Severe Fatigue is Highly Prevalent in Patients with IPF or Sarcoidosis

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Measures
2.2.1. Fatigue
2.2.2. Medical Information
2.2.3. Demographic Data
2.2.4. Symptom and Limitation Measures
2.2.5. Psychological Measures
2.2.6. Health Status
2.3. Statistical Analyses
3. Results
3.1. Patient Characteristics
3.2. Prevalence of Severe Fatigue
3.3. Factors Associated with Severe Fatigue in Patients with IPF
3.4. Factors Associated with Severe Fatigue in Patients with Sarcoidosis
3.5. Correlations of Fatigue
3.6. Determinants of Functional Impairment QoL-RIQ/Activity
4. Discussion
4.1. Severe Fatigue in Patients with IPF or Sarcoidosis
4.2. Factors Associated with Fatigue in Patients with IPF or Sarcoidosis
4.3. Limitations and Strength
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bradley, B.; Branley, H.M.; Egan, J.J.; Greaves, M.S.; Hansell, D.M.; Harrison, N.K.; Hirani, N.; Hubbard, R.; Lake, F.; Millar, A.B.; et al. Interstitial lung disease guideline: The British Thoracic Society in collaboration with the Thoracic Society of Australia and New Zealand and the Irish Thoracic Society. Thorax 2008, 63 (Suppl. 5), v1–v58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Travis, W.D.; Costabel, U.; Hansell, D.M.; King, T.E., Jr.; Lynch, D.A.; Nicholson, A.G.; Ryerson, C.J.; Ryu, J.H.; Selman, M.; Wells, A.U.; et al. An official American Thoracic Society/European Respiratory Society statement: Update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am. J. Respir. Crit. Care Med. 2013, 188, 733–748. [Google Scholar] [CrossRef] [PubMed]
- Landmark-Hoyvik, H.; Reinertsen, K.V.; Loge, J.H.; Kristensen, V.N.; Dumeaux, V.; Fossa, S.D.; Borresen-Dale, A.L.; Edvardsen, H. The genetics and epigenetics of fatigue. PM R. 2010, 2, 456–465. [Google Scholar] [CrossRef] [PubMed]
- Swigris, J.J.; Brown, K.K.; Abdulqawi, R.; Buch, K.; Dilling, D.F.; Koschel, D.; Thavarajah, K.; Tomic, R.; Inoue, Y. Patients’ perceptions and patient-reported outcomes in progressive-fibrosing interstitial lung diseases. Eur. Respir. Rev. 2018, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atkins, C.; Wilson, A.M. Managing fatigue in sarcoidosis—A systematic review of the evidence. Chron. Respir. Dis. 2017, 14, 161–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, O.P. Fatigue and sarcoidosis. Eur. Respir. J. 1999, 13, 713–714. [Google Scholar] [CrossRef] [Green Version]
- U.S. Food and Drug Administration’s. A series of reports from the U.S. Food and Drug Administration’s (FDA’s) Patient-Focused Drug Development Initiative. In Proceedings of the Idiopathic Pulmonary Fibrosis Public Meeting, Silver Spring, MD, USA, 26 September 2014; Available online: http://www.fda.gov/downloads/ForIndustry/UserFees/PrescriptionDrugUserFee/UCM440829.pdf (accessed on 14 January 2017).
- Voortman, M.; Hendriks, C.M.R.; Elfferich, M.D.P.; Bonella, F.; Moller, J.; De Vries, J.; Costabel, U.; Drent, M. The Burden of Sarcoidosis Symptoms from a Patient Perspective. Lung 2019, 197, 155–161. [Google Scholar] [CrossRef] [Green Version]
- Korenromp, I.H.E.; Heijnen, C.J.; Vogels, O.J.M.; van den Bosch, J.M.M.; Grutters, J.C. Characterization of chronic fatigue in patients with sarcoidosis in clinical remission. Chest 2011, 140, 441–447. [Google Scholar] [CrossRef]
- Michielsen, H.J.; Drent, M.; Peros-Golubicic, T.; De Vries, J. Fatigue is associated with quality of life in sarcoidosis patients. Chest 2006, 130, 989–994. [Google Scholar] [CrossRef] [Green Version]
- Holland, A.E.; Hill, C.J.; Conron, M.; Munro, P.; McDonald, C.F. Short term improvement in exercise capacity and symptoms following exercise training in interstitial lung disease. Thorax 2008, 63, 549–554. [Google Scholar] [CrossRef] [Green Version]
- Swigris, J.J.; Fairclough, D.L.; Morrison, M.; Make, B.; Kozora, E.; Brown, K.K.; Wamboldt, F.S. Benefits of pulmonary rehabilitation in idiopathic pulmonary fibrosis. Respir. Care 2011, 56, 783–789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kentson, M.; Todt, K.; Skargren, E.; Jakobsson, P.; Ernerudh, J.; Unosson, M.; Theander, K. Factors associated with experience of fatigue, and functional limitations due to fatigue in patients with stable COPD. Ther. Adv. Respir. Dis. 2016, 10, 410–424. [Google Scholar] [CrossRef] [PubMed]
- Bosse-Henck, A.; Koch, R.; Wirtz, H.; Hinz, A. Fatigue and Excessive Daytime Sleepiness in Sarcoidosis: Prevalence, Predictors, and Relationships between the Two Symptoms. Respiration 2017, 94, 186–197. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.; Teoh, A.; Roberts, M.; Wheatley, J. The prevalence of poor sleep quality and its associated factors in patients with interstitial lung disease: A cross-sectional analysis. ERJ Open Res. 2019, 5, 00062-2019. [Google Scholar] [CrossRef]
- Ito, E.; Inoue, Y. The International Classification of Sleep Disorders, third edition. American Academy of Sleep Medicine. Includes bibliographies and index. Nihon Rinsho. 2015, 73, 916–923. [Google Scholar]
- Fleischer, M.; Hinz, A.; Brahler, E.; Wirtz, H.; Bosse-Henck, A. Factors associated with fatigue in sarcoidosis. Respir. Care 2014, 59, 1086–1094. [Google Scholar] [CrossRef] [Green Version]
- Oltmanns, U.; Kahn, N.; Palmowski, K.; Trager, A.; Wenz, H.; Heussel, C.P.; Schnabel, P.A.; Puderbach, M.; Wiebel, M.; Ehlers-Tenenbaum, S.; et al. Pirfenidone in idiopathic pulmonary fibrosis: Real-life experience from a German tertiary referral center for interstitial lung diseases. Respiration 2014, 88, 199–207. [Google Scholar] [CrossRef]
- Spruit, M.A.; Vercoulen, J.H.; Sprangers, M.A.G.; Wouters, E.F.M. FAntasTIGUE consortium Fatigue in COPD: An important yet ignored symptom. Lancet Respir. Med. 2017, 5, 542–544. [Google Scholar] [CrossRef]
- Raghu, G.; Collard, H.R.; Egan, J.J.; Martinez, F.J.; Behr, J.; Brown, K.K.; Colby, T.V.; Cordier, J.F.; Flaherty, K.R.; Lasky, J.A.; et al. An official ATS/ERS/JRS/ALAT statement: Idiopathic pulmonary fibrosis: Evidence-based guidelines for diagnosis and management. Am. J. Respir. Crit. Care Med. 2011, 183, 788–824. [Google Scholar] [CrossRef]
- Hunninghake, G.W.; Costabel, U.; Ando, M.; Baughman, R.; Cordier, J.F.; du Bois, R.; Eklund, A.; Kitaichi, M.; Lynch, J.; Rizzato, G.; et al. ATS/ERS/WASOG statement on sarcoidosis. American Thoracic Society/European Respiratory Society/World Association of Sarcoidosis and other Granulomatous Disorders. Sarcoidosis Vasc. Diffuse Lung Dis. 1999, 16, 149–173. [Google Scholar]
- Zhou, Y.; Lower, E.E.; Li, H.; Baughman, R.P. Clinical management of pulmonary sarcoidosis. Expert Rev. Respir. Med. 2016, 10, 577–591. [Google Scholar] [CrossRef] [PubMed]
- Vercoulen, J.H.; Swanink, C.M.; Fennis, J.F.; Galama, J.M.; van der Meer, J.W.; Bleijenberg, G. Dimensional assessment of chronic fatigue syndrome. J. Psychosom. Res. 1994, 38, 383–392. [Google Scholar] [CrossRef] [Green Version]
- Beurskens, A.J.; Bultmann, U.; Kant, I.; Vercoulen, J.H.; Bleijenberg, G.; Swaen, G.M. Fatigue among working people: Validity of a questionnaire measure. Occup. Environ. Med. 2000, 57, 353–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bultmann, U.; de Vries, M.; Beurskens, A.J.; Bleijenberg, G.; Vercoulen, J.H.; Kant, I. Measurement of prolonged fatigue in the working population: Determination of a cutoff point for the checklist individual strength. J. Occup. Health Psychol. 2000, 5, 411–416. [Google Scholar] [CrossRef] [PubMed]
- Worm-Smeitink, M.; Gielissen, M.; Bloot, L.; van Laarhoven, H.W.M.; van Engelen, B.G.M.; van Riel, P.; Bleijenberg, G.; Nikolaus, S.; Knoop, H. The assessment of fatigue: Psychometric qualities and norms for the Checklist individual strength. J. Psychosom. Res. 2017, 98, 40–46. [Google Scholar] [CrossRef]
- Quanjer, P.H.; Tammeling, G.J.; Cotes, J.E.; Pedersen, O.F.; Peslin, R.; Yernault, J.C. Lung volumes and forced ventilatory flows. Work Group on Standardization of Respiratory Function Tests. European Community for Coal and Steel. Official position of the European Respiratory Society. Rev. Mal. Respir. 1994, 11 (Suppl. 3), 5–40. [Google Scholar] [PubMed]
- Mahler, D.A.; Rosiello, R.A.; Harver, A.; Lentine, T.; McGovern, J.F.; Daubenspeck, J.A. Comparison of clinical dyspnea ratings and psychophysical measurements of respiratory sensation in obstructive airway disease. Am. Rev. Respir. Dis. 1987, 135, 1229–1233. [Google Scholar] [CrossRef]
- Mahler, D.A.; Wells, C.K. Evaluation of clinical methods for rating dyspnea. Chest 1988, 93, 580–586. [Google Scholar] [CrossRef] [Green Version]
- Johns, M.W. A new method for measuring daytime sleepiness: The Epworth sleepiness scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef] [Green Version]
- Sander, C.; Hegerl, U.; Wirkner, K.; Walter, N.; Kocalevent, R.D.; Petrowski, K.; Glaesmer, H.; Hinz, A. Normative values of the Epworth Sleepiness Scale (ESS), derived from a large German sample. Sleep Breath 2016, 20, 1337–1345. [Google Scholar] [CrossRef]
- Maille, A.; Koning, C.; Zwinderman, A.; Willems, L.; Dijkman, J.; Kaptein, A. The development of the ‘Quality-of-life for Respiratory Illness Questionnaire (QOL-RIQ)’: A disease-specific quality-of-life questionnaire for patients with mild to moderate chronic non-specific lung disease. Respir. Med. 1997, 91, 297–309. [Google Scholar] [CrossRef] [Green Version]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bjelland, I.; Dahl, A.A.; Haug, T.T.; Neckelmann, D. The validity of the Hospital Anxiety and Depression Scale: An updated literature review. J. Psychosom. Res. 2002, 52, 69–77. [Google Scholar] [CrossRef]
- Sullivan, M.J.; Thorn, B.; Haythornthwaite, J.A.; Keefe, F.; Martin, M.; Bradley, L.A.; Lefebvre, J.C. Theoretical perspectives on the relation between catastrophizing and pain. Clin. J. Pain 2001, 17, 52–64. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, M.J.; Bishop, S.R.; Pivik, J. The pain catastrophizing scale: Development and validation. Psychol. Assess. 1995, 7, 524. [Google Scholar] [CrossRef]
- Osman, A.; Barrios, F.X.; Kopper, B.A.; Hauptmann, W.; Jones, J.; O’Neill, E. Factor structure, reliability, and validity of the Pain Catastrophizing Scale. J. Behav. Med. 1997, 20, 589–605. [Google Scholar] [CrossRef]
- Osman, A.; Barrios, F.X.; Gutierrez, P.M.; Kopper, B.A.; Merrifield, T.; Grittmann, L. The Pain Catastrophizing Scale: Further psychometric evaluation with adult samples. J. Behav. Med. 2000, 23, 351–365. [Google Scholar] [CrossRef]
- Sullivan, M.J.L. PCS: Pain Catastrophizing Scale: User manual. Montreal: Departments of Psychology, Medicine, and Neurology, School of Physical and Occupational Therapy; McGill University: Montréal, QC, Canada, 2009. [Google Scholar]
- Vercoulen, J.H.; Swanink, C.M.; Galama, J.M.; Fennis, J.F.; Jongen, P.J.; Hommes, O.R.; van der Meer, J.W.; Bleijenberg, G. The persistence of fatigue in chronic fatigue syndrome and multiple sclerosis: Development of a model. J. Psychosom. Res. 1998, 45, 507–517. [Google Scholar] [CrossRef]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [Green Version]
- Janssen, M.F.; Pickard, A.S.; Golicki, D.; Gudex, C.; Niewada, M.; Scalone, L.; Swinburn, P.; Busschbach, J. Measurement properties of the EQ-5D-5L compared to the EQ-5D-3L across eight patient groups: A multi-country study. Qual. Life Res. 2013, 22, 1717–1727. [Google Scholar] [CrossRef] [Green Version]
- van Reenen, M.; Janssen, B. EQ-5D-5L User Guide: Basic Information on How to Use the EQ-5D-5L Instrument; EuroQol Research Foundation: Rotterdam, The Netherlands, 2015. [Google Scholar]
- Altman, D.G. Practical Statistics for Medical Research; CRC Press: Boca Raton, FL, USA, 1990. [Google Scholar]
- Beurskens, S. Meten in de Praktijk; Bohn Stafleu van Loghum: Houten, The Netherlands, 2008. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Abingdon: Nashville, TN, USA, 1988. [Google Scholar]
- Akinwande, M.O.; Dikko, H.G.; Samson, A. Variance inflation factor: As a condition for the inclusion of suppressor variable (s) in regression analysis. Open J. Stat. 2015, 5, 754. [Google Scholar] [CrossRef] [Green Version]
- Egan, J.J.; Martinez, F.J.; Wells, A.U.; Williams, T. Lung function estimates in idiopathic pulmonary fibrosis: The potential for a simple classification. Thorax 2005, 60, 270–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, J.B.; Heijdra, Y.F.; Daudey, L.; Boer, L.M.; Molema, J.; Dekhuijzen, P.N.; Schermer, T.R.; Vercoulen, J.H. Course of normal and abnormal fatigue in patients with chronic obstructive pulmonary disease, and its relationship with domains of health status. Patient Educ. Couns. 2011, 85, 281–285. [Google Scholar] [CrossRef] [PubMed]
- Goertz, Y.M.J.; Spruit, M.A.; Van ’t Hul, A.J.; Peters, J.B.; Van Herck, M.; Nakken, N.; Djamin, R.S.; Burtin, C.; Thong, M.S.Y.; Coors, A.; et al. Fatigue is highly prevalent in patients with COPD and correlates poorly with the degree of airflow limitation. Ther. Adv. Respir. Dis. 2019, 13, 1753466619878128. [Google Scholar] [CrossRef] [PubMed]
- Van Herck, M.; Antons, J.; Vercoulen, J.H.; Goertz, Y.M.J.; Ebadi, Z.; Burtin, C.; Janssen, D.J.A.; Thong, M.S.Y.; Otker, J.; Coors, A.; et al. Pulmonary Rehabilitation Reduces Subjective Fatigue in COPD: A Responder Analysis. J. Clin. Med. 2019, 8, 1264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Herck, M.; Spruit, M.A.; Burtin, C.; Djamin, R.; Antons, J.; Goertz, Y.M.J.; Ebadi, Z.; Janssen, D.J.A.; Vercoulen, J.H.; Peters, J.B.; et al. Fatigue is Highly Prevalent in Patients with Asthma and Contributes to the Burden of Disease. J. Clin. Med. 2018, 7, 471. [Google Scholar] [CrossRef] [Green Version]
- Abrahams, H.J.; Gielissen, M.F.; Schmits, I.C.; Verhagen, C.A.; Rovers, M.M.; Knoop, H. Risk factors, prevalence, and course of severe fatigue after breast cancer treatment: A meta-analysis involving 12 327 breast cancer survivors. Ann. Oncol. 2016, 27, 965–974. [Google Scholar] [CrossRef]
- Baghai-Ravary, R.; Quint, J.K.; Goldring, J.J.; Hurst, J.R.; Donaldson, G.C.; Wedzicha, J.A. Determinants and impact of fatigue in patients with chronic obstructive pulmonary disease. Respir. Med. 2009, 103, 216–223. [Google Scholar] [CrossRef] [Green Version]
- Engberg, I.; Segerstedt, J.; Waller, G.; Wennberg, P.; Eliasson, M. Fatigue in the general population- associations to age, sex, socioeconomic status, physical activity, sitting time and self-rated health: The northern Sweden MONICA study 2014. BMC Public Health 2017, 17, 654. [Google Scholar] [CrossRef] [Green Version]
- Strookappe, B.; De Vries, J.; Elfferich, M.; Kuijpers, P.; Knevel, T.; Drent, M. Predictors of fatigue in sarcoidosis: The value of exercise testing. Respir. Med. 2016, 116, 49–54. [Google Scholar] [CrossRef] [Green Version]
- Sheth, J.S.; Xia, M.; Murray, S.; Martinez, C.H.; Meldrum, C.A.; Belloli, E.A.; Salisbury, M.L.; White, E.S.; Holtze, C.H.; Flaherty, K.R. Frailty and geriatric conditions in older patients with idiopathic pulmonary fibrosis. Respir. Med. 2019, 148, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Neu, D.; Linkowski, P.; Le Bon, O. Clinical complaints of daytime sleepiness and fatigue: How to distinguish and treat them, especially when they become ‘excessive’ or ‘chronic’? Acta Neurol. Belg. 2010, 110, 15. [Google Scholar] [PubMed]
- Maurer, J.; Rebbapragada, V.; Borson, S.; Goldstein, R.; Kunik, M.E.; Yohannes, A.M.; Hanania, N.A. ACCP Workshop Panel on Anxiety and Depression in COPD Anxiety and depression in COPD: Current understanding, unanswered questions, and research needs. Chest 2008, 134, 43S–56S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holland, A.E.; Fiore, J.F., Jr.; Bell, E.C.; Goh, N.; Westall, G.; Symons, K.; Dowman, L.; Glaspole, I. Dyspnoea and comorbidity contribute to anxiety and depression in interstitial lung disease. Respirology 2014, 19, 1215–1221. [Google Scholar] [CrossRef] [PubMed]
- Solomon, B.K.; Wilson, K.G.; Henderson, P.R.; Poulin, P.A.; Kowal, J.; McKim, D.A. A Breathlessness Catastrophizing Scale for chronic obstructive pulmonary disease. J. Psychosom. Res. 2015, 79, 62–68. [Google Scholar] [CrossRef]
- Lukkahatai, N.; Saligan, L.N. Association of catastrophizing and fatigue: A systematic review. J. Psychosom. Res. 2013, 74, 100–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bahmer, T.; Kirsten, A.M.; Waschki, B.; Rabe, K.F.; Magnussen, H.; Kirsten, D.; Gramm, M.; Hummler, S.; Brunnemer, E.; Kreuter, M.; et al. Clinical Correlates of Reduced Physical Activity in Idiopathic Pulmonary Fibrosis. Respiration 2016, 91, 497–502. [Google Scholar] [CrossRef]
- Nolan, C.M.; Longworth, L.; Lord, J.; Canavan, J.L.; Jones, S.E.; Kon, S.S.; Man, W.D. The EQ-5D-5L health status questionnaire in COPD: Validity, responsiveness and minimum important difference. Thorax 2016, 71, 493–500. [Google Scholar] [CrossRef] [Green Version]
- Szentes, B.L.; Kreuter, M.; Bahmer, T.; Birring, S.S.; Claussen, M.; Waelscher, J.; Leidl, R.; Schwarzkopf, L. Quality of life assessment in interstitial lung diseases: A comparison of the disease-specific K-BILD with the generic EQ-5D-5L. Respir. Res. 2018, 19, 101. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Variables | Patients with ILD (Total Group) | Patients with IPF | Fatigue Severity in IPF Patients | Patients with Sarcoidosis | Fatigue Severity in Sarcoidosis Patients | IPF—Sarcoidosis | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Normal/Mild Fatigue <36 p | Severe Fatigue Fatigue ≥36 p | p-Value | Normal/Mild Fatigue <36 p | Severe Fatigue Fatigue ≥36 p | p-Value | p-Value | ||||
| n (%) | 117 | 59 (50.4) | 31 (52.5) | 28 (47.5) | 58 (49.6) | 18 (31.0) | 40 (69.0) | |||
| CIS-Fat | 37.0 ± 12.1 | 34.1 ± 11.2 | 25.5 ± 7.2 | 43.5 ± 5.8 | p < 0.01 | 40.0 ± 12.3 | 24.9 ± 8.5 | 46.7 ± 6.2 | p < 0.01 | p < 0.01 |
| General Characteristics | ||||||||||
| Gender (male, %) | 73 (62.4) | 45 (76.3) | 20 (64.5) | 25 (89.3) | p < 0.05* | 28 (48.3) | 12 (66.7) | 16 (40.0) | ns | p < 0.01* |
| Age (years, IQR) | 66.0 (53.5–74) | 73.0(70.0–78.0) | 72.0 (70.0–77.0) | 73.0 (70.3–78.8) | ns | 53.5 (45.8–62.0) | 55.5 (48.8–66.0) | 51.5 (43.8–59.8) | ns | p < 0.01 |
| Weight (kg) | 82.2 ± 14.7 | 81.4 ± 14.8 | 82.7 ± 16.1 | 80.0 ± 13.4 | ns | 83.0 ± 14.6 | 84.5 ± 9.5 | 82.3 ± 16.5 | ns | ns |
| BMI a (kg/m2) | 27.6 ± 4.2 | 27.6 ± 4.1 | 28.1 ± 4.4 | 27.0 ± 3.8 | ns | 27.6 ± 4.2 | 27.2 ± 3.1 | 27.7 ± 4.7 | ns | ns |
| Partner (n, %) | 86 (73.5) | 43 (72.9) | 23 (74.2) | 20 (71.4) | ns | 43 (74.1) | 15 (83.3) | 28 (70.0) | ns | ns |
| Living together (n, %) | 80 (68.4) | 39 (66.1) | 21 (67.7) | 18 (64.3) | ns | 41 (70.7) | 15 (83.3) | 26 (65.0) | ns | ns |
| Education b, ≥secondary level (n, %) | 73 (63.5) | 27 (47.4) | 13 (41.9) | 14 (53.8) | ns | 46 (79.3) | 18 (100.0) | 28 (70.0) | p < 0.05# | p < 0.01 |
| Diagnosis time ≤1 year (n, %) | 36 (31.3) | 21 (36.2) | 12 (40.0) | 9 (32.1) | ns | 15 (26.3) | 4 (23.5) | 11 (27.5) | ns | ns |
| Hospitalization ≤1 year (n, %) | 24 (20.7) | 14 (23.7) | 7 (22.6) | 7 (25.0) | ns | 10 (17.5) | 1 (5.6) | 9 (22,5) | ns | ns |
| Work last 2 years (n, %) | 48 (41.0) | 12 (20.3) | 7 (22.6) | 5 (17.9) | ns | 36 (62.1) | 13 (72.2) | 23 (57.5) | ns | p < 0.01 |
| Psychological support (n, %) | 27 (23,1) | 8 (13.6) | 5 (16.1) | 3 (10.7) | ns | 19 (32.8) | 2 (11.1) | 17 (42.5) | p<0.05# | p < 0.05 |
| Smoking a current/former (n, %) | 68 (58.6) | 46 (78.0) | 23 (74.2) | 23 (82.1) | ns** | 22 (38.6) | 5 (29.4) | 17 (42.5) | ns** | p < 0.05** |
| Pack-years+ (n) | 8.5 ± 15.1 | 13.5 ± 18.1 | 12.2 ± 16.4 | 15.1 ± 20.3 | ns | 4.0 ± 9.8 | 0.9 ± 2.6 | 5.7 ± 11.8 | p < 0.05 | p < 0.01 |
| Coffee++ b cup ≥3 (n, %) | 58 (50.4) | 32 (55.2) | 12 (40.0) | 20 (71.4) | p < 0.05* | 26 (45.6) | 9 (52.9) | 17 (42.5) | ns | ns |
| Alcohol++ b glass ≥1 (n, %) | 48 (41.7) | 24 (41.4) | 12 (40.0) | 12 (42.9) | ns | 24 (42.1) | 9 (52.9)) | 15 (37.5) | ns | ns |
| Spirometry, static lung volumes, and diffusing capacity | ||||||||||
| TLC e (liter) | 5.2 ± 1.4 | 4.6 ± 1.1 | 4.4 ± 1.1 | 4.7 ± 1.1 | ns | 6.0 ± 1.3 | 6.3 ± 1.2 | 5.8 ± 1.3 | ns | p < 0.01 |
| TLC f (% predicted) | 85.3 ± 20.8 | 73.3 ± 14.3 | 72.6 ± 12.9 | 74.1 ± 16.0 | ns | 98.6 ± 18.8 | 96.5 ± 12.6 | 99.6 ± 21.2 | ns | p < 0.01 |
| RV d (liter) | 1.8 ± 0.5 | 1.6 ± 0.4 | 1.5 ± 0.4 | 1.7 ± 0.3 | ns | 2.0 ± 0.6 | 2.0 ± 0.6 | 2.0 ± 0.5 | ns | p < 0.01 |
| RV (% predicted) | 80.3 ± 26.6 | 64.4 ± 13.8 | 63.3 ± 14.5 | 65.6 ± 13.3 | ns | 98.0 ± 26.2 | 90.8 ± 18.0 | 101.3 ± 28.9 | ns | p < 0.01 |
| FVC (liter) | 3.4 ± 1.1 | 2.9 ± 0.8 | 2.8 ± 0.8 | 3.0 ± 0.9 | ns | 3.9 ± 1.1 | 4.1 ± 1.1 | 3.8 ± 1.1 | ns | p < 0.01 |
| FVC (% predicted) | 90.7 ± 21.6 | 83.2 ± 19.6 | 83.5 ± 18.7 | 82.9 ± 20.8 | ns | 98.2 ± 21.1 | 100.9 ± 16.3 | 97.0 ± 23.1 | ns | p < 0.01 |
| FEV1 (liter) | 2.6 ± 0.8 | 2.3 ± 0.6 | 2.3 ± 0.7 | 2.3 ± 0.6 | ns | 3.0 ± 0.9 | 3.1 ± 0.9 | 2.9 ± 0.9 | ns | p < 0.01 |
| FEV1 (% predicted) | 89.5 ± 20.7 | 87.3 ± 20.9 | 89.3 ± 22.1 | 84.9 ± 19.5 | ns | 91.9 ± 20.5 | 94.1 ± 17.6 | 90.9 ± 21.8 | ns | ns |
| TLCO c (liter) | 5.5 ± 2.4 | 3.9 ± 1.3 | 4.2 ± 1.5 | 3.6 ± 1.0 | ns | 7.3 ± 2.0 | 7.8 ± 2.0 | 7.1 ± 2.0 | ns | p < 0.01 |
| TLCO d (% predicted) | 65.1 ± 23.2 | 49.1 ± 14.7 | 53.0 ± 15.4 | 45.0 ± 12.8 | p < 0.05 | 82.2 ± 18.0 | 86.6 ± 17.2 | 80.1 ± 18.2 | ns | p < 0.01 |
| Comorbidities | ||||||||||
| Comorbidity (n, %) | ns** | ns** | p < 0.05** | |||||||
| none | 44 (37.6) | 15 (25.4) | 9 (29.0) | 6 (21.4) | 29 (50.0) | 10 (55.6) | 19 (47.5) | |||
| 1 | 42 (35.9) | 25 (42.4) | 13 (41.9) | 12 (42.9) | 17 (29.3) | 3 (16.7) | 14 (35.0) | |||
| >1 | 31 (26.5) | 19 (32.2) | 9 (29.0) | 10 (35.7) | 12 (20.7) | 5 (27.8) | 7 (17.5) | |||
| Medication | ||||||||||
| IPF: antifibrotic (n, %) | 51 (86.4) | 27 (87.1) | 24 (85.7) | 0 (0.0) | 0 (0.0) | 0 (0.0) | p < 0.01* | |||
| Nintenadib (n, %) | 17 (33.3) | 9 (33.3) | 8 (33.3) | ns | ||||||
| Pirfenidon (n, %) | 34 (66.7) | 18 (66.7) | 16 (66.7) | ns | ||||||
| Immunosuppressant+++ (n, %) | 27 (23.1) | 5 (8.5) | 0 (0.0) | 5 (17.9) | p < 0.05# | 22 (37.9) | 5 (27.8) | 17 (42.5) | ns | p < 0.01* |
| Heart rate-lowering medication (n, %) | 23 (19.7) | 15 (25.4) | 9 (29.0) | 6 (21.4) | ns | 8 (13.8) | 3 (16.7) | 5 (12.5) | ns | ns |
| Antidepressant medication (n, %) | 6 (5.1) | 5 (8.5) | 1 (3.2) | 4 (14.3) | ns | 1 (1.7) | 0 (0.0) | 1 (2.5) | ns | ns |
| Antihypertensive medication (n, %) | 37 (31.6) | 25 (42.4) | 16 (51.6) | 9 (32.1) | ns | 12 (20.7) | 4 (22.2) | 8 (20.0) | ns | p < 0.05* |
| Other medication for pulmonary conditions (n, %) | 38 (32.5) | 7 (11.9) | 2 (6.5) | 5 (17.9) | ns | 31 (53.4) | 7 (38.9) | 24 (60.0) | ns | p < 0.01* |
| Variables | Patients with ILD (Total Group) | Patients with IPF | Fatigue Severity in IPF Patients | Patients with Sarcoidosis | Fatigue Severity in Sarcoidosis Patients | IPF—Sarcoidosis | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Normal/Mild Fatigue <36 p | Severe Fatigue Fatigue ≥36 p | p-Value | Normal/Mild Fatigue <36 p | Severe Fatigue Fatigue ≥36 p | p-Value | p-Value | ||||
| n (%) | 117 | 59 (50.4) | 31 (52.5) | 28 (47.5) | 58 (49.6) | 18 (31.0) | 40 (69.0) | |||
| CIS (p, 8–56) | 37.0 ± 12.1 | 34.1 ± 11.2 | 25.5 ± 7.2 | 43.5 ± 5.8 | p < 0.01 | 40.0 ± 12.3 | 24.9 ± 8.5 | 46.7 ± 6.2 | p < 0.01 | p < 0.01 |
| General Characteristics | ||||||||||
| Comorbidity | ||||||||||
| Comorbidity (n, %) | ns** | ns** | p < 0.05** | |||||||
| none | 44 (37.6) | 15 (25.4) | 9 (29.0) | 6 (21.4) | 29 (50.0) | 10 (55.6) | 19 (47.5) | |||
| 1 | 42 (35.9) | 25 (42.4) | 13 (41.9) | 12 (42.9) | 17 (29.3) | 3 (16.7) | 14 (35.0) | |||
| >1 | 31 (26.5) | 19 (32.2) | 9 (29.0) | 10 (35.7) | 12 (20.7) | 5 (27.8) | 7 (17.5) | |||
| Comorbidity ≥1 (n, %) | 73 (62.4) | 44 (74.6) | 22 (71.0) | 22 (78.6) | ns* | 29 (50.0) | 8 (44.4) | 21 (52.5) | ns* | p < 0.01* |
| Comorbidities | ||||||||||
| Hypertension (n, %) | 22 (18.8) | 17 (28.8) | 9 (29.0) | 8 (28.6) | ns* | 5 (8.6) | 1 (5.6) | 4 (10.0) | ns# | p < 0.01* |
| Pulmonary hypertension (n, %) | 2 (1.7) | 2 (3.4) | 0 (0.0) | 2 (7.1) | ns# | 0 (0.0) | 0 (0.0) | 0 (0.0) | - | n s# |
| COPD/asthma (n, %) | 6 (5.1) | 0 (0.0) | 0 (0.0) | 0 (0.0) | - | 6 (10.3) | 1 (5.6) | 5 (12.5) | ns# | p <0.05# |
| Cardiac failure (n, %) | 12 (10.3) | 6 (10.2) | 3 (9.7) | 3 (10.7) | ns# | 6 (10.3) | 4 (22.2) | 2 (5.0) | ns# | ns* |
| Cardiac sarcoidosis (n, %) | 1 (0.9) | 0 (0.0) | 0 (0.0) | 0 (0.0) | - | 1 (1.7) | 1 (5.6) | 0 (0.0) | ns# | ns# |
| Cardiac surgery CABG and/or Heart Valve (n, %) | 8 (6.8) | 6 (10.2) | 4 (12.9) | 2 (7.1) | ns# | 2 (3.4) | 1 (5.6) | 1 (2.5) | ns# | ns# |
| Diabetes Mellitus (n, %) | 12 (10.3) | 8 (13.6) | 3 (9.7) | 5 (17.9) | ns# | 4 (6.9) | 2 (11.1) | 2 (5.0) | ns# | ns# |
| OSAS (n, %) | 4 (3.4) | 3 (5.1) | 1 (3.2) | 2 (7.2) | ns# | 1 (1.7) | 1 (5.6) | 0 (0.0) | ns# | ns# |
| Eyes-Uveitis (n, %) | 5 (4.3) | 0 (0.0) | 0 (0.0) | 0 (0.0) | - | 5 (8.6) | 2 (11.1) | 3 (7.5) | ns# | p <0.05# |
| TIA/CVA (n, %) | 7 (6.0) | 5 (8.5) | 1 (3.2) | 4 (14.3) | ns# | 2 (3.4) | 1 (5.6) | 1 (2.5) | ns# | ns# |
| Carotid artery stenosis/sPAD (n, %) | 6 (5.1) | 5 (8.5) | 2 (6.5) | 3 (10.7) | ns# | 1 (1.7) | 0 (0.0) | 1 (2.5) | ns# | ns# |
| Other comorbidities (n, %) | 36 (30.8) | 20 (33.9) | 13 (41.9) | 7 (25.0) | ns* | 16 (27.6) | 4 (22.2) | 12 (30.0) | ns# | ns* |
| Variables | Patients with ILD (Total Group) | Patients with IPF | Fatigue Severity in IPF Patients | Patients with Sarcoidosis | Fatigue Severity in Sarcoidosis Patients | IPF—Sarcoidosis | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Normal/Mild Fatigue <36 p | Severe Fatigue Fatigue ≥36 p | p-Value | Normal/Mild Fatigue <36 p | Severe Fatigue Fatigue ≥36 p | p-Value | p-Value | ||||
| n (%) | 117 | 59 (50.4) | 31 (52.5) | 28 (47.5) | 58 (49.6) | 18 (31.0) | 40 (69.0) | |||
| CIS (p, 8–56) | 37.0 ± 12.1 | 34.1 ± 11.2 | 25.5 ± 7.2 | 43.5 ± 5.8 | p < 0.01 | 40.0 ± 12.3 | 24.9 ± 8.5 | 46.7 ± 6.2 | p < 0.01 | p < 0.01 |
| Dyspnea | ||||||||||
| mMRC-Dyspnea grade g range 0–4 (p, IQR) | 1.0 (1.0–2.0) | 2.0 (1.0–3.0) | 1.0 (1.0–3.0) | 2.0 (1.0–3.0) | ns** | 1.0 (1.0–2.0) | 0.5 (0.0–1.0) | 1.0 (1.0–2.0) | p < 0.05** | p < 0.05** |
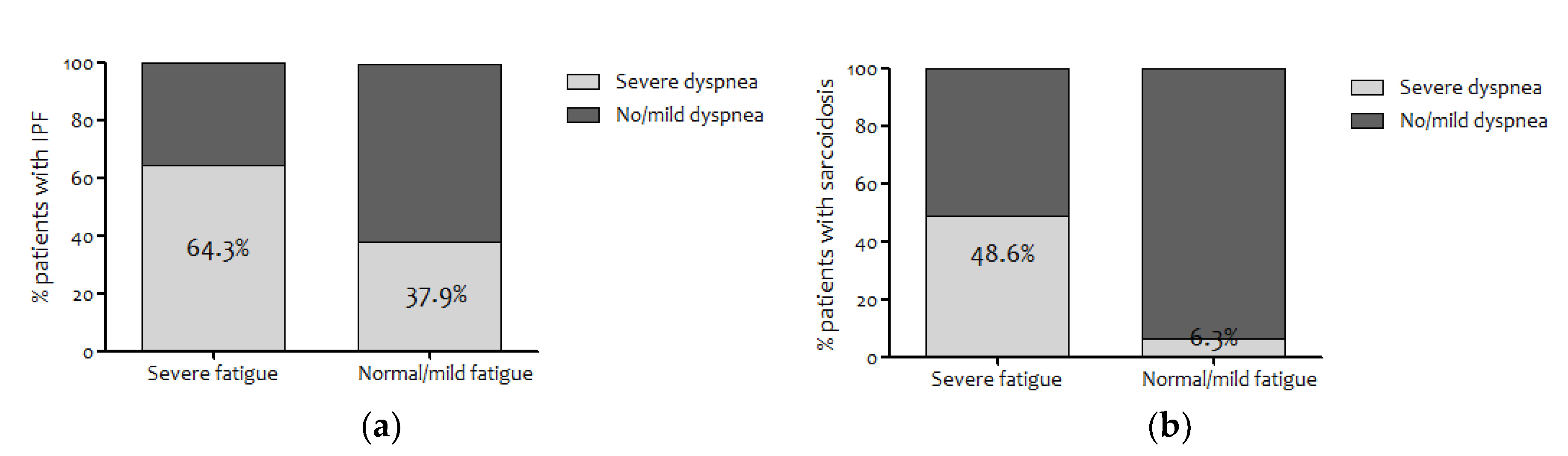
| mMRC g grade ≥2 (moderate-severe dyspnea) (n, %) | 48 (43.6) | 29 (50.9) | 11 (37.9) | 18 (64.3) | p < 0.05 | 19 (35.8) | 1 (6.3) | 18 (48.6) | p < 0.05 | ns |
| Sleepiness | ||||||||||
| ESS i (p, IQR, 0–24) | 5.0 (4.0–8.0) | 5.0 (4.0–8.0) | 4.0 (3.0–7.0) | 5.5 (4.0–8.3) | ns | 5.0 (4.0–8.0) | 5.0 (3.8–6.0) | 6.5 (3.8–10.0) | ns | ns |
| ESS > 10 excessive i (n, %) | 9 (8.4) | 1 (2.0) | 0 | 1 (4.5) | ns | 8 (14.3) | 0 | 8 (21.1) | p < 0.05# | p < 0.05# |
| Anxiety and Depression | ||||||||||
| HADS anxiety e range 0–21 (p, IQR) | 5.0 (2.0–7.8) | 5.0 (2.0–8.0) | 4.0 (2.0–7.8) | 6.0 (4.0–8.0) | ns | 4.0 (2.0–7.0) | 3.0 (2.0–5.3) | 5.0 (3.0–8.0) | p < 0.05** | ns |
| (HADS anxiety ≥11points) e (n, %) | 12 (10.7) | 5 (9.1) | 2 (7.1) | 3 (11.1) | ns | 7 (12.3) | 2 (11.1) | 5 (12.8) | ns | ns |
| HADS depression c range 0–21 (p, IQR) | 4.5 (2.0–7.0) | 5.0 (2.0–7.0) | 3.0 (2.0–6.5) | 5.0 (4.0–8.0) | p < 0.05** | 4.0 (1.0–7.0) | 1.0 (1.0–3.5) | 6.0 (3.0–8.0) | p < 0.01** | ns |
| (HADS depression ≥11 points) c (n, %) | 9 (7.9) | 5 (8.9) | 2 (6.9) | 3 (11.1) | ns | 4 (6.9) | 0 | 4 (10.0) | ns | ns |
| Fatigue-related Catastrophizing | ||||||||||
| FCS f (p, IQR) | 11.0 (3.0–23.0) | 11.0 (2.0–26) | 5.0 (0.3–14.5) | 21.0 (11.0–28.5) | p < 0.01** | 10.0 (3.8–18.0) | 4.0 (0.0–11.5) | 11.5 (6.5–23.0) | p < 0.01** | ns |
| FCS f grade >30 (n, %) | 13 (11,7) | 7 (13.2) | 2 (7.1) | 5 (20) | ns | 6 (10.3) | 0 | 6 (15.0) | ns | ns |
| Causal Attributions of Fatigue | ||||||||||
| CALg Sum score (p, 11–44) | 18.3 ± 5.1 | 18.4 ± 4.5 | 17.8 ± 4.5 | 19.2 ± 4.5 | ns | 18.3 ± 5.6 | 17.6 ± 6.8 | 18.6 ± 5.0 | ns | ns |
| CAL Physical Sum d (p, 5–20) | 9.4 ± 3.4 | 9.7 ± 3.1 | 9.1 ± 3.0 | 10.4 ± 3.1 | ns | 9.1 ± 3.7 | 7.9 ± 4.0 | 9.6 ± 3.5 | ns | ns |
| CAL Non-Physical Sum e (p, 6–24) | 8.9 ± 2.9 | 8.6 ± 2.4 | 8.7 ± 2.6 | 8.5 ± 2.1 | ns | 9.2 ± 3.3 | 9.6 ± 4.1 | 9.0 ± 3.0 | ns | ns |
| Quality of Life Respiratory Illness (Functional Impairment) | ||||||||||
| QoL-RIQ/activity h (p, IQR) | 13.0 (8.0–17.0) | 14.0 (10.3–17.0) | 11.0 (8.0–15.0) | 15.0 (13.0–20.0) | p < 0.01** | 10.5 (7.0–16.8) | 6.0 (4.0–9.0) | 15.0 (9.0-18.0) | p < 0.01** | p < 0.05** |
| Quality of Life, Health Status | ||||||||||
| EQ-5D-5L a, index values (p, 0–1) | 0.74 ± 0.20 | 0.74 ± 0.18 | 0.80 ± 0.16 | 0.67 ± 0.17 | p < 0.01 | 0.75 ± 0.23 | 0.89 ± 0.14 | 0.68 ± 0.23 | p < 0.01 | ns |
| EQ-5D-5Lb, VAS (p, 0–100) | 63.1 ± 18.1 | 63.3 ± 16.5 | 71.0 ± 15.6 | 55.0 ± 13.4 | p < 0.01 | 63.0 ± 19.7 | 81.2 ± 11.5 | 55.3 ± 17.2 | p < 0.01 | ns |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bloem, A.E.M.; Mostard, R.L.M.; Stoot, N.; Vercoulen, J.H.; Peters, J.B.; Janssen, D.J.A.; Custers, J.W.H.; Spruit, M.A. Severe Fatigue is Highly Prevalent in Patients with IPF or Sarcoidosis. J. Clin. Med. 2020, 9, 1178. https://doi.org/10.3390/jcm9041178
Bloem AEM, Mostard RLM, Stoot N, Vercoulen JH, Peters JB, Janssen DJA, Custers JWH, Spruit MA. Severe Fatigue is Highly Prevalent in Patients with IPF or Sarcoidosis. Journal of Clinical Medicine. 2020; 9(4):1178. https://doi.org/10.3390/jcm9041178
Chicago/Turabian StyleBloem, Ada E. M., Rémy L. M. Mostard, Naomi Stoot, Jan H. Vercoulen, Jeannette B. Peters, Daisy J. A. Janssen, Jan W. H. Custers, and Martijn A. Spruit. 2020. "Severe Fatigue is Highly Prevalent in Patients with IPF or Sarcoidosis" Journal of Clinical Medicine 9, no. 4: 1178. https://doi.org/10.3390/jcm9041178