The Effectiveness of Psychological Treatments in Women with Breast Cancer: A Systematic Review and Meta-Analysis

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Method
2.2. Research Strategies
2.3. Eligibility Criteria
2.4. Study Selection
2.5. Data Collection
2.6. Data Synthesis
2.7. Qualitative Assessment
2.8. Quantitative Analysis
3. Results
3.1. Study Selection
3.2. Characteristics of Included Studies
3.3. Qualitative Assessment of the Risk of Bias
3.4. Overall Effect Size Considering Differences between Intervention and Control Group after the Treatment
3.5. Anxiety
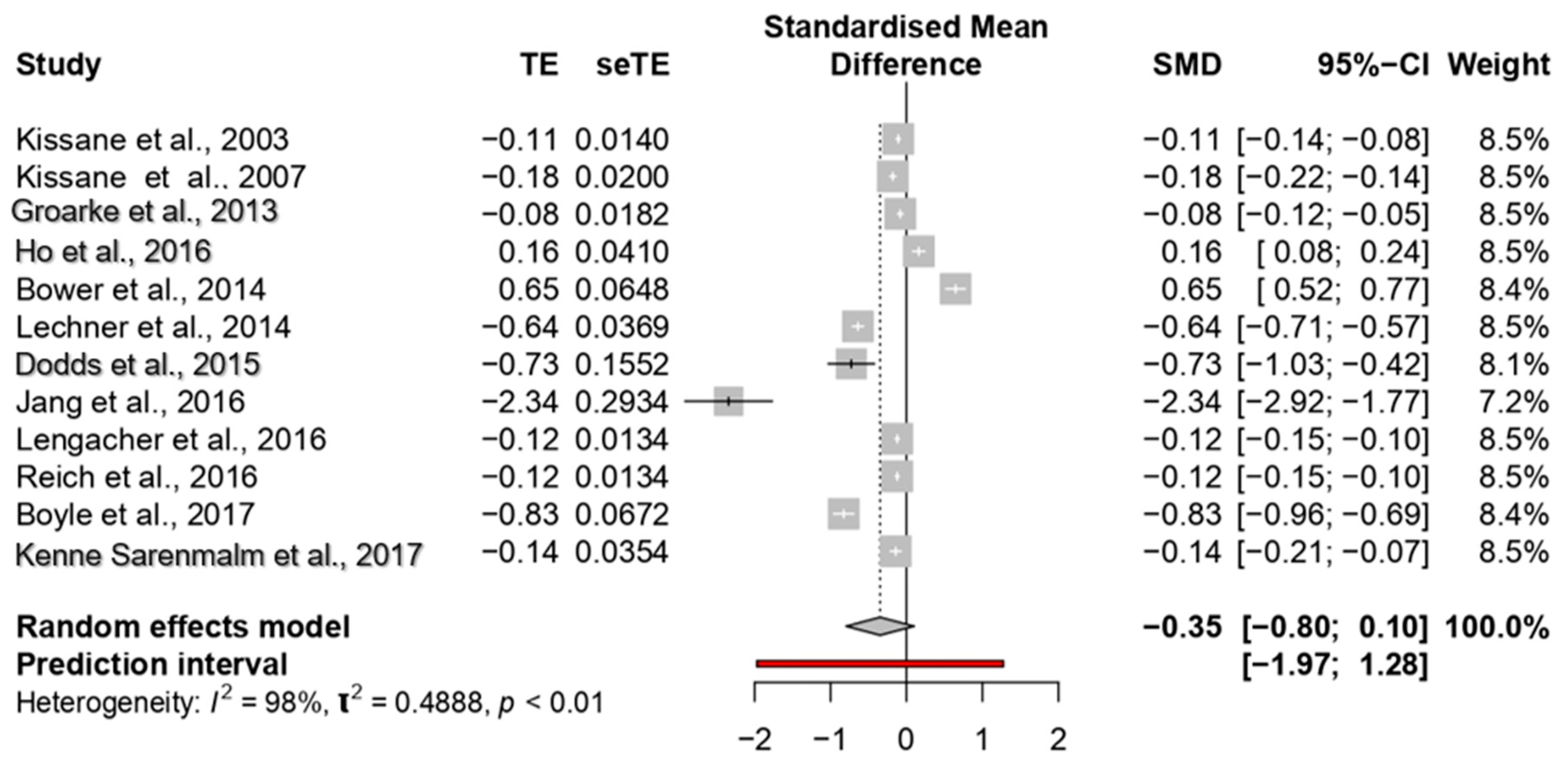
3.6. Depression
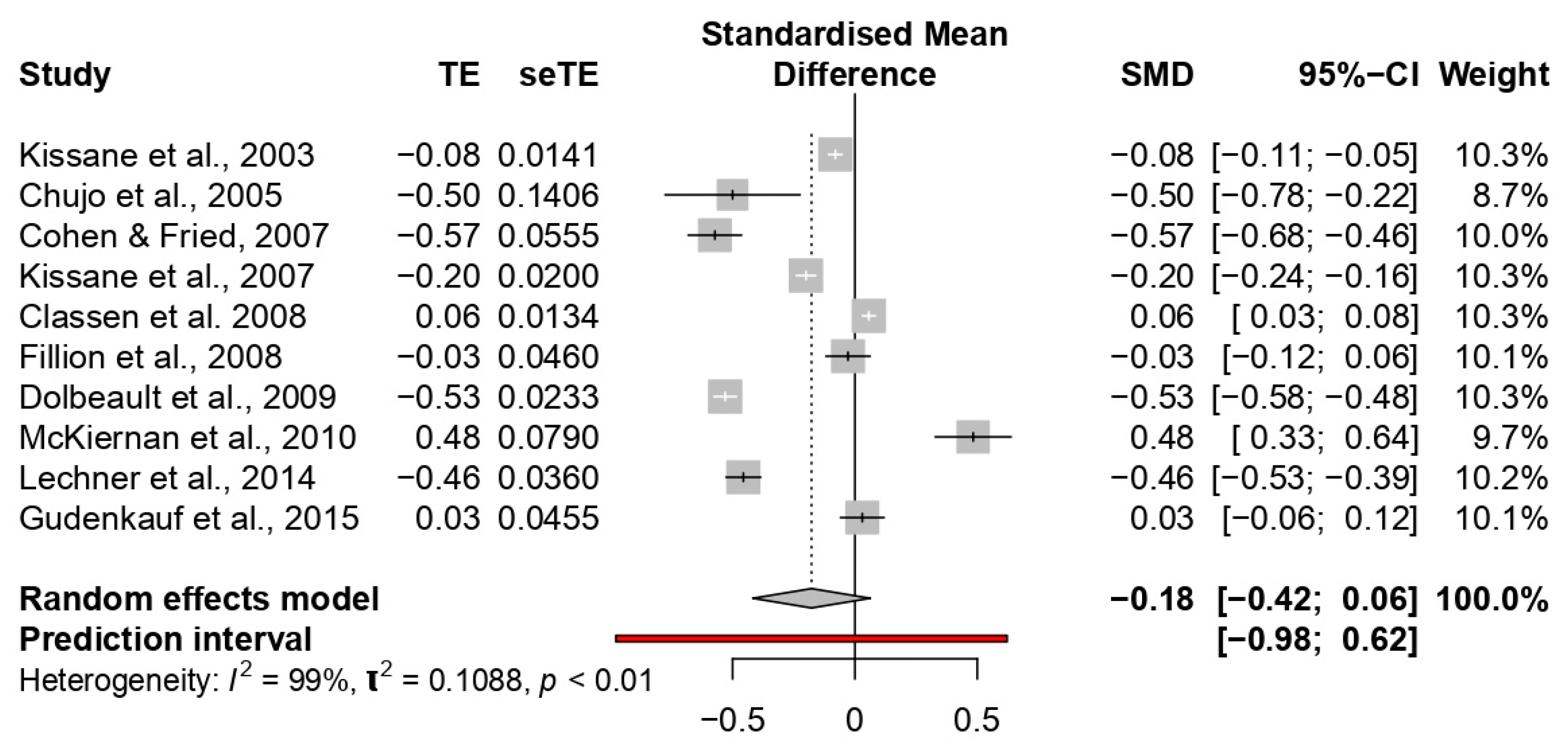
3.7. Mood
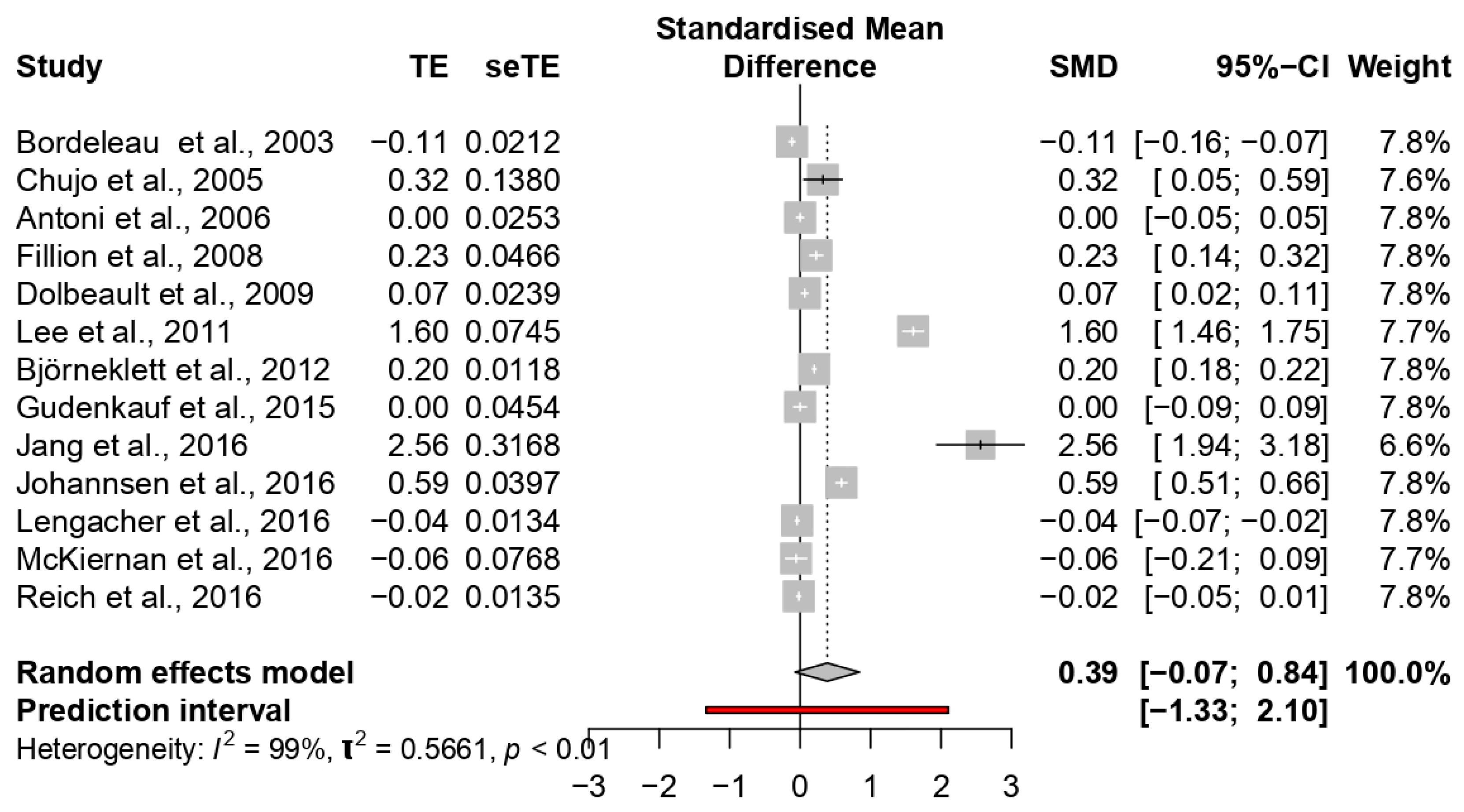
3.8. Quality of Life
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- DeSantis, C.; Ma, J.; Bryan, L.; Jemal, A. Breast cancer statistics. CA Cancer J. Clin. 2014, 64, 52–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGuire, S. World cancer report Geneva, Switzerland: World Health Organization, international agency for research on cancer, WHO Press, 2015. Adv. Nutr. 2016, 7, 418–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stagl, J.M.; Bouchard, L.C.; Lechner, S.C.; Blomberg, B.B.; Gudenkauf, L.M.; Jutagir, D.R.; Glück, S.; Derhagopian, R.P.; Carver, C.S.; Antoni, M.H. Long-term psychological benefits of cognitive-behavioral stress management for women with breast cancer: 11-year follow-up of a randomized controlled trial. Cancer 2015, 121, 1873–1881. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rojas, K.; Stuckey, A. Breast cancer epidemiology and risk factors. Clin. Obstet. Gynecol. 2016, 59, 651–672. [Google Scholar] [CrossRef] [PubMed]
- Howlader, N.; Noone, A.M.; Krapcho, M.; Miller, D.; Bishop, K.; Altekruse, S.F.; Mariotto, A. SEER cancer statistics review, 1975–2013, National Cancer Institute. Bethesda 2016, 1–7. [Google Scholar]
- Klein, D.; Mercier, M.; Abeilard, E.; Puyraveau, M.; Danzon, A.; Dalstein, V.; Velten, M. Long-term quality of life after breast cancer: A French registry-based controlled study. Breast Cancer Res. Treat. 2011, 129, 125–134. [Google Scholar] [CrossRef] [Green Version]
- Koch, L.; Bertram, H.; Eberle, A.; Holleczek, B.; Schmid-Höpfner, S.; Waldmann, A.; Arndt, V. Fear of recurrence in long-term breast cancer survivors—Still an issue. Results on prevalence, determinants, and the association with quality of life and depression from the Cancer Survivorship—A multi-regional population-based study. Psycho-Oncology 2014, 23, 547–554. [Google Scholar] [CrossRef]
- Gallagher, J.; Parle, M.; Cairns, D. Appraisal and psychological distress six months after diagnosis of breast cancer. Br. J. Health Psychol. 2002, 7, 365–376. [Google Scholar] [CrossRef]
- Zabora, J.; BrintzenhofeSzoc, K.; Curbow, B.; Hooker, C.; Piantadosi, S. The prevalence of psychological distress by cancer site. Psycho-Oncology 2001, 10, 19–28. [Google Scholar] [CrossRef]
- Kissane, D.W.; Ildn, J.; Bloch, S.; Vitetta, L.; Clarke, D.M.; Smith, G.C.; McKenzie, D.P. Psychological morbidity and quality of life in Australian women with early-stage breast cancer: A cross-sectional survey. Med. J. Aust. 1998, 169, 192–196. [Google Scholar] [CrossRef]
- Fann, J.R.; Thomas-Rich, A.M.; Katon, W.J.; Cowley, D.; Pepping, M.; McGregor, B.A.; Gralow, J. Major depression after breast cancer: A review of epidemiology and treatment. Gen. Hosp. Psychiatry 2008, 30, 112–126. [Google Scholar] [CrossRef] [PubMed]
- Tang, L.; Fritzsche, K.; Leonhart, R.; Pang, Y.; Li, J.; Song, L.; Fischer, I.; Koch, M.; Wuensch, A.; Mewes, R.; et al. Emotional distress and dysfunctional illness perception are associated with low mental and physical quality of life in Chinese breast cancer patients. Health Qual. Life Outcomes 2017, 15, 231. [Google Scholar] [CrossRef] [PubMed]
- Galiano-Castillo, N.; Ariza-García, A.; Cantarero-Villanueva, I.; Fernández-Lao, C.; Díaz-Rodríguez, L.; Arroyo-Morales, M. Depressed mood in breast cancer survivors: Associations with physical activity, cancer-related fatigue, quality of life, and fitness level. Eur. J. Oncol. Nurs. 2014, 18, 206–210. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, A.; Yamaoka, K.; Tango, T.; Matsuda, T.; Nishimoto, H. Effectiveness of psychoeducational support on quality of life in early-stage breast cancer patients: A systematic review and meta-analysis of randomized controlled trials. Qual. Life Res. 2014, 23, 21–30. [Google Scholar] [CrossRef] [Green Version]
- Denieffe, S.; Gooney, M. A meta-synthesis of women’s symptoms experience and breast cancer. Eur. J. Cancer 2011, 20, 424–435. [Google Scholar] [CrossRef]
- Antoni, S.; Ferlay, J.; Soerjomataram, I.; Znaor, A.; Jemal, A.; Bray, F. Bladder cancer incidence and mortality: A global overview and recent trends. Eur. Urol. 2017, 71, 96–108. [Google Scholar] [CrossRef]
- Cohee, A.A.; Adams, R.N.; Fife, B.L.; Von Ah, D.M.; Monahan, P.O.; Zoppi, K.A.; Cella, D.; Champion, V.L. Relationship Between Depressive Symptoms and Social Cognitive Processing in Partners of Long-Term Breast Cancer Survivors. Oncol. Nurs. Forum 2017, 44, 44–51. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, M.E.; Wiskemann, J.; Steindorf, K. Quality of life, problems, and needs of disease-free breast cancer survivors 5 years after diagnosis. Qual. Life Res. 2018, 27, 2077–2086. [Google Scholar] [CrossRef]
- Fiszer, C.; Dolbeault, S.; Sultan, S.; Brédart, A. Prevalence, intensity, and predictors of the supportive care needs of women diagnosed with breast cancer: A systematic review. Psycho-Oncology 2014, 23, 361–374. [Google Scholar] [CrossRef]
- Cobeanu, O.; David, D. Alleviation of Side Effects and Distress in Breast Cancer Patients by Cognitive-Behavioral Interventions: A Systematic Review and Meta-analysis. J. Clin. Psychol. Med. 2018, 25, 335–355. [Google Scholar] [CrossRef]
- Font, A.; Rodríguez, E. Eficacia de las intervenciones psicológicas en mujeres con cáncer de mama. Psicooncología 2007, 4, 423. [Google Scholar]
- Ye, M.; Du, K.; Zhou, J.; Zhou, Q.; Shou, M.; Hu, B.; Jiang, P.; Dong, N.; He, L.; Liang, S.; et al. A meta-analysis of the efficacy of cognitive behavior therapy on quality of life and psychological health of breast cancer survivors and patients. Psycho-Oncology 2018, 27, 1695–1703. [Google Scholar] [CrossRef]
- Lantheaume, S.; Montagne, M.; Shankland, R. Intervention focused on resources to reduce anxiety and depression disorders in cancer patients: A pilot study. L’Encephale 2019. [Google Scholar] [CrossRef]
- Kissane, D.W.; Bloch, S.; Smith, G.C.; Miach, P.; Clarke, D.M.; Ikin, J.; McKenzie, D. Cognitive-existential group psychotherapy for women with primary breast cancer: A randomised controlled trial. Psycho-Oncology 2003, 12, 532–546. [Google Scholar] [CrossRef]
- Antoni, M.H.; Lechner, S.C.; Kazi, A.; Wimberly, S.R.; Sifre, T.; Urcuyo, K.R.; Carver, C.S. How stress management improves quality of life after treatment for breast cancer. J. Consult. Clin. Psychol. 2006, 74, 1143. [Google Scholar] [CrossRef]
- Keefe, F.J. Cognitive behavioral therapy for managing pain. Clin. Psychol. 1996, 49, 4–5. [Google Scholar]
- Classen, C.C.; Kraemer, H.C.; Blasey, C.; Giese-Davis, J.; Koopman, C.; Palesh, O.G.; Morrow, G.R. Supportive–expressive group therapy for primary breast cancer patients: A randomized prospective multicenter trial. Psycho-Oncology 2008, 17, 438–447. [Google Scholar] [CrossRef] [Green Version]
- Ochoa, C.; Casellas-Grau, A.; Vives, J.; Font, A.; Borràs, J.M. Positive psychotherapy for distressed cancer survivors: Posttraumatic growth facilitation reduces posttraumatic stress. Int. J. Clin. Health Psychol. 2017, 17, 28–37. [Google Scholar] [CrossRef] [Green Version]
- Wu, P.H.; Chen, S.W.; Huang, W.T.; Chang, S.C.; Hsu, M.C. Effects of a Psychoeducational Intervention in Patients with Breast Cancer Undergoing Chemotherapy. Nurs. Res. 2018, 20, 266–279. [Google Scholar] [CrossRef]
- Ho, R.T.; Fong, T.C.; Lo, P.H.; Ho, S.M.; Lee, P.W.; Leung, P.P.; Chan, C.L. Randomized controlled trial of supportive-expressive group therapy and body-mind-spirit intervention for Chinese non-metastatic breast cancer patients. Support. Care Cancer 2016, 24, 4929–4937. [Google Scholar] [CrossRef] [Green Version]
- Cipolletta, S.; Simonato, C.; Faccio, E. The effectiveness of psychoeducational support groups for women with breast cancer and their caregivers: A mixed methods study. Front. Psychol. 2019, 10. [Google Scholar] [CrossRef] [PubMed]
- Dolbeault, S.; Cayrou, S.; Bredart, A.; Viala, A.L.; Desclaux, B.; Saltel, P.; Dickes, P. The effectiveness of a psycho-educational group after early-stage breast cancer treatment: Results of a randomized French study. Psycho-Oncology 2009, 18, 647–656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chujo, M.; Mikami, I.; Takashima, S.; Saeki, T.; Ohsumi, S.; Aogi, K.; Okamura, H. A feasibility study of psychosocial group intervention for breast cancer patients with first recurrence. Support. Care Cancer 2005, 13, 503–514. [Google Scholar] [CrossRef] [PubMed]
- Fillion, L.; Gagnon, P.; Leblond, F.; Gélinas, C.; Savard, J.; Dupuis, R.; Larochelle, M. A brief intervention for fatigue management in breast cancer survivors. Cancer Nurs. 2008, 31, 145–159. [Google Scholar] [CrossRef] [PubMed]
- Naaman, S.C.; Radwan, K.; Fergusson, D.; Johnson, S. Status of psychological trials in breast cancer patients: A report of three meta-analyses. Psychiatry 2009, 72, 50–69. [Google Scholar] [CrossRef]
- Jassim, G.A.; Whitford, D.L.; Hickey, A.; Carter, B. Psychological interventions for women with non-metastatic breast cancer. Cochrane Database Syst. Rev. 2015, 5. [Google Scholar] [CrossRef]
- Fukui, S.; Kugaya, A.; Okamura, H.; Kamiya, M.; Koike, M.; Nakaniski, T.; Imoto, S.; Kanagawa, K.; Uchitomi, Y. A psychosocial group intervention for Japanese women with primary breast carcinoma. Cancer 2000, 89, 1026–1036. [Google Scholar] [CrossRef]
- Phillips, K.M.; Antoni, M.H.; Lechner, S.C.; Blomberg, B.B.; Llabre, M.M.; Avisar, E.; Carver, C.S. Stress management intervention reduces serum cortisol and increases relaxation during treatment for nonmetastatic breast cancer. Psychosom. Med. 2008, 70, 1044–1049. [Google Scholar] [CrossRef] [Green Version]
- Matthews, H.; Grunfeld, E.A.; Turner, A. The efficacy of interventions to improve psychosocial outcomes following surgical treatment for breast cancer: A systematic review and meta-analysis. Psycho-Oncology 2007, 26, 593–607. [Google Scholar] [CrossRef] [Green Version]
- Chow, K.M.; Chan, J.C.; Choi, K.K.; Chan, C.W. A review of psychoeducational interventions to improve sexual functioning, quality of life, and psychological outcomes in gynecological cancer patients. Cancer Nurs. 2016, 39, 20–31. [Google Scholar] [CrossRef]
- Myrhaug, HT.; Mbalilaki, J.A.; Lie, N.K.; Hansen, T.; Nordvik, J.E. The effects of multidisciplinary psychosocial interventions on adult cancer patients: A systematic review and meta-analysis. Disabil. Rehabil. 2018, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Johannsen, M.; Farver, I.; Beck, N.; Zachariae, R. The efficacy of psychosocial intervention for pain in breast cancer patients and survivors: A systematic review and meta-analysis. Breast Cancer Res. Treat. 2013, 138, 675–690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, M.; Huang, L.; Feng, Z.; Shao, L.; Chen, L. Effects of cognitive behavioral therapy on quality of life and stress for breast cancer survivors: A meta-analysis. Min. Med. 2017, 108, 84–93. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Prisma Group. Reprint—Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Phys. Ther. 2009, 89, 873–880. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Erlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Sidik, K.; Jonkman, J.N. A comparison of heterogeneity variance estimators in combining results of studies. Stat. Med. 2007, 26, 1964–1981. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Groarke, A.; Curtis, R.; Kerin, M. Cognitive-behavioural stress management enhances adjustment in women with breast cancer. Br. J. Health Psychol. 2013, 18, 623–641. [Google Scholar] [CrossRef]
- Jang, S.H.; Kang, S.Y.; Lee, H.J.; Lee, S.Y. Beneficial effect of mindfulness-based art therapy in patients with breast cancer—A randomized controlled trial. Explore 2016, 12, 333–340. [Google Scholar] [CrossRef] [Green Version]
- Johannsen, M.; O’Connor, M.; O’Toole, M.S.; Jensen, A.B.; Højris, I.; Zachariae, R. Efficacy of mindfulness-based cognitive therapy on late post-treatment pain in women treated for primary breast cancer: A randomized controlled trial. J. Clin. Oncol. 2016, 34, 3390–3399. [Google Scholar] [CrossRef] [PubMed]
- Lengacher, C.A.; Reich, R.R.; Paterson, C.L.; Ramesar, S.; Park, J.Y.; Alinat, C.; Jacobsen, P.B. Examination of broad symptom improvement resulting from mindfulness-based stress reduction in breast cancer survivors: A randomized controlled trial. J. Clin. Oncol. 2016, 34, 2827. [Google Scholar] [CrossRef] [PubMed]
- Reich, R.R.; Lengacher, C.A.; Alinat, C.B.; Kip, K.E.; Paterson, C.; Ramesar, S.; Budhrani-Shani, P. Mindfulness-based stress reduction in post-treatment breast cancer patients: Immediate and sustained effects across multiple symptom clusters. J. Pain. Symptom Manag. 2017, 53, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.Y.; Zhou, Y.Q.; Feng, Z.W.; Fan, Y.N.; Zeng, G.C.; Wei, L. Randomized controlled trial of mindfulness-based stress reduction (MBSR) on posttraumatic growth of Chinese breast cancer survivors. Psychol. Health Med. 2017, 22, 94–109. [Google Scholar] [CrossRef]
- Kenne Sarenmalm, E.; Martensson, L.B.; Andersson, B.A.; Karlsson, P.; Bergh, I. Mindfulness and its efficacy for psychological and biological responses in women with breast cancer. Cancer Med. 2017, 6, 1108–1122. [Google Scholar] [CrossRef] [PubMed]
- Kissane, D.W.; Grabsch, B.; Clarke, D.M.; Smith, G.C.; Love, A.W.; Bloch, S.; Li, Y. Supportive-expressive group therapy for women with metastatic breast cancer: Survival and psychosocial outcome from a randomized controlled trial. Psycho-Oncology 2007, 16, 277–286. [Google Scholar] [CrossRef] [PubMed]
- Bower, J.E.; Crosswell, A.D.; Stanton, A.L.; Crespi, C.M.; Winston, D.; Arevalo, J.; Ganz, P.A. Mindfulness meditation for younger breast cancer survivors: A randomized controlled trial. Cancer 2015, 121, 1231–1240. [Google Scholar] [CrossRef]
- Lechner, S.C.; Whitehead, N.E.; Vargas, S.; Annane, D.W.; Robertson, B.R.; Carver, C.S.; Antoni, M.H. Does a community-based stress management intervention affect psychological adaptation among underserved black breast cancer survivors? J. Natl. Cancer Inst. 2014, 50, 315–322. [Google Scholar] [CrossRef] [Green Version]
- Dodds, S.E.; Pace, T.W.; Bell, M.L.; Fiero, M.; Negi, L.T.; Raison, C.L.; Weihs, K.L. Feasibility of Cognitively-Based Compassion Training (CBCT) for breast cancer survivors: A randomized, wait list controlled pilot study. Support Care Cancer 2015, 23, 3599–3608. [Google Scholar] [CrossRef]
- Boyle, C.C.; Stanton, A.L.; Ganz, P.A.; Crespi, C.M.; Bower, J.E. Improvements in emotion regulation following mindfulness meditation: Effects on depressive symptoms and perceived stress in younger breast cancer survivors. J. Consult. Clin. Psychol. 2017, 85, 397. [Google Scholar] [CrossRef]
- Bordeleau, L.; Szalai, J.P.; Ennis, M.; Leszcz, M.; Speca, M.; Sela, R.; Pritchard, K.I. Quality of life in a randomized trial of group psychosocial support in metastatic breast cancer: Overall effects of the intervention and an exploration of missing data. J. Clin. Oncol. 2003, 21, 1944–1951. [Google Scholar] [CrossRef] [PubMed]
- McKiernan, A.; Steggles, S.; Guerin, S.; Carr, A. A controlled trial of group cognitive behavior therapy for Irish breast cancer patients. J. Psychosoc. Oncol. 2010, 28, 143–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.; Lim, Y.; Yoo, M.S.; Kim, Y. Effects of a nurse-led cognitive-behavior therapy on fatigue and quality of life of patients with breast cancer undergoing radiotherapy: An exploratory study. Cancer Nurs. 2011, 34, E22–E30. [Google Scholar] [CrossRef] [PubMed]
- Björneklett, H.G.; Lindemalm, C.; Rosenblad, A.; Ojutkangas, M.L.; Letocha, H.; Strang, P.; Bergkvist, L. A randomised controlled trial of support group intervention after breast cancer treatment: Results on anxiety and depression. Acta Oncol. 2012, 51, 198–207. [Google Scholar] [CrossRef] [Green Version]
- Gudenkauf, L.M.; Antoni, M.H.; Stagl, J.M.; Lechner, S.C.; Jutagir, D.R.; Bouchard, L.C.; Avisar, E. Brief cognitive–behavioral and relaxation training interventions for breast cancer: A randomized controlled trial. J. Consult. Clin. Psychol. 2015, 83, 677. [Google Scholar] [CrossRef]
- Cohen, M.; Fried, G. Comparing relaxation training and cognitive-behavioral group therapy for women with breast cancer. Res. Soc. Work Pract. 2007, 17, 313–323. [Google Scholar] [CrossRef]
- Spielberger, C.D. State-Trait anxiety inventory. In The Corsini Encyclopedia of Psychology; John Wiley & Son’s, Inc.: Hoboken, NJ, USA, 2010; p. 1. [Google Scholar]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Morey, L.C. Personality Assessment Inventory: Professional Manual; Psychological Assessment Resources: Tampa, FL, USA, 1991. [Google Scholar]
- Beck, A.T.; Ward, C.; Mendelson, M.; Mock, J.; Erbaugh, J. Beck depression inventory (BDI). Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [Green Version]
- Roberts, R.E.; Vernon, S.W. The Center for Epidemiological Studies Depression Scale: Its use in a community sample. Am. J. Psychiatry 1983, 140, 41–46. [Google Scholar]
- Cella, D.F.; Tulsky, D.S.; Gray, G.; Sarafian, B.; Linn, E.; Bonomi, A.; Eckberg, K. The Functional Assessment of Cancer Therapy scale: Development and validation of the general measure. J. Clin. Oncol. 1993, 11, 570–579. [Google Scholar] [CrossRef]
- Moriwaki, S.Y. The Affect Balance Scale: A validity study with aged samples. J. Gerontol. 1974, 29, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Derogatis, L.R.; Melisaratos, N. The brief symptom inventory: An introductory report. Psych. Med. 1983, 13, 595–605. [Google Scholar] [CrossRef] [Green Version]
- Shacham, S. A shortened version of the Profile of Mood States. J. Pers. 1983, 47, 305–306. [Google Scholar] [CrossRef] [PubMed]
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Kaasa, S. The European Organization for Research and Treatment of Cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. JNCI 1993, 85, 365–376. [Google Scholar] [CrossRef]
- Stewart, A.L.; Hays, R.D.; Ware, J.E. The MOS short-form general health survey. Reliability and validity in a patient population. Med. Care 1998, 26, 724–735. [Google Scholar] [CrossRef]
- Shim, E.J.; Mehnert, A.; Koyama, A.; Cho, S.J.; Inui, H.; Paik, N.S.; Koch, U. Health-related quality of life in breast cancer: A cross-cultural survey of German, Japanese, and South Korean patients. Breast Cancer Res. Treat. 2006, 99, 341–350. [Google Scholar] [CrossRef]
- Sheard, T.; Maguire, P. The effect of psychological interventions on anxiety and depression in cancer patients: Results of two meta-analyses. Br. J. Cancer 1999, 80, 1770. [Google Scholar] [CrossRef] [Green Version]
- Devine, E.C.; Westlake, S.K. The effects of psychoeducational care provided to adults with cancer: Meta-analysis of 116 studies. Oncol. Nurs. Forum 1995, 22, 1369–1382. [Google Scholar]
- Kaczkurkin, A.N.; Foa, E.B. Cognitive-behavioral therapy for anxiety disorders: An update on the empirical evidence. Dialogues Clin. Neurosci. 2015, 17, 337. [Google Scholar]
- Johnson, J.A.; Rash, J.A.; Campbell, T.S.; Savard, J.; Gehrman, P.R.; Perlis, M.; Garland, S.N. A systematic review and meta-analysis of randomized controlled trials of cognitive behavior therapy for insomnia (CBT-I) in cancer survivors. Sleep. Med. Rev. 2016, 27, 20–28. [Google Scholar] [CrossRef]
- Shannonhouse, L.; Myers, J.; Barden, S.; Clarke, P.; Weimann, R.; Forti, A.; Porter, M. Finding your new normal: Outcomes of a wellness-oriented psychoeducational support group for cancer survivors. JSGW 2014, 39, 3–28. [Google Scholar] [CrossRef]
- Jafari, A.; Goudarzian, A.H.; Nesami, M.B. Depression in women with breast cancer: A systematic review of cross-sectional studies in Iran. APJCP 2018, 19, 1. [Google Scholar] [PubMed]
- Driessen, E.; Hollon, S.D. Cognitive behavioral therapy for mood disorders: Efficacy, moderators and mediators. Psychiatr. Clin. 2010, 33, 537–555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohr, D.C.; Boudewyn, A.C.; Goodkin, D.E.; Bostrom, A.; Epstein, L. Comparative outcomes for individual cognitive-behavior therapy, supportive-expressive group psychotherapy, and sertraline for the treatment of depression in multiple sclerosis. J. Consult. Clin. Psychol. 2001, 69, 942. [Google Scholar] [CrossRef]
- Boutin, D.L. Effectiveness of cognitive behavioral and supportive-expressive group therapy for women diagnosed with breast cancer: A review of the literature. JSGW 2007, 32, 267–284. [Google Scholar] [CrossRef]
- Ohlsson-Nevo, E.; Andershed, B.; Nilsson, U. Psycho-educational intervention on mood in patients suffering from colorectal and anal cancer: A randomized controlled trial. Nord. J. Nurs. Res. 2017, 37, 135–142. [Google Scholar] [CrossRef]
- McNair, D.M.; Lorr, M.; Droppleman, L.F. Manual for the Profile of Mood States; Educational Industrial Testing Service: San Diego, CA, USA, 1971. [Google Scholar]
- Bellver-Pérez, A.; Peris-Juan, C.; Santaballa-Beltrán, A. Effectiveness of therapy group in women with localized breast cancer. Int. J. Clin. Health Psychol. 2019, 19, 107–114. [Google Scholar] [CrossRef]
- Fawzy, F.I.; Fawzy, N.W.; Wheeler, J.G. A post-hoc comparison of the efficiency of a psychoeducational intervention for melanoma patients delivered in group versus individual formats: An analysis of data from two studies. Psycho-Oncology 1996, 5, 81–89. [Google Scholar] [CrossRef]
- Stark, D.P.H.; House, A. Anxiety in cancer patients. Br. J. Cancer 2000, 83, 1261. [Google Scholar] [CrossRef]
- Trask, P.C. Assessment of depression in cancer patients. JNCI Monogr. 2004, 2004, 80–92. [Google Scholar] [CrossRef] [Green Version]
- Hofmann, S.G.; Asnaani, A.; Vonk, I.J.; Sawyer, A.T.; Fang, A. The efficacy of cognitive behavioral therapy: A review of meta-analyses. Cognit. Ther. Res. 2012, 36, 427–440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haller, H.; Winkler, M.M.; Klose, P.; Dobos, G.; Kuemmel, S.; Cramer, H. Mindfulness-based interventions for women with breast cancer: An updated systematic review and meta-analysis. Acta Oncol. 2017, 56, 1665–1676. [Google Scholar] [CrossRef] [PubMed]
- Park, E.S.; Kim, S.J.; Kim, S.I.; Chun, Y.J.; Lee, P.S.; Kim, H.J.; Han, K.S. A study of factors influencing health promoting behavior and quality of life in the elderly. J. Korean Acad. Nurs. 1998, 28, 638–649. [Google Scholar] [CrossRef]
- Rosen, K.D.; Paniagua, S.M.; Kazanis, W.; Jones, S.; Potter, J.S. Quality of life among women diagnosed with breast Cancer: A randomized waitlist controlled trial of commercially available mobile app-delivered mindfulness training. Psycho-Oncology 2018, 27, 2023–2030. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Hernandez, E.; Romero, R.; Campos, D.; Burychka, D.; Diego-Pedro, R.; Baños, R.; Cebolla, A. Cognitively-Based Compassion Training (CBCT®) in Breast Cancer Survivors: A Randomized Clinical Trial Study. Integr. Cancer Ther. 2018, 17, 684–696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grégoire, C.; Nicolas, H.; Bragard, I.; Delevallez, F.; Merckaert, I.; Razavi, D.; Vanhaudenhuyse, A. Efficacy of a hypnosis-based intervention to improve well-being during cancer: A comparison between prostate and breast cancer patients. BMC Cancer 2018, 18, 677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mendoza, M.E.; Capafons, A.; Jensen, M.P. Hypnosis attitudes: Treatment effects and associations with symptoms in individuals with cancer. Am. J. Clin. Hypn. 2017, 60, 50–67. [Google Scholar] [CrossRef] [PubMed]
- Téllez, A.; Rodríguez-Padilla, C.; Martínez-Rodríguez, J.L.; Juárez-García, D.M.; Sanchez-Armass, O.; Sánchez, T.; Jaime-Bernal, L. Psychological effects of group hypnotherapy on breast cancer patients during chemotherapy. Am. J. Clin. Hypn. 2017, 60, 68–84. [Google Scholar] [CrossRef]
- Beutel, M.E.; Fischbeck, S.; Binder, H.; Blettner, M.; Brähler, E.; Emrich, K.; Zeissig, S.R. Depression, anxiety and quality of life in long-term survivors of malignant melanoma: A register-based cohort study. PLoS ONE 2015, 10, e0116440. [Google Scholar] [CrossRef]
- Maxwell-Smith, C.; Zeps, N.; Hagger, M.S.; Platell, C.; Hardcastle, S.J. Barriers to physical activity participation in colorectal cancer survivors at high risk of cardiovascular disease. Psycho-Oncology 2017, 26, 808–814. [Google Scholar] [CrossRef]
- Beatty, L.; Kemp, E.; Butow, P.; Girgis, A.; Schofield, P.; Turner, J.; Koczwara, B. A systematic review of psychotherapeutic interventions for women with metastatic breast cancer: Context matters. Psycho-Oncology 2018, 27, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Ehring, T.; Watkins, E.R. Repetitive negative thinking as a transdiagnostic process. Int. J. Cogn. Ther. 2008, 1, 192–205. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Tools | Study | n (Treatment/Control) | Intervention Type | Intervention Duration | Control Condition | Inclusion Criteria | Provider | Stage of Cancer |
|---|---|---|---|---|---|---|---|---|---|
| Anxiety | HADS | Kissane et al. [24] | 145/141 | CBT + Relaxation Lessons | 20 weeks | Relaxation Lessons | Inpatient Treatment | Two Therapists | I; II |
| STAI | Dolbeault et al. [32] | 85/93 | PET | 8 weeks | Wait List | After Treatment | Two Therapists | I; II; III | |
| HADS | Groarke et al. [50] | 102/120 | CB-CBSM | 5 weeks | Usual Care | After Treatment | Clinical Psychologist | From 0 to IV | |
| HADS | Ho et al. [30] | 47/51 | SET | 8 weeks | Social Support | After Treatment | Therapist | I; II; III | |
| PAI | Jang et al. [51] | 12/11 | CBT-MBSR | 12 weeks | Wait List | After Treatment | Mental Health Specialist | From 0 to III | |
| HADS | Johannsen et al. [52] | 46/61 | CBT-MBSR | 8 weeks | Wait List | After Treatment | Mindfulness Instructor | Not Reported | |
| STAI | Lengacher et al. [53] | 152/147 | CBT-MBSR | 6 weeks | Usual Care | After Treatment | Clinical Psychologist | From 0 to III | |
| STAI | Reich et al. [54] | 159/152 | CBT-MBSR | 6 weeks | Usual Care | After Treatment | Clinical Psychologist | From 0 to III | |
| STAI | Zhang et al. [55] | 28/30 | CBT-MBSR | 8 weeks | Usual Care | After Treatment | Psychologist, Expert in Mindfulness | I; II; III | |
| HADS | Kenne Sarenmalm et al. [56] | 62/52 | CBT-MBSR | 8 weeks | Non-MBSR | After Treatment | Mindfulness Instructor | Not Reported | |
| Depression | HADS | Kissane et al. [24] | 145/141 | CBT + Relaxation Lessons | 20 weeks | Relaxation Lessons | Inpatient Treatment | Two Therapists | I; II |
| BDI | Kissane et al. [57] | 115/56 | SET | 13 weeks | Relaxation Lessons | After Treatment | Therapist | IV | |
| HADS | Groarke et al. [50] | 102/120 | CBT-CBSM | 5 weeks | Usual Care | After Treatment | Clinical Psychologist | From 0 to IV | |
| CES-D | Bower et al. [58] | 32/33 | CBT-MAP | 6 weeks | Wait List | After Treatment | Not Reported | From 0 to III | |
| FACT | Lechner et al. [59] | 57/57 | CBT-CBSM | 10 weeks | Educational Program | After Treatment | Clinical Psychologist | From 0 to IV | |
| CES-D | Dodds et al. [60] | 16/12 | CBT-CDCT | 16 weeks | Wait List | After Treatment | Clinically Trained PhD and Social Work Researcher | Not Reported | |
| HADS | Ho et al. [30] | 47/51 | SET | 8 weeks | Social Support | After Treatment | Therapist | I; II; III | |
| PAI | Jang et al. [51] | 12/11 | CBT-MBSR | 12 weeks | Wait List | After Treatment | Mental Health Specialist | From 0 to III | |
| CES-D | Lengacher et al. [53] | 152/147 | CBT-MBSR | 6 weeks | Usual Care | After Treatment | Clinical Psychologist | From 0 to III | |
| CES-D | Reich et al. [54] | 154/146 | CBT-MBSR | 6 weeks | Usual Care | After Treatment | Clinical Psychologist | From 0 to III | |
| CES-D | Boyle et al. [61] | 35/30 | CBT-MAP | 6 weeks | Wait List | After Treatment | Not Reported | From 0 to III | |
| HADS | Kenne Sarenmalm et al. [56] | 62/52 | CBT-MBSR | 8 weeks | Non-MBSR | After Treatment | Mindfulness Instructor | Not Reported | |
| Quality of Life | EORTC-C30 | Bordeleau et al. [62] | 145/70 | SET + Educational Training | 12 weeks | Educational and Relaxation Training | After Treatment | Psychiatrist, Psychologist, Social Workers, Nurse | IV |
| EORTC-C30 | Chujo et al. [33] | 22/11 | PET | 6 weeks | Wait List | After Treatment | Psychiatrist and Nurse | Not Reported | |
| ABS | Antoni et al. [25] | 74/85 | CBT | 10 weeks | Educational Program | After Treatment | Psychologist | From 0 to III | |
| SF-12 | Fillion et al. [34] | 44/43 | PET | 4 weeks | General Information | After Treatment | Nurses | From 0 to III | |
| EORTC-C30 | Dolbeault et al. [32] | 81/87 | PET | 8 weeks | Wait List | After Treatment | Two Therapists | I; II; III | |
| EORTC-C30 | McKiernan et al. [63] | 23/30 | CBT + Educational Training | 6 weeks | Educational Training | After Treatment | Clinical Psychologist and Counselling Psychologist | I; II; Metastasis and Lymph | |
| QoL Scales for Korean Cancer Patients | Lee et al. [64] | 35/36 | CBT | 6 weeks | Not Reported | After Treatment | Nurse | I; II; III | |
| EORTC-C30 | Bjorneklett et al. [65] | 176/164 | PET | 1 week + 4 meetings after 2 months | Wait List | After Treatment | Not Reported | I; II; III | |
| FACT | Gudenkauf et al. [66] | 40/49 | CBT + Relaxation Training | 5 weeks | Relaxation Training | After Treatment | Clinical Psychology student | From 0 to III | |
| EORTC-C30 | Jang et al. [51] | 12/11 | CBT-MBSR | 12 weeks | Wait List | After Treatment | Mental Health Specialist | From 0 to III | |
| WHO-5 | Johannsen et al. [52] | 46/61 | CBT-MBSR | 8 weeks | Wait List | After Treatment | Mindfulness Instructor | Not Reported | |
| SF-36 | Lengacher et al. [53] | 152/147 | CBT-MBSR | 6 weeks | Usual Care | After Treatment | Clinical Psychologist | From 0 to III | |
| SF-36 | Reich et al. [54] | 152/145 | CBT-MBSR | 6 weeks | Usual Care | After Treatment | Clinical Psychologist | From 0 to III | |
| Mood | ABS | Kissane et al. [24] | 145/141 | CBT + Relaxation Training | 20 weeks | Relaxation Training | Inpatient Treatment | Two Therapists | I; II |
| POMS | Chujo et al. [33] | 22/11 | PET | 6 weeks | Wait List | After Treatment | Psychiatrist and Nurse | Not Reported | |
| BSI | Cohen and Fried [67] | 38/37 | CBT + Relaxation Training | 9 weeks | Usual Care | After Treatment | Cohen (Expert in Psycho-Oncology) | I; II | |
| IES | Kissane et al. [57] | 115/56 | SET | 13 weeks | Relaxation Training | After Treatment | Therapist | IV | |
| POMS | Classen et al. [27] | 151/148 | SET | 12 weeks | Educational Program | After Treatment | Nurse, Psychologist, Social Workers | From 0 to III | |
| POMS | Fillion et al. [34] | 44/43 | PET | 4 weeks | General Information | After Treatment | Nurses | From 0 to III | |
| POMS | Dolbeault et al. [32] | 81/87 | PET | 8 weeks | Wait List | After Treatment | Two Therapists | I; II; III | |
| POMS | McKiernan et al. [63] | 23/30 | CBT + Educational Training | 6 weeks | Educational Training | After Treatment | Clinical Psychologist and Counselling Psychologist | I; II; Metastasis and Lymph | |
| POMS | Lechner et al. [59] | 57/57 | CBT-CBSM | 10 weeks | Educational Program | After Treatment | Clinical Psychologist | From 0 to IV | |
| ABS | Gudenkauf et al. [66] | 40/49 | CBT + Relaxation Training | 5 weeks | Relaxation Training | After Treatment | Clinical Psychology student | From 0 to III |
| Study | Intervention Type | Random Sequence Generation | Allocation Concealment | Blinding (Outcome Assessment) | Incomplete Outcome | Selective Reporting | Other Sources of Bias | Overall Risk of Bias |
|---|---|---|---|---|---|---|---|---|
| Bordeleau et al. [62] | SET | + | ? | ? | ? | + | ? | ? |
| Kissane et al. [24] | CBT | + | + | + | ? | ? | ? | ? |
| Chujo et al. [33] | PET | − | − | ? | − | + | ? | − |
| Antoni et al. [23] | CBT | ? | ? | + | + | ? | ? | ? |
| Cohen and Fried [67] | CBT | ? | ? | + | + | + | ? | ? |
| Kissane et al. [57] | SET | + | ? | − | ? | ? | ? | − |
| Classen et al. [27] | SET | + | ? | ? | ? | − | ? | − |
| Fillion et al. [34] | PET | ? | ? | ? | + | + | ? | ? |
| Dolbeault et al. [32] | PET | + | + | ? | ? | + | ? | ? |
| McKiernan et al. [63] | CBT | − | − | ? | ? | ? | ? | − |
| Lee et al. [64] | CBT | − | − | − | ? | ? | ? | − |
| Björneklett et al. [65] | PET | + | + | + | ? | + | ? | ? |
| Groarke et al. [50] | CBT | + | + | ? | + | + | ? | ? |
| Bower et al. [58] | CBT | ? | ? | ? | + | + | ? | ? |
| Lechner et al. [59] | CBT | ? | ? | ? | + | + | ? | ? |
| Dodds et al. [60] | CBT | + | ? | ? | ? | + | ? | ? |
| Gudenkauf et al. [66] | CBT | + | + | + | ? | + | ? | ? |
| Ho et al. [30] | SET | + | ? | ? | + | + | ? | ? |
| Jang et al. [51] | CBT | ? | ? | ? | + | + | ? | ? |
| Johannsen et al. [52] | CBT | + | ? | ? | + | + | ? | ? |
| Langacher et al. [53] | CBT | + | ? | ? | + | + | ? | ? |
| Reich et al. [54] | CBT | ? | ? | − | + | ? | ? | − |
| Zhang et al. [55] | CBT | ? | − | ? | + | + | ? | − |
| Boyle et al. [61] | CBT | − | ? | ? | + | ? | ? | − |
| Kenne Sarenmalm et al. [56] | CBT | + | + | ? | + | + | ? | ? |
| Analyses | Number of Studies | Effect Size (95% CI) | Heterogeneity (I2%) |
|---|---|---|---|
| Anxiety | |||
| Overall Effect Size | 10 | −0.39 [−0.91, 0.14] | 98 |
| Type of Intervention | - | ||
| Cognitive Behavioural Therapy | 8 | −0.45 [−1.14, 0.24] | 97 |
| Psycho-Educational Therapy | 1 | −0.45 [−0.49, −0.40] | - |
| Supportive-Expressive Therapy | 1 | 0.10 [0.02, 0.18] | |
| Type of Provider | |||
| Psychologist | 6 | −0.14 [−0.31, 0.02] | 95 |
| Psychologist + Psychiatrist | 1 | −0.45 [−0.49, −0.40] | - |
| Nurse | - | - | - |
| Other | 3 | −0.94 [−4.47, 2.58] | 98 |
| Not Reported | |||
| Duration of Intervention | |||
| Less than 6 Weeks | 1 | −0.19 [−0.22, −0.15] | - |
| Between 6 and 12 Weeks | 8 | −0.45 [−1.15, 0.26] | 98 |
| More than 12 Weeks | - | - | - |
| Not Reported | 1 | −0.20 [−0.23, −0.18] | - |
| Control Group | |||
| Alternative Intervention | 3 | 0.003 [−0.46, 0.47] | 98 |
| Wait List | 3 | −1.12 [−4.16, 1.90] | 93 |
| Standard Care | 4 | −0.18 [−0.40, 0.04] | 93 |
| Not Reported | |||
| Inclusion Criteria | |||
| In Patient | 1 | −0.21 [−0.24, −0.18] | |
| After Treatment | 9 | −0.41 [−1.01, 0.19] | 98 |
| Not Reported | - | - | - |
| Depression | |||
| Overall Effect Size | 12 | −0.35 [−0.79, −0.10] | 98 |
| Type of Intervention | |||
| Cognitive Behavioural Therapy | 10 | −0.42 [−0.96, 0.12] | 98 |
| Psycho-Educational Therapy | - | - | - |
| Supportive-Expressive Therapy | 2 | −0.10 [−2.18, 2.16] | 98 |
| Type of Provider | |||
| Psychologist | 7 | −0.15 [−0.37, 0.06] | 97 |
| Psychologist + Psychiatrist | - | - | - |
| Nurse | - | - | - |
| Other | 3 | −1.04 [−3.85, 1.76] | 97 |
| Not Reported | 2 | −0.08 [−9.44, 9.26] | 99 |
| Duration of Intervention | |||
| Less than 6 Weeks | 1 | −0.08 [−0.11, −0.04] | - |
| Between 6 and 12 Weeks | 8 | −0.40 [−1.12, 0.33] | 98 |
| More than 12 Weeks | 1 | −0.18 [−0.21, −0.14] | - |
| Not Reported | 2 | −0.39 [−4.31, 3.51] | 93 |
| Control Group | |||
| Alternative Intervention | 5 | −0.18 [−0.53, 0.17] | 98 |
| Wait List | 4 | −0.79 [−2.72, 1.14] | 99 |
| Standard Care | 3 | −0.11 [−0.16, −0.05] | 50 |
| Not Reported | - | - | - |
| Inclusion Criteria | |||
| In Patient | 1 | −0.10 [−0.13, −0.08] | |
| After Treatment | 11 | −0.37 [−0.86, 0.12] | 98 |
| Not Reported | - | - | - |
| Mood | |||
| Overall Effect Size | 10 | −0.17 [−0.41, 0.06] | 98 |
| Type of Intervention | |||
| Cognitive Behavioural Therapy | 5 | −0.12 [−0.64, 0.39] | 98 |
| Psycho-Educational Therapy | 3 | −0.34 [−1.05, 0.36] | 97 |
| Supportive-Expressive Therapy | 2 | −0.07 [−1.70, 1.56] | 99 |
| Type of Provider | |||
| Psychologist | 6 | −0.12 [−0.51, 0.25] | 99 |
| Psychologist + Psychiatrist | - | - | - |
| Nurse | 1 | −0.02 [−0.11, 0.06] | - |
| Other | 3 | −0.33 [−1.19, 0.54] | 98 |
| Not Reported | |||
| Duration of Intervention | |||
| Less than 6 weeks | 2 | 0.001 [−0.36, 0.37] | 0 |
| Between 6 and 12 Weeks | 5 | −0.31 [−0.87, 0.24] | 96 |
| More than 12 Weeks | 2 | −0.07 [−1.70, 1.56] | 99 |
| Not Reported | 1 | .0.08 [−0.10, −0.05] | 99 |
| Control Group | |||
| Alternative Intervention | 6 | −0.03 [−0.35, 0.29] | 98 |
| Wait List | 3 | −0.34 [−1.06, 0.36] | 96 |
| Standard Care | 1 | −0.57 [−0.68, −0.46] | - |
| Not Reported | |||
| Inclusion Criteria | |||
| In Patient | 1 | −0.08 [−0.10, 0.05] | - |
| After Treatment | 9 | −0.18 [−0.46, 0.08] | 98 |
| Not Reported | - | - | - |
| Quality of Life | |||
| Overall Effect Size | 13 | 0.38 [−0.07, 0.84] | 98 |
| Type of Intervention | |||
| Cognitive Behavioural Therapy | 8 | 0.55 [−0.25, 1.35] | 99 |
| Psycho-Educational Therapy | 4 | 0.17 [0.02, 0.32] | 89 |
| Supportive-Expressive Therapy | 1 | −0.11 [−0.15, −0.07] | - |
| Type of Provider | |||
| Psychologist | 6 | 0.08 [−0.18, 0.34] | 93 |
| Psychologist + Psychiatrist | 2 | −0.03 [−1.17, 1.12] | 96 |
| Nurse | 3 | 0.72 [−1.18, 2.63] | 99 |
| Other | 1 | 2.56 [1.93, 3.18] | - |
| Not Reported | 1 | 0.20 [0.17, 0.22] | - |
| Duration of Intervention | |||
| Less than 6 Weeks | 2 | 0.11 [−1.34, 1.57] | 97 |
| Between 6 and 12 Weeks | 10 | 0.46 [−0.15, 1.08] | 90 |
| More than 12 Weeks | - | - | - |
| Not Reported | 1 | 0.20 [0.17, 0.22] | - |
| Control Group | |||
| Alternative Intervention | 6 | 0.27 [−0.41, 0.96] | 98 |
| Wait List | 5 | 0.71 [−0.53, 1.96] | 97 |
| Standard Care | 2 | −0.03 [−0.18, 0.12] | 36 |
| Not Reported | - | - | - |
| Inclusion Criteria | |||
| In Patient | - | - | - |
| After treatment | 13 | 0.38 [−0.07, 0.84] | 98 |
| Not Reported | - | - | - |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guarino, A.; Polini, C.; Forte, G.; Favieri, F.; Boncompagni, I.; Casagrande, M. The Effectiveness of Psychological Treatments in Women with Breast Cancer: A Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 209. https://doi.org/10.3390/jcm9010209
Guarino A, Polini C, Forte G, Favieri F, Boncompagni I, Casagrande M. The Effectiveness of Psychological Treatments in Women with Breast Cancer: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2020; 9(1):209. https://doi.org/10.3390/jcm9010209
Chicago/Turabian StyleGuarino, Angela, Cristina Polini, Giuseppe Forte, Francesca Favieri, Ilaria Boncompagni, and Maria Casagrande. 2020. "The Effectiveness of Psychological Treatments in Women with Breast Cancer: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 9, no. 1: 209. https://doi.org/10.3390/jcm9010209