The Role of Gut Microbiota in Gastrointestinal Symptoms of Children with ASD


1
Department of Developmental Psychology and Didactics, University of Alicante, 03080 Alicante, Spain
2
Department of Agricultural Chemistry, Faculty of Chemistry, University of Murcia, Campus of Espinardo, 30100 Murcia, Spain
3
Department of Chemical Engineering, Faculty of Chemistry, University of Murcia, Campus of Espinardo, 30100 Murcia, Spain
*
Author to whom correspondence should be addressed.
Medicina 2019, 55(8), 408; https://doi.org/10.3390/medicina55080408
Submission received: 27 June 2019
/
Revised: 23 July 2019
/
Accepted: 24 July 2019
/
Published: 26 July 2019
(This article belongs to the Special Issue Autism Spectrum Disorder in Children with Complex Presentations)
Abstract
:Background and objectives: Autism spectrum disorder (ASD) is a neurodevelopmental disorder characterized by impaired communication, social interaction disorder, and repetitive behavior. Dysbiotic gut microbiota (GM) could be a contributing factor to the appearance of ASD, as gastrointestinal (GI) symptoms are comorbidities frequently reported in ASD. As there is a lack of reviews about the role played by GM in the GI symptoms of ASD, this work aimed to carry out a systematic review of current studies comparing the GM of children with ASD and GI symptoms with those of healthy controls in the last six years. Materials and Methods: The systematic review was performed following the PRISMA guidelines. The databases chosen were Web of Science, Scopus, PubMed, and PsycINFO, and the keywords were (gut* OR intestine* OR bowel* OR gastrointestinal*) AND (microbiota* OR microflora* OR bacteria* OR microbiome* OR flora* OR bacterial* OR bacteria* OR microorganism* OR feces* OR stool*) AND (autistic* OR autism* OR ASD*). Results: A total of 16 articles were included. Ten articles performed correlations analysis between GI symptoms and ASD. Among those 10 articles, 7 found differences between the GI symptoms present in children with ASD and healthy controls. The most common GI symptom was constipation. Among the seven articles that found differences, three performed correlations analysis between GI symptoms and gut microbe abundance. Candida, Prevotella, Streptococcus, and Veillonella showed higher and lower abundance, respectively, in children with ASD and GI symptoms in more than one article. Bacteroidetes, Firmicutes, Actinomyces, Dorea, Lactobacillus, Faecalibacterium prausnitzii, and Bacteroidetes/Firmicutes ratios showed abundance discrepancies. Conclusions: It is still too early to draw a conclusion about the gut microbes involved in GI symptoms of ASD. Future research should consider the relationship between ASD behavior, GM, and GI symptoms in a multidisciplinary way and homogenize sample characteristics.
1. Introduction
Autism or autism spectrum disorder (ASD) is defined in the Diagnostic and Statistical Manual for Mental Disorders (Fifth Edition (DSM-5)) as a heterogeneous group of neurodevelopmental disorders featuring the three main characteristics of impaired communication, social interaction disorder, and repetitive behavior [1]. Autism includes Kanner’s autism [2], Asperger’s syndrome [3], and pervasive developmental disorder not otherwise specified (PDD-NOS), and is characterized by persistent deficits in social communication interaction and restricted–repetitive patterns of behavior, interests, or activities [1]. It is worth mentioning that people without neurological, medical, or psychiatric diagnoses are defined as neurotypical in the autism community [4].
Autism originally affected one in 10,000 in the 1950s, but now affects one in every 58 people in USA and around one in 30 in Korea, being more prevalent in men (4:1) [5], and possibly in recent immigrant populations (i.e., Somali expatriates in Sweden [6]), suggesting some link with industrialization. In this sense, there is a need for the scientific community to discover the root causes of ASD and the complex interactions between genetic, epigenetic, immunological, neurological, and environmental factors that might be contributing to the development and expression of ASD in sensitive populations [5,7].
People with ASD develop several comorbidities, including gut-related comorbidities such as gastrointestinal (GI) symptoms, increased permeability of the epithelial barrier in the gut, decreased expression of brush border disaccharidases in the gut epithelium, and altered gut microbiota (GM) composition; brain-related comorbidities such as altered expression of tight junction proteins in the blood–brain barrier and increased amounts of activated microglial cells; and other comorbidities such as mitochondrial dysfunction, fragile X syndrome, Rett syndrome, and tuberous sclerosis, and altered metabolite profiles in urine and blood [8].
Among the comorbidities developed by people with ASD, GI symptoms such as diarrhea, constipation, commutative diarrhea/constipation, abdominal pain, vomiting, reflux, or bloating are quite common, and they are correlated with the severity of the neurobehavioral disorder [9]. In this sense, people with ASD with GI symptoms exhibit more anxiety problems and other somatic complaints, together with less social interaction than ASD people without GI symptoms [8]. For example, Marler et al. [10] reported that constipation was found to be the most common GI symptom in ASD people, and that there is a connection between rigid–compulsive behavior and the occurrence of constipation. In addition, people with ASD and GI problems also show more tantrums, aggressive behavior, self-injury, and sleep disturbances, which might be an expression of abdominal discomfort [8].
The etiology of GI symptoms in ASD remains unknown, and everything seems to indicate that it is a combination of associated factors [9,11]. However, GI symptoms appear to be due, in part, to dysbiotic GM. In this sense, there is enough scientific evidence regarding the relationship between a dysbiotic GM and the development of diverse chronic diseases such as asthma, intestinal inflammation associated with the pathogenesis of obesity, type 2 diabetes mellitus [12], and other neurodevelopmental disorders [13].
The GM encompasses the set of bacteria that inhabit the (GI) tract. These bacteria have a dynamic symbiotic relationship that is both commensal and mutual throughout the host lifecycle [14]. At present, the microbiota–gut–brain axis is an explanatory model that attempts to relate the symptoms of ASD to the findings in neuroscience and bacteriology; it is defined as a bidirectional communication system between the neuronal, immune, endocrine, and metabolic pathways, but still requires a better understanding [15].
As discussed before, as GI symptoms can be related to dysbiotic GM, the use of pre/probiotics and microbiota transfer therapy (MTT) as therapeutic tools to treat people with ASD have been gaining greater interest in recent years, as they may help to restore normal GM, reduce inflammation, restore epithelial barrier function, and possibly improve some behavioral symptoms associated with ASD [16,17,18]. For example, Shaaban et al. [19] observed beneficial effects on both behavioral and GI manifestations in Egyptian ASD children with GI symptoms after administering Lactobacillus acidophilus, Lactobacillus rhamnosus, and Bifidobacteria longum, and Kang et al. [18] reported improvements in the microbiome and both GI and ASD symptoms in American ASD children with GI symptoms after MTT. These improvements were sustained at least 8 weeks after treatment. In addition, it has been reported that diet also has a strong correlation with GI symptoms in children with ASD [20], and GM appears to be affected by diet and has a modulatory role in several disease states. For example, besides pre/probiotics, dietary polyphenols, which are often indigestible, may also positively influence GM [21]. In one case, Sprague Dawley rats with hepatic steatosis who were administered a high-fat diet were later given curcumin, which not only restored intestinal barrier integrity (increasing the expression of tight junction proteins ZO-1 and occluding), but also markedly altered the overall composition of the GM towards that of lean rats maintained on a normal diet [22]. Of note, a strong correlation between GI symptoms and diet problems in ASD children, especially idiosyncratic feeding behavior, has been also reported, and ASD children suffering from multiple GI symptoms tend to be those who also have dietary problems [23].
Traditionally, characterization of GM has been carried out using culture-dependent techniques. One of the great limitations of these techniques is that it is impossible to ensure that the phenotypic behavior of a microorganism in the laboratory is identical to its behavior in vivo, due in part to the processes of metabolic symbiosis between microorganisms. In addition, the number of microorganisms that can be characterized with this technique is limited [24]. However, the emergence and rapid development of culture-independent or molecular techniques has made culture-dependent techniques nearly obsolete, and the characterization of GM is currently largely carried out using culture-independent techniques, as they allow scientists to easily identify a large proportion of bacterial diversity and provide rapid results [25,26]. This has led to many studies that compare the diversity of the GM of ASD children with healthy controls [27,28,29,30,31], of which a bibliographic review can be carried out. In this sense, several bibliographic reviews about GM and ASD can be found in the scientific literature. For example, Hughes et al. [32] and Liu et al. [33] studied the dysbiosis of GM in ASD, and Andreo-Martínez et al. [34] studied the gut microbes belonging to the Fungi kingdom in people with ASD. In addition, there have been few studies that have analyzed the correlation between GM composition and GI symptoms in people with ASD. For example, in a meta-analysis about GI symptoms in ASD [9], performed on studies published until 2012, there was only one study [35] which reported that GI symptoms in people with ASD were correlated with high levels of Clostridium (p = 0.001). However, to the author’s best knowledge, there have been no bibliographic reviews that have attempted to relate the gut microbes involved in the GI symptoms of people with ASD. Therefore, the aim of the present work was to carry out a systematic review on the studies that have compared the GM of people with ASD and GI symptoms with those of healthy controls, continuing the meta-analysis line of McElhanon, McCracken, Karpen, and Sharp [9], during the last six years, to try to find some bacterial abundance patterns and to identify future research strategies.
2. Materials and Methods
The design of the present systematic review was performed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [36]. This systematic approach under the PRISMA perspective covers the developments in the field of the GM of people with ASD and GI symptoms by providing critical analysis of key parameters, such as the role that gut microbes play in the GI symptoms of people with ASD, and gut microbe abundance of people with ASD with GI symptoms.
The bibliographic search was performed for works published between 2012 and February 2019, and the four comprehensive databases chosen to carry out the bibliographic search were: Web of Science, Scopus, PubMed, and PsycINFO. The Boolean strings entered to carry out the search were: (gut* OR intestine* OR bowel* OR gastrointestinal*) AND (microbiota* OR microflora* OR bacteria* OR microbiome* OR flora* OR bacterial* OR bacteria* OR microorganism* OR feces* OR stool*) AND (autistic* OR autism* OR ASD*), and the searches included works published in all language. Scopus search options were: title, abstract, and keywords; Web of Science search option was “theme,” while for PsycINFO and PubMed, the search option selected was all fields.
The inclusion criteria were: (1) articles with human populations; (2) articles published from 2012 to February 2019; and (3) articles comparing the GM of children with ASD and GI symptoms with those of control groups. The exclusion criteria were: (1) descriptive and systematic reviews; (2) books and book chapters; (3) editorial material, letters to the editor, shorts reports, and proceedings of conferences; (4) animal model and in vitro articles; (5) other diseases; (6) articles studying only metabolites in blood, plasma, or urine; and (7) articles published in a language other than English.
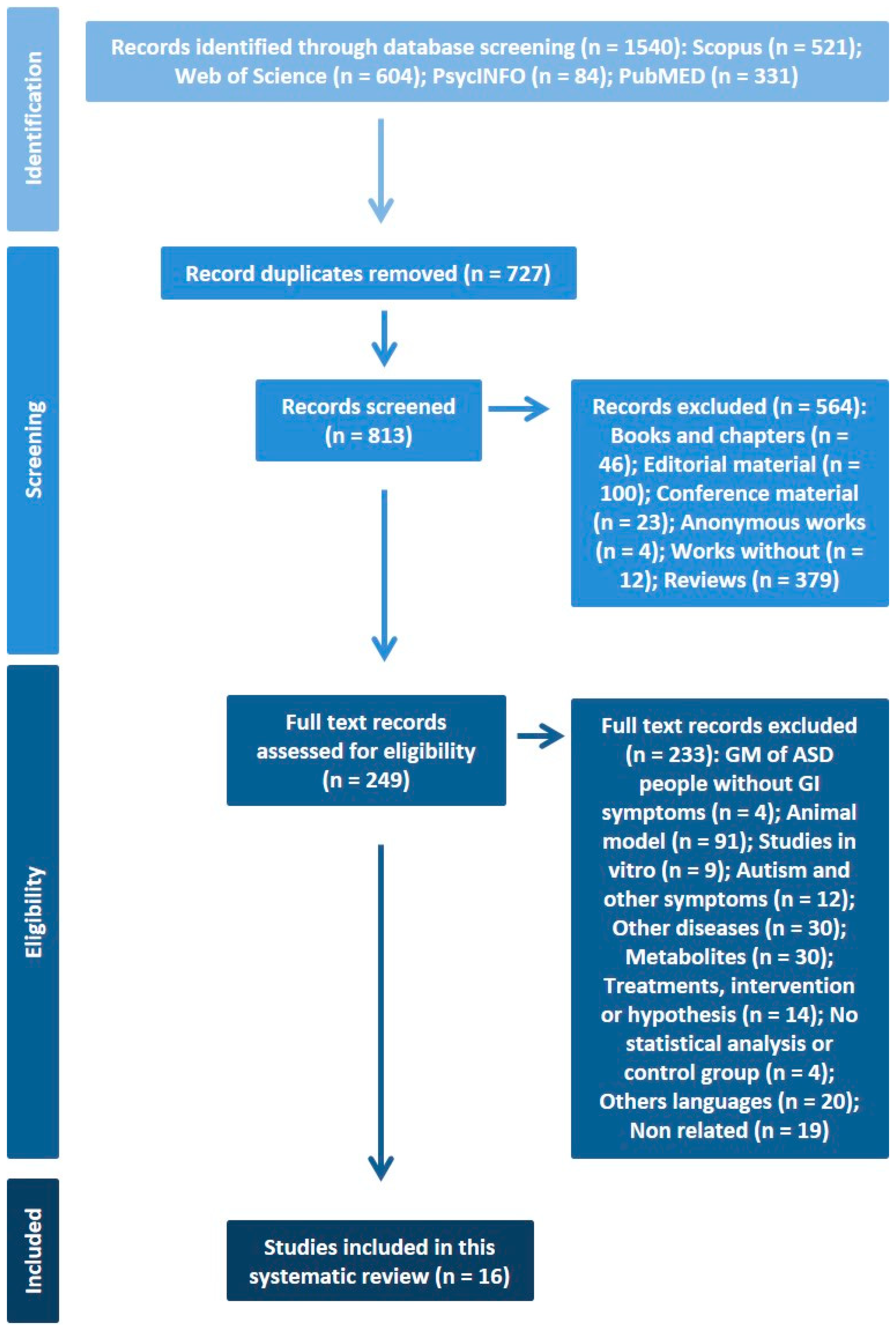
The 1540 works obtained by the four databases were passed through EndNote X7 software (Thomson Reuters, New York, USA) to delete possible duplicated works. According to the PRISMA methodology, A.E.M.-G. and P.A.-M. formed the review team and independently screened titles, abstracts, and full texts of the works for potential inclusion. These two authors evaluated them according to the inclusion or exclusion criteria, and disagreements on whether a given reference should be included or not were resolved through discussion. In addition, the reference lists of the selected works were also examined in search of potentially relevant papers, not finding any additional article in this step. It is noteworthy that some of the works could be included in more than one elimination group, but the final criteria were agreed by the review team. Finally, a total of 16 articles were found to be eligible for the present systematic review and they are shown in Table 1. The risk of bias for each included study was evaluated using the Methods Guide for Comparative Effectiveness Reviews [37]. The forms of bias considered are presented in Table 2.
Figure 1 shows the process of identifying articles for inclusion in the present systematic review.
3. Results
Table 1 shows the sixteen studies included in the present systematic review and the results of the analysis of the samples in children with ASD and GI symptoms.
3.1. Assessment of Risk of Bias for Each Included Article
The 16 articles were identified and assessed as medium to high quality (Table 2). When assessing the quality of selection, the studies presented some limitations in terms of sample size, information on comorbidity of neurodevelopmental disorders, diet of study participants, blinding of participants and personnel, and mean scores and standard deviations in the analysis of study data. Many of these studies were also open-label trials and relied on qualitative, self-reported questionnaires and surveys to gauge treatment response, inviting potential bias into the studies. There might also be various difficulties experienced by the parents in evaluating these aspects, especially owing to the communication deficits typical of children with ASD. More randomized, controlled studies with a larger study population and the use of clinician scoring may lead to more robust studies and results [17].
3.2. Relationship between GI Symptoms and ASD
Among the 16 articles found in the present systematic review, ten of them performed analysis to try to find correlations between GI symptoms and ASD. Seven articles found statistically significant differences between the occurrence of GI symptoms in children with ASD and healthy controls [28,30,31,42,43,44,48], and three articles found no such differences [27,39,41]. The remaining six articles did not perform statistical analysis to analyze correlations between GI symptoms and ASD [29,38,40,45,46,47].
3.3. Relationship between Gut Microbe Abundance and GI Symptoms in Children with ASD
Three articles tried to find correlations between the GI symptoms of children with ASD and gut microbe abundance [31,42,43]. Two of those articles found correlations between certain gut microbes and GI symptoms, specifically constipation [42,43], and irritable bowel syndrome, functional constipation, aerophagia, and abdominal migraine [43]. In light of those results, some genera of bacteria are involved in constipation, but the results between the studies are not coincident (Table 1). The remain article reported no correlation between Desulfovibrio and GI symptoms [31].
3.4. Gut Microbiota Dysbiosis found in children with ASD and GI Symptoms
Seven articles reported statistically significant differences in the presence of GI symptoms in children with ASD compared to healthy controls [28,30,31,42,43,44,48]. These articles also showed significant differences in the abundance of some gut microbes in children with ASD suffering GI symptoms (Table 1) compared to their respective control groups. The gut microbes that were found by more than one article to show significant differences in abundance are listed below.
Candida was found to be the only gut microbe that showed significantly higher abundance in children with ASD and GI symptoms compared to their control groups by more than one article [30,42].
Lower abundance of Prevotella [27,44], Veillonella [42,48], and Streptococcus [44,48] in children with ASD and GI symptoms compared to their control groups was also found to be statistically significant.
In addition, some gut microbes showed discrepancies at a statistically significant level regarding their abundance in children with ASD and GI symptoms compared to their control groups. Specifically, at phylum level, Bacteroidetes [42,48] and Firmicutes [31,48]; at genus level, Actinomyces [44,48], Dorea [42,43], and Lactobacillus [30,31,42]; and at species level, Faecalibacterium prausnitzii [28,43]. The Bacteroidetes/Firmicutes ratio also showed discrepancies at a statistically significant level regarding their abundance in children with ASD and GI symptoms compared to their control groups [31,42,48].
3.5. Limitations
An important limitation of the studies is the absence of a psychometric analysis of the relationship between the severity of behavioral ASD symptoms with GM abundance and GI symptoms. Similarly, none of the studies indicated whether children with ASD presented a diagnosis of intellectual disability, although cognitive difficulties are a determining factor in the severity of ASD symptoms [49].
On the other hand, the present systematic review has the same limitations as other systematic reviews, such as the databases used, the established inclusion/exclusion criteria, database selection, keywords, or time-frame chosen. In addition, the lack of sufficient articles made it impossible to combine the results into a meta-analysis [9].
4. Discussion
The present systematic review found 16 articles that studied the GM in children with ASD and GI symptoms, and, as discussed before, among the 10 articles that analyzed the correlation between GI symptoms and ASD, 7 of them found significant differences. These results are similar to those reported by Adams et al. [50], who found a strong correlation between the 6-GSI score and the Autism Treatment Evaluation Checklist score (Pearson’s correlation coefficient r = 0.60; p < 0.001). Those results are also in line with a meta-analysis which included 15 articles comparing heterogeneous groups (siblings, ASD and healthy control) [9]. Among the 15 selected articles, 10, 12, 9, and 8 reported general GI concerns (p < 0.0001), diarrhea (p < 0.0001), constipation (p < 0.0001), and abdominal pain (p = 0.016), respectively. In conclusion, there seems to be evidence that there is a greater prevalence of GI symptoms among children with ASD compared with control children.
On the other hand, three studies [31,42,43] analyzed the correlation between gut microbe abundance and GI symptoms in children with ASD and GI symptoms. Although the studies are very promising, there is not yet enough scientific evidence to determine the relationships between gut microbe abundance and GI symptoms in children with ASD, as the gut microbes found to be correlated with GI symptoms in children with ASD were different between the different studies (Table 1). In this sense, the results are very premature, and the number of articles found was very low. Therefore, as discussed before, it was not possible to perform a meta-analysis of the relationships between gut microbes and GI symptoms in children with ASD [9].
Regarding the abundance of some gut microbes in children with ASD and GI symptoms, Candida was found to be more abundant by two studies [30,42], Candida albicans being the most frequently identified species [30]. In fact, it has been reported that a high abundance of Candida albicans can cause lower absorption of carbohydrates and minerals, and can generate higher toxins levels in the GI tract that can contribute to some ASD behaviors [51]. It has been also reported that the immunological responses to Candida in the GI tract can be modulated by some Lactobacillus species [42,52]. In this sense, it is possible that a dysbiotic GM in ASD may lead to a Candida population expansion, as can be observed by the lower abundance of Lactobacillus found in Italian children with ASD and GI symptoms compared to their control group [30]. However, a higher abundance of both Lactobacillus and Candida was also found in Italian children with ASD and GI symptoms compared to their control group [42]. Therefore, these results are not conclusive, and, as can be observed, there is a clear lack of investigation of the whole Fungi kingdom in children with ASD, and little is still known about the role of Candida and other types of fungi in both GI and ASD symptoms [34].
Lower abundances of three gut microbe genera (Prevotella [27,44], Veillonella [42,48], and Streptococcus [44,48]) in children with ASD and GI symptoms were also reported by more than one article included in the present systematic review. Lower abundance of Prevotella may act as an indicator of Westernization, and this fact can also result in an altered immune system [53]. In addition, the presence of Prevotella together with other Bacteroidetes is also associated with colon health, and it has been hypothesized that ASD can be triggered by a dysbiosis where Prevotella decreases and Sutterella increases [54]. In this sense, the lower abundance of Prevotella found in American children with ASD was associated with the presence of ASD symptoms instead of GI symptoms [27]. These authors did not find this association in a later work [28], although they found that GI symptoms were significantly more severe in children with ASD compared to their control group.
Streptococcus, together with Lactobacillus, Bifidobacterium, and Lactococcus, are lactate producing bacteria [48]. It is known that children with ASD show elevated levels of both lactate and GI symptoms [55], suggesting an elevation of glycolysis through the phenomenon of aerobic glycolysis in ASD, since the dysregulation of this balance has been also been proposed as a trigger for ASD [56]. In this sense, as Veillonella is also able to ferment lactate, a lower abundance of Veillonella may also disturb the fermentation of lactate in children with ASD [48]. However, it cannot be stated that the elevated levels of lactate in people with ASD and GI symptoms can be attributed only to the GM, since, as discussed before, there are discrepancies in the abundance of other lactate-producing bacteria, such as Lactobacillus. Regarding the implications of Veillonella in GI symptoms presented by children with ASD, Veillonellaceae, together with Prevotellaceae, Prevotella, and Coprococcus, has been included in a probiotic mixture for treating ASD [57], and it is known that the differences in GM composition (especially in Veillonella) of children with ASD may be a consequence of diet [27,46].
The discrepancies found, at a statistically significant level, in the abundance of Bacteroidetes [42,48] and Firmicutes [31,48] phyla; Actinomyces [44,48], Dorea [42,43], and Lactobacillus [30,31,42] genera; Faecalibacterium prausnitzii species 28,43]; and Bacteroidetes/Firmicutes ratio [31,42,48] can be explained by several factors such as ASD heterology, age of participants, nature of control groups, sample location, small sample sizes, different nationalities, inter-individual differences, or different bacterial identification methods [14,31,53,58]. For example, one study used a culture-dependent method to detect Lactobacillus [30], and it was found to be less abundant in children with ASD and GI symptoms compared to the control group. However, two studies [31,42] that used culture-independent methods found opposite results, and although some authors have postulated that both methods yield similar results [59], culture-independent methods are relatively new and they are still developing [26]. Another study found a higher abundance of Dorea in stool samples of children with ASD and GI symptoms [42], while other studies found opposite results taken from rectum mucosal biopsy samples, and it is known that the place where the sample is taken can be relevant for mammalian physiology [14], as there are differences in microbial composition between stool and the GM [60,61]. This was confirmed in a larger-scale study showing that the populations recovered in the stool seemed to combine bacteria derived from the mucous membrane and the luminal part of the intestine, either adherent or not adherent to transient organic matter [62]. It is assumed that microorganisms seen in the stool reflect the microbiology of the colon, particularly the descending colon and rectum. Finally, it is important to highlight that there are still existing gaps in knowledge regarding the interactions between the microbiome and the host in vivo—and the pathways of metabolites—and how their metabolites influence the microenvironment. Therefore, further mechanistic studies involving "omics" technologies, as adapted from previous studies [63], might help shed light on these questions, and future studies should try to homogenize, as much as possible, the characteristics of the samples to be compared, including the place where the sample is taken from and bacterial detection methods, among others.
5. Conclusions
Although recent scientific literature has provided evidence of the relationship between GI symptoms and ASD, it is still too early to draw a conclusion about the gut microbes involved in GI symptoms of children with ASD, due to the limited number of studies reporting correlations between them. Furthermore, the correlation between certain gut microbes and GI problems do not determine the causality of the symptoms. However, it can be said that children with ASD and GI symptoms show higher abundance of Candida, lower abundance of Prevotella, Veillonella, and Streptococcus, and also show discrepancies in the abundance of other gut microbes due to ASD heterology, age of participants, nature of control groups, sample location, small sample sizes, different nationalities, inter-individual differences, or different bacterial identification methods. In addition, we consider that ASD has a wide phenotypic variability, so future studies should consider the relationship between GM, GI symptoms, and behavior of ASD in a more integral and multidisciplinary way. Finally, we argue that future research should homogenize sample characterization in order to develop a meta-analysis on the GM involved in ASD children with GI symptoms.
Author Contributions
A.E.M.-G. and P.A.-M. contributed equally to conceive, design, carry out, and write the present systematic review, and they approve the final version of the manuscript.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Acknowledgments
The authors would like to acknowledge Seonaid McNabb for her English revision.
Conflicts of Interest
The authors declare no conflict of interest.
References
- American Psychiatric Association (APA). Autism spectrum disorder. In Diagnostic and Statistical Manual of Mental Disorders (DSM-5); American Psychiatric Publishing: Washington, DC, USA, 2013. [Google Scholar]
- Kanner, L. Autistic disturbances of affective contact. Nerv. Child 1943, 2, 217–250. [Google Scholar]
- Asperger, H. Die “Autistischen Psychopathen” im Kindesalter. Eur. Arch. Psychiatry Clin. Neurosci. 1944, 117, 76–136. [Google Scholar] [CrossRef]
- Hamilton, K.; Hoogenhout, M.; Malcolm-Smith, S. Neurocognitive considerations when assessing Theory of Mind in Autism Spectrum Disorder. J. Child Adolesc. Ment. Health 2016, 28, 233–241. [Google Scholar] [CrossRef] [PubMed]
- MacFabe, D.F. Enteric short-chain fatty acids: Microbial messengers of metabolism, mitochondria, and mind: Implications in autism spectrum disorders. Microb. Ecol. Health Dis. 2015, 26, 28177. [Google Scholar] [CrossRef] [PubMed]
- Barnevik-Olsson, M.; Gillberg, C.; Fernell, E. Prevalence of autism in children of Somali origin living in Stockholm: Brief report of an at-risk population. Dev. Med. Child Neurol. 2010, 52, 1167–1168. [Google Scholar] [CrossRef] [PubMed]
- Barfi, S.; Narges, C.; Pouretemad, H.R.; Poortahmasebi, V.; Norouzi, M.; Farahmand, M.; Yahyapour, Y.; Ghorbani, S.; Ghalichi, L.; Ofoghi, H.; et al. Measurement of serum hepatitis B surface antibody levels in Iranian autistic children and evaluation of immunological memory after booster dose injection in comparison with controls. J. Med. Virol. 2019, 91, 1272–1278. [Google Scholar] [CrossRef] [PubMed]
- Srikantha, P.; Mohajeri, M.H. The Possible Role of the Microbiota-Gut-Brain-Axis in Autism Spectrum Disorder. Int. J. Mol. Sci. 2019, 20, 2115. [Google Scholar] [CrossRef] [PubMed]
- McElhanon, B.O.; McCracken, C.; Karpen, S.; Sharp, W.G. Gastrointestinal Symptoms in Autism Spectrum Disorder: A Meta-analysis. Pediatrics 2014, 133, 872–883. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marler, S.; Ferguson, B.J.; Lee, E.B.; Peters, B.; Williams, K.C.; McDonnell, E.; Macklin, E.A.; Levitt, P.; Margolis, K.G.; Beversdorf, D.Q.; et al. Association of Rigid-Compulsive Behavior with Functional Constipation in Autism Spectrum Disorder. J. Autism Dev. Disord. 2017, 47, 1673–1681. [Google Scholar] [CrossRef]
- Ferguson, B.J.; Marler, S.; Altstein, L.L.; Lee, E.B.; Mazurek, M.O.; McLaughlin, A.; Macklin, E.A.; McDonnell, E.; Davis, D.J.; Belenchia, A.M.; et al. Associations between cytokines, endocrine stress response, and gastrointestinal symptoms in autism spectrum disorder. Brain Behav. Immun. 2016, 58, 57–62. [Google Scholar] [CrossRef] [Green Version]
- Sanchez-Samper, E.; Gomez-Gallego, C.; Andreo-Martinez, P.; Salminen, S.; Ros, G. Mice gut microbiota programming by using the infant food profile. The effect on growth, gut microbiota and the immune system. Food Funct. 2017, 8, 3758–3768. [Google Scholar] [CrossRef] [PubMed]
- Mangiola, F.; Ianiro, G.; Franceschi, F.; Fagiuoli, S.; Gasbarrini, G.; Gasbarrini, A. Gut microbiota in autism and mood disorders. World J. Gastroenterol. 2016, 22, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Hill, D.A.; Hoffmann, C.; Abt, M.C.; Du, Y.; Kobuley, D.; Kirn, T.J.; Bushman, F.D.; Artis, D. Metagenomic analyses reveal antibiotic-induced temporal and spatial changes in intestinal microbiota with associated alterations in immune cell homeostasis. Mucosal Immunol. 2010, 3, 148–158. [Google Scholar] [CrossRef] [PubMed]
- Jiang, C.; Li, G.; Huang, P.; Liu, Z.; Zhao, B. The Gut Microbiota and Alzheimer’s Disease. J. Alzheimer’s Dis. 2017, 58, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Navarro, F.; Liu, Y.Y.; Rhoads, J.M. Can probiotics benefit children with autism spectrum disorders? World J. Gastroenterol. 2016, 22, 10093–10102. [Google Scholar] [CrossRef] [PubMed]
- Ng, Q.X.; Loke, W.; Venkatanarayanan, N.; Lim, D.Y.; Soh, A.Y.S. A Systematic Review of the Role of Prebiotics and Probiotics in Autism Spectrum Disorders. Medicina 2019, 55, 129. [Google Scholar] [CrossRef] [PubMed]
- Kang, D.-W.; Adams, J.B.; Gregory, A.C.; Borody, T.; Chittick, L.; Fasano, A.; Khoruts, A.; Geis, E.; Maldonado, J.; McDonough-Means, S.; et al. Microbiota Transfer Therapy alters gut ecosystem and improves gastrointestinal and autism symptoms: An open-label study. Microbiome 2017, 5, 10. [Google Scholar] [CrossRef]
- Shaaban, S.Y.; El Gendy, Y.G.; Mehanna, N.S.; El-Senousy, W.M.; El-Feki, H.S.A.; Saad, K.; El-Asheer, O.M. The role of probiotics in children with autism spectrum disorder: A prospective, open-label study. Nutr. Neurosci. 2017. [Google Scholar] [CrossRef]
- Liu, T.; Kelly, J.; Davis, L.; Zamora, K. Nutrition, BMI and Motor Competence in Children with Autism Spectrum Disorder. Medicina 2019, 55, 135. [Google Scholar] [CrossRef]
- Ng, Q.X.; Soh, A.Y.S.; Loke, W.; Venkatanarayanan, N.; Lim, D.Y.; Yeo, W.S. A Meta-Analysis of the Clinical Use of Curcumin for Irritable Bowel Syndrome (IBS). J. Clin. Med. 2018, 7, 298. [Google Scholar] [CrossRef]
- Feng, W.; Wang, H.; Zhang, P.; Gao, C.; Tao, J.; Ge, Z.; Zhu, D.; Bi, Y. Modulation of gut microbiota contributes to curcumin-mediated attenuation of hepatic steatosis in rats. Biochim. Biophys. Acta Gen. Subj. 2017, 1861, 1801–1812. [Google Scholar] [CrossRef] [PubMed]
- Wilson, J.; Wright, B.; Jost, S.; Smith, R.; Pearce, H.; Richardson, S. Can urinary indolylacroylglycine levels be used to determine whether children with autism will benefit from dietary intervention? Pediatr. Res. 2016, 81, 672. [Google Scholar] [CrossRef] [PubMed]
- García-Mazcorro, J.F.; Garza-González, E.; Marroquín-Cardona, A.G.; Tamayo, J.L. Caracterización, influencia y manipulación de la microbiota gastrointestinal en salud y enfermedad. Gastroenterol. Hepatol. 2015, 38, 445–466. [Google Scholar] [CrossRef] [PubMed]
- Salipante, S.J.; Sengupta, D.J.; Rosenthal, C.; Costa, G.; Spangler, J.; Sims, E.H.; Jacobs, M.A.; Miller, S.I.; Hoogestraat, D.R.; Cookson, B.T.; et al. Rapid 16S rRNA Next-Generation Sequencing of Polymicrobial Clinical Samples for Diagnosis of Complex Bacterial Infections. PLoS ONE 2013, 8, e65226. [Google Scholar] [CrossRef]
- Zapka, C.; Leff, J.; Henley, J.; Tittl, J.; De Nardo, E.; Butler, M.; Griggs, R.; Fierer, N.; Edmonds-Wilson, S. Comparison of Standard Culture-Based Method to Culture-Independent Method for Evaluation of Hygiene Effects on the Hand Microbiome. mBio 2017, 8, e00093-17. [Google Scholar] [CrossRef] [Green Version]
- Kang, D.W.; Park, J.G.; Ilhan, Z.E.; Wallstrom, G.; Labaer, J.; Adams, J.B.; Krajmalnik-Brown, R. Reduced incidence of Prevotella and other fermenters in intestinal microflora of autistic children. PLoS ONE 2013, 8, e68322. [Google Scholar] [CrossRef]
- Kang, D.-W.; Ilhan, Z.E.; Isern, N.G.; Hoyt, D.W.; Howsmon, D.P.; Shaffer, M.; Lozupone, C.A.; Hahn, J.; Adams, J.B.; Krajmalnik-Brown, R. Differences in fecal microbial metabolites and microbiota of children with autism spectrum disorders. Anaerobe 2018, 49, 121–131. [Google Scholar] [CrossRef]
- Finegold, S.M.; Summanen, P.H.; Downes, J.; Corbett, K.; Komoriya, T. Detection of Clostridium perfringens toxin genes in the gut microbiota of autistic children. Anaerobe 2017, 45, 133–137. [Google Scholar] [CrossRef]
- Iovene, M.R.; Bombace, F.; Maresca, R.; Sapone, A.; Iardino, P.; Picardi, A.; Marotta, R.; Schiraldi, C.; Siniscalco, D.; Serra, N.; et al. Intestinal Dysbiosis and Yeast Isolation in Stool of Subjects with Autism Spectrum Disorders. Mycopathologia 2017, 182, 349–363. [Google Scholar] [CrossRef]
- Tomova, A.; Husarova, V.; Lakatosova, S.; Bakos, J.; Vlkova, B.; Babinska, K.; Ostatnikova, D. Gastrointestinal microbiota in children with autism in Slovakia. Physiol. Behav. 2015, 138, 179–187. [Google Scholar] [CrossRef]
- Hughes, H.K.; Rose, D.; Ashwood, P. The Gut Microbiota and Dysbiosis in Autism Spectrum Disorders. Curr. Neurol. Neurosci. Rep. 2018, 18, 81. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Li, J.; Wu, F.; Zheng, H.; Peng, Q.; Zhou, H. Altered composition and function of intestinal microbiota in autism spectrum disorders: A systematic review. Transl. Psychiatry 2019, 9, 43. [Google Scholar] [CrossRef] [PubMed]
- Andreo-Martínez, P.; García-Martínez, N.; Quesada-Medina, J.; Sánchez-Samper, E.P.; Martínez-González, A.E. Candida spp. en la microbiota intestinal de las personas con autismo: Revisión sistemática. Rev. Neurol. 2019, 68, 1–6. [Google Scholar]
- Parracho, H.M.; Bingham, M.O.; Gibson, G.R.; McCartney, A.L. Differences between the gut microflora of children with autistic spectrum disorders and that of healthy children. J. Med. Microbiol. 2005, 54, 987–991. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef]
- Viswanathan, M.; Patnode, C.D.; Berkman, N.D.; Bass, E.B.; Chang, S.; Hartling, L.; Murad, M.H.; Treadwell, J.R.; Kane, R.L. Assessing the risk of bias in systematic reviews of health care interventions. In Methods Guide for Effectiveness and Comparative Effectiveness Reviews; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2017. [Google Scholar]
- Williams, B.L.; Hornig, M.; Parekh, T.; Lipkin, W.I. Application of Novel PCR-Based Methods for Detection, Quantitation, and Phylogenetic Characterization of Sutterella Species in Intestinal Biopsy Samples from Children with Autism and Gastrointestinal Disturbances. mBio 2012, 3, e00261-11. [Google Scholar] [CrossRef]
- Gondalia, S.V.; Palombo, E.A.; Knowles, S.R.; Cox, S.B.; Meyer, D.; Austin, D.W. Molecular characterisation of gastrointestinal microbiota of children with autism (with and without gastrointestinal dysfunction) and their neurotypical siblings. Autism Res. 2012, 5, 419–427. [Google Scholar] [CrossRef]
- Wang, L.; Christophersen, C.T.; Sorich, M.J.; Gerber, J.P.; Angley, M.T.; Conlon, M.A. Increased abundance of Sutterella spp. and Ruminococcus torques in feces of children with autism spectrum disorder. Mol. Autism. 2013, 4, 42. [Google Scholar] [CrossRef]
- Son, J.S.; Zheng, L.J.; Rowehl, L.M.; Tian, X.; Zhang, Y.; Zhu, W.; Litcher-Kelly, L.; Gadow, K.D.; Gathungu, G.; Robertson, C.E.; et al. Comparison of Fecal Microbiota in Children with Autism Spectrum Disorders and Neurotypical Siblings in the Simons Simplex Collection. PLoS ONE 2015, 10, e0137725. [Google Scholar] [CrossRef]
- Strati, F.; Cavalieri, D.; Albanese, D.; De Felice, C.; Donati, C.; Hayek, J.; Jousson, O.; Leoncini, S.; Renzi, D.; Calabro, A.; et al. New evidences on the altered gut microbiota in autism spectrum disorders. Microbiome 2017, 5, 24. [Google Scholar] [CrossRef]
- Luna, R.A.; Oezguen, N.; Balderas, M.; Venkatachalam, A.; Runge, J.K.; Versalovic, J.; Veenstra-VanderWeele, J.; Anderson, G.M.; Savidge, T.; Williams, K.C. Distinct Microbiome-Neuroimmune Signatures Correlate With Functional Abdominal Pain in Children With Autism Spectrum Disorder. Cell. Mol. Gastroenterol. Hepatol. 2017, 3, 218–230. [Google Scholar] [CrossRef] [PubMed]
- Kushak, R.I.; Winter, H.S.; Buie, T.M.; Cox, S.B.; Phillips, C.D.; Ward, N.L. Analysis of the Duodenal Microbiome in Autistic Individuals: Association With Carbohydrate Digestion. J. Pediatr. Gastroenterol. Nutr. 2017, 64, e110–e116. [Google Scholar] [CrossRef] [PubMed]
- Gora, B.; Gofron, Z.; Grosiak, M.; Aptekorz, M.; Kazek, B.; Kocelak, P.; Radosz-Komoniewska, H.; Chudek, J.; Martirosian, G. Toxin profile of fecal Clostridium perfringens strains isolated from children with autism spectrum disorders. Anaerobe 2018, 51, 73–77. [Google Scholar] [CrossRef] [PubMed]
- Pulikkan, J.; Maji, A.; Dhakan, D.B.; Saxena, R.; Mohan, B.; Anto, M.M.; Agarwal, N.; Grace, T.; Sharma, V.K. Gut Microbial Dysbiosis in Indian Children with Autism Spectrum Disorders. Microb. Ecol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Rose, D.R.; Yang, H.; Serena, G.; Sturgeon, C.; Ma, B.; Careaga, M.; Hughes, H.K.; Angkustsiri, K.; Rose, M.; Hertz-Picciotto, I.; et al. Differential immune responses and microbiota profiles in children with autism spectrum disorders and co-morbid gastrointestinal symptoms. Brain Behav. Immun. 2018, 70, 354–368. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Ma, W.; Zhang, J.; He, Y.; Wang, J. Analysis of gut microbiota profiles and microbe-disease associations in children with autism spectrum disorders in China. Sci. Rep. 2018, 8, 13981. [Google Scholar] [CrossRef]
- Martinez-Gonzalez, A.E.; Piqueras, J.A. Validation of the Repetitive Behavior Scale-Revised in Spanish-Speakers Participants with Autism Spectrum Disorder. J. Autism Dev. Disord. 2018, 48, 198–208. [Google Scholar] [CrossRef]
- Adams, J.B.; Johansen, L.J.; Powell, L.D.; Quig, D.; Rubin, R.A. Gastrointestinal flora and gastrointestinal status in children with autism–comparisons to typical children and correlation with autism severity. BMC Gastroenterol. 2011, 11, 22. [Google Scholar] [CrossRef]
- Kantarcioglu, A.S.; Kiraz, N.; Aydin, A. Microbiota-Gut-Brain Axis: Yeast Species Isolated from Stool Samples of Children with Suspected or Diagnosed Autism Spectrum Disorders and In Vitro Susceptibility against Nystatin and Fluconazole. Mycopathologia 2016, 181, 1–7. [Google Scholar] [CrossRef]
- Zelante, T.; Iannitti, R.G.; Cunha, C.; De Luca, A.; Giovannini, G.; Pieraccini, G.; Zecchi, R.; D’Angelo, C.; Massi-Benedetti, C.; Fallarino, F.; et al. Tryptophan catabolites from microbiota engage aryl hydrocarbon receptor and balance mucosal reactivity via interleukin-22. Immunity 2013, 39, 372–385. [Google Scholar] [CrossRef]
- Krajmalnik-Brown, R.; Lozupone, C.; Kang, D.-W.; Adams, J.B. Gut bacteria in children with autism spectrum disorders: Challenges and promise of studying how a complex community influences a complex disease. Microb. Ecol. Health Dis. 2015, 26, 26914. [Google Scholar] [CrossRef] [PubMed]
- Ding, H.T.; Taur, Y.; Walkup, J.T. Gut Microbiota and Autism: Key Concepts and Findings. J. Autism Dev. Disord. 2017, 47, 480–489. [Google Scholar] [CrossRef] [PubMed]
- Rossignol, D.A.; Frye, R.E. Mitochondrial dysfunction in autism spectrum disorders: A systematic review and meta-analysis. Mol. Psychiatry 2011, 17, 290. [Google Scholar] [CrossRef] [PubMed]
- Vallée, A.; Vallée, J.-N. Warburg effect hypothesis in autism Spectrum disorders. Mol. Brain 2018, 11, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krajmalnik-Brown, R.; Kang, D.W.; Park, J.G.; Labaer, J.; Ilhan, Z. Microbiome Markers and Therapies for Autism Spectrum Disorders. Google Patents WO 2013176774 A1, 28 November 2013. [Google Scholar]
- Gupta, V.K.; Paul, S.; Dutta, C. Geography, Ethnicity or Subsistence-Specific Variations in Human Microbiome Composition and Diversity. Front. Microbiol. 2017, 8, 1162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alinovi, C.A.; Ward, M.P.; Lin, T.L.; Moore, G.E.; Wu, C.C. Real-time PCR, compared to liquid and solid culture media and ELISA, for the detection of Mycobacterium avium ssp. paratuberculosis. Vet. Microbiol. 2009, 136, 177–179. [Google Scholar] [CrossRef] [PubMed]
- Marteau, P.; Pochart, P.; Dore, J.; Bera-Maillet, C.; Bernalier, A.; Corthier, G. Comparative study of bacterial groups within the human cecal and fecal microbiota. Appl. Environ. Microbiol. 2001, 67, 4939–4942. [Google Scholar] [CrossRef]
- Jin, D.Z.; Wen, S.Y.; Chen, S.H.; Lin, F.; Wang, S.Q. Detection and identification of intestinal pathogens in clinical specimens using DNA microarrays. Mol. Cell. Probes 2006, 20, 337–347. [Google Scholar] [CrossRef]
- Eckburg, P.B.; Bik, E.M.; Bernstein, C.N.; Purdom, E.; Dethlefsen, L.; Sargent, M.; Gill, S.R.; Nelson, K.E.; Relman, D.A. Diversity of the human intestinal microbial flora. Science 2005, 308, 1635–1638. [Google Scholar] [CrossRef]
- Wang, P.; Ng, Q.X.; Zhang, H.; Zhang, B.; Ong, C.N.; He, Y. Metabolite changes behind faster growth and less reproduction of Daphnia similis exposed to low-dose silver nanoparticles. Ecotoxicol. Environ. Saf. 2018, 163, 266–273. [Google Scholar] [CrossRef]
Figure 1.
Flowchart showing the process of identifying relevant studies for the present systematic review.
Figure 1.
Flowchart showing the process of identifying relevant studies for the present systematic review.


{kind=link}
Table 1.
Characteristics of the selected studies on gut microbiota and children with ASD and GI symptoms.
Table 1.
Characteristics of the selected studies on gut microbiota and children with ASD and GI symptoms.
| Reference | Subjects | Method | Findings | Limitations | ||
|---|---|---|---|---|---|---|
| Experimental Group | Control Group | Bacteria | Correlation | |||
| [38] | ASD (n = 23) divided into ASD w GI symptoms (12/23) and ASD w/o GI symptoms (11/23) Range Age 3–10 y (15/23 aged 3–5 y; 6/23 aged 6–7 y; 2/23 aged 8–10 y) All males | HC w GI symptoms (n = 9) Range Age 3–10 y (7/9 aged 3–5 y; 1/9 aged 6–7 y; 1/9 aged 8–10 y). All males | Pyrosequencing of the 16S rRNA gene pan-bacterial (V2 region) on ileal and ceca mucosal biopsy samples PCR-based detection of Sutterella 16S rRNA gene sequences (V6–V8 region and C4–V8 region) on ileal and ceca mucosal biopsy samples | Sutterella ↑ in ASD w GI symptoms vs. HC w GI symptoms (ilea p = 0.022/ceca p = 0.037) | No correlations between GM and GI symptoms were studies | ASD severity was not indicated Was not indicated whether the ASD subjects had intellectual disability |
| [39] | ASD (n = 51) divided into ASD w GI symptoms (28/51) and ASD w/o GI symptoms (23/51) Age 2–12 y 42 males 9 females | NT Sib (n = 53) Age 2–12 y 19 males 34 females | Pyrosequencing (bTEFAP) of the 16S rRNA gene bacterial (V1–V3 regions) on fecal samples | No difference in microbiome between total ASD vs. NT Sib. No difference regarding severity ASD in the bacterial composition. No difference regarding GI symptoms dysfunction in the bacterial composition (No differences within the ASD group compared to both with and without GI symptoms groups) | No metabolites were studied | Was not indicated whether the ASD subjects had intellectual disability |
| [27] | ASD w GI symptoms (n = 20) Age 3–16 y 18 males 2 females | NT w GI symptoms (n = 20) Age 3–16 y 17 males 3 females | Pyrosequencing (bTEFAP) of the 16S rRNA gene bacterial (V2–V3 regions) on fecal samples Quantitative real-time PCR for Prevotella | Prevotella (p = 0.04), Coprococcus (p ≤ 0.06) and unclassified Veillonellaceae (p = 0.04) ↓ in ASD vs. NT. Microbial changes were more closely linked to the presence of autistic symptoms rather than to the severity of GI symptoms and specific diet/supplement regimens | No correlations between GM and GI symptoms were studies | Was not indicated whether the ASD subjects had intellectual disability |
| [40] | ASD (n = 23) w or w/o GI symptoms Age 3–18 y Unrevealed sex | HC (n = 9) and NT sib (n = 22) w or w/o GI symptoms Age 3–18 y Unrevealed sex | qPCR for Sutterella, Ruminococcus torques and R. gnavus on fecal samples. | Sutterella ↑ (p = 0.044) in ASD vs. NT Sib. Sutterella ↑ (p = 0.05) in ASD vs. HC. Sutterella ↑ (p = 0.047) in NT Sib vs. HC. Ruminococcus gnavus ↑ (p = 0.046) in NT Sib vs. HC. Ruminococcus torques ↑ (p = 0.008) in ASD w GI symptoms (n = 9) vs. ASD w/o GI symptoms (n = 14). | No correlations between GM and GI symptoms were studies | ASD severity was not indicated Was not indicated whether the ASD subjects had intellectual disability |
| [41] | ASD (n = 59) divided into ASD w GI symptoms (25/59) and ASD w/o GI symptoms (34/59) Age 7–14 y 52 males 7 females | NT Sib (n = 44) divided into NT Sib w GI symptoms (13/44) and NT Sib w/o GI symptoms (31/44) Age 7–14 y 21 males 23 females | qPCR for total bacteria, Sutterella subgroup, Bacteroidetes subgroup, Prevotella, C. coccoides-E. rectales subgroup, Faecalibacterium prausnitzii and Escherichia coli subgroup on fecal samples Sequencing of the 16S rRNA gene bacterial (V1–V2 and V1–V3 regions) on fecal samples | No difference between total ASD vs NT Sib in bacterial frequency. Increased prevalence of functional constipation GI symptoms in ASD children compared to NT siblings | Increased prevalence of functional constipation GI symptoms in ASD children compared to NT siblings. | ASD severity was not indicated Was not indicated whether the ASD subjects had intellectual disability |
| [31] | ASD (n = 10) divided into ASD w GI symptoms (9/10) and ASD w/o GI symptoms (1/10) Age 2–9, 9 males and 1 female Sib (n = 9) divided into Sib w GI symptoms (7/9) and Sib w/o GI symptoms (2/9) Age 5–17, 7 males and 3 females | HC (n = 10) divided into HC w GI symptoms (6/10) and HC w/o GI symptoms (4/10) Age 2–11, 10 males | qPCR for Bacteroidetes, Firmicutes, Bifidobacterium, Lactobacillus, Clostridium cluster 1, S. thermophiles, Desulfovibrio on fecal samples | Bacteroidetes/Firmicutes ratio↓ in ASD vs. HC (p < 0.05); ↓ Sib vs. ASD (p < 0.05); ↓ Sib vs. HC (p < 0.05) Firmicutes ↑ in Sib vs. HC Lactobacillus ↑ in ASD vs. HC (p < 0.05) Bifidobacterium ↑ in ASD vs. Sib (p < 0.05) | Desulfovibrio with ASD severity in the ADI restricted/repetitive behavior subscale score. There is a correlation of the autism severity with the severity of GI dysfunction. (p = 0.01) No correlation of GI symptoms and Desulfovibrio abundance. | Was not indicated whether the ASD subjects had intellectual disability |
| [42] | ASD (n = 40) divided into severe ASD (36/40) and moderately severe ASD (4/40) 5 constipated 29 non-constipated Average age 11.1 ± 6.8 31 males 9 females | NT (n = 40) 11 constipated 29 non-constipated Average age 9.2 ± 7.9 28 males 12 females | Pyrosequencing of the 16S rRNA gene bacterial (V3–V5 regions) and the internal transcribed spacer (ITS) for fungal (ITS1 rDNA region) on fecal samples | Firmicutes/Bacteroidetes ratio↑, Bacteroidetes ↓, Veillonella ↓, Alistipes ↓, Bilophila↓, Dialister↓, Parabacteroides↓ in ASD vs. NT (p < 0.005) Lactobacillus ↑, Dorea ↑, Corynebacterium ↑, Collinsella ↑, Candida ↑ in ASD vs. NT (p < 0.001) | Escherichia/Shigella and cluster XVIII with GI symptoms or constipation (p < 0.05) | Was not indicated whether the ASD subjects had intellectual disability |
| [30] | Severe ASD (n = 47) w/o or w GI symptoms Average age 6 ± 2.8 y 40 males 7 females | HC (n = 33) w/o or w GI symptoms Average age 7.3 ± 3.1 y 24 males 9 females | Examination and culture of fecal samples: (a) morphological examination, (b) microscopic examination staining, (c) search for toxins a/b of Clostridium difficilis, (d) bacterial/yeast culture and (e) identification of bacteria and yeast colonies by VITEK 2 microbial identification system | Candida aggressive form (pseudo-hyphae presenting) Candida ↑ in ASD vs. HC (p = 8.67 × 10−6) Lactobacillus ↓ in ASD vs. HC (p = 7.28x10−4) Clostridium ↓ in ASD vs. HC (p = 0.01) | GI symptoms in 70.2% ASDs and no controls, with a mild correlation by multivariate analyses of constipation and alternating bowel versus increased permeability to lactulose. | Was not indicated whether the ASD subjects had intellectual disability |
| [43] | ASD w GI symptoms (n = 14) Age 4–13 y 14 males | NT w GI symptoms (n = 15) Age 3–18 y 12 males 3 females NT w/o GI symptoms (n = 6) Age 3–18 y 6 males | Sequencing of the 16S rRNA gene (V1–V3 and V4 regions) on rectum mucosal biopsy samples | Blautia ↓ (p = 0.02), Dorea ↓ (p = 0.006), Sutterella ↓ (p = 0.025) in ASD w GI symptoms vs. NT w GI symptoms Clostridium lituseburense ↑ (p = 0.002), Lachnoclostridium bolteae ↑ (p = 0.017), Lachnoclostridium hathewayi ↑ (p = 0.03), Clostridium aldenense ↑ (p = 0.03), and Flavonifractor plautii ↑ (p = 0.03), in ASD w GI symptoms vs. NT w GI symptoms and NT w/o GI symptoms Faecalibacterium prausnitzii ↑, Roseburia intestinalis ↑, Oscillospira valericigenes ↑, and Bilophila wadsworthia ↑ (p < 0.05) in NT w GI symptoms vs. NT w/o GI symptoms | IBS with ↑ Clostridium aldenense (p = 0.04); Functional constipation with ↓ Flavonifractor plautii (p = 0.03), Bacteroides eggerthii (p = 0.02), Bacteroides uniformis (p = 0.04), Faecalibacterium prausnitzii (p = 0.013), Clostridium clariflavum (p = 0.03); Aerophagia with ↑ Clostridium aldenense (p = 0.03), ↓ in Blautia luti (p = 0.003), Bifidobacterium adolescentis (p = 0.01), Eubacterium ventriosum (p = 0.05), Anoxystipes fissicatena (p = 0.02), Coprococcus comes (p = 0.04), Eubacterium ramulus (p = 0.006), and Phascolarctobacterium faecium (p = 0.04); Abdominal migraine with ↓ in Akkermansia muciniphila (p = 0.03), Coprococcus catus (p = 0.007), Odoribacter splanchnicus (p = 0.05), Clostridium lactatifermentans (p = 0.03) and Ruminococcus lactaris (p = 0.03) Serotonin with Lachnoclostridium bolteae (p = 0.002), Lachnoclostridium hathewayi (p = 0.003) and Flavonifractor plautii (p = 0.001) | ASD severity was not indicated Was not indicated whether the ASD subjects had intellectual disability |
| [29] | ASD w GI symptoms (n = 33) Age 2–9 y Unidentified sex | HC w/o GI symptoms (n = 13) Age 2–9 y Unidentified sex | Selective culture methods for Clostridium and for Clostridium perfringens strains on fecal samples: Brucella and CDC agar. PCR for Clostridium perfringens toxin genes: alpha (cpa), beta (cpb), beta 2 (cpb2), epsilon (ctx), iota (iA), and enterotoxin (cpe) | Clostridium perfringens ↑ in ASD w GI symptoms vs. HC (p = 0.03) | No correlations between GM and GI symptoms were studies | ASD severity was not indicated Was not indicated whether the ASD subjects had intellectual disability |
| [44] | ASD (n = 21) w GI symptoms Age 14.4 ± 1.1 y 19 males 2 females | HC (n = 19) w GI symptoms Age 16 ± 1.2 y 10 males 9 females | Pyrosequencing of the 16S rRNA gene bacterial (V1–V3 regions) on duodenal biopsies samples from the second part of the duodenum | No differences in microbiome diversity (alpha and beta) Burkholderia ↑ (p = 0.03) and Neisseria ↓ (p = 0.01) in ASD vs. HC Bacteroides vulgatus ↓ (p = 0.005), unidentified Bacteroides ↓ (p = 0.04), and Escherichia coli ↓ (p = 0.05) in ASD vs. HC Oscillospira, Actinomyces, Peptostreptococcus, and Ralstonia ↑ (p < 0.05) in ASD vs. HC Devosia, Prevotella, Bacteroides, and Streptococcus ↓ (p < 0.05) in ASD vs. HC | ↑ frequency of constipation in ASD vs. HC (p < 0.005) | ASD severity was not indicated Was not indicated whether the ASD subjects had intellectual disability |
| [45] | ASD (n = 29) w GI symptoms (49 isolated strains of Clostridium perfringens) Age 3.5–18 y 23 males 9 females | HC (n = 17) (30 isolated strains of Clostridium perfringens) Obese children (n = 24) (32 isolated strains of Clostridium perfringens) Unrevealed age and sex | Selective culture method for fecal samples: Columbia blood and reinforced clostridial agar under anaerobic conditions. Hemolysis test, lecithinase, and lipase production on egg yolk agar, and identified with use of ANC cards in VITEK 2 compact. Subcultured in BHI broth and Gene MATRIX DNA Purifi cation Kit by DNA Gdansk for isolation of DN Multiplex PCR for toxin alpha (cpa), toxin beta (cbp), enterotoxin (ecpe), iota-toxin (cpiA), epsilon toxin (etx) genes | The cpa gene encoding alpha toxin was present in all 111 (100%) strains The cpb2 gene encoding beta2 toxin was found in: 45/49 (91.8%) strains isolated from ASD children, 17/30 (56.7%) strains isolated from healthy subjects (p < 0.001), and 12/32 (37.5%) strains isolated from obese children (p < 0.001) Clostridium perfringens (cpb2 gene) was detected in: 27/29 (93.1%) ASD, 10/17 (58.8%) HC (p < 0.008), and 11/24 (45.8%) obese children (p < 0.001) No differences between HC and obese children (cpb2 and Clostridium perfringens with cpb2) | No correlations between GM and GI symptoms were studies | ASD severity was not indicated Was not indicated whether the ASD subjects had intellectual disability A small number of studied patients and strains |
| [28] | ASD (n = 23) divided into ASD w GI symptoms (21/23) and ASD w/o GI symptoms (2/23) Age 4–17 y 15 males 6 females | NT (n = 21) divided into NT w GI symptoms (10/21) and NT w/o GI symptoms (11/21) Age 4–17 y 22 males 1 female | Pyrosequencing of the 16S rRNA gene bacterial (V2–V3 regions) on fecal samples | Gut microbial diversity (alpha) ↓ (p < 0.001) and relative abundances of phylotypes most closely related to Prevotella copri ↓ (p < 0.04) in ASD Faecalibacterium ↓ (p < 0.01) and Haemophilus ↓ (p < 0.05) in ASD vs. NT Feacalibacterium prausnitzii ↓ (p < 0.01) and Haemophilus parainfluenzae ↓ (p < 0.05) in ASD vs. NT | GI symptoms were significantly more severe for children with ASD compared to controls (ATEC subscale = p < 0.01) | ASD severity was not indicated Was not indicated whether the ASD subjects had intellectual disability |
| [46] | ASD (n = 30) divided into severe ASD (28/30) and moderate ASD (2/30) w GI symptoms Age 3–16 y 28 males 2 females BMI 6.9–20.5 | HC mostly Sib or blood relatives to the ASD children (n = 24) w/o GI symptoms Age 3.5–16 y 15 males 9 females BMI 13.4–31 | Sequencing of the 16S rRNA gene bacterial (V3 region) on fecal samples | Firmicutes ↑ in ASD vs. HC Sib (p < 0.05) Prevotellaceae ↓ and Veillonelleaceae ↑ in ASD vs. HC Sib Lactobacillaceae ↑ (p = 0.018), Bifidobacteriaceae ↑ (p = 0.0054), and Veillonellaceae ↑ (p = 0.008) in ASD vs. HC Sib Erysipelotrichaceae ↑ (p = 0.0005), Enterococcaceae ↑ (p = 0.0127), and Desulfovibrionaceae ↑ (p = 0.03) in ASD vs. HC Sib Bifidobacterium ↑ (p = 0.005), Lactobacillus ↑ (p = 0.018), Megasphaera ↑ (p = 0.0008), and Mirsuokella ↑ (p = 0.007) in ASD vs. HC Sib 99% of Lactobacillus was Lactobacillus ruminis in ASD group | No correlations between GM and GI symptoms were studies | Was not indicated whether the ASD subjects had intellectual disability |
| [47] | ASD w GI symptoms (blood: n = 20, 15 males, 5 females) (stool: n = 21, 17 males, 4 females) ASD w/o GI symptoms (blood: n = 26, 19 males, 7 females) (stool: n = 29, 25 males, 4 females) Age 3–12 y | HC w GI symptoms (blood: n = 6, 5 males, 1 female) (stool: n = 7, 6 males, 1 female) HC w/o GI symptoms (blood: n = 35, 24 males, 11 females) (stool: n = 34, 32 males, 2 females) Age 3–12 y | Sequencing of the 16S rRNA gene bacterial (V3–V4 regions) on fecal samples | Bacteroidaceae ↑, Lachnospiraceae ↑, Ruminococcaceae ↑, and Prevotellaceae ↑ in ASD w GI symptoms vs. HC w GI symptoms Il-5, IL-15, and IL-17 ↑ in ASD w GI symptoms vs. ASD w/o GI symptoms (after exposure to the TLR-4 agonist LPS) TGFbeta1↓ in ASD w GI symptoms vs. ASD w/o GI symptoms and HC w/o GI symptoms (p < 0.05) (under the majority of conditions examined) | Differences in the microbiome composition of children with ASD vs HC groups, irrespective of GI symptoms | ASD severity was not indicated. Was not indicated whether the ASD subjects had intellectual disability Limited sample size and younger age of the HC with GI symptoms group |
| [48] | ASD w GI symptoms (n = 35, 29 males, 6 females) Age 3–8 y | HC (n = 6, 5 males, 1 females) Age 3–8 y | Sequencing of the 16S rRNA gene bacterial (V3–V4 regions) on fecal samples. | Firmicutes/Bacteroidetes ratio↑ in ASD w GI symptoms vs. HC (p < 0.05) Bacteroidetes ↑ in ASD w GI symptoms vs. HC (p < 0.05) Firmicutes ↓ in ASD w GI symptoms vs. HC (p < 0.05) Veillonella, Streptococcus, Escherichia, Actinomyces, Parvimonas, Bulleida, and Peptoniphilus ↓ in ASD w GI symptoms vs. HC (p < 0.05) | Positive microbe-based link between periodontitis and ASD Negative microbe-based link between type 1 diabetes, constipation (p < 0.05), IBS, psoriasis, and ASD | ASD severity was not indicated. Was not indicated whether the ASD subjects had intellectual disability A small number of studied patients and strains |
Note: w = with; w/o = without; ASD = Autism Spectrum Disorder; HC = Healthy control; GI = Gastrointestinal; NT = Neurotypical; NT Sib = Neurotypical siblings; Sib = siblings; y = years; ADI = Autism Diagnostic Interview; DHEA-S = dehydroepiandrosteronesulfate; IBS = Irritable Bowel Syndrome; BMI = Body Mass Index, FAA = Free Amino Acids; NT = HC; ATEC = Autism Treatment Evaluation Checklist.
Table 2.
Review of author judgments on quality assessment for each included study.
| Item | [38] | [39] | [27] | [40] | [41] | [31] | [42] | [30] | [43] | [29] | [44] | [45] | [28] | [46] | [47] | [48] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Clear stated aim | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| Appropriate study size | 1 | 2 | 2 | 1 | 2 | 1 | 2 | 2 | 1 | 1 | 2 | 2 | 2 | 2 | 1 | 1 |
| Identified and assessed | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| Comparability | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| Blinding of participants and personnel | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Other bias (dietary intake controlled, reports on comorbidity and severity of ASD) | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Adequate statistical analyses | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| TOTAL | 9 | 10 | 10 | 9 | 9 | 9 | 10 | 10 | 9 | 9 | 10 | 10 | 10 | 10 | 9 | 9 |
| Risk of bias | 5 | 4 | 4 | 5 | 5 | 5 | 4 | 4 | 5 | 5 | 4 | 4 | 4 | 4 | 5 | 5 |
| Overall risk of bias | M | M | M | M | M | M | M | M | M | M | M | M | M | M | M | M |
0 = Not reported, 1 = not adequately assessed, 2 = adequately assessed; M = Medium (8–10); L = Low (9–14); H = High (7–1).
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Martínez-González, A.E.; Andreo-Martínez, P. The Role of Gut Microbiota in Gastrointestinal Symptoms of Children with ASD. Medicina 2019, 55, 408. https://doi.org/10.3390/medicina55080408
AMA Style
Martínez-González AE, Andreo-Martínez P. The Role of Gut Microbiota in Gastrointestinal Symptoms of Children with ASD. Medicina. 2019; 55(8):408. https://doi.org/10.3390/medicina55080408
Chicago/Turabian StyleMartínez-González, Agustín Ernesto, and Pedro Andreo-Martínez. 2019. "The Role of Gut Microbiota in Gastrointestinal Symptoms of Children with ASD" Medicina 55, no. 8: 408. https://doi.org/10.3390/medicina55080408