Longitudinal Associations between Emotion Regulation and Adiposity in Late Adolescence: Indirect Effects through Eating Behaviors

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Procedures and Measures
2.2.1. Emotion Regulation
2.2.2. Emotional Eating and Dietary Restraint
2.2.3. Adiposity
2.2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Skinner, A.C.; Ravanbakht, S.N.; Skelton, J.A.; Perrin, E.M.; Armstrong, S.C. Prevalence of Obesity and Severe Obesity in US Children, 1999–2016. Pediatrics 2018, 141, e20173459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alpert, M.A.; Lavie, C.J.; Agrawal, H.; Kumar, A.; Kumar, S.A. Cardiac Effects of Obesity: Pathophysiologic, Clinical, and Prognostic Consequences—A Review. J. Cardiopulm. Rehabil. Prev. 2016, 36, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Sahoo, K.; Sahoo, B.; Kumar Choudhury, A.; Sofi, N.Y.; Kumar, R.; Bhadoria, A.S. Childhood Obesity: Causes and Consequences. J. Fam. Med. Prim. Care 2015, 4, 187. [Google Scholar] [CrossRef]
- Hill, J.O.; Wyatt, H.R.; Peters, J.C. Energy Balance and Obesity. Circulation 2012. [Google Scholar] [CrossRef] [PubMed]
- Romieu, I.; Dossus, L.; Barquera, S.; Blottière, H.M.; Franks, P.W.; Gunter, M.; Hwalla, N.; Hursting, S.D.; Leitzmann, M.; Margetts, B.; et al. Energy Balance and Obesity: What Are the Main Drivers? Cancer Causes Control. 2017, 28, 247–258. [Google Scholar] [CrossRef] [PubMed]
- Lutter, M.; Nestler, E.J. Homeostatic and Hedonic Signals Interact in the Regulation of Food Intake. J. Nutr. 2009, 139, 629–632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stuckler, D.; McKee, M.; Ebrahim, S.; Basu, S. Manufacturing Epidemics: The Role of Global Producers in Increased Consumption of Unhealthy Commodities Including Processed Foods, Alcohol, and Tobacco. PLoS Med. 2012, 9, e1001235. [Google Scholar] [CrossRef] [PubMed]
- Swinburn, B.; Egger, G.; Raza, F. Dissecting Obesogenic Environments: The Development and Application of a Framework for Identifying and Prioritizing Environmental Interventions for Obesity. Prev. Med. 1999, 59, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.L.; Gearhardt, A.N.; Fredericks, E.M.; Katz, B.; Shapiro, L.F.; Holden, K.; Kaciroti, N.; Gonzalez, R.; Hunter, C.; Lumeng, J.C. Targeting Self-Regulation to Promote Health Behaviors in Children. Behav. Res. Ther. 2018, 101, 71–81. [Google Scholar] [CrossRef] [PubMed]
- Schlam, T.R.; Wilson, N.L.; Shoda, Y.; Mischel, W.; Ayduk, O. Preschoolers’ Delay of Gratification Predicts Their Body Mass 30 Years Later. J. Pediatr. 2013, 162, 90–93. [Google Scholar] [CrossRef] [PubMed]
- Stok, F.M.; De Vet, E.; Wardle, J.; Chu, M.T.; De Wit, J.; De Ridder, D.T.D. Navigating the Obesogenic Environment: How Psychological Sensitivity to the Food Environment and Self-Regulatory Competence Are Associated with Adolescent Unhealthy Snacking. Eat. Behav. 2015, 17, 19–22. [Google Scholar] [CrossRef] [PubMed]
- Calkins, S.D.; Hill, A. Caregiver Influences on Emerging Emotion Regulation: Biological and Environmental Transactions in Early Development. Handb. Emot. Regul. 2007. [Google Scholar] [CrossRef]
- Miller, A.L.; Rosenblum, K.L.; Retzloff, L.B.; Lumeng, J.C. Observed Self-Regulation Is Associated with Weight in Low-Income Toddlers. Appetite 2016, 105, 705–712. [Google Scholar] [CrossRef] [PubMed]
- Power, T.G.; Olivera, Y.A.; Hill, R.A.; Beck, A.D.; Hopwood, V.; Garcia, K.S.; Ramos, G.G.; Fisher, J.O.; O’Connor, T.M.; Hughes, S.O. Emotion Regulation Strategies and Childhood Obesity in High Risk Preschoolers. Appetite 2016, 107, 623–627. [Google Scholar] [CrossRef] [PubMed]
- Kopp, C.B. Regulation of Distress and Negative Emotions: A Developmental View. Dev. Psychol. 1989, 25, 343. [Google Scholar] [CrossRef]
- Mannan, M.; Mamun, A.; Doi, S.; Clavarino, A. Prospective Associations between Depression and Obesity for Adolescent Males and Females- A Systematic Review and Meta-Analysis of Longitudinal Studies. PLoS ONE 2016, 11, e0157240. [Google Scholar] [CrossRef] [PubMed]
- Joormann, J.; Gotlib, I.H. Emotion Regulation in Depression: Relation to Cognitive Inhibition. Cogn. Emot. 2010, 24, 281–298. [Google Scholar] [CrossRef] [PubMed]
- Baños, R.M.; Cebolla, A.; Moragrega, I.; Van Strien, T.; Fernández-Aranda, F.; Agüera, Z.; de la Torre, R.; Casanueva, F.F.; Fernández-Real, J.M.; Fernández-García, J.C.; et al. Relationship between Eating Styles and Temperament in an Anorexia Nervosa, Healthy Control, and Morbid Obesity Female Sample. Appetite 2014, 76, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Van Strien, T.; Konttinen, H.; Homberg, J.R.; Engels, R.C.M.E.; Winkens, L.H.H. Emotional Eating as a Mediator between Depression and Weight Gain. Appetite 2016, 100, 216–224. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders DMS V; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar] [CrossRef]
- Greeno, C.G.; Wing, R.R. Stress-Induced Eating. Psychol. Bull. 1994, 115, 444. [Google Scholar] [CrossRef] [PubMed]
- Devonport, T.J.; Nicholls, W.; Fullerton, C. A Systematic Review of the Association between Emotions and Eating Behaviour in Normal and Overweight Adult Populations. J. Health Psychol. 2017, 24, 3–24. [Google Scholar] [CrossRef] [PubMed]
- Goossens, L.; Braet, C.; Van Vlierberghe, L.; Mels, S. Loss of Control over Eating in Overweight Youngsters: The Role of Anxiety, Depression and Emotional Eating. Eur. Eat. Disord. Rev. 2009, 17, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Katterman, S.N.; Kleinman, B.M.; Hood, M.M.; Nackers, L.M.; Corsica, J.A. Mindfulness Meditation as an Intervention for Binge Eating, Emotional Eating, and Weight Loss: A Systematic Review. Eat. Behav. 2014, 15, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Michels, N.; Sioen, I.; Braet, C.; Eiben, G.; Hebestreit, A.; Huybrechts, I.; Vanaelst, B.; Vyncke, K.; De Henauw, S. Stress, Emotional Eating Behaviour and Dietary Patterns in Children. Appetite 2012, 59, 762–769. [Google Scholar] [CrossRef] [PubMed]
- Nguyen-Michel, S.T.; Unger, J.B.; Spruijt-Metz, D. Dietary Correlates of Emotional Eating in Adolescence. Appetite 2007, 49, 494–499. [Google Scholar] [CrossRef] [PubMed]
- Frayn, M.; Knäuper, B. Emotional Eating and Weight in Adults: A Review. Curr. Psychol. 2018, 37, 924–933. [Google Scholar] [CrossRef]
- Pearson, C.M.; Riley, E.N.; Davis, H.A.; Smith, G.T. Research Review: Two Pathways toward Impulsive Action: An Integrative Risk Model for Bulimic Behavior in Youth. J. Child. Psychol. Psychiatry Allied Discip. 2014, 55, 852–864. [Google Scholar] [CrossRef] [PubMed]
- Stice, E.; Presnell, K.; Spangler, D. Risk Factors for Binge Eating Onset in Adolescent Girls: A 2-Year Prospective Investigation. Health Psychol. 2002, 21, 131. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, J.R.; Woolson, S.L.; Hamer, R.M.; Kalarchian, M.A.; Marcus, M.D.; Bulik, C.M. Evaluating Binge Eating Disorder in Children: Development of the Children’s Binge Eating Disorder Scale (C-BEDS). Int. J. Eat. Disord. 2007, 40, 82–89. [Google Scholar] [CrossRef] [PubMed]
- French, S.A.; Epstein, L.H.; Jeffery, R.W.; Blundell, J.E.; Wardle, J. Eating Behavior Dimensions. Associations with Energy Intake and Body Weight. A Review. Appetite 2012, 59, 541–549. [Google Scholar] [CrossRef] [PubMed]
- Polivy, J.; Herman, C.P. Clinical Depression and Weight Change: A Complex Relation. J. Abnorm. Psychol. 1976, 85, 338. [Google Scholar] [CrossRef] [PubMed]
- Schaumberg, K.; Anderson, D.A.; Anderson, L.M.; Reilly, E.E.; Gorrell, S. Dietary Restraint: What’s the Harm? A Review of the Relationship between Dietary Restraint, Weight Trajectory and the Development of Eating Pathology. Clin. Obes. 2016, 6, 89–100. [Google Scholar] [CrossRef] [PubMed]
- Van Strien, T.; Herman, C.P.; Verheijden, M.W. Dietary Restraint and Body Mass Change. A 3-Year Follow up Study in a Representative Dutch Sample. Appetite 2014, 76, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Anderson, L.M.; Reilly, E.E.; Schaumberg, K.; Dmochowski, S.; Anderson, D.A. Contributions of Mindful Eating, Intuitive Eating, and Restraint to BMI, Disordered Eating, and Meal Consumption in College Students. Eat. Weight Disord. 2016, 21, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Banna, J.C.; Panizza, C.E.; Boushey, C.J.; Delp, E.J.; Lim, E. Association between Cognitive Restraint, Uncontrolled Eating, Emotional Eating and BMI and the Amount of Food Wasted in Early Adolescent Girls. Nutrients 2018, 10, 1279. [Google Scholar] [CrossRef] [PubMed]
- Schembre, S.M.; Albright, C.L.; Lim, U.; Wilkens, L.R.; Murphy, S.P.; Novotny, R.; Ernst, T.; Chang, L.; Kolonel, L.N.; Le Marchand, L. Associations between Weight-Related Eating Behaviors and Adiposity in Postmenopausal Japanese American and White Women. Physiol. Behav. 2012, 106, 651–656. [Google Scholar] [CrossRef] [PubMed]
- Delinsky, S.S.; Wilson, G.T. Weight Gain, Dietary Restraint, and Disordered Eating in the Freshman Year of College. Eat. Behav. 2008, 9, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Johnson, F.; Pratt, M.; Wardle, J. Dietary Restraint and Self-Regulation in Eating Behavior. Int. J. Obes. 2012, 36, 665. [Google Scholar] [CrossRef] [PubMed]
- Evers, C.; Stok, F.; de Ridder, D.T.D. Feeding Your Feelings: Emotion Regulation Strategies and Emotional Eating. Personal. Soc. Psychol. Bull. 2010, 36, 792–804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gianini, L.M.; White, M.A.; Masheb, R.M. Eating Pathology, Emotion Regulation, and Emotional Overeating in Obese Adults with Binge Eating Disorder. Eat. Behav. 2013, 14, 309–313. [Google Scholar] [CrossRef] [PubMed]
- Harrist, A.W.; Hubbs-Tait, L.; Topham, G.L.; Shriver, L.H.; Page, M.C. Emotion Regulation Is Related to Children’s Emotional and External Eating. J. Dev. Behav. Pediatr. 2013, 34, 557–565. [Google Scholar] [CrossRef] [PubMed]
- Lu, Q.; Tao, F.; Hou, F.; Zhang, Z.; Ren, L.L. Emotion Regulation, Emotional Eating and the Energy-Rich Dietary Pattern. A Population-Based Study in Chinese Adolescents. Appetite 2016, 99, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Svaldi, J.; Tuschen-Caffier, B.; Lackner, H.K.; Zimmermann, S.; Naumann, E. The Effects of Emotion Regulation on the Desire to Overeat in Restrained Eaters. Appetite 2012, 59, 256–263. [Google Scholar] [CrossRef] [PubMed]
- Mellendick, K.; Shanahan, L.; Wideman, L.; Calkins, S.; Keane, S.; Lovelady, C. Diets Rich in Fruits and Vegetables Are Associated with Lower Cardiovascular Disease Risk in Adolescents. Nutrients 2018, 10, 136. [Google Scholar] [CrossRef] [PubMed]
- Anzman-Frasca, S.; Stifter, C.A.; Birch, L.L. Temperament and Childhood Obesity Risk: A Review of the Literature. J. Dev. Behav. Pediatr. 2012, 33, 732–745. [Google Scholar] [CrossRef] [PubMed]
- Boswell, N.; Byrne, R.; Davies, P.S.W. Aetiology of Eating Behaviours: A Possible Mechanism to Understand Obesity Development in Early Childhood. Neurosci. Biobehav. Rev. 2018, 95, 438–448. [Google Scholar] [CrossRef] [PubMed]
- Isasi, C.R.; Ostrovsky, N.W.; Wills, T.A. The Association of Emotion Regulation with Lifestyle Behaviors in Inner-City Adolescents. Eat. Behav. 2013, 14, 518–521. [Google Scholar] [CrossRef] [PubMed]
- Calkins, S.D.; Fox, N.A. Self-Regulatory Processes in Early Personality Development: A Multilevel Approach to the Study of Childhood Social Withdrawal and Aggression. Dev. Psychopathol. 2002, 14, 477–498. [Google Scholar] [CrossRef] [PubMed]
- Wideman, L.; Calkins, S.D.; Janssen, J.A.; Lovelady, C.A.; Dollar, J.M.; Keane, S.P.; Perrin, E.M.; Shanahan, L. Rationale, Design and Methods for the RIGHT Track Health Study: Pathways from Childhood Self-Regulation to Cardiovascular Risk in Adolescence. BMC Public Health 2016, 16, 459. [Google Scholar] [CrossRef] [PubMed]
- MacDermott, S.T.; Gullone, E.; Allen, J.S.; King, N.J.; Tonge, B. The Emotion Regulation Index for Children and Adolescents (ERICA): A Psychometric Investigation. J. Psychopathol. Behav. Assess. 2010, 32, 301–314. [Google Scholar] [CrossRef]
- Shields, A.; Cicchetti, D. Emotion Regulation among School-Age Children: The Development and Validation of a New Criterion Q-Sort Scale. Dev. Psychol. 1997, 33, 906. [Google Scholar] [CrossRef] [PubMed]
- Stunkard, A.J.; Messick, S. The Three-Factor Eating Questionnaire to Measure Dietary Restraint, Disinhibition and Hunger. J. Psychosom. Res. 1985, 29, 71–83. [Google Scholar] [CrossRef]
- Bond, M.J.; McDowell, A.J.; Wilkinson, J.Y. The Measurement of Dietary Restraint, Disinhibition and Hunger: An Examination of the Factor Structure of the Three Factor Eating Questionnaire (TFEQ). Int. J. Obes. 2001, 25, 900. [Google Scholar] [CrossRef] [PubMed]
- Okorodudu, D.O.; Jumean, M.F.; Montori, V.M.; Romero-Corral, A.; Somers, V.K.; Erwin, P.J.; Lopez-Jimenez, F. Diagnostic Performance of Body Mass Index to Identify Obesity as Defined by Body Adiposity: A Systematic Review and Meta-Analysis. Int. J. Obes. 2010, 34, 791. [Google Scholar] [CrossRef] [PubMed]
- Fields, D.A.; Goran, M.I.; McCrory, M.A. Body-Composition Assessment via Air-Displacement Plethysmography in Adults and Children: A Review. Am. J. Clin. Nutr. 2002, 75, 453–467. [Google Scholar] [CrossRef] [PubMed]
- Kuczmarski, R.R.J.; Ogden, C.L.C.; Guo, S.S.; Grummer-Strawn, L.M.; Flegal, K.M.; Mei, Z.; Wei, R.; Curtin, L.R.; Roche, A.F.; Johnson, C.L. 2000 CDC Growth Charts for the United States: Methods and Development. Vital Health Stat. 11 2002, 11, 1–201. [Google Scholar]
- Muthén, L.; Muthén, B. Mplus Version 7 User’s Guide; Muthén & Muthén: Los Angeles, CA, USA, 2012. [Google Scholar] [CrossRef]
- Marsh, H.W.; Hau, K.T. Applications of Latent-Variable Models in Educational Psychology: The Need for Methodological-Substantive Synergies. Contemp. Educ. Psychol. 2007, 32, 151–170. [Google Scholar] [CrossRef]
- Bentler, P.M. Comparative Fit Indexes in Structural Models. Psychol. Bull. 1990, 107, 238. [Google Scholar] [CrossRef] [PubMed]
- Cole, D.A.; Maxwell, S.E. Testing Mediational Models with Longitudinal Data: Questions and Tips in the Use of Structural Equation Modeling. J. Abnorm. Psychol. 2003, 112, 558. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.T.; Bentler, P.M. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria versus New Alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- MacKinnon, D.P.; Lockwood, C.M.; Williams, J. Confidence Limits for the Indirect Effect: Distribution of the Product and Resampling Methods. Multivar. Behav. Res. 2004, 39, 99–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogden, C.L.; Carroll, M.D.; Kit, B.K.; Flegal, K.M. Prevalence of Childhood and Adult Obesity in the United States, 2011–2012. JAMA J. Am. Med. Assoc. 2014, 311, 806–814. [Google Scholar] [CrossRef] [PubMed]
- Bleich, S.N.; Segal, J.; Wu, Y.; Wilson, R.; Wang, Y. Systematic Review of Community-Based Childhood Obesity Prevention Studies. Pediatrics 2013, 132, e201–e210. [Google Scholar] [CrossRef] [PubMed]
- Stice, E.; Shaw, H.; Marti, C.N. A Meta-Analytic Review of Obesity Prevention Programs for Children and Adolescents: The Skinny on Interventions That Work. Psychol. Bull. 2006, 135, 667. [Google Scholar] [CrossRef] [PubMed]
- Herman, C.P.; Mack, D. Restrained and Unrestrained Eating. J. Personal. 1975, 43, 647–660. [Google Scholar] [CrossRef]
- Boutelle, K.N.; Braden, A.; Knatz-Peck, S.; Anderson, L.K.; Rhee, K.E. An Open Trial Targeting Emotional Eating among Adolescents with Overweight or Obesity. Eat. Disord. 2018, 26, 79–91. [Google Scholar] [CrossRef] [PubMed]
- Westenhoefer, J.; Engel, D.; Holst, C.; Lorenz, J.; Peacock, M.; Stubbs, J.; Whybrow, S.; Raats, M. Cognitive and Weight-Related Correlates of Flexible and Rigid Restrained Eating Behaviour. Eat. Behav. 2013, 14, 69–72. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.P.; Bittencourt-Hewitt, A.; Sebastian, C.L. Neurocognitive Bases of Emotion Regulation Development in Adolescence. Dev. Cognit. Neurosci. 2015, 15, 11–25. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Cai, L.; Wu, Y.; Wilson, R.F.; Weston, C.; Fawole, O.; Bleich, S.N.; Cheskin, L.J.; Showell, N.N.; Lau, B.D.; et al. What Childhood Obesity Prevention Programmes Work? A Systematic Review and Meta-Analysis. Obes. Rev. 2015, 16, 547–565. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| 1 | 2 | 3 | 4 | 5 | 6 | |
|---|---|---|---|---|---|---|
| 1. Sex | -- | |||||
| 2. 15-year SES | −0.15 | -- | ||||
| 3. 15-year ER | 0.10 | 0.17 * | -- | |||
| 4. 16-year Dietary Restraint | 0.28 ** | 0.03 | 0.17 * | -- | ||
| 5. 16-year Emotional Eating | 0.06 | 0.05 | −0.30 ** | 0.17 ** | -- | |
| 6. 19-year Percent Body Fat | 0.55 *** | −0.16 | 0.03 | 0.33 ** | 0.28 ** | -- |
| Mean | 1.55 | 45.61 | 3.94 | 0.34 | 0.50 | 26.12 |
| Minimum | 1.00 | 13.00 | 2.56 | 0.05 | 0.00 | 2.80 |
| Maximum | 2.00 | 66.00 | 4.89 | 0.90 | 3.00 | 52.80 |
| Standard Deviation | 0.50 | 13.03 | 0.44 | 0.20 | 0.96 | 11.97 |
| Confidence Intervals | ||||
|---|---|---|---|---|
| Estimate | SE | Lower | Upper | |
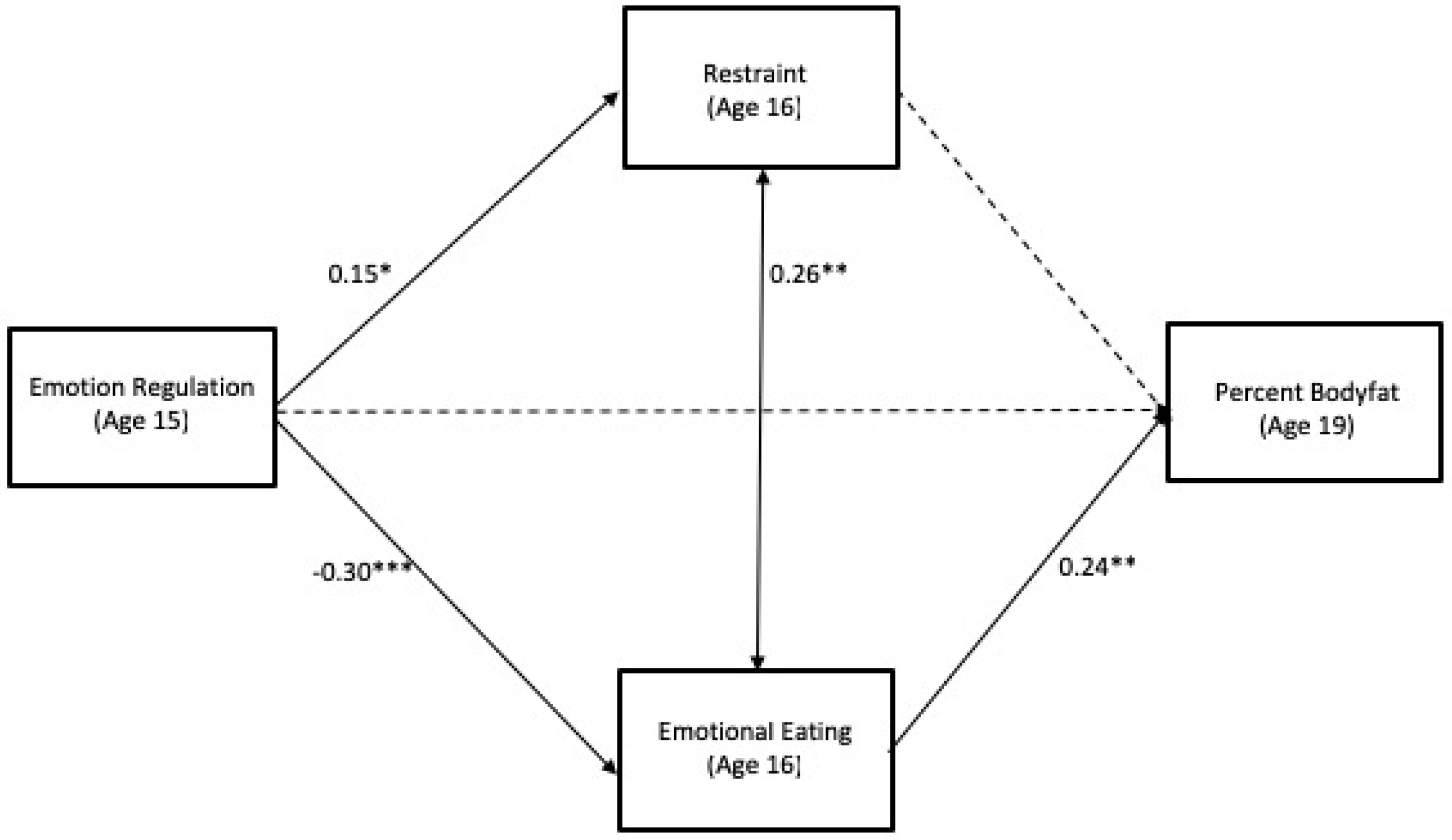
| ER(15yr) → Dietary Restraint(16yr) → Percent Body Fat(19yr) | 0.55 | 0.46 | −0.14 | 2.55 |
| ER(15yr) → Emotional Eating(16yr) → Percent Body Fat(19yr) | −1.97 * | 0.90 | −4.67 | −0.27 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shriver, L.H.; Dollar, J.M.; Lawless, M.; Calkins, S.D.; Keane, S.P.; Shanahan, L.; Wideman, L. Longitudinal Associations between Emotion Regulation and Adiposity in Late Adolescence: Indirect Effects through Eating Behaviors. Nutrients 2019, 11, 517. https://doi.org/10.3390/nu11030517
Shriver LH, Dollar JM, Lawless M, Calkins SD, Keane SP, Shanahan L, Wideman L. Longitudinal Associations between Emotion Regulation and Adiposity in Late Adolescence: Indirect Effects through Eating Behaviors. Nutrients. 2019; 11(3):517. https://doi.org/10.3390/nu11030517
Chicago/Turabian StyleShriver, Lenka H., Jessica M. Dollar, Meg Lawless, Susan D. Calkins, Susan P. Keane, Lilly Shanahan, and Laurie Wideman. 2019. "Longitudinal Associations between Emotion Regulation and Adiposity in Late Adolescence: Indirect Effects through Eating Behaviors" Nutrients 11, no. 3: 517. https://doi.org/10.3390/nu11030517