Effectiveness of a Multicomponent Treatment for Fibromyalgia Based on Pain Neuroscience Education, Exercise Therapy, Psychological Support, and Nature Exposure (NAT-FM): A Pragmatic Randomized Controlled Trial

 , ,
, ,  , , ,
, , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
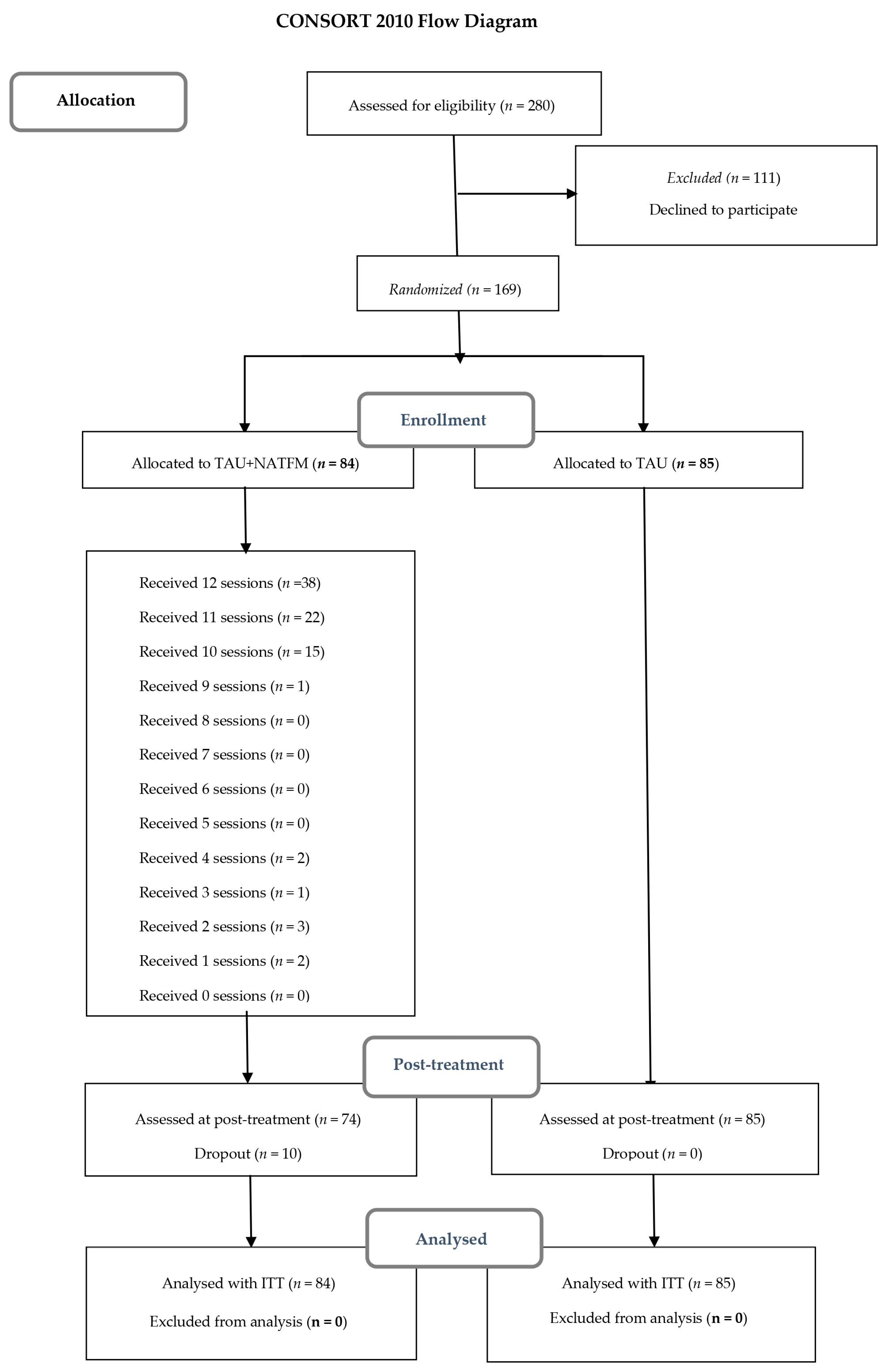
2.1. Design
2.2. Participants
2.3. Procedure
2.4. Study Arms
2.4.1. TAU + NAT-FM
2.4.2. TAU
2.5. Outcome Measures
2.5.1. Classical Structural Assessment (CSA) at Specific Time Points
Primary Outcome
Secondary Outcomes
Process Variables
2.5.2. Ecological Momentary Assessment (EMA)
2.6. Statistical Analysis
3. Results
3.1. Baseline Sociodemographic and Clinical Characteristics of the Groups
3.2. Effects on Functional Impairment (Primary Outcome)
3.3. Effects on Pain, Fatigue, Anxiety-Depression, Physical Functioning, Positive and Negative Affect, Self-Esteem, and Perceived Stress (Secondary Outcomes)
3.4. Effects on Kinesiophobia, Pain Catastrophizing, Personal Perceived Competence, and Cognitive Emotion Regulation (Process Variables)
3.5. Number Needed to Treat
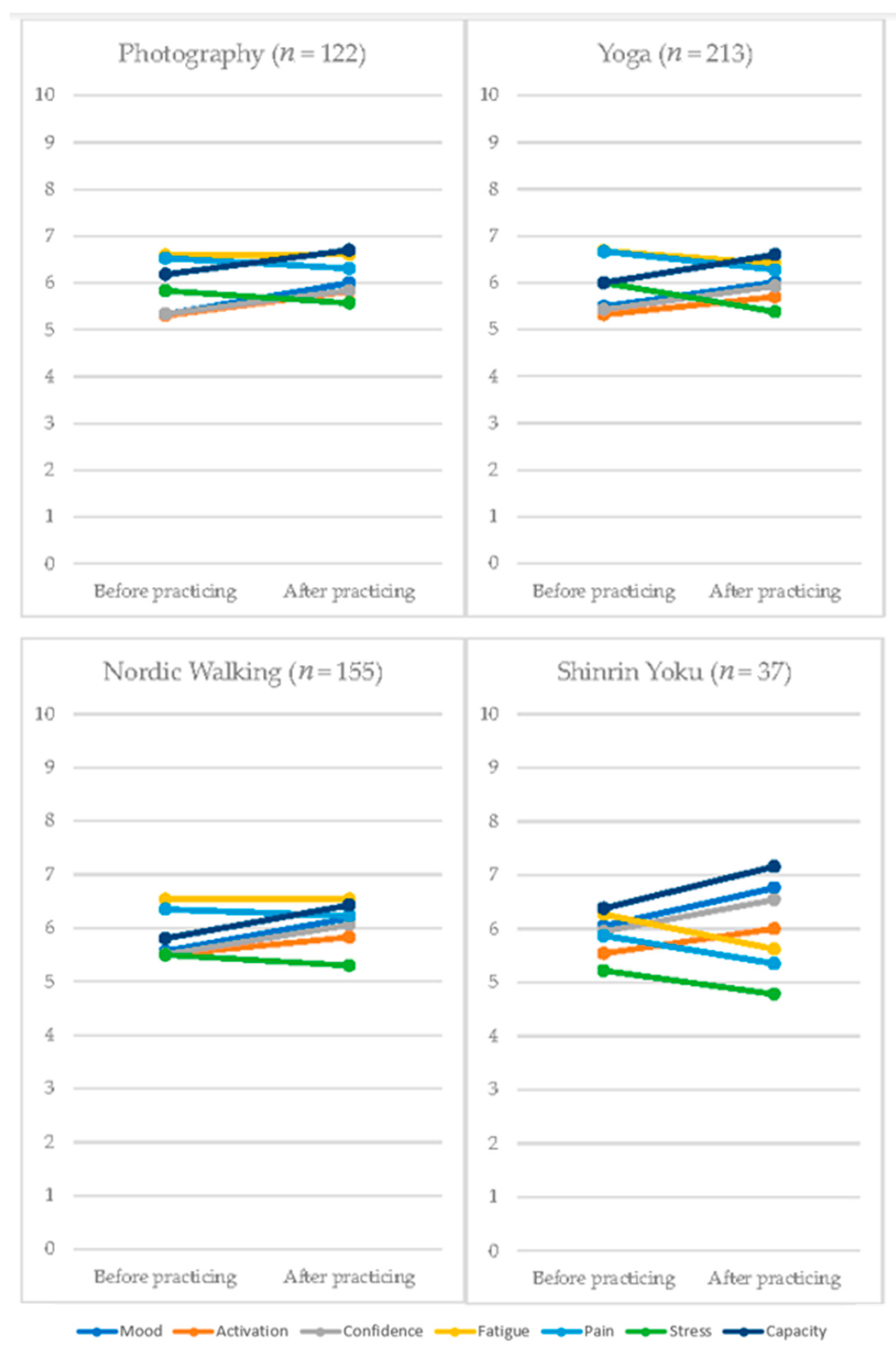
3.6. Effects of the Different Activities Included in TAU + NAT-FM Treatment: Intra-Session Assessments (EMA)
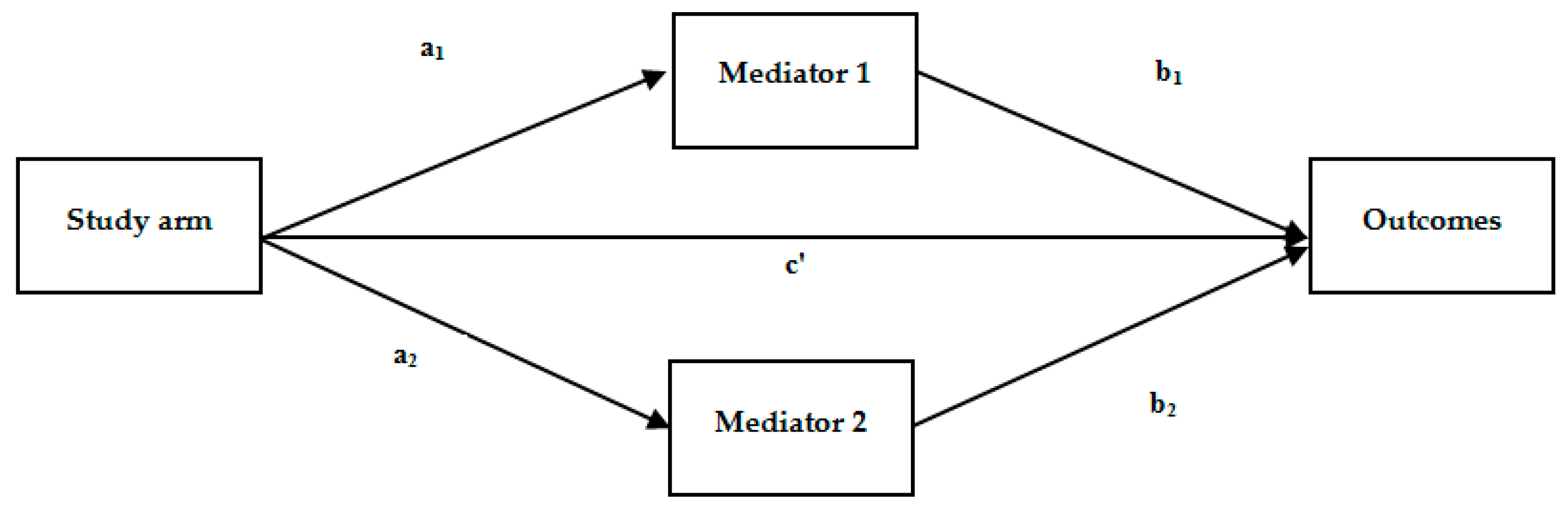
3.7. The Role of Kinesiophobia, Pain Catastrophism, Perceived Competence, and Cognitive Emotion Regulation Strategies as Treatment Mediators
4. Discussion
Limitations and Strengths of This Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Gayà, T.F.; Ferrer, C.B.; Mas, A.J.; Seoane-Mato, D.; Reyes, F.Á.; Sánchez, M.D.; Dubois, C.M.; Sánchez-Fernández, A.S.; Vargas, L.M.R.; Morales, P.V.G.; et al. Prevalence of fibromyalgia and associated factors in Spain. Proyecto EPISER2016. Clin. Exp. Rheumatol 2020, 38, 47–52. [Google Scholar]
- Gormsen, L.; Rosenberg, R.; Bach, F.W.; Jensen, T.S. Depression, anxiety, health-related quality of life and pain in patients with chronic fibromyalgia and neuropathic pain. Eur. J. Pain 2010, 14, e1–e8. [Google Scholar] [CrossRef]
- Häuser, W.; Ablin, J.; Fitzcharles, M.-A.; Littlejohn, G.; Luciano, J.V.; Usui, C.; Walitt, B. Fibromyalgia. Nat. Rev. Dis. Prim. 2015, 1, 15022. [Google Scholar] [CrossRef]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.-A.; Goldenberg, D.L.; Häuser, W.; Katz, R.L.; Mease, P.J.; Russell, A.S.; Russell, I.J.; Walitt, B. 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin. Arthritis Rheum. 2016, 46, 319–329. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, F.; Walitt, B.; Perrot, S.; Rasker, J.J.; Häuser, W. Fibromyalgia diagnosis and biased assessment: Sex, prevalence and bias. PLoS ONE 2018, 13, e0203755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaefer, C.; Chandran, A.; Hufstader, M.; Baik, R.; McNett, M.; Goldenberg, D.; Gerwin, R.; Zlateva, G. The comparative burden of mild, moderate and severe Fibromyalgia: Results from a cross-sectional survey in the United States. Health Qual. Life Outcomes 2011, 9, 71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Staud, R. The Role of Peripheral Input for Chronic Pain Syndromes like Fibromyalgia Syndrome. J. Musculoskelet. Pain 2008, 16, 67–74. [Google Scholar] [CrossRef]
- Woolf, C.J. Central sensitization: Implications for the diagnosis and treatment of pain. Pain 2011, 152, S2–S15. [Google Scholar] [CrossRef]
- Harte, S.E.; Harris, R.E.; Clauw, D.J. The neurobiology of central sensitization. J. Appl. Biobehav. Res. 2018, 23, e12137. [Google Scholar] [CrossRef] [Green Version]
- Nijs, J.; Van Houdenhove, B.; Oostendorp, R.A. Recognition of central sensitization in patients with musculoskeletal pain: Application of pain neurophysiology in manual therapy practice. Man. Ther. 2010, 15, 135–141. [Google Scholar] [CrossRef]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.-A.; Goldenberg, D.L.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B.; Yunus, M.B. The American College of Rheumatology Preliminary Diagnostic Criteria for Fibromyalgia and Measurement of Symptom Severity. Arthritis Care Res. (Hoboken) 2010, 62, 600–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feliu-Soler, A.; Borràs, X.; Peñarrubia-María, M.; Rozadilla-Sacanell, A.; D’Amico, F.; Moss-Morris, R.; Howard, M.; Fayed, N.; Soriano-Mas, C.; Puebla-Guedea, M.; et al. Cost-utility and biological underpinnings of Mindfulness-Based Stress Reduction (MBSR) versus a psychoeducational programme (FibroQoL) for fibromyalgia: A 12-month randomised controlled trial (EUDAIMON study). BMC Complement. Altern. Med. 2016, 16, 81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haugmark, T.; Hagen, K.B.; Provan, S.A.; Bærheim, E.; Zangi, H.A. Effects of a community-based multicomponent rehabilitation programme for patients with fibromyalgia: Protocol for a randomised controlled trial. BMJ Open 2018, 8, 021004. [Google Scholar]
- Häuser, W.; Ablin, J.; Perrot, S.; Fitzcharles, M.-A. Management of fibromyalgia: Practical guides from recent evidence-based guidelines. Pol. Arch. Intern. Med. 2017, 127, 47–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pérez-Aranda, A.; Feliu-Soler, A.; Montero-Marín, J.; García-Campayo, J.; Andrés-Rodríguez, L.; Borràs, X.; Rozadilla-Sacanell, M.; Peñarrubia-Mari, T.; Angarita-Osorio, N.; McCracken, L.M.; et al. A randomized controlled efficacy trial of Mindfulness-Based Stress Reduction compared to an active control group and usual care for fibromyalgia: The EUDAIMON study. Pain 2019, 160, 2508–2523. [Google Scholar] [CrossRef]
- De Miquel, C.A.; Campayo, J.G.; Flórez, M.T.; Arguelles, J.M.G.; Tarrio, E.B.; Montoya, M.G.; Martin, Á.P.; Salio, A.M.; Fuentes, J.V.; Alberch, E.A.; et al. Interdisciplinary consensus document for the treatment of fibromyalgia. Actas Esp. Psiquiatr. 2011, 38, 108–120. [Google Scholar]
- Häuser, W.; Bernardy, K.; Arnold, B.; Offenbächer, M.; Schiltenwolf, M. Efficacy of multicomponent treatment in fibromyalgia syndrome: A meta-analysis of randomized controlled clinical trials. Arthritis Rheum. 2009, 61, 216–224. [Google Scholar] [CrossRef]
- Macfarlane, G.J.; Kronisch, C.; Dean, L.E.; Atzeni, F.; Häuser, W.; Fluß, E.; Choy, E.; Kosek, E.; Amris, K.; Branco, J.; et al. EULAR revised recommendations for the management of fibromyalgia. Ann. Rheum. Dis. 2016, 76, 318–328. [Google Scholar] [CrossRef]
- Bernardy, K.; Klose, P.; Welsch, P.; Häuser, W. Efficacy, acceptability and safety of cognitive behavioural therapies in fibromyalgia syndrome—A systematic review and meta-analysis of randomized controlled trials. Eur. J. Pain 2018, 22, 242–260. [Google Scholar] [CrossRef] [Green Version]
- Galan-Martin, M.A.; Montero-Cuadrado, F.; Lluch-Girbes, E.; Coca-López, M.C.; Mayo-Iscar, A.; Cuesta-Vargas, A. Pain Neuroscience Education and Physical Exercise therapy for Patients with Chronic Spinal Pain in Spanish Physiotherapy Primary Care: A Pragmatic Randomized Controlled Trial. J. Clin. Med. 2020, 9, 1201. [Google Scholar] [CrossRef]
- Malfliet, A.; Van Oosterwijck, J.; Meeus, M.; Cagnie, B.; Danneels, L.; Dolphens, M.; Buyl, R.; Nijs, J. Kinesiophobia and maladaptive coping strategies prevent improvements in pain catastrophizing following pain neuroscience education in fibromyalgia/chronic fatigue syndrome: An explorative study. Physiother. Theory Pract. 2017, 33, 653–660. [Google Scholar] [CrossRef] [PubMed]
- McDowell, C.P.; Cook, D.B.; Herring, M.P. The Effects of Exercise Training on Anxiety in Fibromyalgia Patients: A Meta-analysis. Med. Sci. Sports Exerc. 2017, 49, 1868–1876. [Google Scholar] [CrossRef] [PubMed]
- Nishishinya, M.B.; Rivera, J.; Alegre, C.; Pereda, C.A. Non-pharmacologic and alternative treatments in fibromyalgia. Med. Clin. 2016, 127, 295–299. [Google Scholar] [CrossRef]
- Sharpe, L.; Jones, E.; Ashton-James, C.E.; Nicholas, M.K.; Refshauge, K. Necessary components of psychological treatment in pain management programs: A Delphi study. Eur. J. Pain 2020, 24, 1160–1168. [Google Scholar] [CrossRef]
- Sosa-Reina, M.D.; Núñez-Nagy, S.; Gallego-Izquierdo, T.; Pecos-Martín, D.; Monserrat, J.; Álvarez-Mon, M. Effectiveness of Exercise therapy in fibromyalgia syndrome: A systematic review and meta-analysis of randomized clinical trials. BioMed Res. Int. 2017, 2356346. [Google Scholar] [CrossRef]
- Pérez-Aranda, A.; D’Amico, F.; Feliu-Soler, A.; McCracken, L.M.; Peñarrubia-María, M.T.; Andrés-Rodríguez, L.; Luciano, J.V. Cost–Utility of Mindfulness-Based Stress Reduction for Fibromyalgia versus a Multicomponent Intervention and Usual Care: A 12-Month Randomized Controlled Trial (EUDAIMON Study). J. Clin. Med. 2019, 8, 1068. [Google Scholar] [CrossRef] [Green Version]
- Serrat, M.; Sanabria-Mazo, J.P.; Musté, M.; Soler, A.F.; Méndez-Ulrich, J.L.; Sanz, A.; Luciano, J.V.; Almirall, M. Effectiveness of a Multicomponent Treatment based on Pain Neuroscience Education, Therapeutic Exercise, Cognitive Behavioural Therapy, and Mindfulness in Patients with Fibromyalgia (FIBROWALK study): A Randomized Controlled Trial. PsyArXiv 2020. [Google Scholar] [CrossRef]
- Serrat, M.; Sanabria-Mazo, J.P.; García-Troiteiro, E.; Fontcuberta, A.; Mateo-Canedo, C.; Almirall, M.; Feliu-Soler, A.; Méndez-Ulrich, J.L.; Sanz, A.; Luciano, J.V. Efficacy of a Multicomponent Intervention for Fibromyalgia Based on Pain Neuroscience Education, Exercise Therapy, Psychological Support, and Nature Exposure (NAT-FM): Study Protocol of a Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2020, 17, 634. [Google Scholar] [CrossRef] [Green Version]
- Cole, H.; Triguero-Mas, M.; Connolly, J.J.; Anguelovski, I. Determining the health benefits of green space: Does gentrification matter? Health Place 2019, 57, 1–11. [Google Scholar] [CrossRef]
- Preuß, M.; Nieuwenhuijsen, M.; Márquez, S.; Cirach, M.; Dadvand, P.; Triguero-Mas, M.; Gidlow, C.; Grazuleviciene, R.; Kruize, H.; Zijlema, W.L. Low Childhood Nature Exposure is Associated with Worse Mental Health in Adulthood. Int. J. Environ. Res. Public Health 2019, 16, 1809. [Google Scholar] [CrossRef] [Green Version]
- Trøstrup, C.H.; Christiansen, A.B.; Stølen, K.S.; Nielsen, P.K.; Stelter, R. The effect of nature exposure on the mental health of patients: A systematic review. Qual. Life Res. 2019, 28, 1695–1703. [Google Scholar] [CrossRef]
- Zijlema, W.L.; Avila-Palencia, I.; Triguero-Mas, M.; Gidlow, C.; Maas, J.; Kruize, H.; Andrusaityte, S.; Grazuleviciene, R.; Nieuwenhuijsen, M.J. Active commuting through natural environments is associated with better mental health: Results from the PHENOTYPE project. Environ. Int. 2018, 121, 721–727. [Google Scholar] [CrossRef] [PubMed]
- Berman, M.G.; Kross, E.; Krpan, K.M.; Askren, M.K.; Burson, A.; Deldin, P.J.; Kaplan, S.; Sherdell, L.; Gotlib, I.H.; Jonides, J. Interacting with nature improves cognition and affect for individuals with depression. J. Affect. Disord. 2012, 140, 300–305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luttenberger, K.; Stelzer, E.-M.; Först, S.; Schopper, M.; Kornhuber, J.; Book, S. Indoor rock climbing (bouldering) as a new treatment for depression: Study design of a waitlist-controlled randomized group pilot study and the first results. BMC Psychiatry 2015, 15, 201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stanhope, J.; Breed, M.F.; Weinstein, P. Exposure to greenspaces could reduce the high global burden of pain. Environ. Res. 2020, 187, 109641. [Google Scholar] [CrossRef]
- López-Pousa, S.; Bassets Pagès, G.; Monserrat-Vila, S.; Blanco, M.D.G.; Colomé, J.H.; Garre-Olmo, J. Sense of Well-Being in Patients with Fibromyalgia: Aerobic Exercise Program in a Mature Forest—A Pilot Study. Evid.-Based Complement. Altern. Med. 2015, 2015, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Hofmann, S.G.; Hayes, S.C. The Future of Intervention Science: Process-Based Therapy. Clin. Psychol. Sci. 2019, 7, 37–59. [Google Scholar] [CrossRef]
- Sanabria-Mazo, J.P.; Serrat, M.; Canedo, C.M.; Soler, A.F.; Almirall, M.; Méndez-Ulrich, J.L.; Luciano, J.V.; Sanz, A. Proof of Concept of a Treatment for Fibromyalgia Based on Physical Activity, Psychological Support, and Exposure to Nature (NAT-FM). PsyArXiv. 2020. [Google Scholar] [CrossRef]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.J.; Elbourne, D.; Egger, M.; Altman, D.G. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomized trials. BMJ 2010, 340, c332. [Google Scholar] [CrossRef] [Green Version]
- Wolfe, F.; Smythe, H.A.; Yunus, M.B.; Bennett, R.M.; Bombardier, C.; Goldenberg, D.L.; Tugwell, P.; Campbell, S.M.; Abeles, M.; Clark, P.; et al. The american college of rheumatology. Criteria for the classification of fibromyalgia. Arthritis Rheum. 1990, 33, 160–172. [Google Scholar] [CrossRef]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.-A.; Goldenberg, D.L.; Häuser, W.; Katz, R.S.; Mease, P.J.; Russell, A.S.; Russell, I.J.; Winfield, J.B. Fibromyalgia Criteria and Severity Scales for Clinical and Epidemiological Studies: A Modification of the ACR Preliminary Diagnostic Criteria for Fibromyalgia. J. Rheumatol. 2011, 38, 1113–1122. [Google Scholar] [CrossRef]
- Segura-Jiménez, V.; Aparicio, V.A.; Álvarez-Gallardo, I.C.; Soriano-Maldonado, A.; Estévez-López, F.; Delgado-Fernández, M.; Carbonell-Baeza, A. Validation of the modified 2010 American College of Rheumatology diagnostic criteria for fibromyalgia in a Spanish population. Rheumatology (Oxford) 2014, 53, 1803–1811. [Google Scholar] [CrossRef] [Green Version]
- Bennett, R.M.; Friend, R.; Jones, K.D.; Ward, R.; Han, B.K.; Ross, R.L. The Revised Fibromyalgia Impact Questionnaire (FIQR): Validation and psychometric properties. Arthritis Res. Ther. 2009, 11, R120. [Google Scholar] [CrossRef] [Green Version]
- Luciano, J.V.; Aguado, J.; Serrano-Blanco, A.; Calandre, E.P.; Rodriguez-Lopez, C.M. Dimensionality, reliability, and validity of the Revised Fibromyalgia Impact Questionnaire in two Spanish samples. Arthritis Care Res. 2013, 65, 1682–1689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esteve-Vives, J.; Redondo, J.R.; Salvat, M.I.S.; Blanco, M.D.G.; De Miquel, C.A. Propuesta de una versión de consenso del Fibromyalgia Impact Questionnaire (FIQ) para la población española. Reumatol. Clin. 2007, 3, 21–24. [Google Scholar] [CrossRef]
- Salgueiro, M.; García-Leiva, J.M.; Ballesteros, J.; Hidalgo, J.; Molina, R.; Calandre, E.P. Validation of a Spanish version of the Revised Fibromyalgia Impact Questionnaire (FIQR). Health Qual. Life Outcomes 2013, 11, 132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herrero, M.J.; Blanch, J.; Peri, J.M.; De Pablo, J.; Pintor, L.; Bulbena, A. A validation study of the hospital anxiety and depression scale (HADS) in a Spanish population. Gen. Hosp. Psychiatry 2003, 25, 277–283. [Google Scholar] [CrossRef]
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36) (I). Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef]
- Alonso, J.; Prieto, L.; Antó, J.M. The Spanish version of the SF-36 Health Survey (the SF-36 health questionnaire): An instrument for measuring clinical results. Med. Clin. (Barc.) 1995, 104, 771–776. [Google Scholar]
- Watson, D.; Clark, L.A.; Tellegen, A. Development and validation of brief measures of positive and negative affect: The PANAS Scales. J. Person. Soc. Psych. 1998, 54, 1063–1070. [Google Scholar] [CrossRef]
- López, I.; Hervás, G.; Vázquez, C. Adaptación de la “Escala de afecto positivo y negativo” (PANAS) en una muestra general española. Behav. Psychol. 2015, 23, 529–548. [Google Scholar]
- Rosenberg, M. Society and the Adolescent Self-Image; Princeton University Press: Princeton, NJ, USA, 1965. [Google Scholar]
- Vázquez, A.J.; Vázquez, R. Escala de autoestima de Rosenberg: Fiabilidad y validez en población clínica española. Apuntes Psicol. 2004, 22, 247–255. [Google Scholar]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A Global Measure of Perceived Stress. J. Health Soc. Behav. 1983, 24, 385. [Google Scholar] [CrossRef]
- Pedrero, E.J.; Ruiz, J.M.; Lozoya, P.; Rojo, G.; Llanero, M.; Puerta, C. La “Escala de Estrés Percibido”: Estudio psicométrico sin restricciones en población no clínica y adictos a sustancias en tratamiento. Behav. Psychol. 2015, 23, 305–324. [Google Scholar]
- Kori, S.H.; Miller, R.P.; Todd, D.D. Kinesiophobia: A new view of chronic pain behavior. Pain Manag. 1990, 3, 35–43. [Google Scholar]
- Gómez-Pérez, L.; López-Martínez, A.E.; Ruíz-Párraga, G.T. Psychometric Properties of the Spanish Version of the Tampa Scale for Kinesiophobia (TSK). J. Pain 2011, 12, 425–435. [Google Scholar] [CrossRef]
- Sullivan, M.J.L.; Bishop, S.; Pivik, J. The Pain Catastrophizing Scale: Development and validation. Psychol. Assess. 1995, 7, 524–532. [Google Scholar] [CrossRef]
- García, J.; Rodero, B.; Alda, M.; Sobradiela, N.; Montero, J.; Moreno, S. Validación de la versión española de la escala de la catastrofización ante el dolor (Pain Catastrophizing Scale) en la fibromialgia. Med. Clín. 2008, 131, 487–492. [Google Scholar]
- Wallston, K.A. Hocus-pocus, the focus isn’t strictly on locus: Rotter’s social learning theory modified for health. Cogn. Ther. Res. 1992, 16, 183–199. [Google Scholar] [CrossRef]
- Fernández, J.; Doval, E.; Blasco, T.; Álvarez, M.; Sanz, A. Validación de la Escala de Competencia Personal de Wallston: Implicaciones para el estudio del estrés. Ans. Est. 1998, 4, 31–41. [Google Scholar]
- Garnefski, N.; Kraaij, V.; Spinhoven, P. Negative life events, cognitive emotion regulation and emotional problems. Pers. Individ. Differ. 2001, 30, 1311–1327. [Google Scholar] [CrossRef]
- Feliu-Soler, A.; Reche-Camba, E.; Borràs, X.; Pérez-Aranda, A.; Andrés-Rodríguez, L.; Peñarrubia-María, M.T.; Navarro-Gil, M.; García-Campayo, J.; Bellón, J.A.; Luciano, J.V. Psychometric Properties of the Cognitive Emotion Regulation Questionnaire (CERQ) in Patients with Fibromyalgia Syndrome. Front. Psychol. 2017, 8. [Google Scholar] [CrossRef] [Green Version]
- Shiffman, S.; Stone, A.A.; Hufford, M.R. Ecological Momentary assessment. Annu. Rev. Clin. Psychol. 2008, 4, 1–32. [Google Scholar] [CrossRef]
- Csikszentmihalyi, M. Validity and Reliability of the Experience-Sampling Method; Springer: New York, NY, USA, 2014; p. 322. ISBN 978-94-017-9087-1. [Google Scholar]
- May, M.; Junghaenel, D.U.; Ono, M.; Stone, A.A.; Schneider, S. Ecological Momentary Assessment Methodology in Chronic Pain Research: A Systematic Review. J. Pain 2018, 19, 699–716. [Google Scholar] [CrossRef]
- Twisk, J.; De Boer, M.; De Vente, W.; Heymans, M. Multiple imputation of missing values was not necessary before performing a longitudinal mixed-model analysis. J. Clin. Epidemiol. 2013, 66, 1022–1028. [Google Scholar] [CrossRef]
- Morris, S.B. Estimating Effect Sizes From Pretest-Posttest-Control Group Designs. Organ. Res. Methods 2008, 11, 364–386. [Google Scholar] [CrossRef]
- Ollevier, A.; Vanneuville, I.; Carron, P.; Baetens, T.; Goderis, T.; Gabriel, L.; Van De Velde, D. A 12-week multicomponent therapy in fibromyalgia improves health but not in concomitant moderate depression, an exploratory pilot study. Disabil. Rehabil. 2019, 29, 1–8. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Review Phase (15 min) |
| • Comment on the duties of the previous session. |
| • Review of contents of the previous session. |
| Main Phase (1 h 40 min) |
| • 20 min Pain Neuroscience Education (PNE). |
| • 40 min Exercise therapy (TE) or Nature Activity (NA) or both (20 min each). |
| • 20 min Cognitive Behavioral Therapy (CBT). |
| • 20 min Mindfulness training (MT) |
| Sessions: |
| 1. PNE (1,2) + CBT (1) + MT (1) |
| 2. PNE (3,4) + TE (2) + CBT (2, 13–18) + MT (2) |
| 3. PNE (5,6) + TE (2) + CBT (3, 19–23) + MT (3) + NA (3) |
| 4. PNE (7,8) + TE (4) + CBT (4, 24–28) + MT (4) |
| 5. PNE (9,10) + TE (4) + CBT (5, 15–28) + MT (5) + NA (3) |
| 6. PNE (11) + TE (2) + CBT (6, 29–34) + MT (6) + TE (4) |
| 7. PNE (12) + TE (4) + CBT (7,8, 35–40) + MT (7,8) + NA (5) |
| 8. PNE (13) + TE (4) + CBT (9, 41–44) + MT (9) + NA (3) |
| 9. PNE (14) + TE (2) + CBT (10, 45–48) + MT (10) |
| 10. Family Session (PNE 1–16) + NA (3) |
| 11. PNE (15) + TE (4) + CBT (11, 47–48) + MT (11) + NA (5) |
| 12. PNE (16) + TE (4) + CBT (12, 18, 28, 34, 40, 48) + MT (12) |
| Homework (5 min) |
| • TE (1): first month once per week, second month twice per week, and third month three times per week. • Cognitive (related to CBT and MT) and physical tasks to do at home to increase the patient’s resistance involving a constant challenge for them. |
| Pain Neuroscience Education (PNE) |
|
| Exercise Therapy (TE)/Nature Activities (NA) Used to Work the Cognitive Targets |
|
| Cognitive Behavioral Therapy (CBT) |
General Issues:
Positive affect
|
| Mindfulness Training (MT) |
|
| TAU + NAT-FM (n = 84) | TAU (n = 85) | t/χ2 | p | |
|---|---|---|---|---|
| General measures | ||||
| Gender, n of women (%) | 82 (97.60) | 85 (100) | 0.74 | 0.39 |
| Age, M (SD) | 54.12 (8.62) | 53.15 (9.06) | 0.32 | 0.57 |
| BMI (kg/m2), M (SD) | 27.65 (5.49) | 26.75 (5.75) | 0.48 | 0.62 |
| Years of illness, M (SD) | 19.61 (11.99) | 16.75 (9.74) | 2.92 | 0.08 |
| Married or in couple, n (%) | 57 (67.8) | 43 (50.6) | 10.41 | 0.34 |
| Cohabitating, n (%) | 38 (44.2) | 69 (81.2) | 1.84 | 0.39 |
| Secondary studies, n (%) | 38 (45.3) | 46 (54.7) | 7.45 | 0.15 |
| Labor assets, n (%) | 43 (52.0) | 40 (48.0) | 18.52 | 0.09 |
| Accreditation of disability in process, n (%) | 30 (36.0) | 54 (64.0) | 1.13 | 0.29 |
| Comorbidity with CSS, f (%) | ||||
| Chronic fatigue | 71 (84.6) | 72 (85.3) | 0.32 | 0.59 |
| Multiple chemical sensitivity | 30 (35.8) | 25 (29) | 1.72 | 0.17 |
| Irritable bowel syndrome | 38 (45.9) | 39 (46.3) | 0.08 | 0.70 |
| Migraines | 50 (59) | 49 (57.8) | 0.07 | 0.92 |
| Medication, f (%) | ||||
| Mix of more than two medications | 27 (32.9) | 41 (47.7) | 4.71 | 0.41 |
| TAU M (SD) | TAU + NAT-FM M (SD) | TAU vs. NAT-FM | |||
|---|---|---|---|---|---|
| d | t (p) | B (95% CI) | |||
| Primary outcome | |||||
| FIQR (0–100) * | |||||
| Baseline | 73.21 (14.72) | 73.07 (13.79) | |||
| 6 weeks | 69.68 (13.36) | 58.78 (18.70) | 1.13 | −5.29 (<0.001) | −10.96 (−15.04 to −6.88) |
| Post−treatment | 69.18 (17.88) | 50.69 (18.05) | 1.83 | −8.16 (<0.001) | −18.07 (−22.43 to −13.72) |
| Secondary outcomes | |||||
| VAS PAIN (0–10) * | |||||
| Baseline | 7.80 (1.61) | 7.74 (1.52) | |||
| 6 weeks | 7.52 (1.59) | 6.78 (1.99) | 0.66 | −3.02 (0.003) | −0.77 (−1.28 to −0.27) |
| Post-treatment | 7.47 (1.79) | 5.60 (1.98) | 5.62 | −6.53 (<0.001) | −1.79 (−2.33 to −1.25) |
| VAS FATIGUE (0–10) * | |||||
| Baseline | 7.76 (1.91) | 7.61 (1.89) | |||
| 6 weeks | 7.32 (2.09) | 5.98 (2.10) | 0.77 | −3.10 (0.002) | −1.26 (−2.06 to −0.46) |
| Post-treatment | 7.08 (2.34) | 5.58 (2.00) | 0.93 | −3.87 (<0.001) | −1.53 (−2.31 to −0.75) |
| HADS-A (0–21) * | |||||
| Baseline | 13.13 (4.22) | 13.95 (3.80) | |||
| 6 weeks | 12.35 (4.07) | 11.03 (4.25) | 0.99 | −4.52 (<0.001) | −2.20 (−3.16 to −1.24) |
| Post-treatment | 12.68 (4.63) | 10.16 (4.19) | 1.59 | −7.08 (<0.001) | −3.51 (−4.48 to −2.53) |
| HADS-D (0–21) * | |||||
| Baseline | 11.49 (4.64) | 11.27 (3.71) | |||
| 6 weeks | 11.22 (5.02) | 9.66 (4.47) | 0.49 | −2.23 (0.027) | −1.10 (−2.07 to −0.13) |
| Post-treatment | 11.67 (5.18) | 8.18 (4.42) | 1.45 | −6.40 (<0.001) | −3.37 (−4.41 to −2.34) |
| SF-36 (0–100) * | |||||
| Baseline | 26.04 (18.11) | 27.03 (18.85) | |||
| 6 weeks | 28.24 (17.38) | 35.09 (20.47) | 0.53 | 2.41 (0.017) | 5.51 (1.00 to 10.02) |
| Post-treatment | 25.07 (15.86) | 43.42 (20.92) | 1.59 | 7.01 (<0.001) | 17.15 (12.34 to 21.96) |
| PANAS-PA (0–50) * | |||||
| Baseline | 12.26 (4.38) | 11.95 (5.79) | |||
| 6 weeks | 12.20 (4.30) | 12.81 (5.39) | 0.19 | 1.00 (0.319) | 0.79 (−0.77 to 2.35) |
| Post-treatment | 13.01 (4.03) | 14.11 (4.28) | 0.40 | 2.07 (0.039) | 1.68 (0.08 to 3.27) |
| PANAS-NA (0–50) * | |||||
| Baseline | 14.34 (5.81) | 13.84 (6.08) | |||
| 6 weeks | 13.94 (5.13) | 13.22 (4.83) | 0.13 | −0.37 (0.714) | −0.29 (−1.87 to 1.28) |
| Post-treatment | 14.95 (4.50) | 13.12 (4.24) | 0.28 | −1.38 (0.167) | −1.14 (−2.75 to 0.48) |
| RSES (10–40) * | |||||
| Baseline | 15.41 (3.57) | 16.03 (3.36) | |||
| 6 weeks | 15.48 (2.57) | 16.60 (2.70) | 0.37 | 1.23 (0.219) | 0.68 (−0.40 to 1.75) |
| Post-treatment | 16.25 (3.45) | 16.53 (2.25) | 0.03 | −0.24 (0.809) | −0.13 (−1.20 to 0.94) |
| PSS (0–16) * | |||||
| Baseline | 8.88 (2.15) | 8.93 (2.31) | |||
| 6 weeks | 8.81 (1.90) | 7.91 (1.87) | 0.43 | −1.88 (0.062) | −0.77 (−1.57 to 0.04) |
| Post-treatment | 8.88 (2.20) | 8 (1.87) | 0.37 | −1.66 (0.098) | −0.67 (−1.47 to 0.12) |
| TAU M (SD) | TAU+NAT-FM M (SD) | TAU vs. TAU+NAT-FM | |||
|---|---|---|---|---|---|
| d | t (p) | B (95% CI) | |||
| TSK (11–44) * | |||||
| Baseline | 29.92 (7.58) | 29.23 (7.40) | |||
| 6 weeks | 25.59 (6.46) | 21.36 (6.83) | 1.18 | −5.35 (<0.001) | −4.73 (−6.47 to −2.98) |
| Post-treatment | 28 (7.44) | 17.95 (4.97) | 2.2 | −9.65 (<0.001) | −9.15 (−11.01 to −7.28) |
| PCS (0–52) * | |||||
| Baseline | 27.72 (12.65) | 27.04 (11.33) | |||
| 6 weeks | 26.72 (13.25) | 17.83 (9.56) | 1.21 | −5.53 (<0.001) | −7.30 (−9.90 to −4.70) |
| Post-treatment | 27.49 (13.35) | 13.53 (8.87) | 2.03 | −8.93 (<0.001) | −12.56 (−15.33 to −9.80) |
| PPCS | |||||
| Baseline | 25.05 (7.84) | 23.77 (7.98) | |||
| 6 weeks | 25.35 (8.22) | 27.50 (8.08) | 0.72 | 3.44 (0.001) | 3.73 (1.59 to 5.86) |
| Post-treatment | 24.57 (8.50) | 28.67 (8.62) | 1.2 | 5.47 (<0.001) | 6.17 (3.95 to 8.38) |
| CERQ Acceptance (0–20) * | |||||
| Baseline | 6.46 (2.33) | 6.19 (2.27) | |||
| 6 weeks | 6.28 (2.37) | 7.02 (2.12) | 0.47 | 2.28 (0.023) | 0.93 (0.13 to 1.73) |
| Post-treatment | 6.77 (2.28) | 7.47 (2.15) | 0.53 | 2.52 (0.012) | 1.04 (0.23 to 1.84) |
| CERQ Self-blame (0–20) * | |||||
| Baseline | 5.14 (2.39) | 4.47 (2.26) | |||
| 6 weeks | 4.63 (2.01) | 4.24 (2.09) | 0.12 | 1.14 (0.256) | 0.40 (−0.29 to 1.08) |
| Post-treatment | 4.43 (2.13) | 3.74 (1.96) | 0.14 | 0.03 (0.980) | 0.01 (−0.68 to 0.70) |
| CERQ Rumination (0–20) * | |||||
| Baseline | 6.45 (2.33) | 5.89 (2.11) | |||
| 6 weeks | 5.80 (2.21) | 5.36 (2.06) | 0.03 | 0.30 (0.763) | 0.11 (−0.60 to 0.82) |
| Post-treatment | 5.84 (2.48) | 4.70 (2.10) | 0.47 | −1.60 (0.110) | −0.59 (−1.32 to 0.13) |
| CERQ Refocusing (0–20) * | |||||
| Baseline | 4.48 (1.94) | 4.26 (1.92) | |||
| 6 weeks | 4.70 (1.99) | 5.19 (2.11) | 0.52 | 2.50 (0.013) | 0.80 (0.17 to 1.42) |
| Post-treatment | 4.77 (2.13) | 5.82 (2.20) | 0.99 | 4.49 (<0.001) | 1.47 (0.83 to 2.11) |
| CERQ Planning (0–20) * | |||||
| Baseline | 5.58 (2.11) | 5.41 (2.20) | |||
| 6 weeks | 5.63 (2.17) | 6.38 (2) | 0.58 | 2.71 (0.007) | 0.98 (0.27 to 1.70) |
| Post-treatment | 5.28 (2.23) | 6.40 (2.11) | 0.83 | 3.76 (<0.001) | 1.38 (0.65 to 2.11) |
| CERQ Positive reappraisal (0–20) * | |||||
| Baseline | 5.12 (2.11) | 4.96 (2.42) | |||
| 6 weeks | 4.80 (1.77) | 6.07 (2.26) | 0.92 | 4.17 (<0.001) | 1.44 (0.76 to 2.11) |
| Post-treatment | 4.67 (2.23) | 6.42 (2.28) | 1.42 | 6.27 (<0.001) | 2.19 (1.50 to 2.87) |
| CERQ Perspective (0–20) * | |||||
| Baseline | 5.45 (2.25) | 5.45 (2.23) | |||
| 6 weeks | 5.52 (2.08) | 6.03 (2.14) | 0.17 | 0.79 (0.431) | 0.27 (−0.40 to 0.93) |
| Post-treatment | 5.23 (1.95) | 6.46 (2.51) | 0.71 | 3.15 (0.002) | 1.12 (0.42 to 1.81) |
| CERQ Catastrophizing (0–20) * | |||||
| Baseline | 5.34 (2.37) | 5.27 (2.17) | |||
| 6 weeks | 4.87 (2.07) | 4.09 (1.83) | 0.47 | −2.04 (0.043) | −0.65 (−1.27 to −0.02) |
| Post-treatment | 5.04 (2.21) | 3.70 (1.72) | 0.85 | −3.64 (<0.001) | −1.18 (−1.82 to −0.54) |
| CERQ Blame others (0–20) * | |||||
| Baseline | 3.45 (2.16) | 3.42 (2.20) | |||
| 6 weeks | 3.20 (1.65) | 2.97 (1.62) | 0.14 | −1.23 (0.219) | −0.34 (−0.88 to 0.20) |
| Post-treatment | 3.20 (1.70) | 3.02 (1.72) | 0.11 | −0.50 (0.620) | −0.14 (−0.69 to 0.41) |
| Outcome and Mediators (R2) | Direct Effects | Indirect Effects | ||||||
|---|---|---|---|---|---|---|---|---|
| Path | Coeff. | SE | p | Path | Boot. | SE | 95% CI | |
| FIQR (0.48) | ||||||||
| M1 = TSK (0.17) | a1 | −5.39 | 1.21 | <0.001 | a1 × b1 | −4.10 | 1.29 | −7.22 to −2.06 |
| a2 | 7.50 | 1.46 | <0.001 | |||||
| M2 = PPCS (0.21) | b1 | 0.76 | 0.19 | <0.001 | a2 × b2 | −4.23 | 1.83 | −8.39 to −1.25 |
| b2 | −0.56 | 0.19 | 0.002 | |||||
| c’ | −9.76 | 2.79 | <0.001 | |||||
| VAS Pain (0.30) | ||||||||
| M1 = TSK (0.17) | a1 | −5.39 | 1.19 | <0.001 | a1 × b1 | −0.44 | 0.19 | −0.89 to −0.13 |
| a2 | 7.50 | 1.46 | <0.001 | |||||
| M2 = PPCS (0.21) | b1 | 0.08 | 0.03 | 0.008 | a2 × b2 | −0.38 | 0.19 | −0.82 to −0.07 |
| b2 | −0.05 | 0.02 | 0.010 | |||||
| c’ | −1.00 | 0.39 | 0.010 | |||||
| VAS Fatigue (0.20) | ||||||||
| M1 = TSK (0.17) | a1 | −5.39 | 1.18 | <0.001 | a1 × b1 | −0.64 | 0.22 | −1.16 to −0.29 |
| b1 | 0.12 | 0.04 | 0.004 | |||||
| c’ | −0.76 | 0.49 | 0.120 | |||||
| HADS Anxiety (0.41) | ||||||||
| M1 = TSK (0.17) | a1 | −5.39 | 1.19 | <0.001 | a1 × b1 | −0.56 | 0.29 | −1.28 to −0.11 |
| a2 | 7.50 | 1.46 | <0.001 | |||||
| M2 = PPCS (0.21) | b1 | 0.10 | 0.05 | 0.022 | a2 × b2 | −1.31 | 0.50 | −2.54 to −0.54 |
| b2 | −0.17 | 0.05 | <0.001 | |||||
| c’ | −1.39 | 0.58 | 0.017 | |||||
| HADS Depression (0.37) | ||||||||
| M1 = TSK (0.17) | a1 | −5.39 | 1.21 | <0.001 | a1 × b1 | −0.70 | 0.29 | −1.40 to −0.23 |
| a2 | 5.40 | 1.45 | <0.001 | |||||
| M2 = PPCS (0.21) | b1 | 0.13 | 0.05 | 0.008 | a2 × b2 | −1.17 | 0.57 | −2.47 to −0.28 |
| b2 | −0.16 | 0.06 | 0.011 | |||||
| c’ | −1.60 | 0.83 | 0.055 | |||||
| SF36 (0.40) | ||||||||
| M1 = TSK (0.17) | a1 | −5.39 | 1.19 | <0.001 | a1 × b1 | 3.06 | 1.63 | 0.48 to 7.09 |
| a2 | 7.50 | 1.46 | <0.001 | |||||
| M2 = PPCS (0.21) | b1 | −0.57 | 0.27 | 0.036 | a2 × b2 | 4.47 | 1.84 | 1.59 to 8.92 |
| b2 | 0.60 | 0.20 | 0.003 | |||||
| c’ | 10.57 | 3.07 | 0.001 | |||||
| PANAS—(0.12) | ||||||||
| M1 = PPCS (0.21) | a1 | 7.50 | 1.47 | <0.001 | a1 × b1 | −1.43 | 0.53 | −2.60 to −0.49 |
| b1 | −0.19 | 0.06 | 0.003 | |||||
| c’ | 0.98 | 1.06 | 0.355 | |||||
| RSES (0.06) | ||||||||
| M1 = CERQ Positive Reappraisal (0.17) | a1 | 1.91 | 0.41 | <0.001 | a1 × b1 | −0.66 | 0.34 | −1.45 to −0.09 |
| b1 | −0.35 | 0.17 | 0.040 | |||||
| c’ | 0.41 | 0.67 | 0.539 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Serrat, M.; Almirall, M.; Musté, M.; Sanabria-Mazo, J.P.; Feliu-Soler, A.; Méndez-Ulrich, J.L.; Luciano, J.V.; Sanz, A. Effectiveness of a Multicomponent Treatment for Fibromyalgia Based on Pain Neuroscience Education, Exercise Therapy, Psychological Support, and Nature Exposure (NAT-FM): A Pragmatic Randomized Controlled Trial. J. Clin. Med. 2020, 9, 3348. https://doi.org/10.3390/jcm9103348
Serrat M, Almirall M, Musté M, Sanabria-Mazo JP, Feliu-Soler A, Méndez-Ulrich JL, Luciano JV, Sanz A. Effectiveness of a Multicomponent Treatment for Fibromyalgia Based on Pain Neuroscience Education, Exercise Therapy, Psychological Support, and Nature Exposure (NAT-FM): A Pragmatic Randomized Controlled Trial. Journal of Clinical Medicine. 2020; 9(10):3348. https://doi.org/10.3390/jcm9103348
Chicago/Turabian StyleSerrat, Mayte, Míriam Almirall, Marta Musté, Juan P. Sanabria-Mazo, Albert Feliu-Soler, Jorge L. Méndez-Ulrich, Juan V. Luciano, and Antoni Sanz. 2020. "Effectiveness of a Multicomponent Treatment for Fibromyalgia Based on Pain Neuroscience Education, Exercise Therapy, Psychological Support, and Nature Exposure (NAT-FM): A Pragmatic Randomized Controlled Trial" Journal of Clinical Medicine 9, no. 10: 3348. https://doi.org/10.3390/jcm9103348