Instruments of Choice for Assessment and Monitoring Diabetic Foot: A Systematic Review

 , , , and
, , , and
Abstract
:1. Introduction
2. Material and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Sources and Search
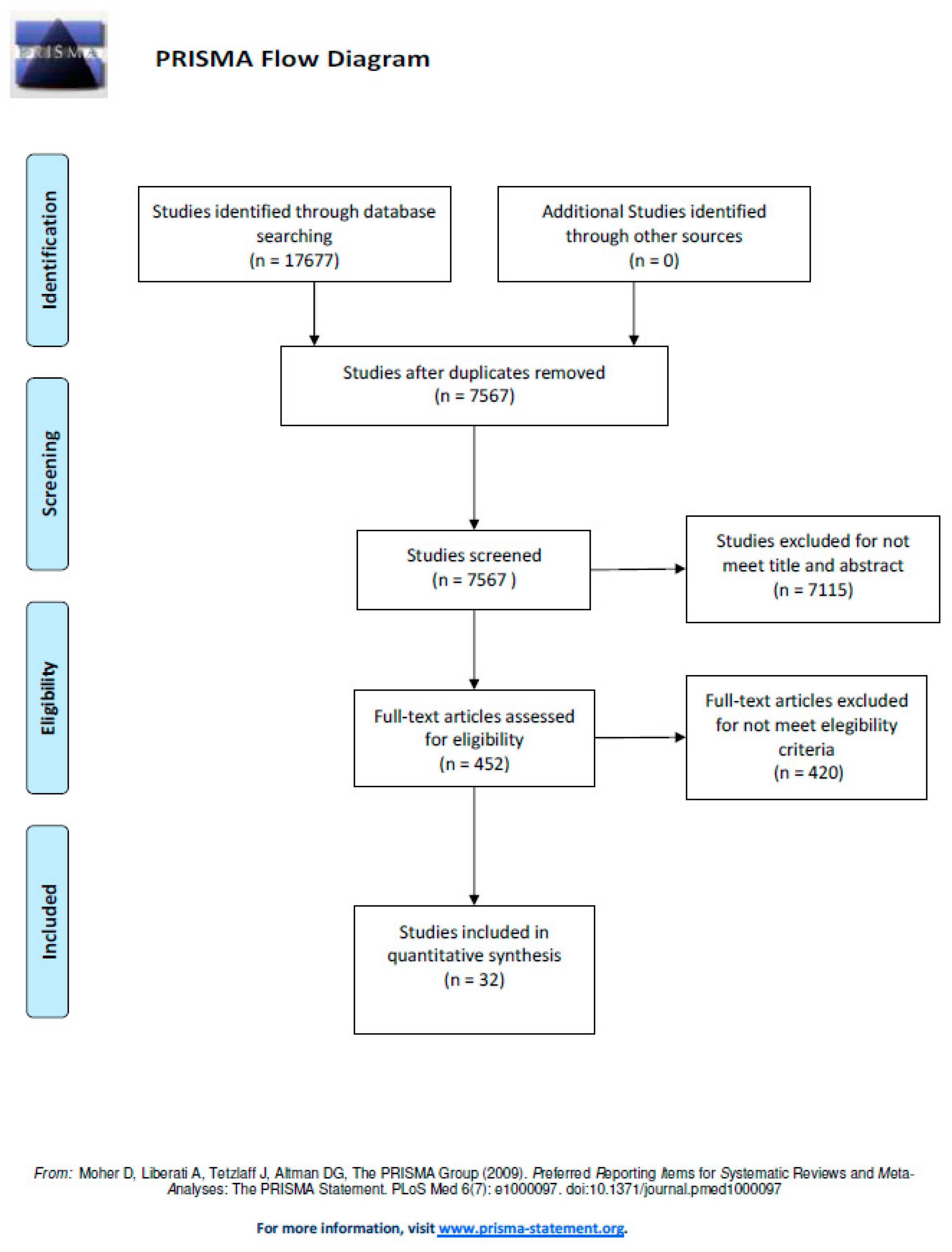
2.4. Study Selection
2.5. Data Extraction and Synthesis of Results
3. Results
4. Discussion
4.1. Psychometric Properties Calculated in OCOMs
4.2. Variables and OCOMs for Assessment of Diabetic Neuropathy
4.3. Variables and OCOMs for Assessment of the Peripheral Component of Diabetic Neuropathy
4.4. Variables and OCOMs for Assessment of the Proximal Component of Diabetic Neuropathy
4.5. Variables and OCOMs for Assessment of the Autonomic Component of Diabetic Neuropathy
4.6. Variables and OCOM for the Assessment of a Diabetic Autonomic Neuropathy (DAN)
4.7. Variables and OCOMs for Assessment of Peripheral Arterial Disease (PAD) in Diabetes
4.8. Variables and OCOMs for Assessment of the Characteristics of Diabetic Ulcers
4.9. Clinical Recommendations for OCOMs Evaluated in the Review
4.10. Research Recommendations for OCOMs Evaluated in the Review
4.11. Limitations of the Study
5. Conclusion
Author Contributions
Conflicts of Interest
References
- Singh, R.; Kishore, L.; Kaur, N. Diabetic peripheral neuropathy: Current perspective and future directions. Pharmacol. Res. 2014, 80, 21–35. [Google Scholar] [CrossRef]
- Faruque, L.I.; Wiebe, N.; Ehteshami-Afshar, A.; Liu, Y.; Dianati-Maleki, N.; Hemmelgarn, B.R.; Tonelli, M. Effect of telemedicine on glycated hemoglobin in diabetes: A systematic review and meta-analysis of randomized trials. CMAJ Can. Med. Assoc. J. J. Assoc. Med. Can. 2017, 189, E341–E364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roglic, G. ; World Health Organization. Global Report on Diabetes; World Health Organization: Geneva, Switzerland, 2016; p. 86. [Google Scholar]
- Salvo, P.; Calisi, N.; Melai, B.; Dini, V.; Paoletti, C.; Lomonaco, T.; Romanelli, M. Temperature- and pH-sensitive wearable materials for monitoring foot ulcers. Int. J. Nanomed. 2017, 12, 949–954. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kronenberg, M.P.L. Williams Textbook of Endocrinology, 13th ed.; Elsevier: Amsterdam, The Netherlands, 2016; p. 1872. [Google Scholar]
- Shaw, J.E.; Sicree, R.A.; Zimmet, P.Z. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res. Clin. Pract. 2010, 87, 4–14. [Google Scholar] [CrossRef]
- Ibrahim, A. IDF Clinical Practice Recommendation on the Diabetic Foot: A guide for healthcare professionals. Diabetes Res. Clin. Pract. 2017, 127, 285–287. [Google Scholar] [CrossRef]
- Cuesta-Vargas, A.I.; González-Sánchez, M. Ability to discriminate between healthy and low back pain sufferers using ultrasound during maximum lumbar extension. Arch. Phys. Med. Rehabil. 2014, 95, 1093–1099. [Google Scholar] [CrossRef] [PubMed]
- González-Sánchez, M.; Velasco-Ramos, E.; Muñoz, M.R.; Cuesta-Vargas, A.I. Relationship between patient-reported outcome measures (PROM) and three measures of foot-ankle alignment in patients with metatarsal head pain: A cross-sectional study. J. Foot Ankle Res. 2016, 9, 49. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Mokkink, L.B.; Terwee, C.B.; Patrick, D.L.; Alonso, J.; Stratford, P.W.; Knol, D.L.; De Vet, H.C. The COSMIN checklist for assessing the methodological quality of studies on measurement properties of health status measurement instruments: An international Delphi study. Qual. Life Res. 2010, 19, 539–549. [Google Scholar] [CrossRef] [Green Version]
- Papanas, N.; Giassakis, G.; Papatheodorou, K.; Papazoglou, D.; Monastiriotis, C.; Christakidis, D.; Maltezos, E. Use of the new indicator test (Neuropad) for the assessment of the staged severity of neuropathy in type 2 diabetic patients. Exp. Clin. Endocrinol. Diabetes Off. J. Ger. Soc. Endocrinol. Ger. Diabetes Assoc. 2007, 115, 58–61. [Google Scholar] [CrossRef]
- Bracewell, N.; Game, F.; Jeffcoate, W.; Scammell, B.E. Clinical evaluation of a new device in the assessment of peripheral sensory neuropathy in diabetes. Diabet. Med. J. Br. Diabet. Assoc. 2012, 29, 1553–1555. [Google Scholar] [CrossRef] [PubMed]
- Malik, R.A.; Veves, A.; Tesfaye, S.; Smith, G.; Cameron, N.; Zochodne, D.; Toronto Consensus Panel on Diabetic Neuropathy. Small fibre neuropathy: Role in the diagnosis of diabetic sensorimotor polyneuropathy. Diabetes Metab. Res. Rev. 2011, 27, 678–684. [Google Scholar] [CrossRef] [PubMed]
- Shibata, Y.; Himeno, T.; Kamiya, T.; Tani, H.; Nakayama, T.; Kojima, C.; Sugiura-Roth, Y.; Naito, E.; Kondo, M.; Tsunekawa, S.; et al. Validity and reliability of a point-of-care nerve conduction device in diabetes patients. J. Diabetes Investig. 2019, 10, 1291–1298. [Google Scholar] [CrossRef] [PubMed]
- Vileikyte, L.; Hutchings, G.; Hollis, S.; Boulton, A.J. The tactile circumferential discriminator. A new, simple screening device to identify diabetic patients at risk of foot ulceration. Diabetes Care 1997, 20, 623–626. [Google Scholar] [CrossRef]
- Jin, J.; Wang, W.; Gu, T.; Chen, W.; Lu, J.; Bi, Y.; Zhu, D. The Application of SUDOSCAN for Screening Diabetic Peripheral Neuropathy in Chinese Population. Exp. Clin. Endocrinol. Diabetes Off. J. Ger. Soc. Endocrinol. Ger. Diabetes Assoc. 2018, 126, 472–477. [Google Scholar] [CrossRef]
- Bijli, A.H.; Rasool, A.; Wani, A.H.; Yasir, M.; Bhat, T.A.; Laway, B.A. Footboards: Indigenous and Novel Method of Screening for Diabetes Peripheral Neuropathy—A Pilot Study. Indian J. Endocrinol. Metab. 2017, 21, 293–296. [Google Scholar]
- Ejskjaer, N.; Fleischer, J.; Fleischer, J.; Jacobsen, P.E.; Poulsen, P.L.; Nygaard, H. A Pocket-size Device to Detect Autonomic Neuropathy. J. Diabetes Sci. Technol. 2008, 2, 692–696. [Google Scholar] [CrossRef] [Green Version]
- Deng, W.; Dong, X.; Zhang, Y.; Jiang, Y.; Lu, D.; Wu, Q.; Chen, B. Transcutaneous oxygen pressure (TcPO2): A novel diagnostic tool for peripheral neuropathy in type 2 diabetes patients. Diabetes Res. Clin. Pract. 2014, 105, 336–343. [Google Scholar] [CrossRef]
- Masson, E.A.; Veves, A.; Fernando, D.; Boulton, A.J. Current perception thresholds: A new, quick, and reproducible method for the assessment of peripheral neuropathy in diabetes mellitus. Diabetologia 1989, 32, 724–728. [Google Scholar] [CrossRef] [Green Version]
- Ponirakis, G.; Petropoulos, I.N.; Fadavi, H.; Alam, U.; Asghar, O.; Marshall, A.; Malik, R.A. The diagnostic accuracy of Neuropad for assessing large and small fibre diabetic neuropathy. Diabet. Med. J. Br. Diabet. Assoc. 2014, 31, 1673–1680. [Google Scholar] [CrossRef] [Green Version]
- Ponirakis, G.; Odriozola, M.N.; Odriozola, S.; Petropoulos, I.N.; Azmi, S.; Fadavi, H.; Kheyami, A. NerveCheck: An inexpensive quantitative sensory testing device for patients with diabetic neuropathy. Diabetes Res. Clin. Pract. 2016, 113, 101–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, S.; Kerry, C.; Atkins, H.; Rayman, G. The Ipswich Touch Test: A simple and novel method to screen patients with diabetes at home for increased risk of foot ulceration. Diabet Med. 2014, 31, 1100–1103. [Google Scholar] [CrossRef] [PubMed]
- Bril, V.; Kojic, J.; Ngo, M.; Clark, K. Comparison of a neurothesiometer and vibration in measuring vibration perception thresholds and relationship to nerve conduction studies. Diabetes Care 1997, 20, 1360–1362. [Google Scholar] [CrossRef] [PubMed]
- Severinsen, K.; Obel, A.; Jakobsen, J.; Andersen, H. Atrophy of foot muscles in diabetic patients can be detected with ultrasonography. Diabetes Care 2007, 30, 3053–3057. [Google Scholar] [CrossRef] [Green Version]
- Spallone, V.; Morganti, R.; Siampli, M.; Fedele, T.; D’Amato, C.; Cacciotti, L.; Maiello, M.R. Neuropad as a diagnostic tool for diabetic autonomic and sensorimotor neuropathy. Diabet. Med. J. Br. Diabet. Assoc. 2009, 26, 686–692. [Google Scholar] [CrossRef]
- Tehan, P.E.; Bray, A.; Chuter, V.H. Non-invasive vascular assessment in the foot with diabetes: Sensitivity and specificity of the ankle brachial index, toe brachial index and continuous wave Doppler for detecting peripheral arterial disease. J. Diabetes Complicat. 2016, 30, 155–160. [Google Scholar] [CrossRef]
- Ballard, J.L.; Eke, C.C.; Bunt, T.J.; Killeen, J.D. A prospective evaluation of transcutaneous oxygen measurements in the management of diabetic foot problems. J. Vasc. Surg. 1995, 22, 485–492. [Google Scholar] [CrossRef] [Green Version]
- Ma, J.; Liu, M.; Chen, D.; Wang, C.; Liu, G.; Ran, X. The Validity and Reliability between Automated Oscillometric Measurement of Ankle-Brachial Index and Standard Measurement by Eco-Doppler in Diabetic Patients with or without Diabetic Foot. Int. J. Endocrinol. 2017. [Google Scholar] [CrossRef]
- Aragón-Sánchez, J.; Quintana-Marrero, Y.; Aragón-Hernández, C.; Hernández-Herero, M.J. ImageJ: A Free, Easy, and Reliable Method to Measure Leg Ulcers Using Digital Pictures. Int. J. Low Extrem. Wounds 2017, 16, 269–273. [Google Scholar] [CrossRef]
- Foltynski, P.; Ladyzynski, P.; Sabalinska, S.; Wojcicki, J.M. Accuracy and precision of selected wound area measurement methods in diabetic foot ulceration. Diabetes Technol. Ther. 2013, 15, 712–721. [Google Scholar] [CrossRef]
- Jørgensen, L.B.; Skov-Jeppesen, S.M.; Halekoh, U.; Rasmussen, B.S.; Sørensen, J.A.; Jemec, G.B.E.; Yderstraede, K.B. Validation of three-dimensional wound measurements using a novel 3D-WAM camera. Wound Repair Regen 2018, 26, 456–462. [Google Scholar] [CrossRef] [Green Version]
- Hazenberg, C.E.V.B.; van Netten, J.J.; van Baal, S.G.; Bus, S.A. Assessment of signs of foot infection in diabetes patients using photographic foot imaging and infrared thermography. Diabetes Technol. Ther. 2014, 16, 370–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hazenberg, C.E.V.B.; van Baal, J.G.; Manning, E.; Bril, A.; Bus, S.A. The validity and reliability of diagnosing foot ulcers and pre-ulcerative lesions in diabetes using advanced digital photography. Diabetes Technol. Ther. 2010, 12, 1011–1017. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Sheng, M.; Xie, L.; Liu, F.; Yan, G.; Wang, W.; Lin, A.; Zhao, F.; Chen, Y. Tear proteomic analysis of patients with type 2 diabetes and dry eye syndrome by two-dimensional nano-liquid chromatography coupled with tandem mass spectrometry. Investig. Ophthalmol. Vis. Sci. 2014, 55, 177–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yudovsky, D.; Nouvong, A.; Schomacker, K.; Pilon, L. Assessing diabetic foot ulcer development risk with hyperspectral tissue oximetry. J. Biomed. Opt. 2011, 16, 026009. [Google Scholar] [CrossRef] [PubMed]
- Morales Lozano, R.; González Fernández, M.L.; Martinez Hernández, D.; Beneit Montesinos, J.V.; Guisado Jiménez, S.; Gonzalez Jurado, M.A. Validating the probe-to-bone test and other tests for diagnosing chronic osteomyelitis in the diabetic foot. Diabetes Care 2010, 33, 2140–2145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nawaz, A.; Torigian, D.A.; Siegelman, E.S.; Basu, S.; Chryssikos, T.; Alavi, A. Diagnostic performance of FDG-PET, MRI, and plain film radiography (PFR) for the diagnosis of osteomyelitis in the diabetic foot. Mol. Imaging Biol. MIB Off. Publ. Acad. Mol. Imaging 2010, 12, 335–342. [Google Scholar] [CrossRef]
- Ertugrul, M.B.; Baktiroglu, S.; Salman, S.; Unal, S.; Aksoy, M.; Berberoglu, K.; Calangu, S. The diagnosis of osteomyelitis of the foot in diabetes: Microbiological examination vs. magnetic resonance imaging and labelled leucocyte scanning. Diabet. Med. 2006, 23, 649–653. [Google Scholar] [CrossRef]
- Lalkhen, A.G.; McCluskey, A. Clinical tests: Sensitivity and specificity. Contin. Educ. Anaesth. Crit. Care Pain 2008, 8, 221–223. [Google Scholar] [CrossRef] [Green Version]
- Gallagher, E.J. The problem with sensitivity and specificity. Ann. Emerg. Med. 2003, 42, 298–303. [Google Scholar] [CrossRef]
- Ranganathan, P.; Aggarwal, R. Common pitfalls in statistical analysis: Understanding the properties of diagnostic tests—Part 1. Perspect Clin. Res. 2018, 9, 40–43. [Google Scholar] [CrossRef]
- Silva Fuente-Alba, C.; Molina Villagra, M. Likelihood ratio (razón de verosimilitud): Definición y aplicación en Radiología. Rev. Argent. Radiol. 2017, 81, 204–208. [Google Scholar] [CrossRef]
- Said, G. Focal and multifocal diabetic neuropathies. Arq. Neuropsiquiatr. 2007, 65, 1272–1278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papanas, N.; Papatheodorou, K.; Papazoglou, D.; Christakidis, D.; Monastiriotis, C.; Maltezos, E. Reproducibility of the new indicator test for sudomotor function (Neuropad) in patients with type 2 diabetes mellitus: Short communication. Exp. Clin. Endocrinol. Diabetes Off. J. Ger. Soc. Endocrinol. Ger. Diabetes Assoc. 2005, 113, 577–581. [Google Scholar] [CrossRef] [PubMed]
- Ponirakis, G.; Odriozola, M.N.; Odriozola, S.; Petropoulos, I.N.; Azmi, S.; Ferdousi, M.; Miro, A. NerveCheck for the Detection of Sensory Loss and Neuropathic Pain in Diabetes. Diabetes Technol. Ther. 2016, 18, 800–805. [Google Scholar] [CrossRef] [Green Version]
- Wagenaar, I.; Post, E.; Brandsma, W.; Ziegler, D.; Rahman, M.; Alam, K.; Richardus, J.H. Early detection of neuropathy in leprosy: A comparison of five tests for field settings. Infect. Dis. Poverty 2017, 6, 115. [Google Scholar] [CrossRef] [Green Version]
- Wang, F.; Zhang, J.; Yu, J.; Liu, S.; Zhang, R.; Ma, X.; Wang, P. Diagnostic accuracy of monofilament tests for detecting diabetic peripheral neuropathy: A systematic review and meta-analysis. J. Diabetes Res. 2017. [Google Scholar] [CrossRef] [Green Version]
- Aragón Sánchez, F.J.; Lázaro Martínez, J.L. Atlas de Manejo Práctico del Pie Diabético; Aragón Sánchez, F.J., Lázaro Martínez, J.L., Eds.; CPG Ediciones: Barcelona, Spain, 2004; p. 161. [Google Scholar]
- Ansede, G.; Lee, J.C.; Healy, J.C. Musculoskeletal sonography of the normal foot. Skelet. Radiol. 2010, 39, 225–242. [Google Scholar] [CrossRef]
- Crofts, G.; Angin, S.; Mickle, K.J.; Hill, S.; Nester, C.J. Reliability of ultrasound for measurement of selected foot structures. Gait Posture 2014, 39, 35–39. [Google Scholar] [CrossRef]
- Zouari, H.G.; Ng, W.; Tin, S.; Wahab, A.; Damy, T.; Lefaucheur, J.-P. Assessment of autonomic innervation of the foot in familial amyloid polyneuropathy. Eur. J. Neurol. 2019, 26, 94-e10. [Google Scholar] [CrossRef] [Green Version]
- Xu, X.; Liao, J.; Dong, Q.; Qin, F.; Li, J.; Sun, X.; Qiu, W. Clinical utility of SUDOSCAN in predicting autonomic neuropathy in patients with Parkinson’s disease. Parkinsonism Relat. Disord. 2019, 64, 60–65. [Google Scholar] [CrossRef]
- Fleischer, J.; Nielsen, R.; Laugesen, E.; Nygaard, H.; Poulsen, P.L.; Ejskjaer, N. Self-monitoring of cardiac autonomic function at home is feasible. J. Diabetes Sci. Technol. 2011, 5, 107–112. [Google Scholar] [CrossRef] [Green Version]
- Gulichsen, E.; Fleischer, J.; Ejskjaer, N.; Eldrup, E.; Tarnow, L. Screening for diabetic cardiac autonomic neuropathy using a new handheld device. J. Diabetes Sci. Technol. 2012, 6, 965–972. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bundó, M.; Urrea, M.; Muñoz-Ortíz, L.; Pérez, C.; Llussà, J.; Forés, R.; Torán, P. Measurement of the ankle brachial index with a non-mercury sphygmomanometer in diabetic patients: A concordance study. BMC Cardiovasc. Disord. 2013, 13, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brooks, B.; Dean, R.; Patel, S.; Wu, B.; Molyneaux, L.; Yue, D.K. TBI or not TBI: That is the question. Is it better to measure toe pressure than ankle pressure in diabetic patients? Diabet. Med. J. Br. Diabet. Assoc. 2001, 18, 528–532. [Google Scholar] [CrossRef]
- Ladurner, R.; Kueper, M.; Königsrainer, I.; Löb, S.; Wichmann, D.; Koenigsrainer, A.; Beckert, S. Predictive value of routine transcutaneous tissue oxygen tension (tcpO2) measurement for the risk of non-healing and amputation in diabetic foot ulcer patients with non-palpable pedal pulses. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2010, 16, CR273–CR277. [Google Scholar]
- Nabuurs-Franssen, M.H.; Houben, A.J.; Tooke, J.E.; Schaper, N.C. The effect of polyneuropathy on foot microcirculation in Type II diabetes. Diabetologia 2002, 45, 1164–1171. [Google Scholar] [PubMed] [Green Version]
- Senneville, E.M.; Lipsky, B.A.; van Asten, S.A.V.; Peters, E.J. Diagnosing diabetic foot osteomyelitis. Diabetes Metab. Res. Rev. 2020, e3250. [Google Scholar] [CrossRef] [Green Version]
- Li, X.H.; Guan, L.Y.; Lin, H.Y.; Wang, S.H.; Cao, Y.Q.; Jiang, X.Y.; Wang, Y.B. Fibrinogen: A Marker in Predicting Diabetic Foot Ulcer Severity. J. Diabetes Res. 2016, 2016, 2358321. [Google Scholar] [CrossRef]
- Jørgensen, L.B.; Sørensen, J.A.; Jemec, G.B.; Yderstraede, K.B. Methods to assess area and volume of wounds—A systematic review. Int. Wound J. 2016, 13, 540–553. [Google Scholar] [CrossRef]
- Bandyk, D.F. The diabetic foot: Pathophysiology, evaluation, and treatment. Semin. Vasc. Surg. 2018, 31, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Hirschfeld, G.; von Glischinski, M.; Knop, C.; Wiesel, T.; Reinehr, T.; Aksu, F.; Zernikow, B. Difficulties in screening for peripheral neuropathies in children with diabetes. Diabet. Med. J. Br. Diabet. Assoc. 2015, 32, 786–789. [Google Scholar] [CrossRef] [PubMed]
- Maiya, A.G.; Parameshwar, A.; Hande, M.; Nandalike, V. Relationship between Glycated Hemoglobin and Vibration Perception Threshold in Diabetic Peripheral Neuropathy. Int. J. Low Extrem. Wounds 2019. [Google Scholar] [CrossRef] [PubMed]
- Sima, A.A.F.; Kamiya, H. Diabetic neuropathy differs in type 1 and type 2 diabetes. Ann. N. Y. Acad. Sci. 2006, 1084, 235–249. [Google Scholar] [CrossRef]


{kind=link}
| Variable | OCOM | Aut | Type | n | Sens (%) | Spec (%) | PPV (%) | NPV (%) | Lr+ | Lr− | AUC-ROC (%) | Gold Standard (GS) | Agreement with GS | Inter-Rater | Intra-Rater |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Assessment of peripheral neuropathy * | Neuropad | Papanas et al. 2007 [12] | 2 | 120 | 93 to 100 | 97 to 100 | _ | _ | _ | _ | _ | MNSI | tau-b = 0.848 | _ | _ |
| 10-g monofilament | Bracewell et al., 2012 [13] | 1/2 | 141 | 84 | 83 | 78 | 88 | 5.01 | 0.19 | _ | Neurothesiometer | _ | _ | _ | |
| Neurotip | Bracewell et al., 2012 [13] | 1/2 | 141 | 74 | 83 | 75 | 82 | 4.4 | 0.31 | _ | Neurothesiometer | _ | _ | _ | |
| 128 Hz tuning fork | Bracewell et al., 2012 [13] | 1/2 | 141 | 69 | 90 | 81 | 83 | 7.16 | 0.34 | _ | Neurothesiometer | _ | _ | _ | |
| VibraTip | Bracewell et al., 2012 [13] | 1/2 | 141 | 79 | 82 | 75 | 85 | 4.39 | 0.25 | _ | Neurothesiometer | _ | _ | r = 0.88 (n =18) | |
| NeurAp-pathy App | Maliket al., 2011 [14] | 1/2 | 61 | 80 | 95 | 94 | 83 | _ | _ | _ | _ | Accuracy = 88% | _ | _ | |
| DPN-Check | Shibata et al., 2019 [15] | 1/2 | 57 | 86.5 | 43.8 | _ | _ | _ | _ | 0.582; 0.696 | Sural nerve conduction velocity (SNCV); Sural nerve conduction amplitude | r = 0.81; r = 0.62 | ICC: 0.807; 0.783 | ICC: 0.842; 0.877 | |
| Tactile Circunferencial Discriminator (TDC) | Vileikyte et al., 1997 [16] | 1/2 | 133 | 92.3 | 64.2 | _ | _ | _ | _ | _ | Biosthesiometer; S-W Monofilament | r2 = 0.76; r2 = 0.73 | _ | _ | |
| Sudoscan | Jin et al., 2017 [17] | 2 | 60 | 88.2 to 89.8 | 41.2 to 46.9 | _ | _ | _ | _ | 0.61 to 0.713 | NCS | _ | _ | _ | |
| Footboard (FB) | Bijli et al., 2017 [18] | _ | 244 | 63 to 100 | 9 to 90 | 58 to 93 | 48 to 100 | _ | _ | _ | S-W monofilament; 128 Hz tuning-fork | _ | _ | ||
| Diabetic autonomic neuropathy (DAN) | Vagus® | Ejskjaer et al., 2008 [19] | 1 | 18/323 | - | - | - | - | - | - | - | Varia Pulse TF3 | r2 = 0.81–0.98 | 0.66–0.94 | 0.85–0.91 |
| Transcutaneous partial pressure of oxygen (TcPO2) * | TCM 400 system | Deng et al., 2014 [20] | 2 | 381 | 61.1 | 73.8 | _ | _ | _ | _ | 0.722 | NCS | p < 0.01 | _ | _ |
| Current perception threshold * | Neurometer | Masson et al., 1989 [21] | 1/2 | 121 | _ | _ | _ | _ | _ | _ | _ | Peroneal motor conduction velocity; Biosthesiometer; Thermoesthesiometer | PCC: (−0.66); 0.69; 0.69. | _ | _ |
| Assessment of small fiber diabetic neuropathy * | Neuropad | Ponirakis et al., 2014 [22] | 1/2 | 127 | 68 to 83 | 49 to 80 | 26 to 54 | 44 to 95 | 1.33 to 4.15 | 0.21 to 0.65 | 0.60 to 0.85 | MEDOC TSA II; Corneal nerve fiber density and length | _ | _ | _ |
| NerveCheck (cold perception part only) | Ponirakis et al., 2016 [23] | _ | 130 | 53; 67 | 82; 85 | _ | _ | _ | _ | 0.7; 0.78 | Intradermal epidermic nerve fiber density; Corneal nerve fiber density | _ | |||
| Assessment of large fiber diabetic neuropathy * | Neuropad | Ponirakis et al., 2014 [22] | 1/2 | 127 | 64 to 83 | 50 to 64 | 26 to 63 | 39 to 91 | 1.39 to 1.94 | 0.32 to 0.67 | 0.66 to 0.73 | NCS; neurothesiometer; NDS | _ | _ | _ |
| NerveCheck (vibration perception part only) | Ponirakis et al., 2016 [23] | _ | 130 | 88 | 82 | _ | _ | _ | _ | 0.84 | SNCV | ||||
| Assessing nerve conduction * | Electromyograph (EMG) | Shibata et al., 2019 [15] | 1/2 | 57 | 96.2 | 40.6 | 71.4 | 66.7 | _ | _ | 0.615; 0.721 | DPN Check | _ | ICC: 0.74–0.79 | ICC:0.52−0.88 |
| Loss of foot sensation * | Ipswich Touch Test | Sharma et al., 2014 [24] | _ | 331 | 78.3 to 81.2 | 93.9 to 96.4 | 81.2 to 89.9 | 92.8 to 96.9 | 12.9 to 15 | 0.05 to 0.23 | 0.87 to 0.97 | 10-g Neuropen monofilament | _ | _ | _ |
| NerveCheck | Ponirakis et al., 2016 [23] | _ | 130 | 84 | 81 | _ | _ | 4.36 | _ | 0.72 to 0.86 | Neurothesiometer; TSA-II-NeuroSensory Analyser | _ | _ | 0.71–0.86 | |
| Vibration perception thresholds * | Neurothesiometer | Bril et al., 1997 [25] | _ | 152 | _ | _ | _ | _ | _ | _ | _ | NCS | r2 = 0.228–0.307 | _ | _ |
| Vibratron | Bril et al., 1997 [25] | _ | 152 | _ | _ | _ | _ | _ | _ | _ | NCS | r2 = 0.042–0.120 | _ | _ | |
| NerveCheck | Ponirakis et al., 2016 [23] | _ | 130 | 88 | 82 | _ | _ | _ | _ | 0.82 to 0.84 | SNCV; sural nerve action potential | _ | _ | _ | |
| Neuropathic pain * | NerveCheck | Ponirakis et al., 2016 [23] | _ | 130 | 40 to 70 | 68 to 84 | _ | _ | _ | _ | 0.7 | McGill Pain Questionnaire | _ | _ | _ |
| Cold perception testing * | NerveCheck | Ponirakis et al., 2016 [23] | _ | 130 | 53 | 82 | _ | _ | _ | _ | 0.7 | Intradermal epidermic nerve fiber density | _ | _ | _ |
| Warm perception testing * | NerveCheck | Ponirakis et al., 2016 [23] | _ | 130 | 56 | 81 | _ | _ | _ | _ | 0.71 | Intradermal epidermic nerve fiber density | _ | _ | _ |
| Atrophy of foot muscles ** | Ultrasonography | Severinsen et al., 2007 [26] | 1/2 | 52 | _ | _ | _ | _ | _ | _ | _ | MRI | r2=0.71–0.77 | _ | _ |
| Assessment of autonomic neuropathy *** | Sudoscan | Jin et al., 2017 [17] | 2 | 60 | 73.9 to 85.6 | 67.3 to 76.1 | _ | _ | _ | _ | 0.704 to 0.859 | NCS | _ | _ | _ |
| Neuropad | Spallone et al., 2009 [27] | 1/2 | 51 | 73 to 82 | 27 to 75 | 24 to 44 | 85 to 91 | 1.13 to 2.92 | 0.34 to 0.67 | 0.71 | “Deep breathing. lying to standing. Valsalva and postural hypotension tests” | _ | _ | _ |
| Variable | OCOM | Aut | Type | n | Sens (%) | Spec (%) | PPV (%) | NPV (%) | Lr+ | Lr− | AUC-ROC (%) | Gold standard (GS) | Agreement with GS | Inter-rater | Intra-rater |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Peripheral arterial disease | Ankle Brachial Index (ABI) | Tehan et al., 2015 [28] | _ | 117 | 45.16 | 92.68 | 82.35 | 69.09 | 6.17 | 0.59 | 0.58 | Color Duplex Ultrasound | _ | _ | ICC = 0.62 |
| Toe Brachial Index (TBI) | Tehan et al., 2015 [28] | _ | 117 | 63.64 | 82.05 | 75 | 72.73 | 10.39 | 0.28 | 0.75 | Color Duplex Ultrasound | _ | _ | ICC = 0.8 | |
| Transcutaneous partial pressure of oxygen (TcPO2) | Novametrix 800 monitor | Ballard et al., 1995 [29] | 1/2 | 55 | 98 | 44 | 91 | 80 | _ | _ | _ | _ | Accuracy: 90% | _ | _ |
| Measurement of ABI | OMRON BP-203RPEIII | Ma et al., 2017 [30] | _ | 230 | 94.5 | 98.99 | _ | _ | 55.12 | 0.056 | 0.981 | Eco-Doppler | K = 0.928 | _ | _ |
| VARIABLE | OCOM | AUT | TYPE | n | SENS (%) | SPEC (%) | PPV (%) | NPV (%) | LR+ | LR− | AUC-ROC (%) | GOLD STANDARD (GS) | AGREEMENT WITH GS | INTER-RATER | INTRA-RATER |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Wound area measurement | ImageJ | Aragón-Sánchez et al., 2017 [31] | _ | 25 | _ | _ | _ | _ | _ | _ | _ | _ | _ | ICC = 1 | ICC = 0.99 |
| SilhouetteMobile | Foltynski et al., 2013 [32] | _ | 16 | _ | _ | _ | _ | _ | _ | _ | Elliptical method | MAE = 1.7 to 4.5 | _ | _ | |
| VisiTrak | Foltynski et al., 2013 [32] | _ | 16 | _ | _ | _ | _ | _ | _ | _ | Elliptical method | MAE = 1.8 to 3 | _ | _ | |
| TeleDiaFos | Foltynski et al., 2013 [32] | _ | 16 | _ | _ | _ | _ | _ | _ | _ | Elliptical method | MAE = 1.7 to 12.9 | _ | _ | |
| Wound area and volume measurement | 3D Wound Assessment Camera | Jorgensen et al., 2018 [33] | _ | 47 | _ | _ | _ | _ | _ | _ | _ | 3D camera; gel injection | ICC = 0.975 ICC = 0.977 | ICC = 0.946 to 0.999 | ICC = 0.971 to 0.997 |
| Assessment of foot infection | Photographic Foot Imaging Device (PFID) | Hazenberg et al., 2014 [34] | _ | 38 | 57 | 86 | 73 | 76 | _ | _ | _ | Live assessment | _ | ICC = 0.44 | ICC = 0.52 to 0.77 |
| Diagnosis of ulcer | PFID | Hazenberg et al., 2010 [35] | _ | 32 | 88 | 98 | _ | _ | _ | _ | _ | Live assessment | Kappa = 0.87 | ICC = 0.74 to 0.88 | ICC = 0.91 to 1 |
| Diagnosis of callus | PFID | Hazenberg et al., 2010 [35] | _ | 32 | 69 | 89 | _ | _ | _ | _ | _ | Live assessment | Kappa = 0.61 | ICC = 0.52 to 0.73 | ICC = 0.7 to 1 |
| Diagnosis of absence of signs | PFID | Hazenberg et al., 2010 [35] | _ | 32 | 90 | 90 | _ | _ | _ | _ | _ | Live assessment | Kappa = 0.83 | ICC = 0.62 to 0.73 | ICC = 0.89 to 1 |
| Severity of diabetic foot ulcer | Plasma fibrinogen via immunoturbidimetric assay | Li et al., 2014 [36] | _ | 152 | 80.9 | 82.6 | 78.6 | 89 | _ | _ | 0.858 | Neutrophil counting; white blood cell counting, C-reactive protein | SCC = 0.614; 0.616; 0.705 | _ | _ |
| Predicting risk of ulcer formation | Hyperspectral imaging device | Yudovsky et al., 2011 [37] | 1/2 | 66 | 0 to 100 | 72 to 100 | _ | _ | _ | _ | 0.89 | _ | _ | _ | _ |
| Diagnosis of osteomielitis | Probe-to-bone test | Morales-Lozano et al., 2016 [38] | 1/2 | 132 | 98.1 | 77.78 | 94.5 | 91.3 | 4.45 | 0.02 | _ | Intraoperative histology and culture | Kappa = 0.803 | _ | _ |
| Plain radiography | Nawaz et al. 2009 [39] | _ | 110 | 63 | 87 | 60 | 88 | _ | _ | _ | Intraoperative histology and culture | Accuracy = 81% | _ | _ | |
| [18F]-2-fluoro-2-deoxy-Dglucose (FDG)-positron emission tomography (PET) | Nawaz et al. 2009 [39] | _ | 110 | 81 | 93 | 78 | 94 | _ | _ | _ | Intraoperative histology and culture | Accuracy = 90% | _ | _ | |
| MRI | Nawaz et al. 2009 [39] | _ | 110 | 91 | 78 | 96 | 57 | _ | _ | _ | Intraoperative histology and culture | Accuracy = 81% | _ | _ | |
| Leucocyte counting | Ertugrul et al., 2006 [40] | _ | 31 | 91 | 67 | 95 | 50 | _ | _ | _ | CT scan contrast with Tc99 | _ | _ | _ |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-Torres, R.; Ruiz-Muñoz, M.; Pérez-Panero, A.J.; García-Romero, J.; Gónzalez-Sánchez, M. Instruments of Choice for Assessment and Monitoring Diabetic Foot: A Systematic Review. J. Clin. Med. 2020, 9, 602. https://doi.org/10.3390/jcm9020602
Fernández-Torres R, Ruiz-Muñoz M, Pérez-Panero AJ, García-Romero J, Gónzalez-Sánchez M. Instruments of Choice for Assessment and Monitoring Diabetic Foot: A Systematic Review. Journal of Clinical Medicine. 2020; 9(2):602. https://doi.org/10.3390/jcm9020602
Chicago/Turabian StyleFernández-Torres, Raúl, María Ruiz-Muñoz, Alberto J. Pérez-Panero, Jerónimo García-Romero, and Manuel Gónzalez-Sánchez. 2020. "Instruments of Choice for Assessment and Monitoring Diabetic Foot: A Systematic Review" Journal of Clinical Medicine 9, no. 2: 602. https://doi.org/10.3390/jcm9020602