A Systematic Review and Meta-Analysis of the Impact of Mindfulness Based Interventions on Heart Rate Variability and Inflammatory Markers


Abstract
:1. Introduction
2. Methods
2.1. Eligibility Criteria
2.2. Search Strategy
2.3. Study Selection and Data Extraction
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
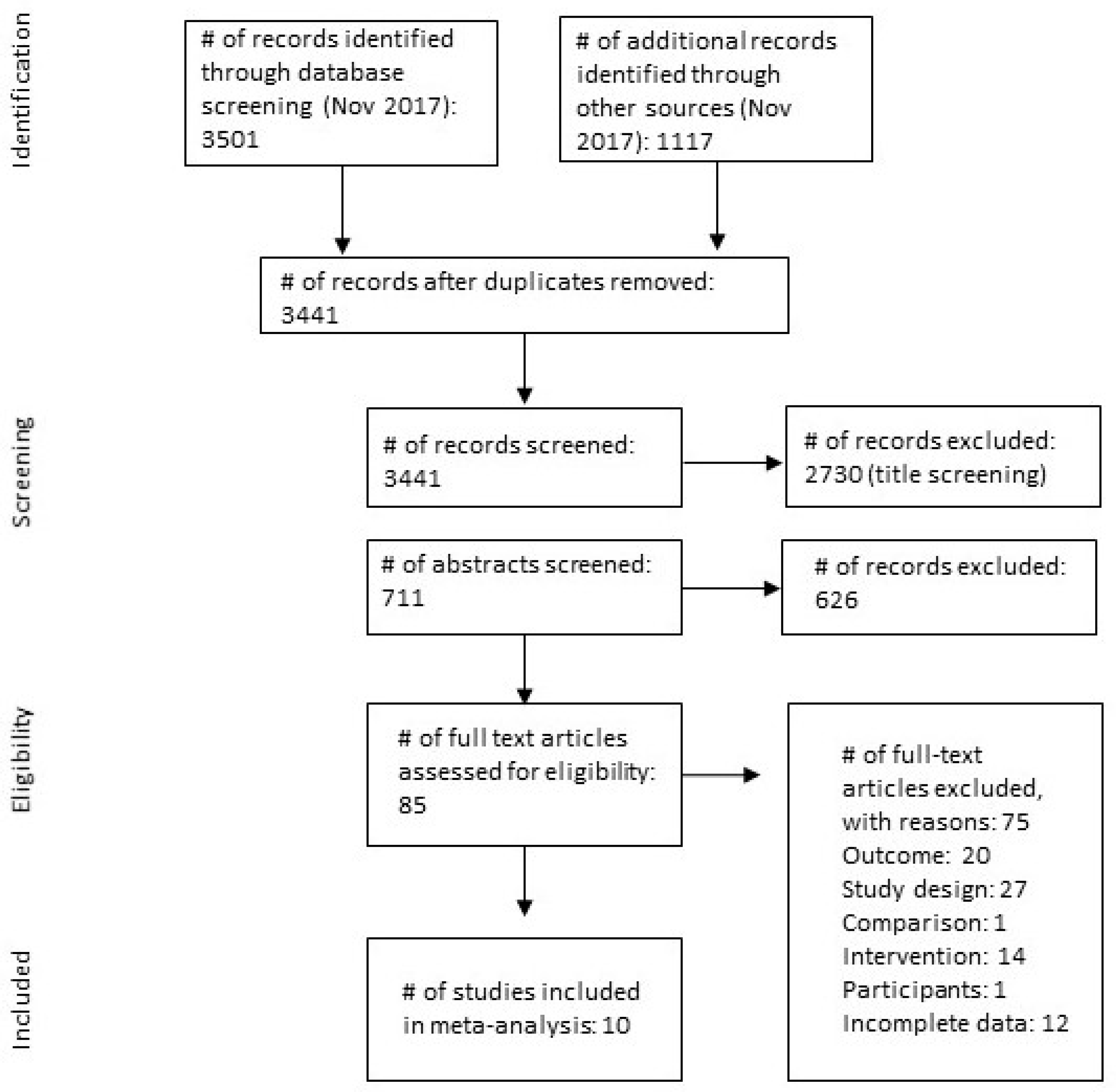
3.1. Search Results
3.2. Characteristics of Included Studies
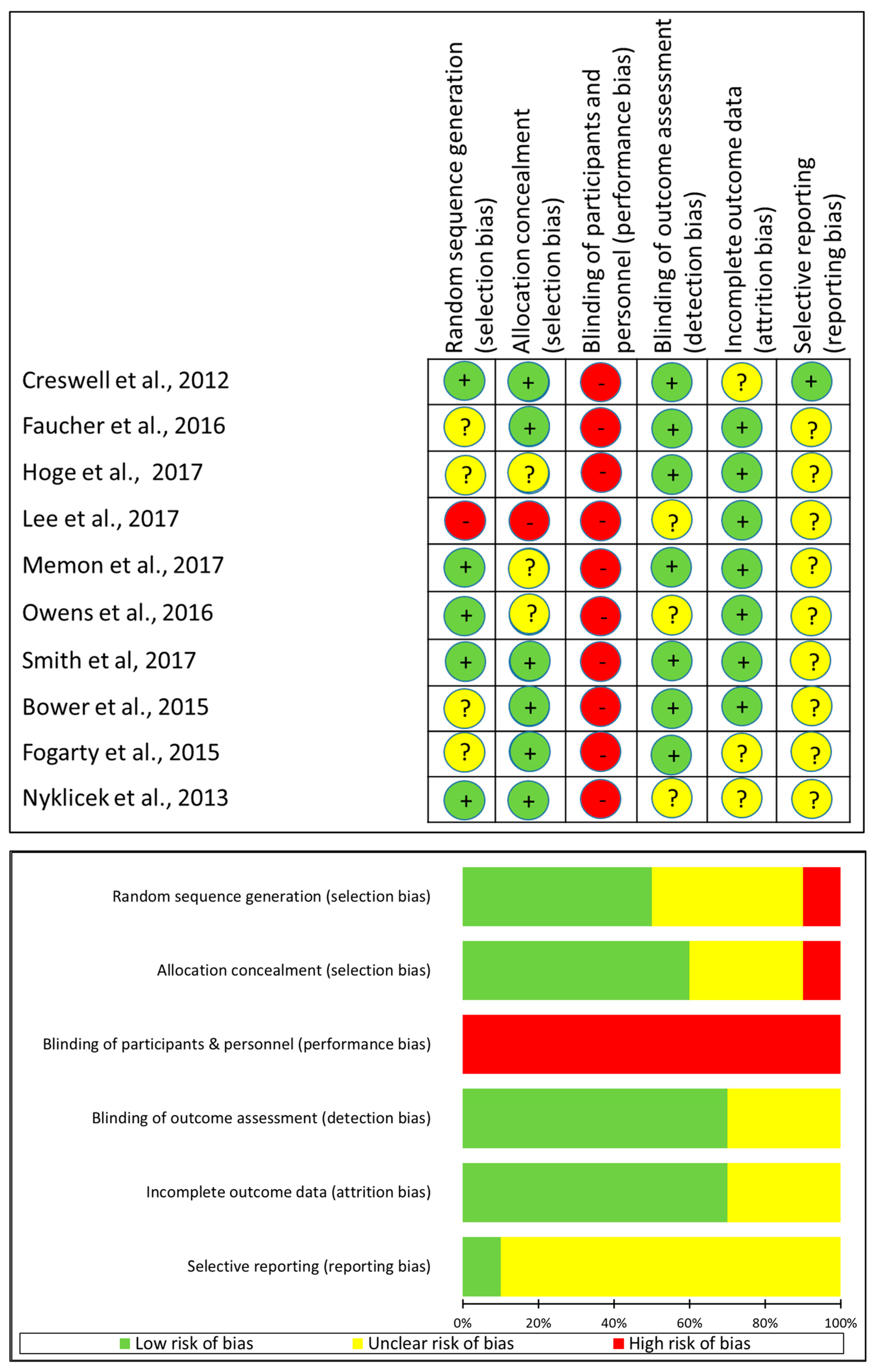
3.3. Assessment of Study Quality
3.4. Meta-Analysis of Inflammatory Markers
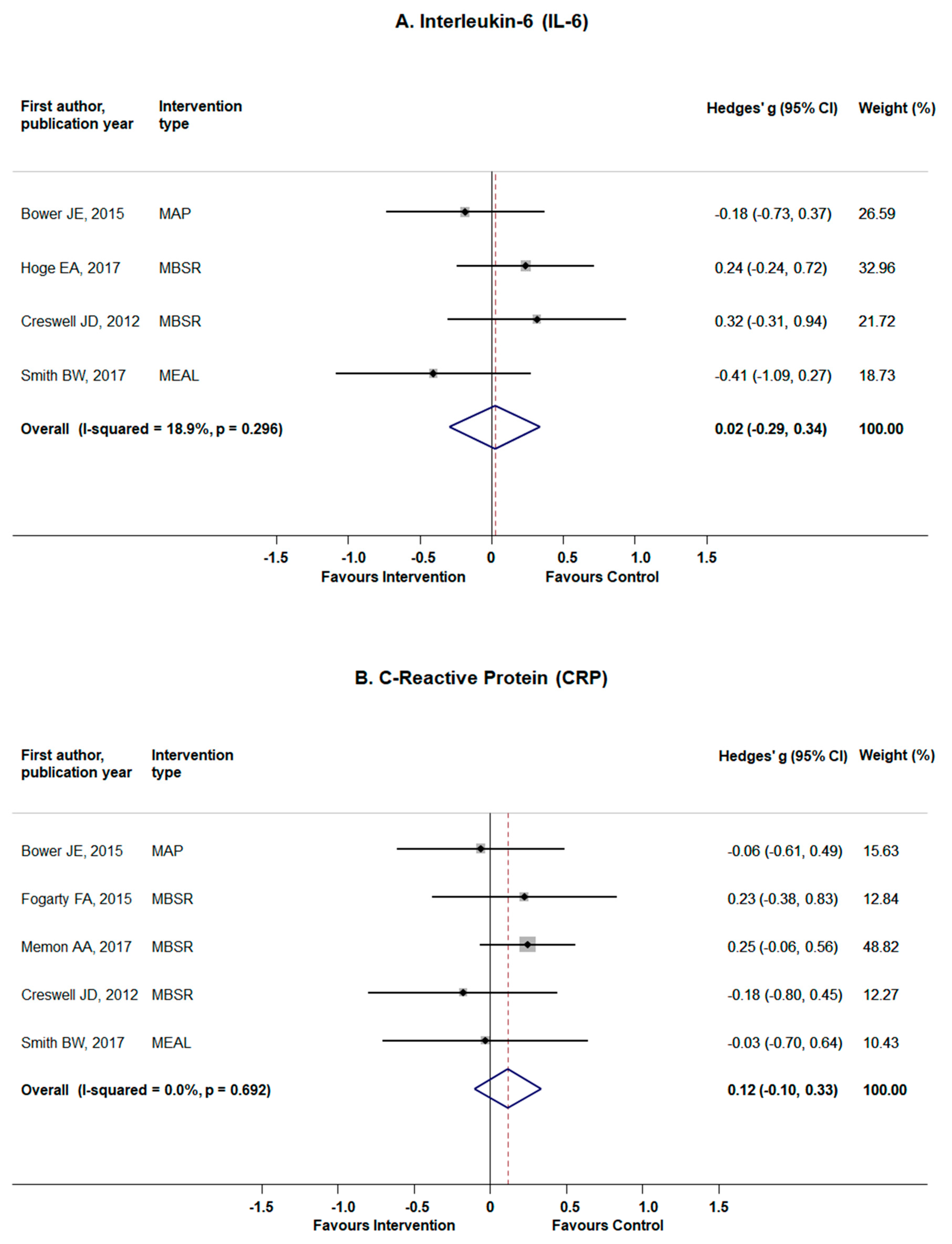
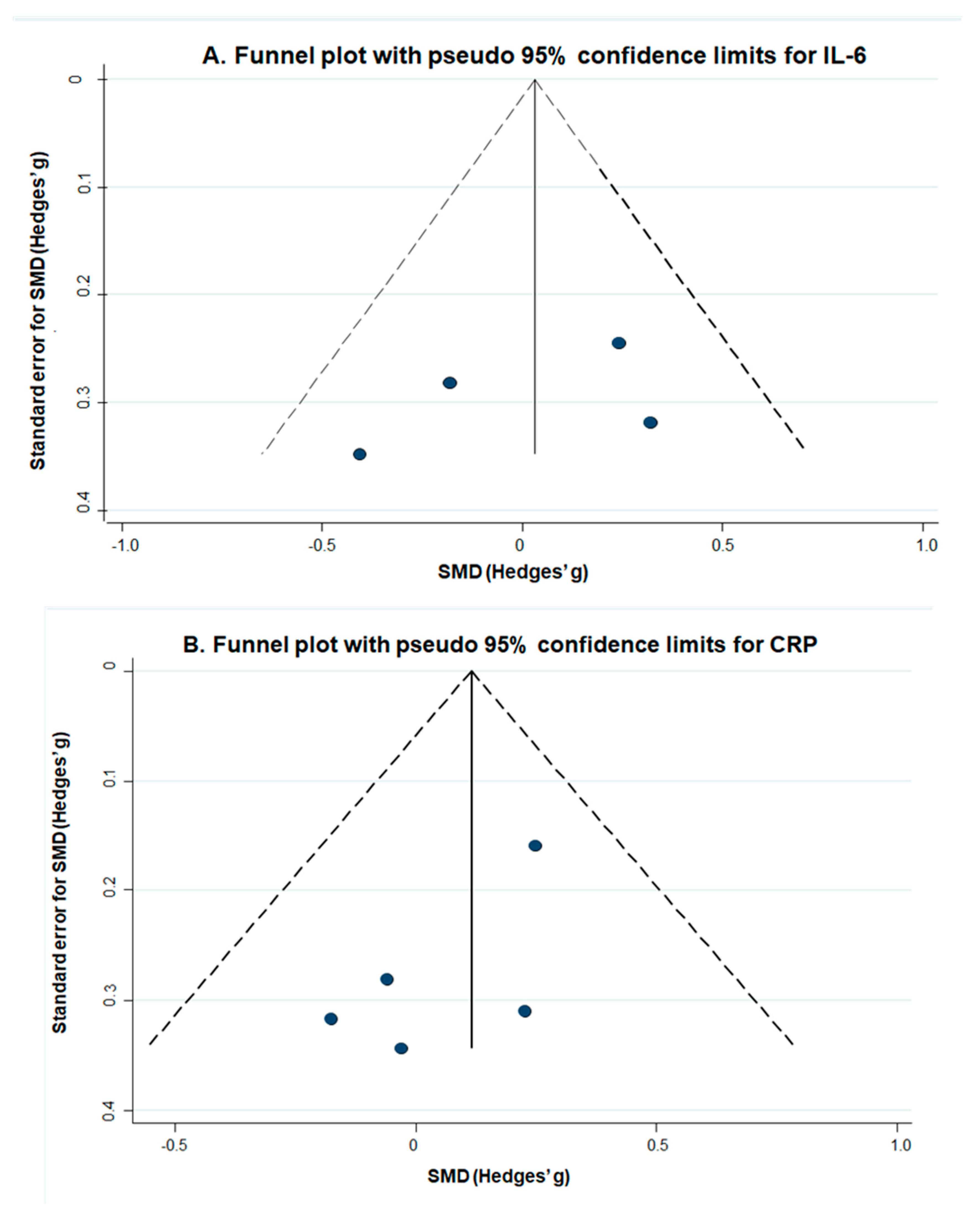
3.4.1. Interleukin-6
3.4.2. C-Reactive Protein
3.5. Meta-Analysis of Heart Rate Variability Measures
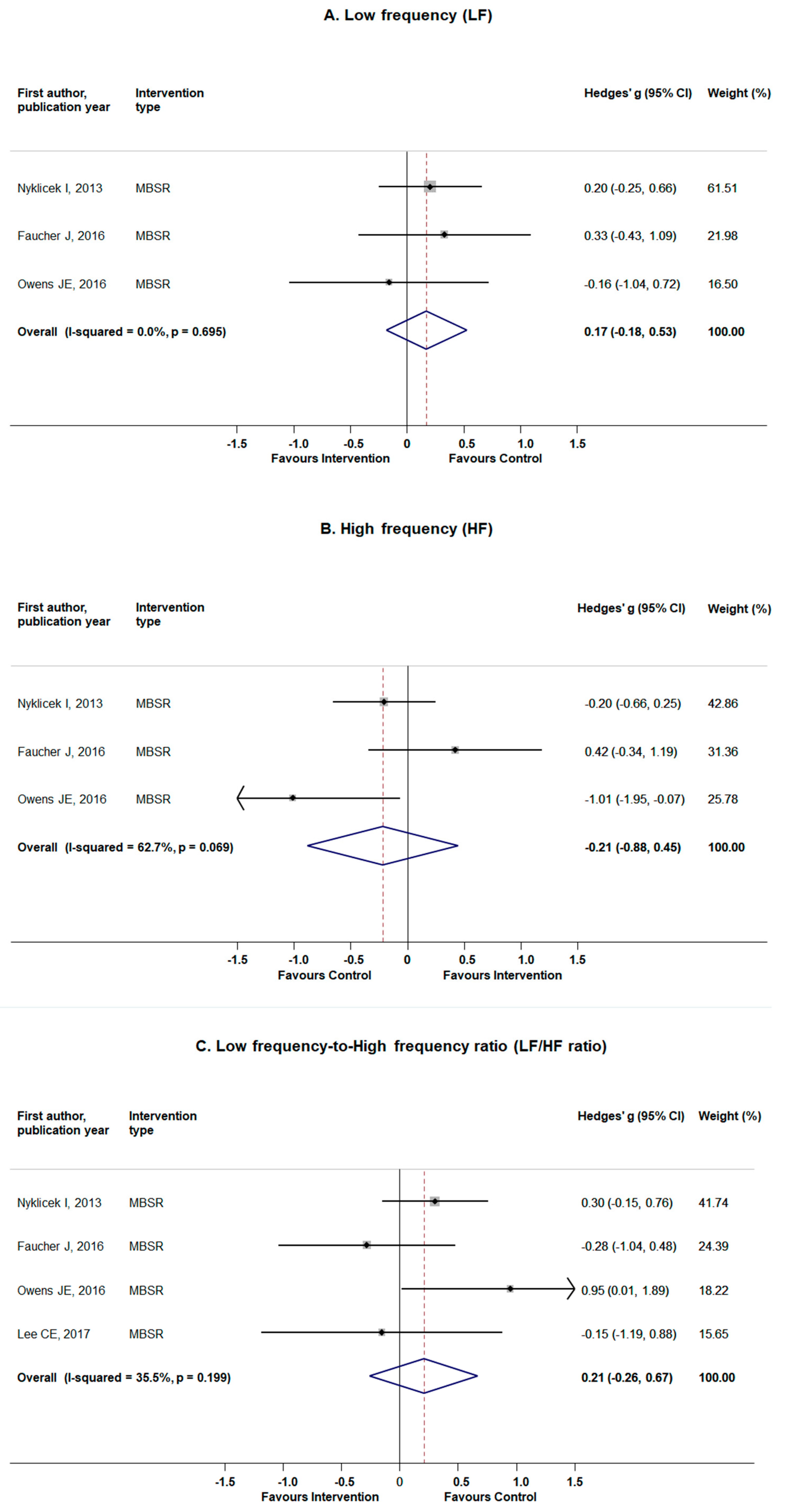
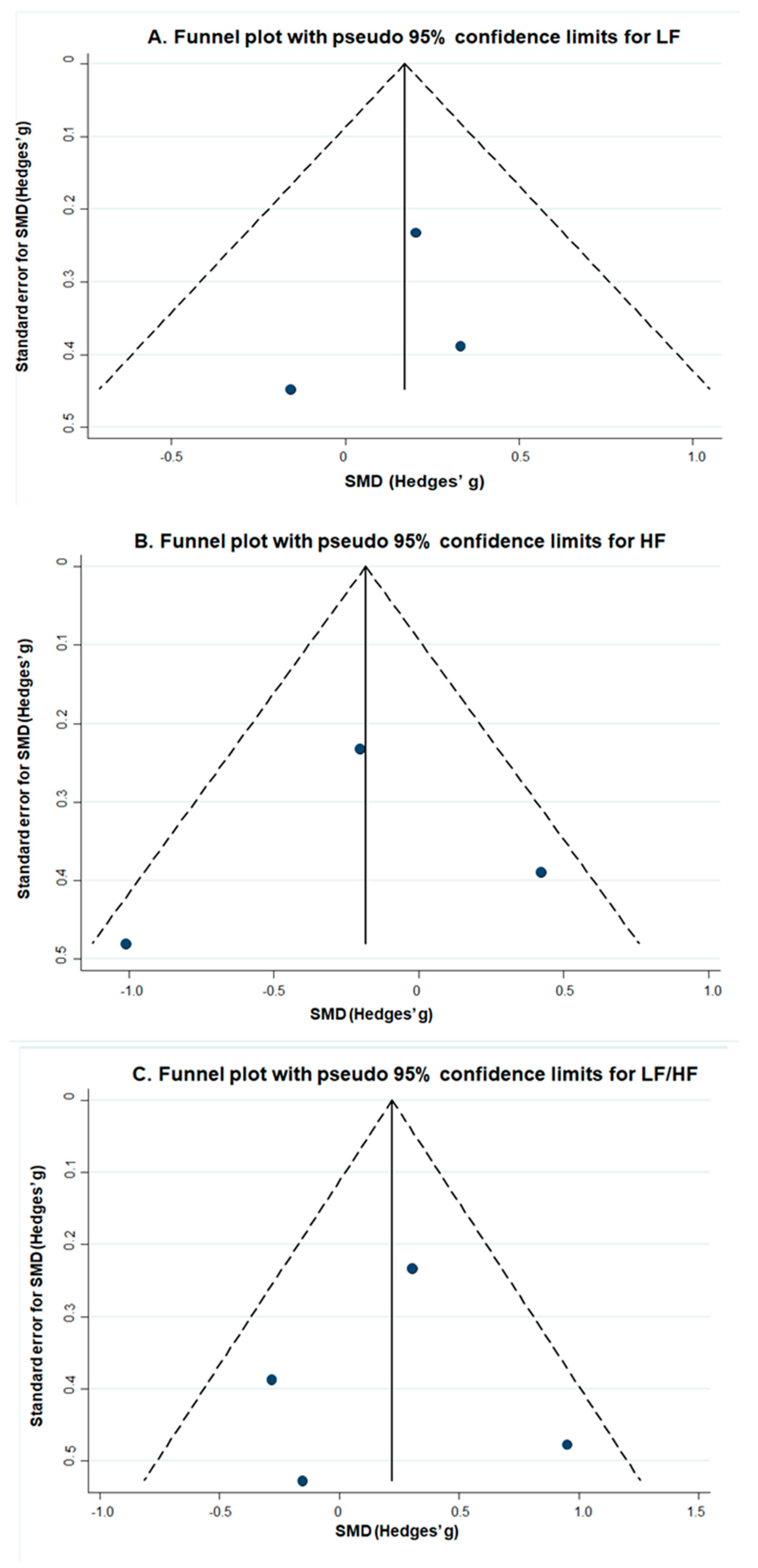
3.5.1. Frequency Domain Measures: LF, HF, and LF/HF Ratio
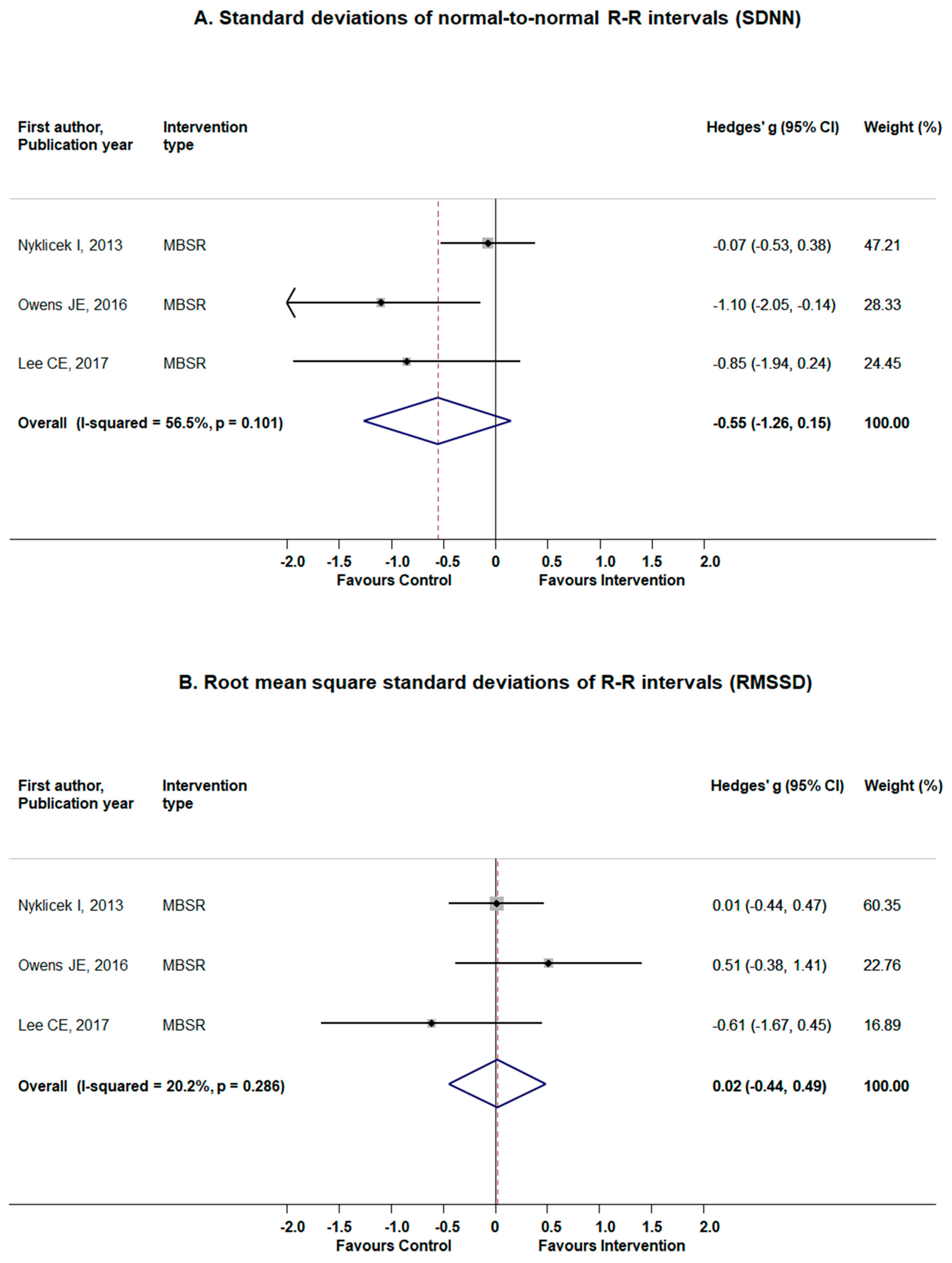
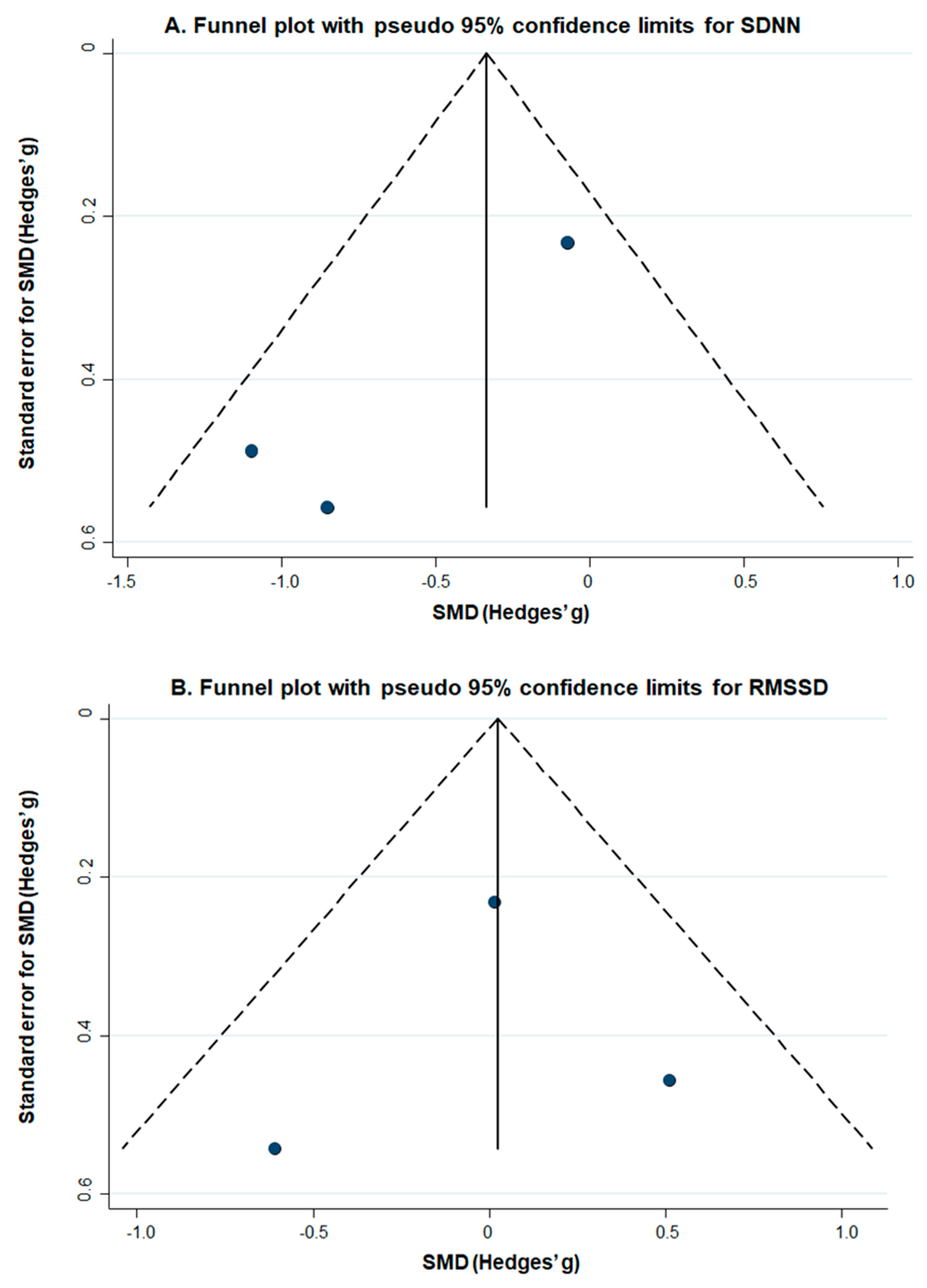
3.5.2. Time Domain Measures: SDNN and RMSSD
4. Discussion
4.1. Comparison to Existing Literature
4.2. Limitations
4.3. Clinical Implications and Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Outcome | Study Omitted and Ill-Health Status of Study Population | Pooled Hedges’ g (95% CI) if Indicated Study Is Omitted |
|---|---|---|
| IL-6 | Pooled results from the main analysis | 0.02 (−0.29 to 0.34) |
| Creswell, 2012 (healthy individuals) | −0.06 (−0.44 to 0.31) | |
| Smith, 2017 (post-menopausal BMI > 30) | 0.12 (−0.19 to 0.44) | |
| Bower, 2015 (breast cancer) | 0.09 (−0.32 to 0.50) | |
| Hoge, 2017 (generalized anxiety disorder) | −0.08 (−0.49 to 0.32) | |
| CRP | Pooled results from the main analysis | 0.12 (−0.10 to 0.33) |
| Creswell, 2012 (healthy individuals) | 0.16 (−0.07 to 0.39) | |
| Memon, 2017 (moderate depression & anxiety) | −0.01 (−0.31 to 0.29) | |
| Smith, 2017 (post-menopausal BMI > 30) | 0.13 (−0.10 to 0.36) | |
| Bower, 2015 (breast cancer) | 0.15 (−0.09 to 0.39) | |
| Fogarty, 2015 (rheumatoid arthritis) | 0.10 (−0.13 to 0.33) | |
| LF | Pooled results from the main analysis | 0.17 (−0.18 to 0.53) |
| Nyklicek, 2013 (stress-related complaints) | 0.12 (−0.45 to 0.70) | |
| Owens, 2016 (heart palpitation) | 0.24 (−0.15 to 0.63) | |
| Faucher, 2016 (social anxiety) | 0.13 (−0.28 to 0.53) | |
| HF | Pooled results from the main analysis | −0.21 (−0.88 to 0.45) |
| Nyklicek, 2013 (stress-related complaints) | −0.26 (−1.67 to 1.13) | |
| Owens, 2016 (heart palpitation) | 0.03 (−0.56 to 0.62) | |
| Faucher, 2016 (social anxiety) | −0.49 (−1.25 to 0.26) | |
| LF/HF ratio | Pooled results from the main analysis | 0.21 (−0.26 to 0.67) |
| Lee, 2017 (breast cancer) | 0.28 (−0.29 to 0.85) | |
| Nyklicek, 2013 (stress-related complaints) | 0.15 (−0.62 to 0.92) | |
| Owens, 2016 (heart palpitation) | 0.11 (−0.25 to 0.48) | |
| Faucher, 2016 (social anxiety) | 0.36 (−0.11 to 0.83) | |
| SDNN | Pooled results from the main analysis | −0.55 (−1.26 to 0.15) |
| Lee, 2017 (breast cancer) | −0.49 (−1.48 to 0.49) | |
| Nyklicek, 2013 (stress-related complaints) | −0.99 (−1.71 to −0.27) | |
| Owens, 2016 (heart palpitation) | −0.30 (−0.99 to 0.39) | |
| RMSSD | Pooled results from the main analysis | 0.02 (−0.44 to 0.49) |
| Lee, 2017 (breast cancer) | −0.12 (−0.29 to 0.52) | |
| Nyklicek, 2013 (stress-related complaints) | −0.01 (−1.11 to 1.08) | |
| Owens, 2016 (heart palpitation) | −0.10 (−0.58 to 0.37) |



References
- Goldberg, S.B.; Tucker, R.P.; Greene, P.A.; Davidson, R.J.; Wampold, B.E.; Kearney, D.J.; Simpson, T.L. Mindfulness-based interventions for psychiatric disorders: A systematic review and meta-analysis. Clin. Psychol. Rev. 2018, 59, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Van Dam, N.T.; van Vugt, M.K.; Vago, D.R.; Schmalzl, L.; Saron, C.D.; Olendzki, A.; Meissner, T.; Lazar, S.W.; Kerr, C.E.; Gorchov, J.; et al. Mind the Hype: A Critical Evaluation and Prescriptive Agenda for Research on Mindfulness and Meditation. Perspect. Psychol. Sci. 2018, 13, 36–61. [Google Scholar] [CrossRef] [PubMed]
- Chiesa, A.; Anselmi, R.; Serretti, A. Psychological Mechanisms of Mindfulness-Based Interventions: What Do We Know? Holist. Nurs. Pract. 2014, 28, 124–148. [Google Scholar] [CrossRef] [PubMed]
- Sze, J.A.; Gyurak, A.; Yuan, J.W.; Levenson, R.W. Coherence between emotional experience and physiology: Does body awareness training have an impact? Emotion 2010, 10, 803–814. [Google Scholar] [CrossRef] [Green Version]
- Bishop, S.R. Mindfulness: A Proposed Operational Definition. Clin. Psychol. Sci. Pract. 2004, 11, 230–241. [Google Scholar] [CrossRef]
- Carmody, J.; Baer, R.A.; Lykins, E.L.B.; Olendzki, N. An empirical study of the mechanisms of mindfulness in a mindfulness-based stress reduction program. J. Clin. Psychol. 2009, 65, 613–626. [Google Scholar] [CrossRef]
- Shapiro, S.L.; Carlson, L.E.; Astin, J.A.; Freedman, B. Mechanisms of mindfulness. J. Clin. Psychol. 2006, 62, 373–386. [Google Scholar] [CrossRef]
- Brown, K.W.; Ryan, R.M.; Creswell, J.D. Mindfulness: Theoretical Foundations and Evidence for its Salutary Effects. Psychol. Inq. 2007, 18, 211–237. [Google Scholar] [CrossRef]
- Hölzel, B.K.; Lazar, S.W.; Gard, T.; Schuman-Olivier, Z.; Vago, D.R.; Ott, U. How Does Mindfulness Meditation Work? Proposing Mechanisms of Action from a Conceptual and Neural Perspective. Perspect. Psychol. Sci. 2011, 6, 537–559. [Google Scholar] [CrossRef]
- Niijar, P.; Puppala, V.K.; Dickinson, O.; Duval, S.; Duprez, D.; Kreitzer, M.J.; Benditt, D.G. Modulation of the autonomic nervous system assessed through heart rate variability by a mindfulness-based stress reduction program. Int. J. Cardiol. 2014, 177, 557–559. [Google Scholar] [CrossRef]
- Billman, G.E. Heart Rate Variability—A Historical Perspective. Front. Physiol. 2011, 2, 86. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Heal. 2017, 5, 5. [Google Scholar] [CrossRef] [PubMed]
- Gevirtz, R.N.; Lehrer, P.M.; Schwartz, M.S. Cardiorespiratory biofeedback. In Biofeedback: A Practitioner’s Guide; Schwartz, M.S., Andrasik, F., Eds.; The Guilford Press: New York, NY, USA, 2016; pp. 196–213. [Google Scholar]
- Gorman, J.M.; Sloan, R.P. Heart rate variability in depressive and anxiety disorders. Am. Hear. J. 2000, 140, S77–S83. [Google Scholar] [CrossRef] [PubMed]
- Burg, J.; Wolf, O.; Michalak, J. Mindfulness as Self-Regulated Attention: Associations with Heart Rate Variability. Swiss J. Psychol. 2012, 71, 135–139. [Google Scholar] [CrossRef]
- Malik, M.; Bigger, J.T.; Camm, A.J.; Kleiger, R.E.; Malliani, A.; Moss, A.J.; Schwartz, P.J. Heart rate variability: Standards of measurement, physiological interpretation, and clinical use. Eur. Hear. J. 1996, 17, 354–381. [Google Scholar] [CrossRef] [Green Version]
- Leonard, B.E. Inflammation and depression: A causal or coincidental link to the pathophysiology? Acta Neuropsychiatr. 2018, 30, 1–16. [Google Scholar] [CrossRef]
- Miller, A.H.; Raison, C.L. The role of inflammation in depression: From evolutionary imperative to modern treatment target. Nat. Rev. Immunol. 2016, 16, 22–34. [Google Scholar] [CrossRef]
- Dantzer, R.; O’Connor, J.C.; Freund, G.G.; Johnson, R.W.; Kelley, K.W. From inflammation to sickness and depression: When the immune system subjugates the brain. Nat. Rev. Neurosci. 2008, 9, 46–56. [Google Scholar] [CrossRef]
- Irwin, M.R.; Cole, S.W. Reciprocal regulation of the neural and innate immune systems. Nat. Rev. Immunol. 2011, 11, 625–632. [Google Scholar] [CrossRef]
- Raison, C.L.; Capuron, L.; Miller, A.H. Cytokines sing the blues: Inflammation and the pathogenesis of depression. Trends Immunol. 2006, 27, 24–31. [Google Scholar] [CrossRef]
- Stuart, M.; Baune, B. Chemokines and chemokine receptors in mood disorders, schizophrenia, and cognitive impairment: A systematic review of biomarker studies. Neurosci. Biobehav. Rev. 2014, 42, 93–115. [Google Scholar] [CrossRef] [PubMed]
- Kohler, C.A.; Freitas, T.H.; Stubbs, B.; Maes, M.; Solmi, M.; Veronese, N.; de Andrade, N.Q.; Morris, G.; Fernandes, B.S.; Brunoni, A.R.; et al. Peripheral Alterations in Cytokine and Chemokine Levels After Antidepressant Drug Treatment for Major Depressive Disorder: Systematic Review and Meta-Analysis. Mol. Neurobiol. 2018, 55, 4195–4206. [Google Scholar] [CrossRef] [PubMed]
- Valkanova, V.; Ebmeier, K.P.; Allan, C.L. CRP, IL-6 and depression: A systematic review and meta-analysis of longitudinal studies. J. Affect. Disord. 2013, 150, 736–744. [Google Scholar] [CrossRef] [PubMed]
- Krishnadas, R.; Cavanagh, J. Depression: An inflammatory illness? J. Neurol. Neurosurg. Psychiatry 2012, 83, 495–502. [Google Scholar] [CrossRef]
- Black, D.S.; Slavich, G.M. Mindfulness meditation and the immune system: A systematic review of randomized controlled trials. Ann. N. Y. Acad. Sci. 2016, 1373, 13–24. [Google Scholar] [CrossRef]
- Morgan, N.; Irwin, M.R.; Chung, M.; Wang, C. The Effects of Mind-Body Therapies on the Immune System: Meta-Analysis. PLoS ONE 2014, 9, e100903. [Google Scholar] [CrossRef]
- Zou, L.; Sasaki, J.E.; Wei, G.-X.; Huang, T.; Yeung, A.S.; Neto, O.B.; Chen, K.W.; Hui, S.S.-C. Effects of Mind–Body Exercises (Tai Chi/Yoga) on Heart Rate Variability Parameters and Perceived Stress: A Systematic Review with Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2018, 7, 404. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Chichester, UK, 2011. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [Green Version]
- UK Network for Mindfulness-Based Teachers. Good Practice Guidelines for Teaching Mindfulness-Based Courses. Available online: www.mindfulnessteachersuk.org.uk (accessed on 7 October 2019).
- Lengacher, C.A.; Johnson-Mallard, V.; Post-White, J.; Moscoso, M.S.; Jacobsen, P.B.; Klein, T.W.; Widen, R.H.; Fitzgerald, S.G.; Shelton, M.M.; Barta, M.; et al. Randomized controlled trial of mindfulness-based stress reduction (MBSR) for survivors of breast cancer. Psycho-Oncology 2009, 18, 1261–1272. [Google Scholar] [CrossRef]
- Duncan, L.G.; Bardacke, N. Mindfulness-Based Childbirth and Parenting Education: Promoting Family Mindfulness During the Perinatal Period. J. Child. Fam. Stud. 2010, 19, 190–202. [Google Scholar] [CrossRef]
- Centre for Reviews and Dissemination. Systematic Reviews; University of York: York, UK, 2009. [Google Scholar]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.E.; Kim, S.; Joo, H.M. Effects of a Mindfulness-Based Stress Reduction Program on the Physical and Psychological Status and Quality of Life in Patients with Metastatic Breast Cancer. Holist. Nurs. Pract. 2017, 31, 260–269. [Google Scholar] [CrossRef] [PubMed]
- Fogarty, F.A.; Booth, R.J.; Gamble, G.D.; Dalbeth, N.; Consedine, N.S. The effect of mindfulness-based stress reduction on disease activity in people with rheumatoid arthritis: A randomised controlled trial. Ann. Rheum. Dis. 2015, 74, 472–474. [Google Scholar] [CrossRef] [PubMed]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. Effect sizes based on means. In Introduction to Meta-Analysis; Borenstein, M., Hedges, L.V., Higgins, J.P.T., Rothstein, H.R., Eds.; Wiley: Chichester, UK, 2009; pp. 21–32. [Google Scholar]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Creswell, J.D.; Irwin, M.R.; Burklund, L.J.; Lieberman, M.D.; Arevalo, J.M.G.; Ma, J.; Breen, E.C.; Cole, S.W. Mindfulness-Based Stress Reduction training reduces loneliness and pro-inflammatory gene expression in older adults: A small randomized controlled trial. Brain Behav. Immun. 2012, 26, 1095–1101. [Google Scholar] [CrossRef] [Green Version]
- Nyklíček, I.; Mommersteeg, P.M.C.; Van Beugen, S.; Ramakers, C.; Van Boxtel, G.J. Mindfulness-based stress reduction and physiological activity during acute stress: A randomized controlled trial. Health Psychol. 2013, 32, 1110–1113. [Google Scholar] [CrossRef]
- Bower, J.E.; Crosswell, A.D.; Stanton, A.L.; Crespi, C.M.; Winston, D.; Arevalo, J.; Ma, J.; Cole, S.W.; Ganz, P.A. Mindfulness Meditation for Younger Breast Cancer Survivors: A Randomized Controlled Trial. Cancer 2015, 121, 1231–1240. [Google Scholar] [CrossRef]
- Owens, J.E.; Schorling, J.; Plews-Ogan, M.; Goodman, M.; Moorman, R.; Zaklin, R.; Dent, J. A randomized controlled trial evaluating Mindfulness-Based Stress Reduction (MBSR) for the treatment of palpitations: A pilot study. Int. J. Cardiol. 2016, 223, 25–27. [Google Scholar] [CrossRef]
- Fu, R.; Vandermeer, B.W.; Shamliyan, T.A.; O’Neil, M.E.; Yazdi, F.; Fox, S.H.; Morton, S.C. Handling Continuous Outcomes in Quantitative Synthesis. Methods Guide for Comparative Effectiveness Reviews; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2013.
- Higgins, J.P.T.; White, I.R.; Anzures-Cabrera, J. Meta-analysis of skewed data: Combining results reported on log-transformed or raw scales. Stat. Med. 2008, 27, 6072–6092. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Tobias, A. Assessing the influence of a single study in the meta-anyalysis estimate. Stata Tech. Bull. 1999, 8, 15–17. [Google Scholar]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazumdar, M.; Begg, C.B. Operating Characteristics of a Rank Correlation Test for Publication Bias. Biometrics 1994, 50, 1088. [Google Scholar]
- Faucher, J.; Koszycki, D.; Bradwejn, J.; Merali, Z.; Bielajew, C. Effects of CBT Versus MBSR Treatment on Social Stress Reactions in Social Anxiety Disorder. Mindfulness 2016, 7, 514–526. [Google Scholar] [CrossRef]
- Hoge, E.A.; Bui, E.; Palitz, S.A.; Schwarz, N.R.; Owens, M.E.; Johnston, J.M.; Pollack, M.H.; Simon, N.M. The effect of mindfulness meditation training on biological acute stress responses in generalized anxiety disorder. Psychiatry Res. 2017, 262, 328–332. [Google Scholar] [CrossRef] [PubMed]
- Memon, A.A.; Sundquist, K.; Ahmad, A.; Wang, X.; Hedelius, A.; Sundquist, J. Role of IL-8, CRP and epidermal growth factor in depression and anxiety patients treated with mindfulness-based therapy or cognitive behavioral therapy in primary health care. Psychiatry Res. Neuroimaging 2017, 254, 311–316. [Google Scholar] [CrossRef]
- Smith, B.W.; Shelley, B.M.; Sloan, A.L.; Colleran, K.; Erickson, K. A Preliminary Randomized Controlled Trial of a Mindful Eating Intervention for Post-menopausal Obese Women. Mindfulness 2017, 9, 836–849. [Google Scholar] [CrossRef]
- Heckenberg, R.A.; Eddy, P.; Kent, S.; Wright, B.J. Do workplace-based mindfulness meditation programs improve physiological indices of stress? A systematic review and meta-analysis. J. Psychosom. Res. 2018, 114, 62–71. [Google Scholar] [CrossRef]





| First Author (Year) | Country | Setting | Inclusion Criteria | Design | Outcome | Main Findings |
|---|---|---|---|---|---|---|
| Bower et al. (2015) | USA | Out-patient | Patients with diagnosis of stage 0, I, II, or III breast cancer at or before age 50 years; and who had completed local and/or adjuvant cancer therapy (except hormone therapy) | RCT comparing MAP (mindful awareness practices) with TAU | IL-6 | There were no significant intervention effects for IL-6 (p > 0.20 for both). |
| Creswell et al. (2012) | USA | Non-clinical | Healthy older adults who indicated an interest in learning mindfulness meditation techniques, English-speaking, not currently practicing any mind–body therapies, non-smokers, mentally and physically healthy for the last three months, and not currently taking medications that affect immune, cardiovascular, endocrine, or psychiatric functioning | RCT comparing MBSR with a wait-list control group | IL-6 and CRP | There was a trend for MBSR to reduce CPR (treatment condition - time interaction): (F(1,33) = 3.39, p = 0.075). |
| Faucher et al. (2016) | Canada | Out-patient | Outpatients with social anxiety disorder, according to DMS-IV criteria, and score > 50 on Liebowitz Social Anxiety Scale, and score > 4 on Clinical Global Impression of Illness subscale, medication-free. | RCT comparing MBSR with a CBT group program | HRV (LF, HF and LF/HF) | No physiological differences were found as a function of treatment |
| Fogarty et al. (2015) | New Zealand | Out-patient | Patients with reumathoid arthritis, according to the 1987 American College of Rheumatology classification criteria and without any prior meditation experience | RCT comparing MBSR with TAU | CRP | There were no significant group-time effects on CRP levels |
| Hoge et al. (2017) | USA | Out-patient | Individuals age 18 or older were eligible if they: (a) met DSM-IV criteria forcurrent primary GAD and designated GAD as the primary problem, and (b) scored 20 or above on the Hamilton Anxiety scale (HAM-A). | RCT comparing MBSR with additional metta (loving-kindness meditation) already in the first class, compared to an active control consisting of Stress Management Education (attention control) | IL-6 | The MBSR group had a greater reduction in inflammatory cytokines IL-6 AUC concentrations compared to controls |
| Lee et al. (2017) | South Korea | Out-patient | Patients diagnosed with metastatic breast cancer who were currently undergoing anti cancerous treatment in an outpatient clinic, were 20 years of age or older, and were able to read and write in Korean | Non-randomized controlled trial with non-equivalent control group comparing MBSR with TAU | HRV (SDNN, RMSSD, LF/HF) | For HRV, although there was no significant difference between the groups for SDNN, RMSS, total power, and LF/HF, improved tendencies were observed in the MBSR group for SDNN from 24.81 to 53.93 (p = 0.051) |
| Memon et al. (2017) | Sweden | Out-patient | Patients with mild to moderate depression and anxiety, aged between 20 and 64 years, were fluent in Swedish and had a score of ≥10 on the PHQ-9, ≥7 on the HADS-D or HADS-A or a score on the MADRS between 13 and 34. | RCT comparing MBSR with TAU (including CBT and pharmacological treatment for some patients) | IL-6 and hsCRP | Levels of inflammatory markers analyzed in this study, were not significantly associated with treatment response on any scale. |
| Nyklicek et al. (2013) | The Netherlands | Non-clinical | People having stress-related complaints, potential participants were eligible if they answered with "regularly" or "often" to the question “how often would you say you feel distressed?” | RCT comparing MBSR with TAU | HRV (SDNN, RMSSD, LF/HF, HF and LF) | No effects were obtained on HRV measures. |
| Owens et al. (2016) | USA | Out-patient | Patients reporting heart palpitations of at least two months duration, willingness to attend MBSR classes and comply with the data collection protocol. | RCT comparing MBSR with TAU | HRV (SDNN, RMSSD, LF/HF, HF and LF) | There were no significant differences between the MBSR and Control groups on any of the HRV measures at baseline, 8 weeks, or 12 weeks. An association was found between HRV balance (as measured by the Ln LF/HF ratio) and improvement in palpitations in the MBSR group (r = 0.8, p < 0.001) |
| Smith et al. (2017) | USA | Out-patient | Women aged 50–70 years with post-menopausal status, a BMI of more than 30, ability to participate in the study for 1 year, fluency in English, and ability to walk at least 10 min without stopping. | RCT comparing MEAL (Mindful eating and living) with a group session with same schedule as the intervention | IL-6, CRP | The reductions in IL-6 and CRP were significantly greater for the MEAL as compared with the control group. |
| Participant Characteristics | Intervention and Control Condition Name and Duration | |||
|---|---|---|---|---|
| First Author (Year) | Mean Age and (Range) in Years | Female (%) | N Total | |
| Bower et al. (2015) | I: 46.1 (28.4–60.0) C: 47.7 (31.1–59.6) | I: 100%; C: 100% | 65 | A 6-week Mindful Awareness Practices intervention consisting of 2-h weekly meetings. Comparison: TAU |
| Creswell et al. (2012) | I: 64.35 (N/A) C: 65.16 (N/A) | I: 85%; C: 75% | 40 | An 8-week Mindfulness Based Stress Reduction intervention consisting of 2-h weekly meetings and a 7-h weekend day retreat. Comparison: wait-list control |
| Faucher et al. (2016) | I: 36.64 (N/A) C: 39.31 (N/A) | I: 35.7% C: 38.5% | 38 | An 8-week Mindfulness Based Stress Reduction intervention consisting of 2.5 h weekly meetings and a 7.5 h weekend day retreat. Comparison: a 12-week Cognitive Behavioural Group Therapy intervention consisting of 2.5 h weekly meetings (included psychoeducation, exposure, cognitive restructuring and homework assignments). |
| Fogarty et al. (2015) | I: 52 (N/A) C: 55 (N/A) | I: 91%; C: 86% | 51 | An 8-week Mindfulness Based Stress Reduction intervention consisting of 2-h weekly meetings and a full day weekend retreat. Comparison: TAU |
| Hoge et al. (2017) | I: 40 (N/A) C: 38 (N/A) | I: 43C: 50 | 70 | An 8-week Mindfulness Based Stress Reduction consisting of 2-h weekly meetings and a 4-h weekend retreat, including an additional loving-kindness practice introduced already at the first session. Comparison: Stress Management Education lectures on overall health and wellness such as diet, exercise, sleep, and time management. |
| Lee et al. (2017) | I: 52 (33–64) C: 57 (37–67) | I: 100%; C: 100% | 32 | An 8-week Mindfulness Based Stress Reduction intervention consisting of 2 h weekly meetings. Comparison: TAU |
| Memon et al. (2017) | I: 42 (N/A) C: 41 (N/A) | I: 83%; C: 92% | 166 | An 8-week Mindfulness Based Stress Reduction intervention consisting of 2 h weekly meetings. Comparison: TAU (including CBT and pharmacological treatment for some patients) |
| Nyklicek et al. (2013) | I: 47.4 (N/A) C: 44.9 (N/A) | I: 65% C: 76% | 85 | An 8-week Mindfulness Based Stress Reduction intervention consisting of 2.5-h weekly meetings. Comparison: TAU |
| Owens et al. (2016) | I: N/A (N/A) C: N/A (N/A) | I: N/A; C: N/A% | 20 | An 8-week Mindfulness Based Stress Reduction intervention consisting of 2.5-h weekly meetings. Comparison: TAU |
| Smith et al. (2017) | I: 58.56 (N/A) 58.56 (N/A) | I: 100% C: 100% | 40 | A 6-week Mindful Eating and Living (MEAL) intervention consisting of 2-h weekly meetings. Comparison: A control program created to match the intervention, and consisting of weight loss group sessions conducted according to the same schedule as the MEAL group. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rådmark, L.; Sidorchuk, A.; Osika, W.; Niemi, M. A Systematic Review and Meta-Analysis of the Impact of Mindfulness Based Interventions on Heart Rate Variability and Inflammatory Markers. J. Clin. Med. 2019, 8, 1638. https://doi.org/10.3390/jcm8101638
Rådmark L, Sidorchuk A, Osika W, Niemi M. A Systematic Review and Meta-Analysis of the Impact of Mindfulness Based Interventions on Heart Rate Variability and Inflammatory Markers. Journal of Clinical Medicine. 2019; 8(10):1638. https://doi.org/10.3390/jcm8101638
Chicago/Turabian StyleRådmark, Lina, Anna Sidorchuk, Walter Osika, and Maria Niemi. 2019. "A Systematic Review and Meta-Analysis of the Impact of Mindfulness Based Interventions on Heart Rate Variability and Inflammatory Markers" Journal of Clinical Medicine 8, no. 10: 1638. https://doi.org/10.3390/jcm8101638