Cost-Utility of Attachment-Based Compassion Therapy (ABCT) for Fibromyalgia Compared to Relaxation: A Pilot Randomized Controlled Trial

 ,
,  , , and
, , and 
Abstract
:1. Introduction
1.1. Loving-Kindness Meditation and Compassion-Based Interventions
1.2. The Importance of Economic Evaluations in Healthcare
1.3. Why It Is Important to Know the Cost-Utility of ABCT
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Procedure
2.4. Treatments
2.4.1. ABCT
2.4.2. REL
2.5. Study Measures
2.5.1. Sociodemographic-Clinical Questionnaire
2.5.2. The EuroQoL Questionnaire (EQ-5D-3L)
2.5.3. The Client Service Receipt Inventory (CSRI)
2.6. Data Analyses
2.6.1. Description of The Costing Procedure from The Healthcare Perspective
2.6.2. Utility Scores
2.6.3. Cost-Utility Analyses
- (i)
- ABCT costs less and is more effective than Relaxation;
- (ii)
- ABCT costs more and is less effective than Relaxation;
- (iii)
- ABCT costs less but is less effective than Relaxation;
- (iv)
- ABCT costs more and is more effective than Relaxation.
3. Results
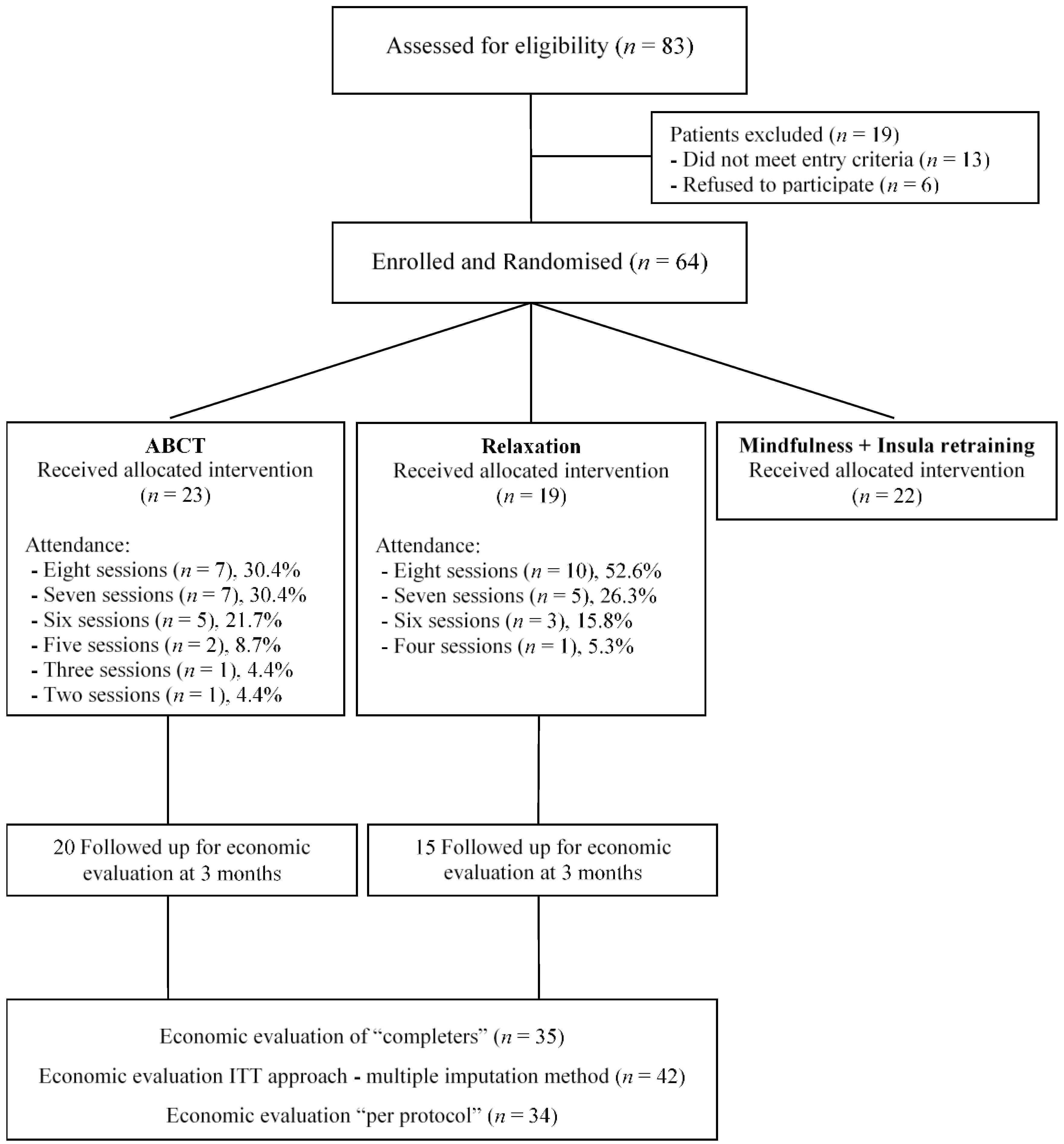
3.1. Participant Characteristics, Flow and Compliance
3.2. Direct Costs and QALYs
3.3. Cost-Utility of ABCT Compared to Relaxation
4. Discussion
4.1. Summary of Key Findings
4.2. Comparison with Relevant Findings from Previous Published Studies
4.3. Strengths and Limitations of This Study
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Peteet, J.R. A fourth wave of psychotherapies: Moving beyond recovery toward well-being. Harv. Rev. Psychiatry 2018, 26, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Shonin, E.; Van Gordon, W.; Compare, A.; Zangeneh, M.; Griffiths, M.D. Buddhist-derived loving-kindness and compassion meditation for the treatment of psychopathology: A systematic review. Mindfulness 2015, 6, 1161–1180. [Google Scholar] [CrossRef] [Green Version]
- Galante, J.; Galante, I.; Bekkers, M.J.; Gallacher, J. Effect of kindness-based meditation on health and well-being: A systematic review and meta-analysis. J. Consult. Clin. Psychol. 2014, 82, 1101–1114. [Google Scholar] [CrossRef] [PubMed]
- Graser, J.; Stangier, U. Compassion and loving-kindness meditation: An overview and prospects for the application in clinical samples. Harv. Rev. Psychiatry 2018, 26, 201–215. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, S.G.; Grossman, P.; Hinton, D.E. Loving-kindness and compassion meditation: Potential for psychological interventions. Clin. Psychol. Rev. 2011, 31, 1126–1132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strauss, C.; Taylor, B.L.; Gu, J.; Kuyken, W.; Baer, R.; Jones, F.; Cavanagh, K. What is compassion and how can we measure it? A review of definitions and measures. Clin. Psychol. Rev. 2016, 47, 15–27. [Google Scholar] [CrossRef] [Green Version]
- Kirby, J.N. Compassion interventions: The programmes, the evidence, and implications for research and practice. Psychol. Psychother. 2017, 90, 432–455. [Google Scholar] [CrossRef]
- Pace, T.W.; Negi, L.T.; Adame, D.D.; Cole, S.P.; Sivilli, T.I.; Brown, T.D.; Issa, M.J.; Raison, C.L. Effect of compassion meditation on neuroendocrine, innate immune and behavioral responses to psychosocial stress. Psychoneuroendocrinology 2009, 34, 87–98. [Google Scholar] [CrossRef] [Green Version]
- Kemeny, M.E.; Foltz, C.; Cavanagh, J.F.; Cullen, M.; Giese-Davis, J.; Jennings, P.; Rosenberg, E.L.; Gillath, O.; Shaver, P.R.; Wallace, B.A.; et al. Contemplative/emotion training reduces negative emotional behavior and promotes prosocial responses. Emotion 2012, 12, 338–350. [Google Scholar] [CrossRef]
- Neff, K.D.; Germer, C.K. A pilot study and randomized controlled trial of the mindful self-compassion program. J. Clin. Psychol. 2013, 69, 28–44. [Google Scholar] [CrossRef]
- Jazaieri, H.; Jinpa, G.T.; McGonigal, K.; Rosenberg, E.L.; Finkelstein, J.; Simon-Thomas, E.; Cullen, M.; Doty, J.R.; Gross, J.J.; Goldin, P.R. Enhancing compassion: A randomized controlled trial of a compassion cultivation training program. J. Happiness Stud. 2013, 14, 1113–1126. [Google Scholar] [CrossRef]
- Gilbert, P. The origins and nature of compassion focused therapy. Br. J. Clin. Psychol. 2014, 53, 6–41. [Google Scholar] [CrossRef] [PubMed]
- García-Campayo, J.; Navarro-Gil, M.; Demarzo, M. Attachment-based compassion therapy. Mindfulness Compassion. 2016, 1, 68–74. [Google Scholar] [CrossRef]
- Kirby, J.N.; Tellegen, C.L.; Steindl, S.R. A meta-analysis of compassion-based interventions: Current state of knowledge and future directions. Behav. Ther. 2017, 48, 778–792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montero-Marín, J.; Navarro-Gil, M.; Puebla-Guedea, M.; Luciano, J.V.; Van Gordon, W.; Shonin, E.; García-Campayo, J. Efficacy of "Attachment-Based Compassion Therapy" in the treatment of fibromyalgia: A randomized controlled trial. Front Psychiatry 2018, 8, 307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sambamoorthi, U.; Tan, X.; Deb, A. Multiple chronic conditions and healthcare costs among adults. Expert Rev. Pharmacoecon. Outcomes Res. 2015, 15, 823–832. [Google Scholar] [CrossRef] [Green Version]
- van Lier, L.I.; Bosmans, J.E.; van Hout, H.P.J.; Mokkink, L.B.; van den Hout, W.B.; de Wit, G.A.; Dirksen, C.D.; Nies, H.L.G.R.; Hertogh, C.M.P.M.; van der Roest, H.G. Consensus-based cross-European recommendations for the identification, measurement and valuation of costs in health economic evaluations: A European Delphi study. Eur. J. Health Econ. 2018, 19, 993–1008. [Google Scholar] [CrossRef] [Green Version]
- Haycox, A. What Is Health Economics? Hayward Medical Communications: London, UK, 2009. [Google Scholar]
- Drummond, M.F.; Sculpher, M.J.; Torrance, G.W.; O’Brien, B.J.; Stoddart, G. Methods for the Economic Evaluation of Health Care Programmes, 3rd ed.; Oxford University Press: Oxford, UK, 2005. [Google Scholar]
- Higgins, A.M.; Harris, A.H. Health economic methods: Cost-minimization, cost-effectiveness, cost-utility, and cost-benefit evaluations. Crit. Care Clin. 2012, 28, 11–24. [Google Scholar] [CrossRef]
- Konnopka, A.; Schaefert, R.; Heinrich, S.; Kaufmann, C.; Luppa, M.; Herzog, W.; König, H.H. Economics of medically unexplained symptoms: A systematic review of the literature. Psychother. Psychosom. 2012, 81, 265–275. [Google Scholar] [CrossRef]
- Leaviss, J.; Uttley, L. Psychotherapeutic benefits of compassion-focused therapy: An early systematic review. Psychol. Med. 2015, 45, 927–945. [Google Scholar] [CrossRef] [Green Version]
- Feliu-Soler, A.; Cebolla, A.; McCracken, L.M.; D’Amico, F.; Knapp, M.; López-Montoyo, A.; García-Campayo, J.; Soler, J.; Baños, R.M.; Pérez-Aranda, A.; et al. Economic impact of third-wave cognitive behavioral therapies: A systematic review and quality assessment of economic evaluations in randomized controlled trials. Behav. Ther. 2018, 49, 124–147. [Google Scholar] [CrossRef] [PubMed]
- Duarte, R.; Lloyd, A.; Kotas, E.; Andronis, L.; White, R. Are acceptance and mindfulness-based interventions ‘value for money’? Evidence from a systematic literature review. Br. J. Clin. Psychol. 2019, 58, 187–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wentz, K.; Lindberg, C.; Hallberg, L. Psychological functioning in women with fibromyalgia: A grounded theory study. Health. Care Women Int. 2004, 25, 702–729. [Google Scholar] [CrossRef] [PubMed]
- Peñacoba, C.; Pérez-Calvo, S.; Blanco, S.; Sanroman, L. Attachment styles, pain intensity and emotional variables in women with fibromyalgia. Scand. J. Caring Sci. 2018, 32, 535–544. [Google Scholar] [CrossRef] [PubMed]
- Husereau, D.; Drummond, M.; Petrou, S.; Carswell, C.; Moher, D.; Greenberg, D.; Augustovski, F.; Briggs, A.H.; Mauskopf, J.; Loder, E.; et al. Consolidated Health Economic Evaluation Reporting Standards (CHEERS) statement. BMC Med. 2013, 11, 80. [Google Scholar] [CrossRef] [Green Version]
- Ramsey, S.D.; Willke, R.J.; Glick, H.; Reed, S.D.; Augustovski, F.; Jonsson, B.; Briggs, A.; Sullivan, S.D. Cost-effectiveness analysis alongside clinical trials II-An ISPOR good research practices task force report. Value Health. 2015, 18, 161–172. [Google Scholar] [CrossRef] [Green Version]
- Whitehead, A.L.; Julious, S.A.; Cooper, C.L.; Campbell, M.J. Estimating the sample size for a pilot randomised trial to minimise the overall trial sample size for the external pilot and main trial for a continuous outcome variable. Stat. Methods Med. Res. 2016, 25, 1057–1073. [Google Scholar] [CrossRef]
- Wolfe, F.; Smythe, H.A.; Yunus, M.B.; Bennett, R.M.; Bombardier, C.; Goldenberg, D.L.; Tugwell, P.; Campbell, S.M.; Abeles, M.; Clar, P. The American College Rheumatology 1990 Criteria for the Classification of Fibromyalgia: Report of the Multicenter Criteria Committee. Arthritis Rheum. 1990, 33, 160–172. [Google Scholar] [CrossRef]
- Navarro-Gil, M.; Lopez-del-Hoyo, Y.; Modrego-Alarcón, M.; Montero-Marin, J.; Van Gordon, W.; Shonin, E.; Garcia-Campayo, J. Effects of Attachment-Based Compassion Therapy (ABCT) on self-compassion and attachment style in healthy people. Mindfulness 2020, 11, 51–62. [Google Scholar] [CrossRef]
- Meeus, M.; Nijs, J.; Vanderheiden, T.; Baert, I.; Descheemaeker, F.; Struyf, F. The effect of relaxation therapy on autonomic functioning, symptoms and daily functioning, in patients with chronic fatigue syndrome or fibromyalgia: A systematic review. Clin. Rehabil. 2015, 29, 221–233. [Google Scholar] [CrossRef]
- Badia, X.; Roset, M.; Montserrat, S.; Herdman, M.; Segura, A. The Spanish version of EuroQol: A description and its applications: European Quality of Life scale. Med. Clin. 1999, 112, 79–85. [Google Scholar]
- Vázquez-Barquero, J.L.; Gaite, L.; Cuesta, M.J.; Garcia-Usieto, E.; Knapp, M.; Beecham, J. Spanish version of the CSRI: A mental health cost evaluation interview. Arch. Neurobiol. 1997, 60, 171–184. [Google Scholar]
- Badia, X.; Roset, M.; Herdman, M.; Kind, P. A comparison of United Kingdom and Spanish general population time trade-off values for EQ-5D health states. Med. Decis. Making 2001, 21, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Briggs, A.H.; Wonderling, D.E.; Mooney, C.Z. Pulling cost-effectiveness analysis up by its bootstraps: A non-parametric approach to confidence interval estimation. Health. Econ. 1997, 6, 327–340. [Google Scholar] [CrossRef]
- Vallejo-Torres, L.; García-Lorenzo, B.; Serrano-Aguilar, P. Estimating a cost-effectiveness threshold for the Spanish NHS. Health. Econ. 2018, 27, 746–761. [Google Scholar] [CrossRef] [PubMed]
- Kemani, M.K.; Olsson, G.L.; Lekander, M.; Hesser, H.; Andersson, E.; Wicksell, R.K. Efficacy and cost-effectiveness of acceptance and commitment therapy and applied relaxation for longstanding pain: A randomized controlled trial. Clin. J. Pain. 2015, 31, 1004–1016. [Google Scholar] [CrossRef]
- Luciano, J.V.; D’Amico, F.; Feliu-Soler, A.; McCracken, L.M.; Aguado, J.; Peñarrubia-María, M.T.; Knapp, M.; Serrano-Blanco, A.; García-Campayo, J. Cost-utility of group Acceptance and Commitment Therapy for fibromyalgia versus recommended drugs: An economic analysis alongside a 6-month randomised controlled trial conducted in Spain (EFFIGACT study). J. Pain. 2017, 18, 868–880. [Google Scholar] [CrossRef]
- Herman, P.M.; Anderson, M.L.; Sherman, K.J.; Balderson, B.H.; Turner, J.A.; Cherkin, D.C. Cost-effectiveness of mindfulness-based stress reduction versus cognitive behavioral therapy or usual care among adults with chronic low back pain. Spine 2017, 42, 1511–1520. [Google Scholar] [CrossRef]
- Johannsen, M.; Sørensen, J.; O’connor, M.; Jensen, A.B.; Zachariae, R. Mindfulness-Based Cognitive Therapy (MBCT) is cost-effective compared to a wait-list control for persistent pain in women treated for primary breast cancer—Results from a randomized controlled trial. Psychooncology 2017, 26, 2208–2214. [Google Scholar] [CrossRef]
- Patel, A.; Rendu, A.; Moran, P.; Leese, M.; Mann, A.; Knapp, M. A comparison of two methods of collecting economic data in primary care. Fam. Pract. 2005, 22, 323–327. [Google Scholar] [CrossRef] [Green Version]
- Öst, L.G. The efficacy of Acceptance and Commitment Therapy: An updated systematic review and meta-analysis. Behav. Res. Ther. 2014, 61, 105–121. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Service (Unit) | Costs (€) | |
|---|---|---|
| Healthcare | General practitioner (per appointment) | 36.97 |
| Nurse/psychiatric nurse (per appointment) | 34.13 | |
| Social worker (per appointment) | 35.78 | |
| Clinical psychologist (per appointment) | 45.06 | |
| Psychiatrist (per appointment) | 45.06 | |
| Other medical specialists (per appointment) | 43.82 | |
| Accident and Emergency in hospital (per attendance) | 99.34 | |
| Hospital stay (per night) | 112 | |
| Diagnostic tests (range) | 6.13–455.53 | |
| Pharmacological treatment (per daily dose) * | Various | |
| Attachment-Based Compassion Therapy (ABCT) and Relaxation (REL) (per participant per group session) | 35 | |
| Baseline Characteristics | ABCT (n = 23) | REL (n = 19) | Test Statistic | p |
|---|---|---|---|---|
| Gender, % female | 23 (100) | 19 (100) | (*) | 1.00 |
| Age (M, SD) | 50.83 (8.70) | 52.21 (5.95) | T = 0.56 (40) | 0.56 |
| Marital status, % with partner | 18 (78.3) | 13 (68.4) | (*) | 0.50 |
| Dwelling, % own home | 21 (91.3) | 17 (89.5) | (*) | 1.00 |
| Educational level | ||||
| Primary | 10 (43.5) | 4 (21.1) | (*) | 0.31 |
| Secondary | 8 (34.8) | 8 (42.1) | ||
| University | 5 (21.7) | 7 (36.8) | ||
| Work status | ||||
| Housework | 10 (43.5) | 6 (31.6) | (*) | 0.54 |
| Employed | 4 (17.4) | 3 (15.8) | ||
| Sick leave/inability | 7 (30.4) | 5 (26.3) | ||
| Unemployed | 2 (8.7) | 5 (26.3) |
| Baseline (n = 42) Time Frame: Last 12 Months | ABCT (n = 23) M (SD) | REL (n = 19) M (SD) | p | Cohen’s d * |
|---|---|---|---|---|
| Costs (€) | ||||
| Primary healthcare services | 499.7 (325.1) | 441.1 (377.6) | 0.82 | 0.17 |
| Specialized healthcare services | 1037.1 (957.4) | 897.4 (940.1) | 0.79 | 0.15 |
| Medical tests | 367.3 (378.8) | 510.8 (636.4) | 0.23 | 0.29 |
| FM-related medications | 748.8 (780.4) | 520.3 (485.9) | 0.62 | 0.35 |
| Direct costs | 2653.0 (1357.1) | 2369.6 (1948.8) | 0.84 | 0.18 |
| Outcomes | ||||
| EQ-5D Utility score | 0.61 (0.17) | 0.52 (0.23) | 0.43 | 0.46 |
| Follow-up (n = 35) Time frame: last 3 months | ABCT (n = 20) M (SD) | REL (n = 15) M (SD) | p | Cohen’s d * |
| Costs (€) | ||||
| Primary healthcare services | 83.8 (33.9) | 119.0 (40.6) | 0.11 | 0.98 |
| Specialized healthcare services | 116.7 (65.4) | 247.3 (120.9) | 0.57 | 1.45 |
| Medical tests | 36.8 (64.2) | 108.8 (114.1) | 0.81 | 0.83 |
| FM-related medications | 108.3 (117.8) | 151.3 (125.6) | 0.75 | 0.35 |
| Interventions (ABCT – REL) | 313.6 (41.1) | 305.2 (30.4) | 0.00 | 0.23 |
| Direct costs | 659.2 (164.4) | 931.6 (217.5) | 0.30 | 1.49 |
| Outcomes | ||||
| EQ-5D Utility score | 0.72 (0.14) | 0.51 (0.25) | 0.30 | 1.11 |
| QALY (based on EQ-5D utility score) | 0.17 (0.04) | 0.13 (0.06) | 0.49 | 0.83 |
| Incremental Cost Mean (95% Bootstrap CI) | Incremental Effect Mean (95% Bootstrap CI) | ICER ABCT vs. REL | |
|---|---|---|---|
| Completers (n = 35) EQ-5D (QALY) | −194.1 (−450.3, 356.1) | 0.023 (0.010, 0.141) | ABCT dominant |
| ITT (n = 42) EQ-5D (QALY) | −256.3 (−447.4, −65.3) | 0.021 (0.009, 0.033) | ABCT dominant |
| Per protocol (n = 34) EQ-5D (QALY) | −168.3 (−499.7, 548.8) | 0.003 (−0.013, 0.071) | ABCT dominant |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Amico, F.; Feliu-Soler, A.; Montero-Marín, J.; Peñarrubía-María, M.T.; Navarro-Gil, M.; Van Gordon, W.; García-Campayo, J.; Luciano, J.V. Cost-Utility of Attachment-Based Compassion Therapy (ABCT) for Fibromyalgia Compared to Relaxation: A Pilot Randomized Controlled Trial. J. Clin. Med. 2020, 9, 726. https://doi.org/10.3390/jcm9030726
D’Amico F, Feliu-Soler A, Montero-Marín J, Peñarrubía-María MT, Navarro-Gil M, Van Gordon W, García-Campayo J, Luciano JV. Cost-Utility of Attachment-Based Compassion Therapy (ABCT) for Fibromyalgia Compared to Relaxation: A Pilot Randomized Controlled Trial. Journal of Clinical Medicine. 2020; 9(3):726. https://doi.org/10.3390/jcm9030726
Chicago/Turabian StyleD’Amico, Francesco, Albert Feliu-Soler, Jesús Montero-Marín, María T. Peñarrubía-María, Mayte Navarro-Gil, William Van Gordon, Javier García-Campayo, and Juan V. Luciano. 2020. "Cost-Utility of Attachment-Based Compassion Therapy (ABCT) for Fibromyalgia Compared to Relaxation: A Pilot Randomized Controlled Trial" Journal of Clinical Medicine 9, no. 3: 726. https://doi.org/10.3390/jcm9030726