Parental Child-Feeding in the Context of Child Temperament and Appetitive Traits: Evidence for a Biopsychosocial Process Model of Appetite Self-Regulation and Weight Status


Abstract
:1. Introduction
1.1. Child Temperament and Appetitive Traits
1.2. Parental Controlling Child-Feeding Behavior
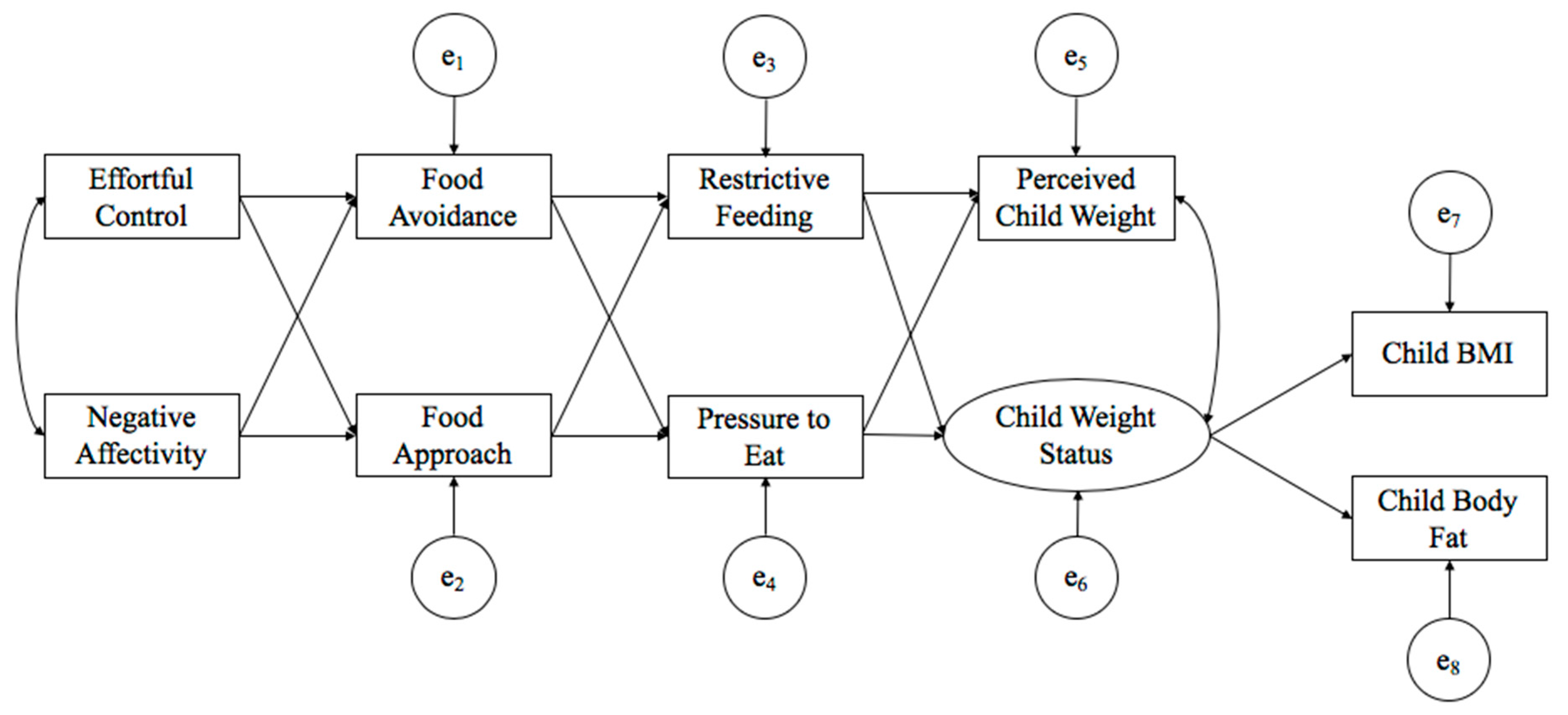
1.3. Present Study
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.3. Measures
2.4. Data Analysis
3. Results
3.1. Descriptive Statistics
3.2. Path Model
3.3. Mediation Analyses.
3.4. Tests of Sex, Poverty Status and Racial/Ethnic Group Differences
4. Discussion
4.1. Relations Among Study Variables
4.2. Links Between Temperament Traits and Appetitive Traits
4.3. Links between Appetitive Traits and Parental Controlling Feeding Practices
4.4. Links between Controlling Feeding Practices and Child Weight
4.5. Mediating Mechanisms from Child Temperament to Child Body Composition
4.6. Sex, Poverty Status and Race/Ethnicity Differences
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- National Heart, Lung, and Blood Institute. Working Group Report on Future Research Directions in Childhood Obesity Prevention and Treatment. 2007. Available online: https://www.nhlbi.nih.gov/events/2007/working-group-report-future-research-directions-childhood-obesity-prevention-and (accessed on 30 October 2020).
- Skinner, A.C.; Perrin, E.M.; Skelton, J.A. Prevalence of obesity and severe obesity in US children, 1999–2014. Obesity 2016, 24, 1116–1123. [Google Scholar] [CrossRef] [Green Version]
- Anzman-Frasca, S.; Stifter, C.A.; Birch, L.L. Temperament and Childhood Obesity Risk. J. Dev. Behav. Pediatr. 2012, 33, 732–745. [Google Scholar] [CrossRef]
- Haycraft, E.; Farrow, C.; Meyer, C.; Powell, F.; Blissett, J. Relationships between temperament and eating behaviours in young children. Appetite 2011, 56, 689–692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, T.; Dixon, W.E.; Dalton, W.T.; Tudiver, F.; Liu, X. Joint Effects of Child Temperament and Maternal Sensitivity on the Development of Childhood Obesity. Matern. Child Health J. 2010, 15, 469–477. [Google Scholar] [CrossRef] [PubMed]
- Braden, A.; Rhee, K.; Peterson, C.B.; Rydell, S.A.; Zucker, N.; Boutelle, K. Associations between child emotional eating and general parenting style, feeding practices, and parent psychopathology. Appetite 2014, 80, 35–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russell, C.G.; Russell, A. A biopsychosocial approach to processes and pathways in the development of overweight and obesity in childhood: Insights from developmental theory and research. Obes. Rev. 2019, 20, 725–749. [Google Scholar] [CrossRef] [PubMed]
- Derryberry, D.; Rothbart, M.K. Arousal, affect, and attention as components of temperament. J. Personal. Soc. Psychol. 1988, 55, 958–966. [Google Scholar] [CrossRef]
- Rothbart, M.K. Temperament, Development, and Personality. Curr. Dir. Psychol. Sci. 2007, 16, 207–212. [Google Scholar] [CrossRef]
- Posner, M.I.; Rothbart, M.K.; Sheese, B.E. Attention genes. Dev. Sci. 2007, 10, 24–29. [Google Scholar] [CrossRef]
- Caspi, A.; Roberts, B.W.; Shiner, R.L. Personality Development: Stability and Change. Annu. Rev. Psychol. 2005, 56, 453–484. [Google Scholar] [CrossRef] [Green Version]
- Elliot, A.J.; Thrash, T.M. Approach and Avoidance Temperament as Basic Dimensions of Personality. J. Pers. 2010, 78, 865–906. [Google Scholar] [CrossRef] [PubMed]
- Stoeckel, L.E.; Birch, L.L.; Heatherton, T.; Mann, T.; Hunter, C.; Czajkowski, S.; Onken, L.; Berger, P.K.; Savage, C.R. Psychological and neural contributions to appetite self-regulation. Obesity 2017, 25, S17–S25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saltzman, J.A.; Fiese, B.H.; Bost, K.K.; McBride, B.A. Development of Appetite Self-Regulation: Integrating Perspectives From Attachment and Family Systems Theory. Child Dev. Perspect. 2017, 12, 51–57. [Google Scholar] [CrossRef]
- Webber, L.; Cooke, L.; Hill, C.; Wardle, J. Associations between Children’s Appetitive Traits and Maternal Feeding Practices. J. Am. Diet. Assoc. 2010, 110, 1718–1722. [Google Scholar] [CrossRef]
- Powell, F.C.; Farrow, C.V.; Meyer, C. Food avoidance in children. The influence of maternal feeding practices and behaviours. Appetite 2011, 57, 683–692. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Z.; SooHoo, M.; Zhou, Q.; Perez, M.; Liew, J. Temperament as Risk and Protective Factors in Obesogenic Eating: Relations Among Parent Temperament, Child Temperament, and Child Food Preference and Eating. J. Genet. Psychol. 2019, 180, 75–79. [Google Scholar] [CrossRef]
- Carnell, S.; Wardle, J. Appetitive traits and child obesity: Measurement, origins and implications for intervention. Proc. Nutr. Soc. 2008, 67, 343–355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russell, C.G.; Worsley, T.; Worsley, A. Associations between appetitive traits and food preferences in preschool children. Food Qual. Prefer. 2016, 52, 172–178. [Google Scholar] [CrossRef]
- Zhou, Z.; Liew, J.; Yeh, Y.-C.; Perez, M. Appetitive Traits and Weight in Children: Evidence for Parents’ Controlling Feeding Practices as Mediating Mechanisms. J. Genet. Psychol. 2019, 181, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Larsen, J.K.; Hermans, R.C.; Sleddens, E.F.; Engels, R.C.; Fisher, J.O.; Kremers, S.P. How parental dietary behavior and food parenting practices affect children’s dietary behavior. Interacting sources of influence? Appetite 2015, 89, 246–257. [Google Scholar] [CrossRef]
- Black, M.M.; Aboud, F.E. Responsive Feeding Is Embedded in a Theoretical Framework of Responsive Parenting. J. Nutr. 2011, 141, 490–494. [Google Scholar] [CrossRef] [Green Version]
- Wehrly, S.E.; Bonilla, C.; Perez, M.; Liew, J. Controlling parental feeding practices and child body composition in ethnically and economically diverse preschool children. Appetite 2013, 73, 163–171. [Google Scholar] [CrossRef] [Green Version]
- Ventura, A.K.; Birch, L.L. Does parenting affect children’s eating and weight status? Int. J. Behav. Nutr. Phys. Act. 2008, 5, 15. [Google Scholar] [CrossRef] [Green Version]
- Birch, L.L.; Fisher, J.O.; Davison, K.K. Learning to overeat: Maternal use of restrictive feeding practices promotes girls’ eating in the absence of hunger. Am. J. Clin. Nutr. 2003, 78, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Hurley, K.M.; Cross, M.B.; Hughes, S.O. A Systematic Review of Responsive Feeding and Child Obesity in High-Income Countries. J. Nutr. 2011, 141, 495–501. [Google Scholar] [CrossRef] [Green Version]
- Jansen, P.W.; Tharner, A.; Van Der Ende, J.; Wake, M.; Raat, H.; Hofman, A.; Verhulst, F.C.; Van Ijzendoorn, M.H.; Jaddoe, V.W.; Tiemeier, H. Feeding practices and child weight: Is the association bidirectional in preschool children? Am. J. Clin. Nutr. 2014, 100, 1329–1336. [Google Scholar] [CrossRef] [Green Version]
- Rodgers, R.F.; Paxton, S.J.; Massey, R.; Campbell, K.J.; Wertheim, E.H.; Skouteris, H.; Gibbons, K. Maternal feeding practices predict weight gain and obesogenic eating behaviors in young children: A prospective study. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jansen, E.; Mallan, K.M.; Daniels, L.A. Extending the validity of the Feeding Practices and Structure Questionnaire. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 90. [Google Scholar] [CrossRef] [Green Version]
- Jansen, P.W.; De Barse, L.M.; Jaddoe, V.W.; Verhulst, F.C.; Franco, O.H.; Tiemeier, H. Bi-directional associations between child fussy eating and parents’ pressure to eat: Who influences whom? Physiol. Behav. 2017, 176, 101–106. [Google Scholar] [CrossRef]
- Kidwell, K.M.; Kozikowski, C.; Roth, T.; Lundahl, A.; Nelson, T.D. Concurrent and Longitudinal Associations Among Temperament, Parental Feeding Styles, and Selective Eating in a Preschool Sample. J. Pediatr. Psychol. 2017, 43, 572–583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braungart-Rieker, J.M.; Moore, E.S.; Planalp, E.M.; Lefever, J.B. Psychosocial pathways to childhood obesity: A pilot study involving a high risk preschool sample. Eat. Behav. 2014, 15, 528–531. [Google Scholar] [CrossRef]
- Harrison, K.; Bost, K.K.; McBride, B.A.; Donovan, S.M.; Grigsby-Toussaint, D.S.; Kim, J.; Liechty, J.M.; Wiley, A.; Teran-Garcia, M.; Jacobsohn, G.C. Toward a Developmental Conceptualization of Contributors to Overweight and Obesity in Childhood: The Six-Cs Model. Child Dev. Perspect. 2011, 5, 50–58. [Google Scholar] [CrossRef]
- Peña, M.-M.; Dixon, B.; Taveras, E.M. Are You Talking to ME? The Importance of Ethnicity and Culture in Childhood Obesity Prevention and Management. Child. Obes. 2012, 8, 23–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Putnam, S.P.; Rothbart, M.K. Development of Short and Very Short Forms of the Children’s Behavior Questionnaire. J. Pers. Assess. 2006, 87, 102–112. [Google Scholar] [CrossRef] [PubMed]
- Wardle, J.; Guthrie, C.A.; Sanderson, S.; Rapoport, L. Development of the Children’s Eating Behaviour Questionnaire. J. Child Psychol. Psychiatry 2001, 42, 963–970. [Google Scholar] [CrossRef] [Green Version]
- Birch, L.; Fisher, J.; Grimm-Thomas, K.; Markey, C.; Sawyer, R.; Johnson, S. Confirmatory factor analysis of the Child Feeding Questionnaire: A measure of parental attitudes, beliefs and practices about child feeding and obesity proneness. Appetite 2001, 36, 201–210. [Google Scholar] [CrossRef]
- McCarthy, H.D.; Cole, T.J.; Fry, T.; A Jebb, S.; Prentice, A.M. Body fat reference curves for children. Int. J. Obes. 2006, 30, 598–602. [Google Scholar] [CrossRef] [Green Version]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 7th ed.; Muthén & Muthén: Los Angelas, CA, USA, 1998. [Google Scholar]
- Schafer, J.L. Multiple imputation: A primer. Stat. Methods Med. Res. 1999, 8, 3–15. [Google Scholar] [CrossRef]
- Bennett, D.A. How can I deal with missing data in my study? Aust. N. Z. J. Public Heal. 2001, 25, 464–469. [Google Scholar] [CrossRef]
- Cheung, M.W. Comparison of Approaches to Constructing Confidence Intervals for Mediating Effects Using Structural Equation Models. Struct. Equ. Model. A Multidiscip. J. 2007, 14, 227–246. [Google Scholar] [CrossRef]
- MacKinnon, D.P.; Lockwood, C.M.; Williams, J. Confidence Limits for the Indirect Effect: Distribution of the Product and Resampling Methods. Multivar. Behav. Res. 2004, 39, 99–128. [Google Scholar] [CrossRef] [Green Version]
- MacKinnon, D.P.; Lockwood, C. Distribution of products tests for the mediated effect. 2020; Unpublished manuscript. [Google Scholar]
- Ryu, E. Effects of skewness and kurtosis on normal-theory based maximum likelihood test statistic in multilevel structural equation modeling. Behav. Res. Methods 2011, 43, 1066–1074. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stevens, J.P. Outliers and influential data points in regression analysis. Psychol. Bull. 1984, 95, 334–344. [Google Scholar] [CrossRef]
- Zijlstra, W.P.; Van Der Ark, L.A.; Sijtsma, K. Outliers in Questionnaire Data: Can They Be Detected and Should They Be Removed? J. Educ. Behav. Stat. 2011, 36, 186–212. [Google Scholar] [CrossRef]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. A Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Liew, J.; Eisenberg, N.; Reiser, M. Preschoolers’ effortful control and negative emotionality, immediate reactions to disappointment, and quality of social functioning. J. Exp. Child Psychol. 2004, 89, 298–319. [Google Scholar] [CrossRef]
- Bridgett, D.J.; Oddi, K.B.; Laake, L.M.; Murdock, K.W.; Bachmann, M.N. Integrating and differentiating aspects of self-regulation: Effortful control, executive functioning, and links to negative affectivity. Emotion 2013, 13, 47–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hafstad, G.S.; Abebe, D.S.; Torgersen, L.; von Soest, T. Picky eating in preschool children: The predictive role of the child’s temperament and mother’s negative affectivity. Eat. Behav. 2013, 14, 274–277. [Google Scholar] [CrossRef]
- Carper, J.; Fisher, J.O.; Birch, L. Young girls’ emerging dietary restraint and disinhibition are related to parental control in child feeding. Appetite 2000, 35, 121–129. [Google Scholar] [CrossRef] [Green Version]
- Francis, L.A.; Hofer, S.M.; Birch, L.L. Predictors of maternal child-feeding style: Maternal and child characteristics. Appetite 2001, 37, 231–243. [Google Scholar] [CrossRef]
- Else-Quest, N.M.; Hyde, J.S.; Goldsmith, H.H.; Van Hulle, C.A. Gender differences in temperament: A meta-analysis. Psychol. Bull. 2006, 132, 33–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suglia, S.F.; Duarte, C.S.; Chambers, E.C.; Boynton-Jarrett, R. Cumulative Social Risk and Obesity in Early Childhood. Pediatrics 2012, 129, e1173–e1179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wisniewski, A.B.; Chernausek, S.D. Gender in childhood obesity: Family environment, hormones, and genes. Gend. Med. 2009, 6, 76–85. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A.; E Specter, S. Poverty and obesity: The role of energy density and energy costs. Am. J. Clin. Nutr. 2004, 79, 6–16. [Google Scholar] [CrossRef]
- Bentley, M.E.; Gavin, L.; Black, M.M.; Teti, L. Infant feeding practices of low-income, African-American, adolescent mothers: An ecological, multigenerational perspective. Soc. Sci. Med. 1999, 49, 1085–1100. [Google Scholar] [CrossRef]
- Brown, K.M.; Schreiber, G.B.; McMahon, R.P.; Crawford, P.; Ghee, K.L. Maternal influences on body satisfaction in Black and White girls aged 9 and 10: The NHLBI Growth and Health Study (NGHS). Ann. Behav. Med. 1995, 17, 213–220. [Google Scholar] [CrossRef]
- Tofighi, D.; MacKinnon, D.P. Monte Carlo confidence intervals for complex functions of indirect effects. Struct. Equ. Model. Multidiscip. J. 2016, 23, 194–205. [Google Scholar] [CrossRef]
- Liew, J.; Johnson, A.Y.; Smith, T.R.; Thoemmes, F. Parental Expressivity, Child Physiological and Behavioral Regulation, and Child Adjustment: Testing a Three-Path Mediation Model. Early Educ. Dev. 2011, 22, 549–573. [Google Scholar] [CrossRef]
- Taylor, A.B.; MacKinnon, D.P.; Tein, J.-Y. Tests of the Three-Path Mediated Effect. Organ. Res. Methods 2007, 11, 241–269. [Google Scholar] [CrossRef]
- Birch, L.L. Child Feeding Practices and the Etiology of Obesity. Obesity 2006, 14, 343–344. [Google Scholar] [CrossRef] [Green Version]
- Stifter, C.A.; Moding, K.J. Temperament in obesity-related research: Concepts, challenges, and considerations for future research. Appetite 2019, 141, 104308. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Mean | SD | Skewness | Kurtosis | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Effortful Control | 5.28 | 0.66 | −0.36 | −0.28 | 1 | ||||||||
| 2 | Negative Affectivity | 4.07 | 0.76 | −0.01 | 0.04 | −0.22 ** | 1 | |||||||
| 3 | Food Avoidance | 1.35 | 0.60 | 0.08 | 0.98 | −0.20 ** | 0.07 | 1 | ||||||
| 4 | Food Approach | 2.49 | 0.60 | 0.25 | 0.12 | −0.19 ** | 0.37 ** | −0.01 | 1 | |||||
| 5 | Restrictive Feeding | 3.36 | 0.97 | −0.45 | −0.51 | −0.10 | 0.25 ** | 0.08 | 0.41 ** | 1 | ||||
| 6 | Pressure to Eat | 2.58 | 1.10 | 0.24 | −0.96 | −0.07 | 0.13 | 0.29 ** | 0.10 | 0.14 * | 1 | |||
| 7 | Perceived Child Weight | 2.21 | 1.29 | 0.88 | −0.41 | −0.06 | 0.15 * | −0.01 | 0.28 ** | 0.39 ** | 0.09 | 1 | ||
| 8 | Child BMI | 16.68 | 2.16 | 1.48 | 4.69 | −0.12 | 0.05 | −0.20 ** | 0.10 | 0.16 * | −0.25 ** | 0.34 ** | 1 | |
| 9 | Child Body Fat | 22.29 | 5.73 | 0.09 | 1.98 | −0.10 | 0.05 | −0.18 ** | 0.06 | 0.17 * | −0.21 ** | 0.31 ** | 0.85 ** | 1 |
| Indirect Effect | Estimate | SE | 95% CI | |
|---|---|---|---|---|
| Effortful Control → Child Weight Status | Effortful Control → Food Avoidance → Restrictive Feeding → Child Weight Status | −0.01 | 0.01 | (−0.04, 0.001) |
| Effortful Control → Food Approach → Restrictive Feeding → Child Weight Status | −0.03 | 0.02 | (−0.09, −0.01) | |
| Effortful Control → Food Avoidance → Pressure to Eat → Child Weight Status | 0.06 * | 0.02 | (0.01, 0.13) | |
| Effortful Control → Food Approach → Pressure to Eat → Child Weight Status | 0.01 | 0.01 | (−0.001, 0.05) | |
| Negative Affectivity → Child Weight Status | Negative Affectivity → Food Avoidance → Restrictive Feeding → Child Weight Status | 0.001 | 0.003 | (−0.004, 0.015) |
| Negative Affectivity → Food Approach → Restrictive Feeding → Child Weight Status | 0.09 * | 0.03 | (0.03, 0.17) | |
| Negative Affectivity → Food Avoidance → Pressure to Eat → Child Weight Status | −0.01 | 0.02 | (−0.05, 0.03) | |
| Negative Affectivity → Food Approach → Pressure to Eat → Child Weight Status | −0.03 | 0.02 | (−0.08, 0.01) | |
| Effortful Control → Perceived Child Weight | Effortful Control → Food Avoidance → Restrictive Feeding → Perceived Child Weight | −0.01 | 0.01 | (−0.04, 0.002) |
| Effortful Control → Food Approach → Restrictive Feeding → Perceived Child Weight | −0.04 | 0.02 | (−0.09, −0.001) | |
| Effortful Control → Food Avoidance → Pressure to Eat → Perceived Child Weight | −0.004 | 0.01 | (−0.02, 0.01) | |
| Effortful Control → Food Approach → Pressure to Eat → Perceived Child Weight | −0.001 | 0.002 | (−0.01, 0.001) | |
| Negative Affectivity → Perceived Child Weight | Negative Affectivity → Food Avoidance → Restrictive Feeding → Perceived Child Weight | 0.001 | 0.004 | (−0.005, 0.02) |
| Negative Affectivity → Food Approach → Restrictive Feeding → Perceived Child Weight | 0.1 ** | 0.03 | (0.05, 0.16) | |
| Negative Affectivity → Food Avoidance → Pressure to Eat → Perceived Child Weight | 0 | 0.001 | (−0.003, 0.01) | |
| Negative Affectivity → Food Approach → Pressure to Eat → Perceived Child Weight | 0.002 | 0.004 | (−0.004, 0.02) |
| Above the Poverty Line (n = 138) | Below the Poverty Line (n = 81) | |||||
|---|---|---|---|---|---|---|
| Mean | SE | Mean | SE | F | p | |
| Effortful Control | 5.31 | 0.06 | 5.24 | 0.07 | 0.51 | 0.47 |
| Negative Affectivity | 3.96 | 0.06 | 4.21 | 0.08 | 5.88 | 0.02 |
| Food Avoidance | 1.41 | 0.05 | 1.26 | 0.07 | 3.24 | 0.07 |
| Food Approach | 2.49 | 0.04 | 2.45 | 0.08 | 0.19 | 0.67 |
| Restrictive Feeding | 3.41 | 0.08 | 3.27 | 0.11 | 0.99 | 0.32 |
| Pressure to Eat | 2.43 | 0.09 | 2.84 | 0.13 | 7.43 | 0.01 |
| Perceived Child Weight | 2.01 | 0.11 | 2.49 | 0.15 | 7.07 | 0.01 |
| Child BMI | 16.31 | 0.16 | 17.37 | 0.30 | 11.64 | <0.01 |
| Child Body Fat | 21.58 | 0.41 | 23.68 | 0.84 | 6.41 | 0.01 |
| White Non-Hispanic (n = 106) | White Hispanic (n = 63) | Black (n = 51) | ||||||
|---|---|---|---|---|---|---|---|---|
| Mean | SE | Mean | SE | Mean | SE | F | p | |
| Effortful Control | 5.28 | 0.06 | 5.38 | 0.08 | 5.20 | 0.10 | 1.06 | 0.35 |
| Negative Affectivity | 4.04 | 0.06 | 4.02 | 0.11 | 4.19 | 0.12 | 0.84 | 0.43 |
| Food Avoidance | 1.46 | 0.06 | 1.38 | 0.07 | 1.14 | 0.07 | 4.99 | 0.01 |
| Food Approach | 2.53 | 0.05 | 2.46 | 0.08 | 2.43 | 0.10 | 0.62 | 0.54 |
| Restrictive Feeding | 3.33 | 0.09 | 3.36 | 0.15 | 3.44 | 0.11 | 0.23 | 0.80 |
| Pressure to Eat | 2.29 | 0.10 | 2.72 | 0.13 | 3.04 | 0.16 | 9.22 | <0.01 |
| Perceived Child Weight | 1.90 | 0.11 | 2.58 | 0.18 | 2.31 | 0.18 | 6.17 | <0.01 |
| Child BMI | 16.30 | 0.17 | 16.83 | 0.29 | 17.17 | 0.38 | 3.13 | 0.05 |
| Child Body Fat | 21.33 | 0.49 | 22.95 | 0.83 | 23.14 | 0.88 | 2.42 | 0.09 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liew, J.; Zhou, Z.; Perez, M.; Yoon, M.; Kim, M. Parental Child-Feeding in the Context of Child Temperament and Appetitive Traits: Evidence for a Biopsychosocial Process Model of Appetite Self-Regulation and Weight Status. Nutrients 2020, 12, 3353. https://doi.org/10.3390/nu12113353
Liew J, Zhou Z, Perez M, Yoon M, Kim M. Parental Child-Feeding in the Context of Child Temperament and Appetitive Traits: Evidence for a Biopsychosocial Process Model of Appetite Self-Regulation and Weight Status. Nutrients. 2020; 12(11):3353. https://doi.org/10.3390/nu12113353
Chicago/Turabian StyleLiew, Jeffrey, Zhiqing Zhou, Marisol Perez, Myeongsun Yoon, and Mirim Kim. 2020. "Parental Child-Feeding in the Context of Child Temperament and Appetitive Traits: Evidence for a Biopsychosocial Process Model of Appetite Self-Regulation and Weight Status" Nutrients 12, no. 11: 3353. https://doi.org/10.3390/nu12113353