Fruit and Vegetable Intake Assessed by Food Frequency Questionnaire and Plasma Carotenoids: A Validation Study in Adults

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Experimental Section
2.1. Biochemical Assay
2.2. Ethics
2.3. Statistical Methods

{kind=link}
{kind=link}
| All | Healthy Weight (BMI < 25) | Overweight (BMI ≥ 25) | p | ||||
|---|---|---|---|---|---|---|---|
| n = 38 | n = 20 | n = 18 | |||||
| Female | 25 (66%) | 14 (70%) | 11 (61%) | 0.73 | |||
| Supplement use | 20 (53%) | 10 (50%) | 10 (56%) | 0.76 | |||
| Median | (Min–Max) | Median | (Min–Max) | Median | (Min–Max) | ||
| Age (years) | 43.3 | (33.5–52.6) | 42.9 | (36.8–50.6) | 44.9 | (33.5–52.6) | 0.64 |
| Height (cm) | 169.3 | (151.4–188.0) | 169.8 | (161.6–184.5) | 168.3 | (151.4–188.0) | 0.24 |
| Weight (Kg) | 68.8 | (55.6–99.6) | 64.4 | (55.6–78.5) | 79.4 | (61.5–99.6) | <0.01 |
| BMI (kg/m2) | 24.4 | (19.4–37.8) | 22.5 | (19.4–24.5) | 27.9 | (25.1–37.8) | <0.01 |
| Waist (cm) | 83.4 | (67.7–111.4) | 78.8 | (67.7–91.4) | 91.1 | (76.9–111.4) | <0.01 |
| Fat Mass (Kg) | 21.3 | (7.0–48.3) | 14.6 | (7.0–23.8) | 24.5 | (14.5–48.3) | <0.01 |
| Fat Mass (%) | 26.6 | (11.2–50.9) | 20.8 | (11.2–35.3) | 34.3 | (17.8–50.9) | <0.01 |
| Fat Free Mass (Kg) | 48.1 | (38.9–77.4) | 48.1 | (40.6–63.4) | 48.5 | (38.9–77.4) | 0.70 |
| Fat Free Mass (%) | 73.4 | (49.1–88.8) | 79.2 | (64.7–88.8) | 65.7 | (49.1–82.2) | <0.01 |
| All | Healthy Weight (BMI < 25) | Overweight (BMI ≥ 25) | p | ||||
|---|---|---|---|---|---|---|---|
| n = 38 | n = 20 | n = 18 | |||||
| Median | (Min–Max) | Median | (Min–Max) | Median | (Min–Max) | ||
| Plasma Carotenoid (µg/dL) | |||||||
| α-carotene | 6.40 | (0.80–29.30) | 7.35 | (1.90–29.30) | 3.85 | (0.80–28.40) | 0.05 |
| β-carotene | 40.65 | (3.50–176.80) | 46.4 | (7.30–162.40) | 25.4 | (3.50–176.80) | 0.01 |
| Lycopene | 40.85 | (7.20–114.30) | 38.7 | (7.20–114.30) | 43.3 | (13.40–94.60) | 0.64 |
| Lutein-zeaxanthin | 21.05 | (7.50–64.60) | 24.95 | (9.40–64.60) | 16.3 | (7.50–38.40) | 0.05 |
| Cryptoxanthin | 7.60 | (1.70–18.80) | 8.95 | (1.70–16.50) | 5.25 | (2.70–18.80) | 0.06 |
| Median | (Min–Max) | Median | (Min–Max) | Median | (Min–Max) | ||
| FFQ Carotenoid (μg/day) | |||||||
| α-carotene | 12.78 | (3.67–74.16) | 12.8 | (3.67–74.16) | 12.15 | (4.30–26.89) | 0.88 |
| β-carotene | 57.72 | (11.98–191.3) | 57.65 | (11.98–191.33) | 59.84 | (26.09–98.53) | 0.98 |
| Lycopene | 95.27 | (34.09–194.3) | 89.15 | (34.09–194.28) | 96.11 | (39.27–176.69) | 0.54 |
| Lutein-zeaxanthin | 29.35 | (6.49–72.9) | 30.78 | (6.49–72.89) | 29.11 | (12.35–52.96) | 0.27 |
| Cryptoxanthin | 3.56 | (0.45–9.18) | 3.56 | (0.45–9.18) | 3.42 | (1.00–7.59) | 1 |
| FFQ Vegetables (serves/day) | |||||||
| All | 4.26 | (1.07–9.07) | 4.43 | (1.57–9.07) | 3.94 | (1.07–6.71) | 0.24 |
| FFQ Fruit (serves/day) | |||||||
| All | 2.57 | (0.20–4.71) | 2.57 | (0.20–4.01) | 2.55 | (0.30–4.71) | 0.77 |
3. Results
3.1. Descriptive Statistics
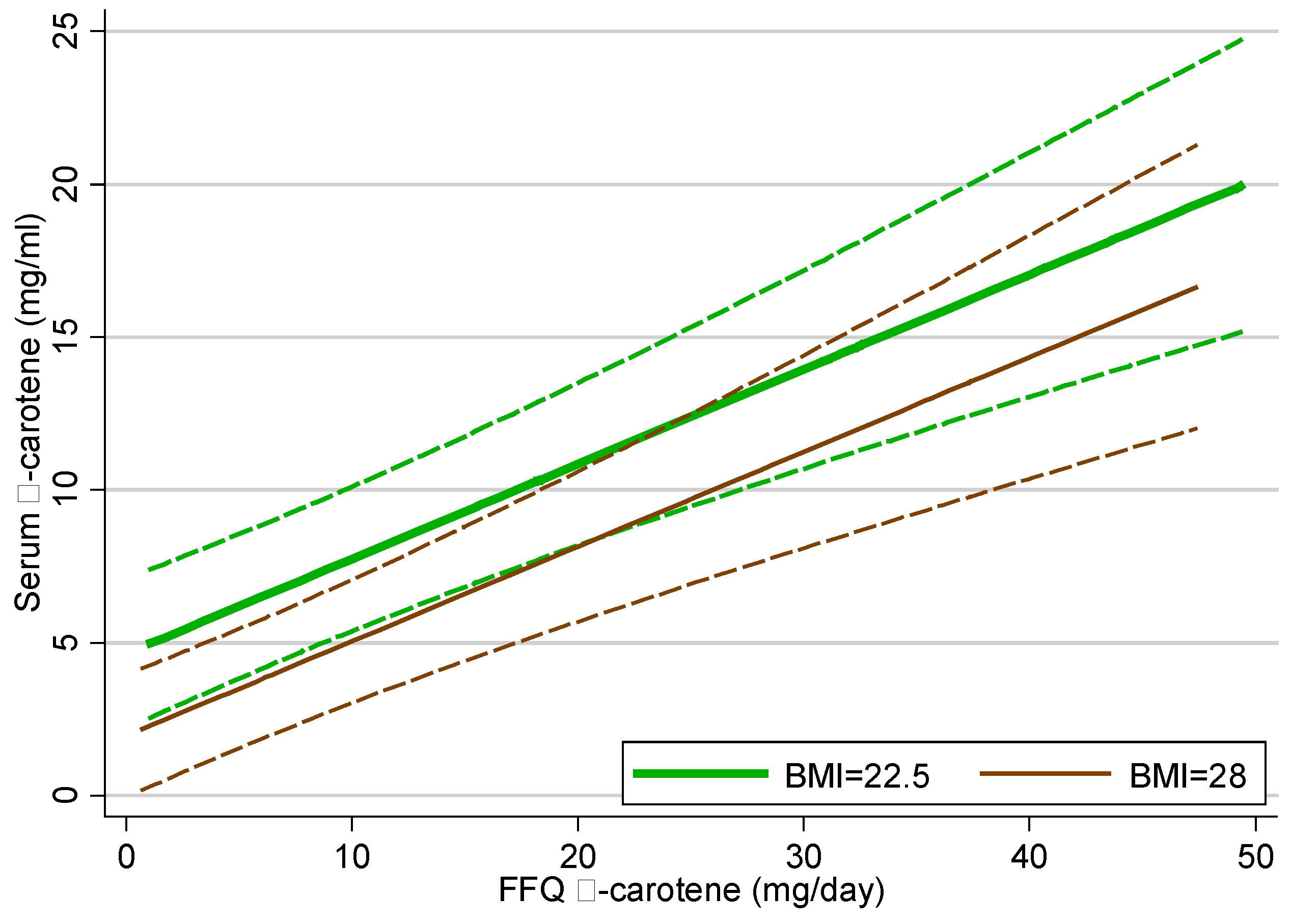
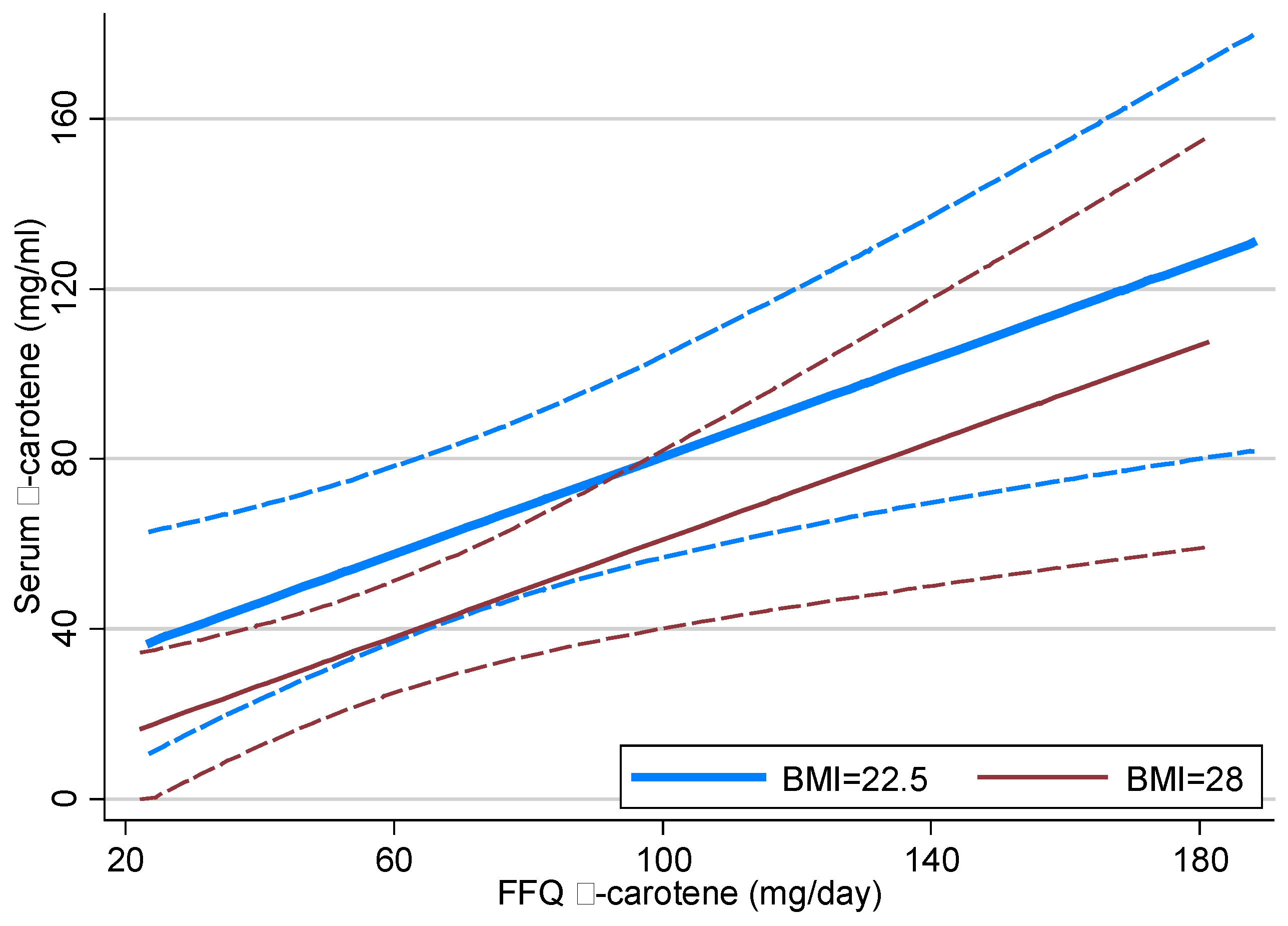
3.2. Linear Regression Modelling
| Anthropometric | p | FFQ Intake | p | Model R-squared | FFQ—Plasma Correlation | Correlation 95% CI |
|---|---|---|---|---|---|---|
| Plasma α-carotene | ||||||
| α-carotene | <0.001 | 0.26 | 0.52 | 0.35, 0.69 | ||
| BMI | 0.004 | α-carotene | <0.001 | 0.34 | 0.49 | 0.33, 0.64 |
| BMI | 0.001 | 0.11 | ||||
| Plasma β-carotene | ||||||
| β-carotene | 0.003 | 0.21 | 0.47 | 0.18, 0.75 | ||
| Veg Serves | 0.007 | 0.17 | 0.42 | 0.12, 0.71 | ||
| BMI | 0.016 | β-carotene | 0.004 | 0.31 | 0.41 | 0.15, 0.68 |
| Fat mass | 0.013 | Veg Serves | 0.013 | 0.25 | 0.34 | 0.08, 0.61 |
| BMI | 0.004 | 0.14 | ||||
| Fat mass | 0.003 | 0.14 | ||||
| Plasma Lycopene | ||||||
| Lycopene | 0.756 | 0.00 | ||||
| Plasma Lutein/zeaxanthin | ||||||
| Lutein/zeax | 0.041 | 0.09 | 0.26 | 0.01, 0.51 | ||
| BMI | <0.001 | Lutein/zeax | 0.095 | 0.20 | ||
| BMI | <0.001 | 0.14 | ||||
| Plasma Cryptoxanthin | ||||||
| Cryptoxant | 0.236 | 0.08 | ||||
| Fat mass | 0.005 | Supplements | 0.003 | 0.35 | ||
| Fat mass | <0.001 | 0.22 | ||||


4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Dauchet, L.; Amouyel, P.; Hercberg, S.; Dallongeville, J. Fruit and vegetable consumption and risk of coronary heart disease: A meta-analysis of cohort studies. J. Nutr. 2006, 136, 2588–2593. [Google Scholar] [PubMed]
- He, F.J.; Nowson, C.A.; Lucas, M.; MacGregor, G.A. Increased consumption of fruit and vegetables is related to a reduced risk of coronary heart disease: Meta-analysis of cohort studies. J. Hum. Hypertens. 2007, 21, 717–728. [Google Scholar] [CrossRef] [PubMed]
- Dauchet, L.; Amouyel, P.; Dallongeville, J. Fruit and vegetable consumption and risk of stroke: A meta-analysis of cohort studies. Neurology 2005, 65, 1193–1197. [Google Scholar] [CrossRef] [PubMed]
- He, F.J.; Nowson, C.A.; MacGregor, G.A. Fruit and vegetable consumption and stroke: Meta-analysis of cohort studies. Lancet 2006, 367, 320–326. [Google Scholar] [CrossRef] [PubMed]
- Villegas, R.; Shu, X.O.; Gao, Y.T.; Yang, G.; Elasy, T.; Li, H.; Zheng, W. Vegetable but not fruit consumption reduces the risk of type 2 diabetes in Chinese women. J. Nutr. 2008, 138, 574–580. [Google Scholar] [PubMed]
- Hamer, M.; Chida, Y. Intake of fruit, vegetables, and antioxidants and risk of type 2 diabetes: Systematic review and meta-analysis. J. Hypertens. 2007, 25, 2361–2369. [Google Scholar] [CrossRef] [PubMed]
- Park, J.Y.; Vollset, S.E.; Melse-Boonstra, A.; Chajes, V.; Ueland, P.M.; Slimani, N. Dietary intake and biological measurement of folate: A qualitative review of validation studies. Mol. Nutr. Food Res. 2013, 57, 562–581. [Google Scholar] [CrossRef] [PubMed]
- Preis, S.R.; Spiegelman, D.; Zhao, B.B.; Moshfegh, A.; Baer, D.J.; Willett, W.C. Application of a repeat-measure biomarker measurement error model to 2 validation studies: Examination of the effect of within-person variation in biomarker measurements. Am. J. Epidemiol. 2011, 173, 683–694. [Google Scholar] [CrossRef] [PubMed]
- Andersen, L.F.; Veierød, M.B.; Johansson, L.; Sakhi, A.; Solvoll, K.; Drevon, C.A. Evaluation of three dietary assessment methods and serum biomarkers as measures of fruit and vegetable intake, using the method of triads. Br. J. Nutr. 2005, 93, 519–527. [Google Scholar] [CrossRef] [PubMed]
- McNaughton, S.; Marks, G.; Gaffney, P.; Williams, G.; Green, A. Validation of a food frequency questionnaire assessment of carotenoid and vitamin E intake using weighed food records and plasma biomarkers: The method of triads model. Eur. J. Clin. Nutr. 2005, 59, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Block, G.; Norkus, E.; Hudes, M.; Mandel, S.; Helzlsouer, K. Which plasma antioxidants are most related to fruit and vegetable consumption? Am. J. Epidemiol. 2001, 154, 1113–1118. [Google Scholar] [CrossRef] [PubMed]
- Campbell, D.; Gross, M.; Martini, M.; Grandits, G.; Slavin, J.; Potter, J. Plasma carotenoids as biomarkers of vegetable and fruit intake. Cancer Epidem. Biomar. 1994, 3, 493–500. [Google Scholar]
- Collins, C.; Burrows, T.; Truby, H.; Morgan, P.; Wright, I.; Davies, P.; Callister, R. Comparison of energy intake in toddlers assessed by food frequency questionnaire and total energy expenditure measured by the doubly labeled water method. J. Acad. Nutr. Diet. 2013, 113, 459–463. [Google Scholar] [CrossRef] [PubMed]
- Collins, C.; Watson, J.; Guest, M.; Boggess, M.; Duncanson, K.; Pezdirc, K.; Rollo, M.; Hutchesson, M.; Burrows, T. Reproducibility and comparative validity of a food frequency questionnaire for adults. Clin. Nutr. 2014, 33, 906–914. [Google Scholar] [CrossRef] [PubMed]
- Burrows, T.; Truby, H.; Morgan, P.; Callister, R.; Davies, P.; Collins, C. A comparison and validation of child versus parent reporting of children’s energy intake using food frequency questionnaires versus food records: Who’s an accurate reporter? Clin. Nutr. 2013, 32, 613–618. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. National Nutrition Survey: Nutrient Intakes and Physical Measurements; Australian Bureau of Statistics: Canberra, Australia, 1998.
- Chug-Ahuja, J.; Holden, J.; Forman, M.; Reed Mangels, A.; Beecher, G.; Lanza, E. The development and application of a carotenoid database for fruits, vegetables and selected multi-component foods. J. Am. Diet. Assoc. 1993, 93, 318–323. [Google Scholar] [CrossRef] [PubMed]
- Barua, A.; Kostic, D.; Olsen, J. New simplified procedures for the extraction and simultaneous high-performance liquid chromatographic analysis of retinol, tocopherols, and carotenoids in human serum. J. Chromatogr. B 1993, 617, 257–264. [Google Scholar] [CrossRef]
- Burrows, T.; Warren, J.; Colyvas, K.; Garg, M.; Collins, C. Validation of overweight children’s fruit and vegetable intake using plasma carotenoids. Obesity 2009, 17, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Reitman, A.; Friedrich, I.; Ben-Amotz, A.; Levy, Y. Low plasma antioxidants and normal plasma B vitamins and homocysteine in patients with severe obesity. Isr. Med. Assoc. J. 2002, 4, 590–593. [Google Scholar] [PubMed]
- Williams, R. A note on robust variance estimation for cluster-correlated data. Biometrics 2000, 56, 645–646. [Google Scholar] [CrossRef] [PubMed]
- StataCorp LP. Stata MP, version 12; Stata Statistical Software: College Station, TX, USA, 2012. [Google Scholar]
- Al-Delaimy, W.; van Kappel, A.; Ferrari, P.; Slimani, N.; Steghens, J.; Bingham, S.; Johansson, I.; Wallstrom, P.; Overvad, K.; Tionneland, A.; et al. Plasma carotenoids as biomarkers of intake of fruits and vegetables: Ecological level correlations in the European Prospective Investigation into Caner and Nutrition (EPIC). Eur. J. Clin. Nutr. 2005, 59, 1397–1408. [Google Scholar]
- Eliassen, A.; Hendrickson, S.; Brinton, L.; Buring, J.; Campos, H.; Dai, Q.; Dorgan, J.; Franke, A.; Gao, Y.; Goodman, M. Circulating carotenoids and risk of breast cancer: Pooled analysis of eight prospective studies. J. Natl. Cancer Inst. 2012, 104, 1905–1916. [Google Scholar] [CrossRef] [PubMed]
- Svilaas, A.; Sakhi, A.; Andersen, L.; Svilaas, T.; Ström, E.; Jacobs, D.; Ose, L.; Blomhoff, R. Intakes of antioxidants in coffee, wine, vegetables are correlated with plasma carotenoids in humans. J. Nutr. 2003, 134, 562–587. [Google Scholar]
- Castenmiller, J.; West, C. Bioavailability and bioconversion of carotenoids. Annu. Rev. Nutr. 1998, 18, 19–38. [Google Scholar] [CrossRef] [PubMed]
- Coyne, T.; Ibiebele, T.I.; Baade, P.D.; Dobson, A.; McClintock, C.; Dunn, S.; Leonard, D.; Shaw, J. Diabetes mellitus and serum carotenoids: Findings of a population-based study in Queensland, Australia. Am. J. Clin. Nutr. 2005, 82, 685–693. [Google Scholar] [PubMed]
- Satia, J.; Watters, J.; Galanko, J. Validation of an antioxidant nutrient questionnaire in whites and African Americans. J. Am. Diet. Assoc. 2009, 109, 502–508. [Google Scholar] [CrossRef] [PubMed]
- Coates, R.; Eley, J.; Block, G.; Gunter, E.; Sowell, A.; Grossman, C.; Greenberg, R. An evaluation of a Food Frequency Questionnaire for assessing dietary intake of specific carotenoids and vitamin E among low income black women. Am. J. Epidemiol. 1991, 134, 658–670. [Google Scholar] [PubMed]
- Goodman, G.; Thornquist, M.; Kestin, M.; Methc, B.; Anderson, G.; Omenn, G. The association between participant characteristics and serum concentrations of beta-carotene, retinol, retinyl palmitate, and alpha-tocopherol among participants in the Carotene and Retinol Efficacy Trial (CARET) for prevention of lung cancer. Cancer Epidem. Biomar. 1996, 5, 815–821. [Google Scholar]
- Molnar, D.; Decsi, T.; Koletzko, B. Reduced antioxidant status in obese children with multi-metabolic syndrome. Int. J. Obesity 2004, 28, 1197–1202. [Google Scholar] [CrossRef]
- Chung, H.-Y.; Ferreira, A.L.A.; Epstein, S.; Paiva, S.A.; Castaneda-Sceppa, C.; Johnson, E.J. Site-specific concentrations of carotenoids in adipose tissue: Relations with dietary and serum carotenoid concentrations in healthy adults. Am. J. Clin. Nutr. 2009, 90, 533–539. [Google Scholar] [CrossRef] [PubMed]
- Michaud, D.S.; Giovannucci, E.L.; Ascherio, A.; Rimm, E.B.; Forman, M.R.; Sampson, L.; Willett, W.C. Associations of plasma carotenoid concentrations and dietary intake of specific carotenoids in samples of two prospective cohort studies using a new carotenoid database. Cancer Epidemiol. Biomarkers Prev. 1998, 7, 283–290. [Google Scholar]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burrows, T.L.; Hutchesson, M.J.; Rollo, M.E.; Boggess, M.M.; Guest, M.; Collins, C.E. Fruit and Vegetable Intake Assessed by Food Frequency Questionnaire and Plasma Carotenoids: A Validation Study in Adults. Nutrients 2015, 7, 3240-3251. https://doi.org/10.3390/nu7053240
Burrows TL, Hutchesson MJ, Rollo ME, Boggess MM, Guest M, Collins CE. Fruit and Vegetable Intake Assessed by Food Frequency Questionnaire and Plasma Carotenoids: A Validation Study in Adults. Nutrients. 2015; 7(5):3240-3251. https://doi.org/10.3390/nu7053240
Chicago/Turabian StyleBurrows, Tracy L., Melinda J. Hutchesson, Megan E. Rollo, May M. Boggess, Maya Guest, and Clare E. Collins. 2015. "Fruit and Vegetable Intake Assessed by Food Frequency Questionnaire and Plasma Carotenoids: A Validation Study in Adults" Nutrients 7, no. 5: 3240-3251. https://doi.org/10.3390/nu7053240