostral ventrolateral medulla regulates cholinergic signaling and cardiovascular and sympathetic responses in hypertensive rats. Neurosci Bull 35(1):67–78. https://doi.org/10.1007/s12264-018-0298-3
Chen R, Wang K, Yu J, Chen Z, Wen C, Xu Z (2020) The spatial and cell-type distribution of SARS-CoV-2 receptor ACE2 in human and mouse brain. bioRxiv. https://doi.org/10.1101/2020.04.07.030650
Netland J, Meyerholz DK, Moore S, Cassell M, Perlman S (2008) Severe acute respiratory syndrome coronavirus infection causes neuronal death in the absence of encephalitis in mice transgenic for human ACE2. J Virol 82(15):7264–7275. https://doi.org/10.1128/jvi.00737-08
Brann DH, Tsukahara T, Weinreb C, Lipovsek M, Van den Berge K, Gong B, Chance R, Macaulay IC, Chou H-j, Fletcher R, Das D, Street K, de Bezieux HR, Choi Y-G, Risso D, Dudoit S, Purdom E, Mill JS, Hachem RA, Matsunami H, Logan DW, Goldstein BJ, Grubb MS, Ngai J, Datta SR (2020) Non-neuronal expression of SARS-CoV-2 entry genes in the olfactory system suggests mechanisms underlying COVID-19-associated anosmia. bioRxiv. https://doi.org/10.1101/2020.03.25.009084
Fodoulian L, Tuberosa J, Rossier D, Landis BN, Carleton A, Rodriguez I (2020) SARS-CoV-2 receptor and entry genes are expressed by sustentacular cells in the human olfactory neuroepithelium. bioRxiv. https://doi.org/10.1101/2020.03.31.013268
Desforges M, Le Coupanec A, Dubeau P, Bourgouin A, Lajoie L, Dubé M, Talbot PJ (2019) Human coronaviruses and other respiratory viruses: underestimated opportunistic pathogens of the central nervous system? Viruses. https://doi.org/10.3390/v12010014
Meneses G, Cárdenas G, Espinosa A, Rassy D, Pérez-Osorio IN, Bárcena B, Fleury A, Besedovsky H, Fragoso G, Sciutto E (2019) Sepsis: developing new alternatives to reduce neuroinflammation and attenuate brain injury. Ann N Y Acad Sci 1437(1):43–56. https://doi.org/10.1111/nyas.13985
Eccles R (2005) Understanding the symptoms of the common cold and influenza. Lancet Infect Dis 5(11):718–725. https://doi.org/10.1016/s1473-3099(05)70270-x
Liu L, Wei Q, Lin Q, Fang J, Wang H, Kwok H, Tang H, Nishiura K, Peng J, Tan Z, Wu T, Cheung KW, Chan KH, Alvarez X, Qin C, Lackner A, Perlman S, Yuen KY, Chen Z (2019) Anti-spike IgG causes severe acute lung injury by skewing macrophage responses during acute SARS-CoV infection. JCI Insight. https://doi.org/10.1172/jci.insight.123158
Bolles M, Deming D, Long K, Agnihothram S, Whitmore A, Ferris M, Funkhouser W, Gralinski L, Totura A, Heise M, Baric RS (2011) A double-inactivated severe acute respiratory syndrome coronavirus vaccine provides incomplete protection in mice and induces increased eosinophilic proinflammatory pulmonary response upon challenge. J Virol 85(23):12201–12215. https://doi.org/10.1128/jvi.06048-11
Acknowledgements
This project was supported by the National Natural Science Foundation of China (number 81201026), National Natural Science Foundation of Hubei province (number 2017CFB394, 2016CFB643), Key Support Project of fundamental frontier in Wuhan (number 2019020701011458).
Funding
This project was supported by the National Natural Science Foundation of China (number 81201026), National Natural Science Foundation of Hubei province (numbers 2017CFB394, 2016CFB643), Key Support Project of fundamental frontier in Wuhan (number 2019020701011458).
Author information
Authors and Affiliations
Contributions
HW supervised and conceived the study, analyzed and interpreted data, and wrote and revised the manuscript. LW and YS performed the study, searched the literature, collected and analyzed data, and wrote the first draft of manuscript. ML, HC, YY, and HZ conceived the study and contributed to data interpretation and substantial revision of the manuscript.
Corresponding author
Ethics declarations
Conflicts of interest
All authors declare no conflicts of interest.
Ethics approval
This study was approved by the Ethics Committee of the Tongji Medical College, Huazhong University of Science and Technology.
Informed consent
The informed consent was exempted because it was a secondary analysis of the published studies.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Wang, L., Shen, Y., Li, M. et al. Clinical manifestations and evidence of neurological involvement in 2019 novel coronavirus SARS-CoV-2: a systematic review and meta-analysis. J Neurol 267, 2777–2789 (2020). https://doi.org/10.1007/s00415-020-09974-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-020-09974-2