Comparison of Rigid and Soft-Brace Treatments for Acute Osteoporotic Vertebral Compression Fracture: A Prospective, Randomized, Multicenter Study

 , ,
, ,
Abstract
:1. Introduction
2. Experimental Section
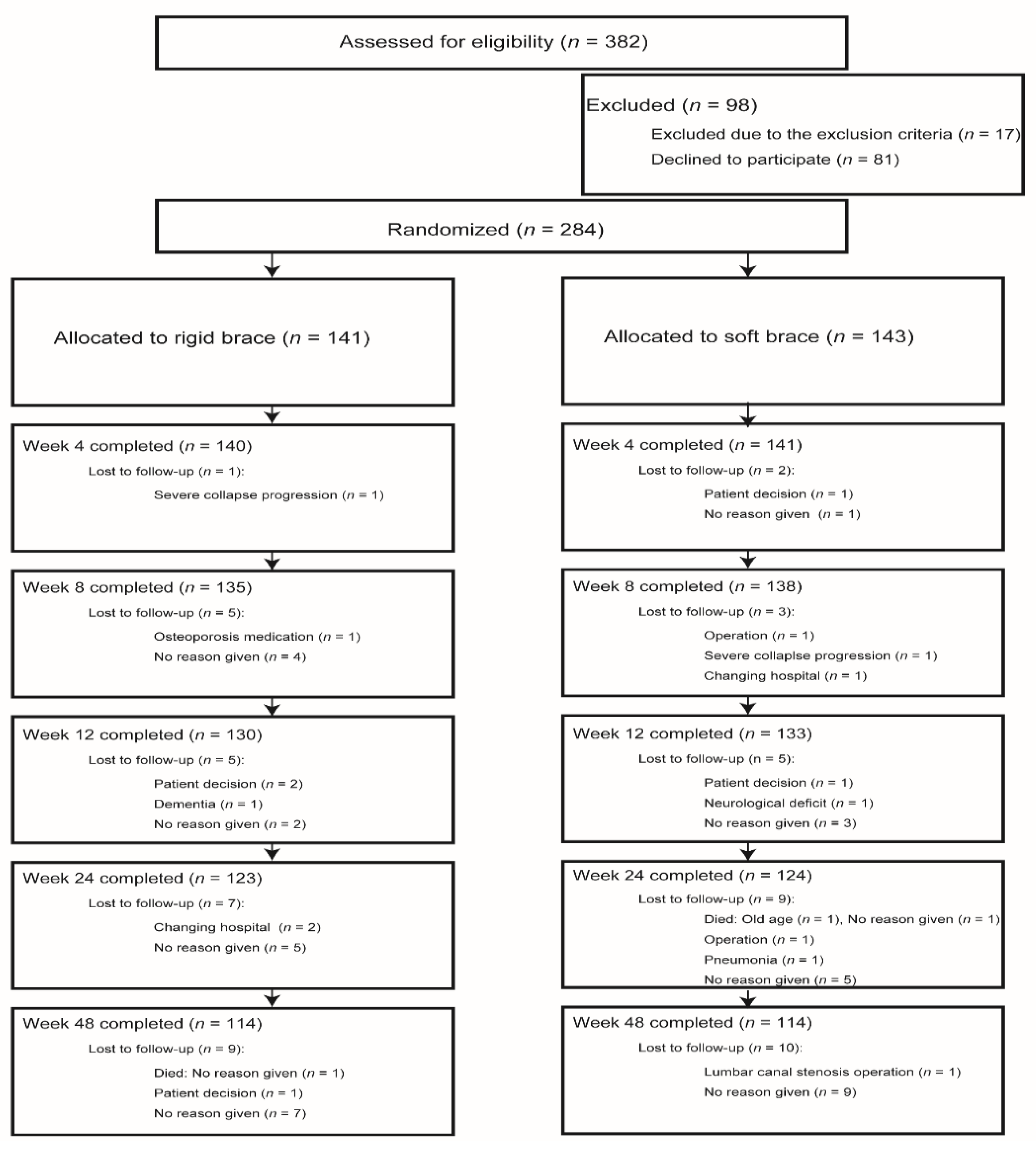
2.1. Trial Design
2.2. Interventions
2.3. Data Collection and Outcomes
2.4. Statistical Analysis
2.5. Availability of Data and Material
2.6. Trial Registration
3. Results
3.1. Baseline Characteristics of the Patients
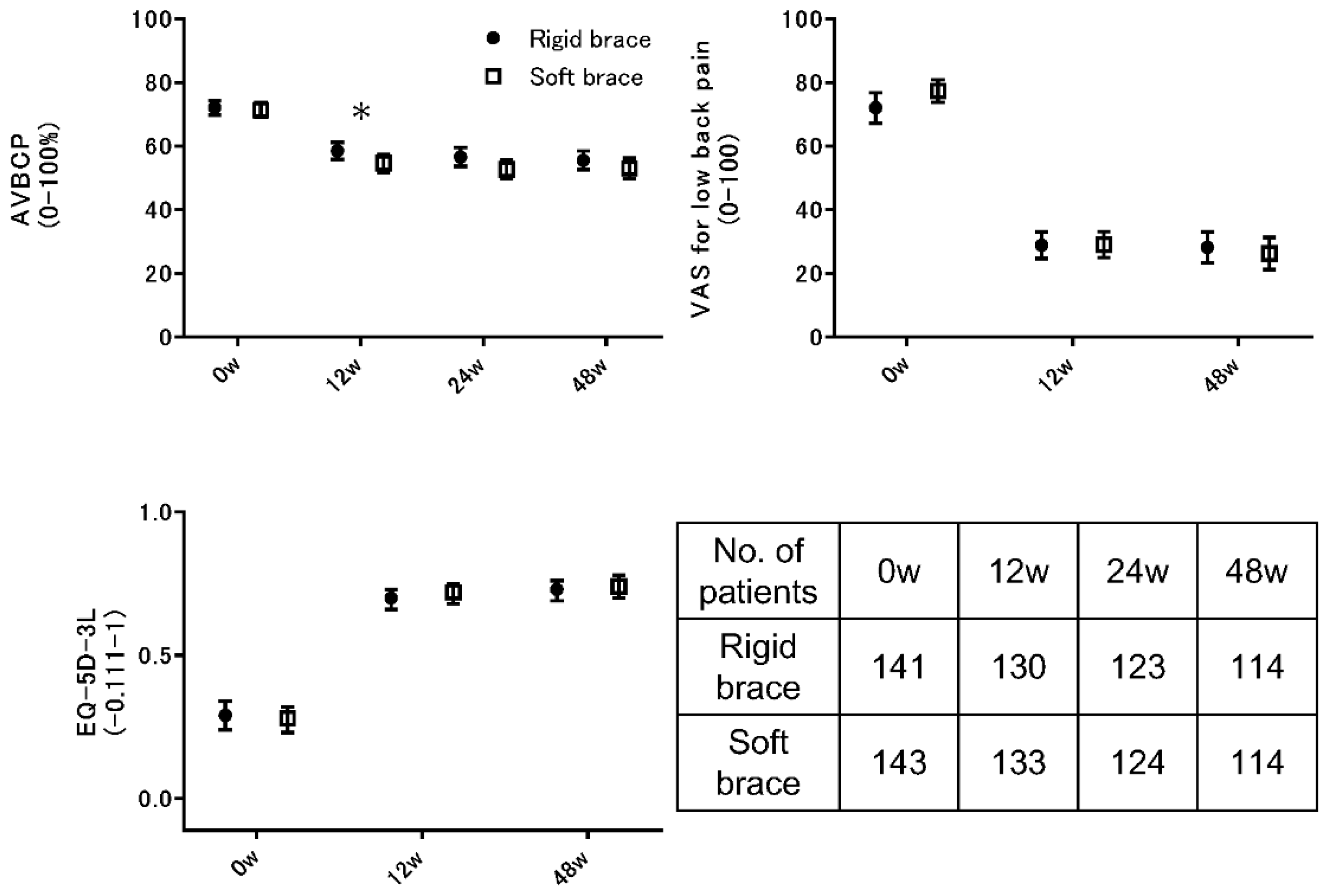
3.2. Primary Outcome
3.3. Secondary Outcomes
3.4. Ancillary Analysis
3.5. Brace Compliance and the Use of Analgesics
3.6. Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Genant, H.K.; Cooper, C.; Poor, G.; Reid, I.; Ehrlich, G.; Kanis, J.; Nordin, B.E.; Barrett-Connor, E.; Black, D.; Bonjour, J.P.; et al. Interim report and recommendations of the World Health Organization Task-Force for Osteoporosis. Osteoporos. Int. 1999, 10, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Van Der Klift, M.; De Laet, C.E.; Mccloskey, E.V.; Hofman, A.; Pols, H.A. The incidence of vertebral fractures in men and women: The Rotterdam Study. J. Bone Min. Res. 2002, 17, 1051–1056. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.C.; McGirt, M.J. Vertebral compression fractures: A review of current management and multimodal therapy. J. Multidiscip. Healthc. 2013, 6, 205–214. [Google Scholar] [PubMed]
- Genev, I.K.; Tobin, M.K.; Zaidi, S.P.; Khan, S.R.; Amirouche, F.M.; Mehta, A.I. Spinal Compression Fracture Management: A Review of Current Treatment Strategies and Possible Future Avenues. Glob. Spine J. 2017, 7, 71–82. [Google Scholar] [CrossRef] [PubMed]
- Edidin, A.A.; Ong, K.L.; Lau, E.; Kurtz, S.M. Mortality risk for operated and nonoperated vertebral fracture patients in the medicare population. J. Bone Min. Res. 2011, 26, 1617–1626. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Vaccaro, A.R. Osteoporotic compression fractures of the spine; current options and considerations for treatment. Spine J. 2006, 6, 479–487. [Google Scholar] [CrossRef]
- Lantz, S.A.; Schultz, A.B. Lumbar spine orthosis wearing. I. Restriction of gross body motions. Spine 1986, 11, 834–837. [Google Scholar] [CrossRef]
- Pfeifer, M.; Kohlwey, L.; Begerow, B.; Minne, H.W. Effects of two newly developed spinal orthoses on trunk muscle strength, posture, and quality-of-life in women with postmenopausal osteoporosis: A randomized trial. Am. J. Phys. Med. Rehabil. 2011, 90, 805–815. [Google Scholar] [CrossRef]
- Meccariello, L.; Muzii, V.F.; Falzarano, G.; Medici, A.; Carta, S.; Fortina, M.; Ferrata, P. Dynamic corset versus three-point brace in the treatment of osteoporotic compression fractures of the thoracic and lumbar spine: A prospective, comparative study. Aging Clin. Exp. Res. 2017, 29, 443–449. [Google Scholar] [CrossRef]
- Giele, B.M.; Wiertsema, S.H.; Beelen, A.; van der Schaaf, M.; Lucas, C.; Been, H.D.; Bramer, J.A. No evidence for the effectiveness of bracing in patients with thoracolumbar fractures. Acta Orthop. 2009, 80, 226–232. [Google Scholar] [CrossRef]
- Matsunaga, S.; Hayashi, K.; Naruo, T.; Nozoe, S.I.; Komiya, S. Psychologic management of brace therapy for patients with idiopathic scoliosis. Spine (Phila Pa 1976) 2005, 30, 547–550. [Google Scholar] [CrossRef]
- Newman, M.; Lowe, C.M.; Barker, K. Spinal Orthoses for Vertebral Osteoporosis and Osteoporotic Vertebral Fracture: A Systematic Review. Arch. Phys. Med. Rehabil. 2016, 97, 1013–1025. [Google Scholar] [CrossRef]
- Chiba, K.; Yoshida, M.; Shinomiya, K.; Satomi, K.; Nagata, K. Conservative managements for osteoporotic vertebral fractures: Results of pilot multicenter prospective randomized controlled trial. J. Jpn. Orthop. Assoc. 2011, 85, 934–941. [Google Scholar]
- Kim, H.J.; Yi, J.M.; Cho, H.G.; Chang, B.S.; Lee, C.K.; Kim, J.H.; Yeom, J.S. Comparative study of the treatment outcomes of osteoporotic compression fractures without neurologic injury using a rigid brace, a soft brace, and no brace: A prospective randomized controlled non-inferiority trial. J. Bone Joint Surg. 2014, 96, 1959–1966. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Law, S.W.; Cheng, J.; Kee, H.M.; Wong, M.S. A comparison study on the efficacy of SpinoMed(R) and soft lumbar orthosis for osteoporotic vertebral fracture. Prosthet. Orthot. Int. 2015, 39, 270–276. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; Loppini, M.; Denaro, L.; Maffulli, N.; Denaro, V. Osteoporotic vertebral fractures: Current concepts of conservative care. Br. Med. Bull. 2012, 102, 171–189. [Google Scholar] [CrossRef]
- Keynan, O.; Fisher, C.G.; Vaccaro, A.; Fehlings, M.G.; Oner, F.C.; Dietz, J.; Kwon, B.; Rampersaud, R.; Bono, C.; France, J.; et al. Radiographic measurement parameters in thoracolumbar fractures: A systematic review and consensus statement of the spine trauma study group. Spine 2006, 31, E156–E165. [Google Scholar] [CrossRef] [PubMed]
- EuroQol, G. EuroQol—A new facility for the measurement of health-related quality of life. Health Policy (Amsterdam, Netherlands) 1990, 16, 199–208. [Google Scholar]
- McCormack, H.M.; David, J.D.L.; Sheather, S. Clinical applications of visual analogue scales: A critical review. Psychol. Med. 1988, 18, 1007–1019. [Google Scholar] [CrossRef]
- Fukui, M.; Chiba, K.; Kawakami, M.; Kikuchi, S.; Konno, S.; Miyamoto, M.; Seichi, A.; Shimamura, T.; et al. JOA Back Pain Evaluation Questionnaire: initial report. J. Orthop. Sci. 2007, 12, 443–450. [Google Scholar] [CrossRef] [PubMed]
- Team, R.C. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2013. [Google Scholar]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transp. 2013, 48, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, S.; Hoshino, M.; Takayama, K.; Iseki, K.; Sasaoka, R.; Tsujio, T.; Yasuda, H.; Sasaki, T.; Kanematsu, F.; Kono, H.; et al. Predicting delayed union in osteoporotic vertebral fractures with consecutive magnetic resonance imaging in the acute phase: A multicenter cohort study. Osteoporos. Int. 2016, 27, 3567–3575. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, H.; Hoshino, M.; Tsujio, T.; Terai, H.; Namikawa, T.; Kato, M.; Matsumura, A.; Suzuki, A.; Takayama, K.; Takahashi, S.; et al. Difference of clinical course between cases with bone union and those with delayed union following osteoporotic vertebral fractures. Arch. Osteoporos. 2017, 13, 3. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, K.; Okamoto, M.; Hatsushikano, S.; Shimoda, H.; Ono, M.; Watanabe, K. Normative values of spino-pelvic sagittal alignment, balance, age, and health-related quality of life in a cohort of healthy adult subjects. Eur. Spine J. 2016, 25, 3675–3686. [Google Scholar] [CrossRef] [PubMed]
- Chaléat-Valayer, E.; Mac-Thiong, J.M.; Paquet, J.; Berthonnaud, E.; Siani, F.; Roussouly, P. Sagittal spino-pelvic alignment in chronic low back pain. Eur. Spine J. 2011, 20, 634–640. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.T.; Lane, J.M. Nonmedical management of osteoporosis. Curr. Opin. Rheumatol. 2002, 14, 441–446. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Rigid Brace | Soft Brace |
|---|---|---|
| n = 141 | n = 143 | |
| Mean age (SD), years | 76.0 (5.2) | 75.5 (5.4) |
| Mean time since fracture, weeks | 1.5 (1.2) | 1.5 (1.3) |
| No previous osteoporosis therapy, n (%) | 21 (15) | 26 (18) |
| No prevalent vertebral fracture, n (%) | 107 (76) | 105 (73) |
| Any prevalent vertebral fracture, n (%) | 34 (24) | 38 (27) |
| Level, n (%) | ||
| T10 | 3 (2) | 3 (2) |
| T11 | 13 (9) | 11(8) |
| T12 | 45 (32) | 62 (43) |
| L1 | 49 (35) | 46 (32) |
| L2 | 31 (22) | 21 (15) |
| AVBCP, (%) | 72.2 (13.5) | 71.4 (14.3) |
| EQ-5D-3L score | 0.29 (0.30) | 0.28 (0.28) |
| VAS score for back pain | 72.1 (28.5) | 77.4 (21.3) |
| JOABPEQ score | ||
| Pain-related disorders | 34.9 (30.6) | 29.7 (30.6) |
| Lumbar function | 19.8 (27.4) | 18.0 (23.4) |
| Walking ability | 21.8 (28.4) | 20.9 (26.5) |
| Social life function | 21.7 (25.6) | 21.9 (26.2) |
| Mental health | 39.1 (22.4) | 38.7 (21.9) |
| Rigid Brace | Soft Brace | Difference (95% CI) | p-Value | |
|---|---|---|---|---|
| Mean (SD) | Mean (SD) | |||
| Primary outcome | ||||
| AVBCP score | ||||
| Week 12 | 58.5 (15.7) | 54.6 (16.3) | −3.9 (−7.8 to −0.03) | 0.04002 * |
| Week 24 | 56.6 (16.9) | 52.7 (16.9) | −3.9 (−8.1 to 0.4) | 0.07 |
| Week 48 | 55.5 (16.2) | 53.0 (17.3) | −2.5 (−7.0 to 1.8) | 0.20 |
| Secondary outcomes | ||||
| VAS for lower back pain | ||||
| Week 12 | 28.9 (24.1) | 29.1 (23.9) | 0.2 (−5.6 to 6.1) | 0.95 |
| Week 48 | 28.2 (25.8) | 26.3 (27.0) | −1.9 (−8.7 to 5.1) | 0.43 |
| EQ-5D-3L score | ||||
| Week 12 | 0.70 (0.20) | 0.72 (0.18) | 0.02 (−0.03 to 0.06) | 0.58 |
| Week 48 | 0.73 (0.20) | 0.74 (0.22) | 0.01 (−0.04 to 0.07) | 0.67 |
| JOABPEQ | ||||
| Pain-related disorder | ||||
| Week 12 | 69.5 (31.7) | 73.1 (30.0) | 3.6 (−3.9 to 11.1) | 0.38 |
| Week 48 | 57.3 (29.8) | 60.6 (29.4) | 3.3 (−4.4 to 11.0) | 0.43 |
| Lumbar function | ||||
| Week 12 | 55.9 (30.0) | 60.1 (28.8) | 4.2 (−3.0 to 11.3) | 0.29 |
| Week 48 | 66.4 (28.4) | 64.8 (31.1) | −1.6 (−9.5 to 6.1) | 0.91 |
| Walking ability | ||||
| Week 12 | 54.7 (33.4) | 55.0 (32.0) | 0.3 (−7.6 to 8.3) | 0.92 |
| Week 48 | 61.9 (33.3) | 62.3 (34.7) | 0.4 (−8.5 to 9.3) | 0.82 |
| Social life function | ||||
| Week 12 | 50.9 (27.8) | 53.6 (26.0) | 2.7 (−3.8 to 9.3) | 0.36 |
| Week 48 | 57.7 (28.4) | 63.4 (24.2) | 5.7 (−1.2 to 12.6) | 0.12 |
| Mental health | ||||
| Week 12 | 52.1 (19.2) | 54.5 (19.7) | 2.4 (−2.3 to 7.1) | 0.14 |
| Week 48 | 55.9 (19.2) | 55.6 (19.4) | −0.3 (−5.3 to 4.8) | 0.96 |
| Outcome | Spearman’s Rank Correlation Rho | p |
|---|---|---|
| EQ-5D-3L score | 0.09 | 0.19 |
| VAS score for back pain | −0.19 | 0.003 * |
| JOABPEQ score | ||
| Pain-related disorders | 0.24 | 0.0002 * |
| Lumbar function | 0.11 | 0.37 |
| Walking ability | 0.06 | 0.31 |
| Social life function | 0.06 | 0.39 |
| Mental health | 0.01 | 0.87 |
| Time | Group | 4 Weeks | 8 Weeks | 12 Weeks |
|---|---|---|---|---|
| <6 h/day | Rigid brace | 14 | 18 | 24 |
| Soft brace | 7 | 12 | 22 | |
| 6–12 h/day | Rigid brace | 18 | 20 | 22 |
| Soft brace | 19 | 22 | 27 | |
| >12 h/day | Rigid brace | 108 | 97 | 84 |
| Soft brace | 115 | 104 | 84 | |
| Numbers | Rigid brace | 140 | 135 | 130 |
| Soft brace | 141 | 138 | 133 | |
| p-value | 0.30 | 0.49 | 0.77 |
| Medication | Group | 4 Weeks | 8 Weeks | 12 Weeks | 24 Weeks | 48 Weeks |
|---|---|---|---|---|---|---|
| No medication | Rigid brace | 43 | 82 | 98 | 102 | 97 |
| Soft brace | 34 | 77 | 93 | 94 | 96 | |
| Non-opiate medication | Rigid brace | 86 | 46 | 29 | 19 | 17 |
| Soft brace | 92 | 53 | 34 | 25 | 16 | |
| Weak opiates | Rigid brace | 11 | 7 | 3 | 2 | 0 |
| Soft brace | 15 | 8 | 6 | 5 | 2 | |
| Numbers | Rigid brace | 140 | 135 | 130 | 123 | 114 |
| Soft brace | 141 | 138 | 133 | 124 | 114 | |
| p-value | 0.38 | 0.74 | 0.50 | 0.30 | 0.63 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kato, T.; Inose, H.; Ichimura, S.; Tokuhashi, Y.; Nakamura, H.; Hoshino, M.; Togawa, D.; Hirano, T.; Haro, H.; Ohba, T.; et al. Comparison of Rigid and Soft-Brace Treatments for Acute Osteoporotic Vertebral Compression Fracture: A Prospective, Randomized, Multicenter Study. J. Clin. Med. 2019, 8, 198. https://doi.org/10.3390/jcm8020198
Kato T, Inose H, Ichimura S, Tokuhashi Y, Nakamura H, Hoshino M, Togawa D, Hirano T, Haro H, Ohba T, et al. Comparison of Rigid and Soft-Brace Treatments for Acute Osteoporotic Vertebral Compression Fracture: A Prospective, Randomized, Multicenter Study. Journal of Clinical Medicine. 2019; 8(2):198. https://doi.org/10.3390/jcm8020198
Chicago/Turabian StyleKato, Tsuyoshi, Hiroyuki Inose, Shoichi Ichimura, Yasuaki Tokuhashi, Hiroaki Nakamura, Masatoshi Hoshino, Daisuke Togawa, Toru Hirano, Hirotaka Haro, Tetsuro Ohba, and et al. 2019. "Comparison of Rigid and Soft-Brace Treatments for Acute Osteoporotic Vertebral Compression Fracture: A Prospective, Randomized, Multicenter Study" Journal of Clinical Medicine 8, no. 2: 198. https://doi.org/10.3390/jcm8020198