
The Contribution of “Individual Participant Data” Meta-Analyses of Psychotherapies for Depression to the Development of Personalized Treatments: A Systematic Review

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
2.1. Identification and Selection of Studies
2.2. Data Extraction
2.3. Integration of Findings
3. Results
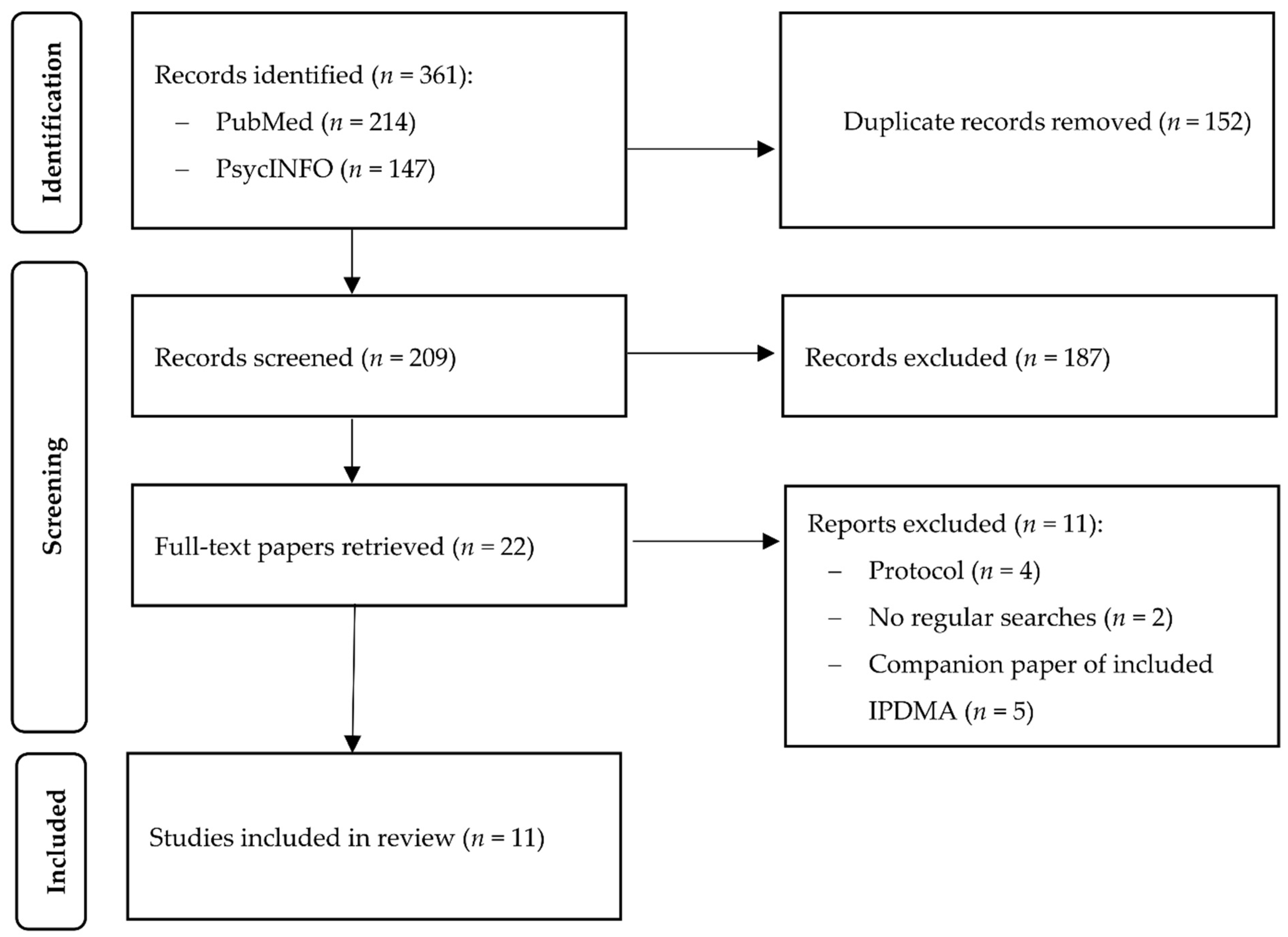
3.1. Selection and Inclusion of Studies
3.2. Characteristics of the Included Studies
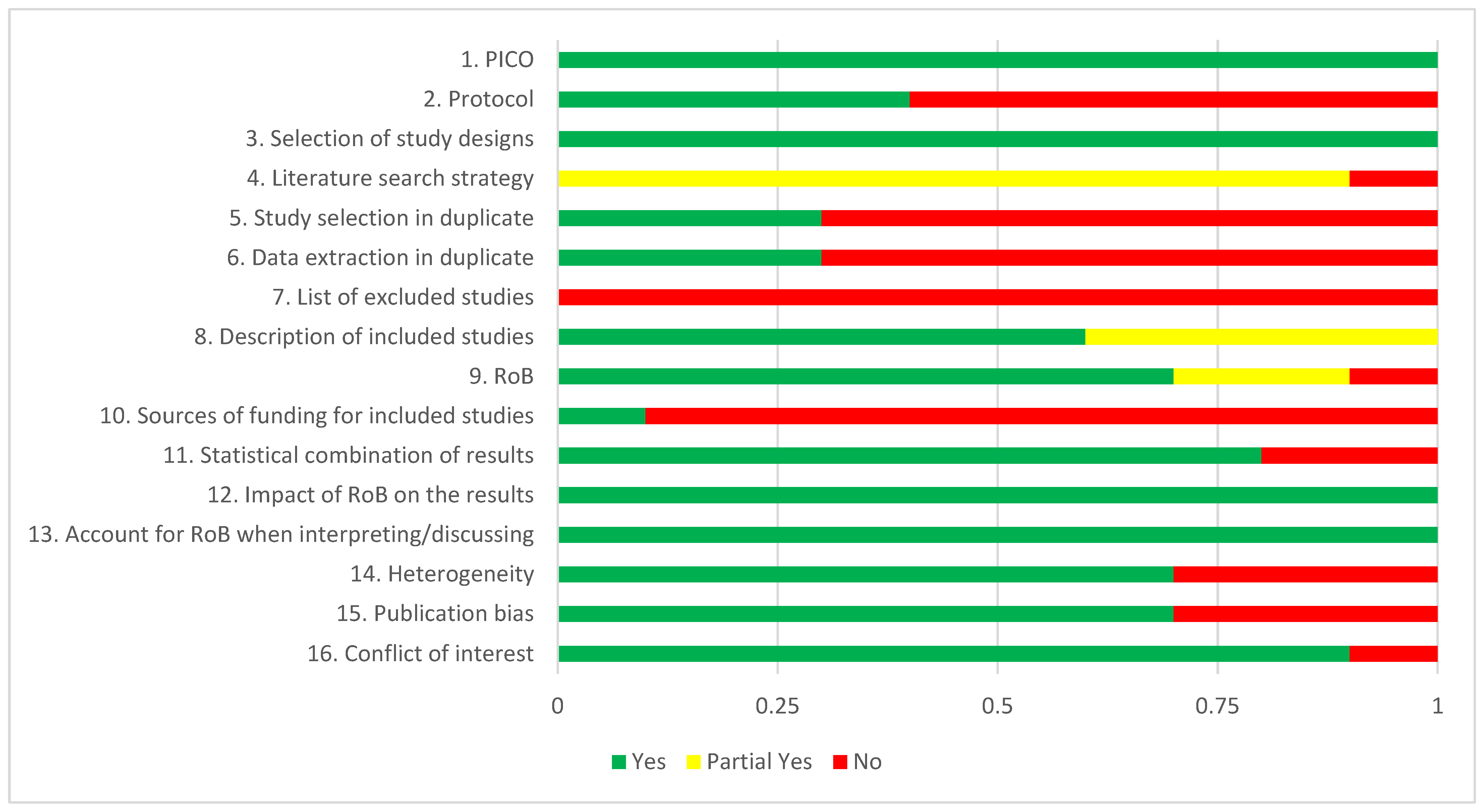
3.3. AMSTAR-2 Ratings
3.4. Predictors and Moderators in Pairwise IPD Meta-Analyses
3.5. Predictors and Moderators in IPD Network Meta-Analyses
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Search Strings
Appendix A.1. PubMed
Appendix A.2. PsycINFO
References
- Cuijpers, P.; Karyotaki, E. A Meta-Analytic Database of Randomised Trials on Psychotherapies for Depression; OSFHome: Charlottesville, VA, USA, 2020; Available online: https://doi.org/10.17605/OSF.IO/825C6 (accessed on 25 November 2021).
- Cuijpers, P.; Quero, S.; Noma, H.; Ciharova, M.; Miguel, C.; Karyotaki, E.; Cipriani, A.; Cristea, I.A.; Furukawa, T.A. Psychotherapies for depression: A network meta-analysis covering efficacy, acceptability and long-term outcomes of all main treatment types. World Psychiatry 2021, 20, 283–293. [Google Scholar] [CrossRef]
- Cuijpers, P.; Noma, H.; Karyotaki, E.; Vinkers, C.H.; Cipriani, A.; Furukawa, T.A. A network meta-analysis of the effects of psychotherapies, pharmacotherapies and their combination in the treatment of adult depression. World Psychiatry 2020, 19, 92–107. [Google Scholar] [CrossRef]
- Furukawa, T.A.; Shinohara, K.; Sahker, E.; Karyotaki, E.; Miguel, C.; Ciharova, M.; Bockting, C.L.; Breedvelt, J.J.; Tajika, A.; Imai, H.; et al. Initial treatment choices to achieve sustained response in major depression: A systematic review and network meta-analysis. World Psychiatry 2021, 20, 387–396. [Google Scholar] [CrossRef]
- Paul, G.L. Strategy of outcome research in psychotherapy. J. Consult. Psychol. 1967, 31, 109–118. [Google Scholar] [CrossRef]
- Turner, J.A.; Holtzman, A.; Mancl, L. Mediators, moderators, and predictors of therapeutic change in cognitive–behavioral therapy for chronic pain. Pain 2007, 127, 276–286. [Google Scholar] [CrossRef]
- Brookes, S.T.; Whitely, E.; Egger, M.; Smith, G.D.; Mulheran, P.A.; Peters, T.J. Subgroup analyses in randomized trials: Risks of subgroup-specific analyses; power and sample size for the interaction test. J. Clin. Epidemiol. 2004, 57, 229–236. [Google Scholar] [CrossRef] [PubMed]
- Tierney, J.F.; Vale, C.; Riley, R.; Smith, C.T.; Stewart, L.; Clarke, M.; Rovers, M. Individual Participant Data (IPD) Meta-analyses of Randomised Controlled Trials: Guidance on Their Use. PLoS Med. 2015, 12, e1001855. [Google Scholar] [CrossRef] [Green Version]
- Cuijpers, P. The Contribution of ‘Individual Patient Data’ Meta-Analyses of Psychotherapies for Depression to the Development of Personalised Treatments: A Systematic Review; OSFHome: Charlottesville, VA, USA, 2021; Available online: https://osf.io/dkyxt (accessed on 25 November 2021).
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. Br. Med. J. 2017, 358, j4008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bower, P.; Kontopantelis, E.; Sutton, A.; Kendrick, T.; Richards, D.A.; Gilbody, S.; Knowles, S.; Cuijpers, P.; Andersson, G.; Christensen, H.; et al. Who should get low-intensity treatments for depression? An individual patient data meta-analysis. Br. Med. J. 2013, 346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weitz, E.S.; Hollon, S.D.; Twisk, J.; van Straten, A.; Huibers, M.J.H.; David, D.; DeRubeis, R.J.; Dimidjian, S.; Dunlop, B.W.; Cristea, I.A. Does baseline depression severity moderate depression outcomes between CBT versus pharmacotherapy? An individual patient data meta-analysis. JAMA Psychiatry 2015, 72, 1102–1109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reins, J.A.; Buntrock, C.; Zimmermann, J.; Grund, S.; Harrer, M.; Lehr, D.; Baumeister, H.; Weisel, K.; Domhardt, M.; Imamura, K.; et al. Efficacy and Moderators of Internet-Based Interventions in Adults with Subthreshold Depression: An Individual Participant Data Meta-Analysis of Randomized Controlled Trials. Psychother. Psychosom. 2021, 90, 94–106. [Google Scholar] [CrossRef] [PubMed]
- Furukawa, T.A.; Weitz, E.S.; Tanaka, S.; Hollon, S.D.; Hofmann, S.G.; Andersson, G.; Twisk, J.; DeRubeis, R.J.; Dimidjian, S.; Hegerl, U.; et al. Initial severity of depression and efficacy of cognitive-behaviour therapy, An individual-participant data meta-analysis of pill-placebo-controlled trials. Br. J. Psychiatry 2017, 210, 190–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karyotaki, E.; Ebert, D.D.; Donkin, L.; Riper, H.; Twisk, J.; Burger, S.; Rozental, A.; Lange, A.; Williams, A.D.; Zarski, A.C.; et al. Do Guided Internet-Based Interventions Result in Clinically Relevant Changes for Patients with Depression? An Individual Participant Data Meta-Analysis. Clin. Psychol. Rev. 2018, 63, 80–92. [Google Scholar] [CrossRef] [PubMed]
- Karyotaki, E.; Riper, H.; Twisk, J.; Hoogendoorn, A.; Kleiboer, A.; Mira, A.; Mackinnon, A.; Meyer, B.; Botella, C.; Littlewood, E.; et al. Efficacy of self-guided internet-based cognitive behavioral therapy (iCBT) in treatment of depressive symptoms: An individual participant data meta-analysis. JAMA Psychiatry 2017, 74, 351–359. [Google Scholar] [CrossRef]
- Kuyken, W.; Warren, F.C.; Taylor, R.S.; Whalley, B.; Crane, C.; Bondolfi, G.; Hayes, R.; Huijbers, M.; Ma, H.; Schweizer, S.; et al. Efficacy of Mindfulness-Based Cognitive Therapy in Prevention of Depressive Relapse: An Individual Patient Data Meta-Analysis from Randomized Trials. JAMA Psychiatry 2016, 73, 565–574. [Google Scholar] [CrossRef] [PubMed]
- Driessen, E.; Dekker, J.J.; Peen, J.; Van, H.L.; Maina, G.; Rosso, G.; Rigardetto, S.; Cuniberti, F.; Vitriol, V.G.; Florenzano, R.U.; et al. The efficacy of adding short-term psychodynamic psychotherapy to antidepressants in the treatment of depression: A systematic review and meta-analysis of individual participant data. Clin. Psychol. Rev. 2020, 80, 101886. [Google Scholar] [CrossRef]
- Furukawa, T.A.; Efthimiou, O.; Weitz, E.S.; Cipriani, A.; Keller, M.B.; Kocsis, J.H.; Klein, D.N.; Michalak, J.; Salanti, G.; Cuijpers, P.; et al. Cognitive-behavioral analysis system of psychotherapy (CBASP), drug, or their combination for persistent depressive disorder: Personalizing the treatment choice using individual participant data network meta-regression. Psychother. Psychosom. 2018, 87, 140–153. [Google Scholar] [CrossRef]
- Karyotaki, E.; Efthimiou, O.; Miguel, C.; Bermpohl, F.M.; Furukawa, T.A.; Cuijpers, P. Individual Patient Data Meta-Analyses for Depression (IPDMA-DE) Collaboration. Internet-based Cognitive Behavioral Therapy for Depression; An Individual Patient Data Network Meta-Analysis. JAMA Psychiatry 2020, 78, 361–371. [Google Scholar] [CrossRef]
- Cuijpers, P.; Weitz, E.; Twisk, J.; Kuehner, C.; Cristea, I.; David, D.; DeRubeis, R.J.; Dimidjian, S.; Dunlop, B.W.; Faramarzi, M.; et al. Gender as predictor and moderator of outcome in cognitive behavior therapy and pharmacotherapy for adult depression: An “individual patient data” meta-analysis. Depress. Anx. 2014, 31, 941–951. [Google Scholar] [CrossRef] [Green Version]
- Vittengl, J.R.; Jarrett, R.B.; Weitz, E.; Hollon, S.D.; Twisk, J.; Cristea, I.; David, D.; DeRubeis, R.J.; Dimidjian, S.; Dunlop, B.W.; et al. Divergent outcomes in cognitive behavioral therapy and pharmacotherapy for adult depression. Am. J. Psychiatry 2015, 173, 481–490. [Google Scholar] [CrossRef] [Green Version]
- Ebert, D.D.; Donkin, L.; Andersson, G.; Andrews, G.; Berger, T.; Carlbring, P.; Rozenthal, A.; Choi, I.; Laferton, J.A.C.; Johansson, R.; et al. Does Internet-based guided-self-help for depression cause harm? An individual participant data meta-analysis on deterioration rates and its moderators in randomized controlled trials. Psychol. Med. 2016, 46, 2679–2693. [Google Scholar] [CrossRef]
- Karyotaki, E.; Kemmeren, L.; Riper, H.; Twisk, J.; Hoogendoorn, A.; Kleiboer, A.; Mira, A.; Mackinnon, A.; Meyer, B.; Botella, C.; et al. Is self-guided internet-based cognitive behavioural therapy (iCBT) harmful? An individual participant data meta-analysis. Psychol. Med. 2018, 48, 2456–2466. [Google Scholar] [CrossRef]
- Kolovos, S.; van Dongen, J.M.; Riper, H.; Buntrock, C.; Cuijpers, P.; Ebert, D.D.; Geraedts, A.S.; Kenter, R.M.; Nobis, S.; Smith, A.; et al. Cost effectiveness of guided Internet-based interventions for depression in comparison with control conditions: An individual–participant data meta-analysis. Depress. Anx. 2018, 35, 209–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boschloo, L.; Bekhuis, E.; Weitz, E.S.; Reijnders, M.; DeRubeis, R.J.; Dimidjian, S.; Dunner, D.L.; Dunlop, B.W.; Hegerl, U.; Hollon, S.D.; et al. The symptom-specific efficacy of cognitive behavioral therapy versus antidepressant medication in the treatment of depression: Results from an individual patient data meta-analysis. World Psychiatry 2019, 18, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Furukawa, T.A.; Suganuma, A.; Ostinelli, E.G.; Andersson, G.; Beevers, C.G.; Shumake, J.; Berger, T.; Boele, F.W.; Buntrock, C.; Carlbring, P.; et al. Dismantling, optimising and personalising internet cognitive-behavioural therapy for depression: A systematic review and individual participant data component network meta-analysis. Lancet Psychiatry 2021. epub ahead of print. [Google Scholar] [CrossRef]
- Kessler, R.C.; Van Loo, H.M.; Wardenaar, K.J.; Bossarte, R.M.; Brenner, L.A.; Ebert, D.D.; de Jonge, P.; Nierenberg, A.A.; Rosellini, A.J.; Sampson, N.A.; et al. Using patient self-reports to study heterogeneity of treatment effects in major depressive disorder. Epidemiol. Psychiatr. Sci. 2017, 26, 22–36. [Google Scholar] [CrossRef] [Green Version]
- Cuijpers, P.; Karyotaki, E.; de Wit, L.; Ebert, D.D. The effects of fifteen evidence-supported therapies for adult depression: A meta-analytic review. Psychother. Res. 2020, 30, 279–293. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| AMSTAR-2 a) | |||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study | Intervention | Comparison | Type b) | Nst | Npart | Proportion | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | Tot Y/PY |
| Bower et al., 2013 [11] | Low intens. CBT | Usual care | ma | 16 | 2470 | 55.2 (16/29) | Y | N | Y | N | N | Y | N | PY | N | N | Y | Y | Y | N | Y | Y | 9 |
| Weitz et al., 2015 [12] | CBT | ADM | ma | 16 | 1700 | 66.7 (16/24) | Y | Y | Y | PY | Y | N | N | Y | Y | N | Y | Y | Y | Y | N | Y | 12 |
| Reins et al., 2020 [13] | Indicated prevention | Usual care or WL | ma | 7 | 2186 | 87.5 (7/8) | Y | N | Y | PY | N | N | N | Y | Y | N | N | Y | Y | N | N | Y | 8 |
| Furukawa et al., 2017 [14] | CBT | Pill placebo | ma | 5 | 509 | 100 (5/5) | Y | Y | Y | PY | N | N | N | PY | Y | Y | Y | Y | Y | Y | Y | Y | 13 |
| Karyotaki et al., 2018 [15] | Guided iCBT | Any control | ma | 24 | 4889 | 88.9 (24/27) | Y | N | Y | PY | Y | N | N | Y | Y | N | Y | Y | Y | Y | Y | Y | 12 |
| Karyotaki et al., 2017 [16] | Unguided iCBT | Any control | ma | 13 | 3876 | 81.3 (13/16) | Y | N | Y | PY | Y | Y | N | Y | Y | N | Y | Y | Y | Y | Y | N | 12 |
| Kuyken et al., 2016 [17] | MBCT | Any control or active treatment | ma | 10 | 1258 | 90.0 (9/10) | Y | Y | Y | PY | N | Y | N | Y | Y | N | Y | Y | Y | Y | Y | Y | 13 |
| Driessen et al., 2020 [18] | Dynamic+ADM | ADM | ma | 7 | 482 | 100 (7/7) | Y | N | Y | PY | N | N | N | PY | Y | N | Y | Y | Y | Y | Y | Y | 11 |
| Furukawa et al., 2018 [19] | CBASP vs. ADM | vs. COMB | nma | 3 | 1036 | 100 (3/3) | Y | Y | Y | PY | N | N | N | Y | PY | N | N | Y | Y | N | N | Y | 9 |
| Karyotaki et al., 2021 [20] | Guided iCBT vs. Unguided iCBT | vs. any control | nma | 39 | 8107 | 92.9 (39/42) | Y | N | Y | PY | N | N | N | PY | PY | N | Y | Y | Y | Y | Y | Y | 11 |
| Study | Contrast a) | Effect Size | Significant Predictors/Moderators b) | Non-significant Predictors/Moderators c) |
|---|---|---|---|---|
| IPD meta-analyses | ||||
| Bower et al., 2013 [11] | Low-intensity CBT vs. CTR | CBT > CTR: SMD = −0.42 (95% CI: −0.55; −0.29) | SPE: Baseline severity | - |
| Weitz et al., 2015 [12] | CBT vs. ADM | ADM > CBT (on HAM-D: β = −0.88; p = 0.03) | - | SPE/NSP/MOD: Gender MOD: Baseline severity |
| Furukawa et al., 2017 [14] | CBT vs. pill placebo | CBT > placebo: SMD: −0.22 (95% CI: −0.42; 0.02) | - | SPE: Baseline severity |
| Karyotaki et al., 2018 [18] | Guided iCBT vs. CTR | Guided iCBT > CTR; OR = 2.49 response; OR = 2.41 remission | SPE: Older age; native-born; baseline severity | SPE: Sex; relationship; education; medication use; anxiety; previous episodes; alcohol problems |
| Karyotaki et al., 2017 [16] | Unguided iCBT vs. CTR | Unguided iCBT > control; g = 0.27 | SPE: None | SPE: Age, sex, education, relation-ship status anxiety, baseline severity |
| Kuyken et al., 2016 [17] | MBCT for relapse vs. CTR | MBCT > CTR: HR of relapse = 0.69 (95% CI: 0.58; 0.82) | SPE: Baseline severity | SPE: Age, sex, education, relationship status |
| Driessen et al., 2020 [18] | Dynamic vs. combined treatment | Combined > dynamic therapy; d = 0.26 | - | - |
| Reins et al., 2020 [13] | Internet interventions for subthreshold depression | Internet interventions > control; d = 0.39 | SPE: Higher baseline severity; Older age | SPE: Gender; relationship; employment; previous therapy; medication use; anxiety; medical condition; education |
| IPD network meta-analyses | Examined moderators/predictors and models | |||
| Furukawa et al., 2018 [19] |
|
|
| |
| Karyotaki et al., 2021 [20] |
|
|
| |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cuijpers, P.; Ciharova, M.; Quero, S.; Miguel, C.; Driessen, E.; Harrer, M.; Purgato, M.; Ebert, D.; Karyotaki, E. The Contribution of “Individual Participant Data” Meta-Analyses of Psychotherapies for Depression to the Development of Personalized Treatments: A Systematic Review. J. Pers. Med. 2022, 12, 93. https://doi.org/10.3390/jpm12010093
Cuijpers P, Ciharova M, Quero S, Miguel C, Driessen E, Harrer M, Purgato M, Ebert D, Karyotaki E. The Contribution of “Individual Participant Data” Meta-Analyses of Psychotherapies for Depression to the Development of Personalized Treatments: A Systematic Review. Journal of Personalized Medicine. 2022; 12(1):93. https://doi.org/10.3390/jpm12010093
Chicago/Turabian StyleCuijpers, Pim, Marketa Ciharova, Soledad Quero, Clara Miguel, Ellen Driessen, Mathias Harrer, Marianna Purgato, David Ebert, and Eirini Karyotaki. 2022. "The Contribution of “Individual Participant Data” Meta-Analyses of Psychotherapies for Depression to the Development of Personalized Treatments: A Systematic Review" Journal of Personalized Medicine 12, no. 1: 93. https://doi.org/10.3390/jpm12010093