Patient-Reported Outcome Measures for Patients with Diabetes Mellitus Associated with Foot and Ankle Pathologies: A Systematic Review

 , , and
, , and 
Abstract
:1. Introduction
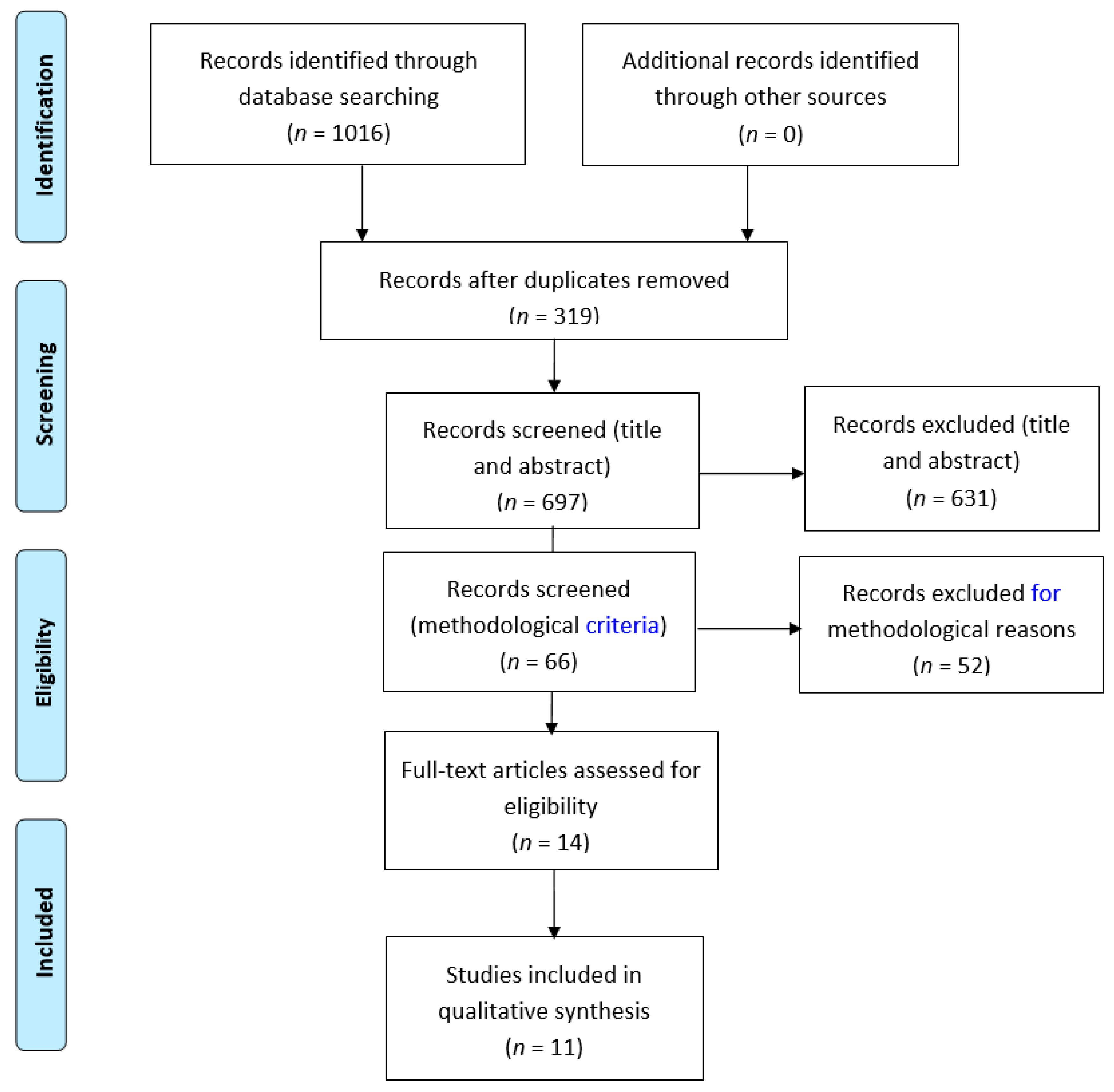
2. Material and Methods
2.1. Design
2.2. Search Strategy
2.3. Inclusion Criteria
- Types of participants: Patients with diabetes mellitus (TIDM or TIIDM), aged >18 years. The studies should be specifically focused on the foot and ankle.
- Types of studies: Psychometric validation studies on patient-reported outcome measures, published in English or Spanish.
- Types of outcomes: Psychometric or clinimetric properties based on criteria according to Terwee (content validity, internal consistency, criterion validity, construct validity, reproducibility, agreement, reliability, responsiveness, floor/ceiling effect and interpretability) or COSMIN (structural validity, internal consistency, reliability, measurement error, hypothesis testing for construct validity, cross cultural validity/measurement invariance, criterion validity and responsiveness).
2.4. Exclusion Criteria
- Types of studies: Studies using questionnaires without evidence supporting their validity or reliability.
2.5. Quality Appraisal
2.6. Study Selection
2.7. Data Extraction
3. Results
3.1. Population
3.2. Dimensions and Items
3.3. Psychometric Properties
3.3.1. Content Validity
3.3.2. Internal Consistency
3.3.3. Criterion Validity
3.3.4. Construct Validity
3.3.5. Reproducibility
3.3.6. Responsiveness
3.3.7. Floor/Ceiling Effect
3.3.8. Interpretability
3.4. Cross-Cultural Adaptation
3.5. Methodological Quality
3.5.1. Structural Validity
3.5.2. Internal Consistency
3.5.3. Reliability
3.5.4. Measurement Error
3.5.5. Hypothesis Testing for Construct Validity
3.5.6. Cross-Cultural Validity/Measurement Invariance
3.5.7. Criterion Validity
3.5.8. Responsiveness
3.6. Methodological Quality Scores Per Study on A Measurement Property
4. Discussion
5. Limitations
6. Clinical Implications
7. Conclusions
Supplementary Materials
Author Contributions
Conflicts of Interest
References
- World Health Organization. Global Report on Diabetes; World Health Organization: Geneva, Switzerland, 2016; ISBN 9789241565257. [Google Scholar]
- Almeida, P.H.R.F.; Silva, T.B.C.; de Assis Acurcio, F.; Guerra Júnior, A.A.; Araújo, V.E.; Diniz, L.M.; Godman, B.; Almeida, A.M.; Alvares, J. Quality of Life of Patients with Type 1 Diabetes Mellitus Using Insulin Analog Glargine Compared with NPH Insulin: A Systematic Review and Policy Implications. Patient 2018, 11, 377–389. [Google Scholar] [CrossRef] [PubMed]
- Shaw, J.E.; Sicree, R.A.; Zimmet, P.Z. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res. Clin. Pract. 2010, 87, 4–14. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association Diabetes Care. Standards of Medical Care in Diabetes—2018. Diabetes Care 2018, 41 (Suppl. 1), S1–S2. [Google Scholar] [CrossRef]
- Palomo-López, P.; Losa-Iglesias, M.E.; Becerro-de-Bengoa-Vallejo, R.; López-López, D.; Rodríguez-Sanz, D.; Romero-Morales, C.; Calvo-Lobo, C. Specific foot health-related quality-of-life impairment in patients with type II versus type I diabetes. Int. Wound J. 2019, 16, 47–51. [Google Scholar] [CrossRef] [PubMed]
- Bôas, N.C.R.V.; Salomé, G.M.; Ferreira, L.M. Frailty syndrome and functional disability among older adults with and without diabetes and foot ulcers. J. Wound Care 2018, 27, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Gebala-Prajsnar, K.; Stanek, A.; Pasek, J.; Prajsnar, G.; Berszakiewicz, A.; Sieron, A.; Cholewka, A. Selected physical medicine interventions in the treatment of diabetic foot syndrome. Acta Angiol. 2015, 21, 140–145. [Google Scholar] [CrossRef]
- Olinic, D.M.; Spinu, M.; Olinic, M.; Homorodean, C.; Tataru, D.A.; Liew, A.; Schernthaner, G.H.; Stanek, A.; Fowkes, G.; Catalano, M. Epidemiology of peripheral artery disease in Europe: VAS educational paper. Int. Angiol. 2018, 37, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Lepäntalo, M.; Apelqvist, J.; Setacci, C.; Ricco, J.B.; De Donato, G.; Becker, F.; Robert-Ebadi, H.; Cao, P.; Eckstein, H.H.; De Rango, P.; et al. Chapter V: Diabetic foot. Eur. J. Vasc. Endovasc. Surg. 2011, 42, S60–S74. [Google Scholar] [CrossRef]
- Sturt, J.; Hearnshaw, H.; Wakelin, M. Validity and reliability of the DMSES UK: A measure of self-efficacy for type 2 diabetes self-management. Prim. Heal. Care Res. Dev. 2010, 11, 374–381. [Google Scholar] [CrossRef]
- Tamir, O.; Wainstein, J.; Abadi-Korek, I.; Horowitz, E.; Shemer, J. The patient-perceived difficulty in diabetes treatment (PDDT) scale identifies barriers to care. Diabetes Metab. Res. Rev. 2012, 28, 246–251. [Google Scholar] [CrossRef]
- Irvine, A.A.; Saunders, J.T.; Blank, M.B.; Carter, W.R. Validation of scale measuring environmental barriers to diabetes-regimen adherence. Diabetes Care 1990, 13, 705–711. [Google Scholar] [CrossRef] [PubMed]
- Meadows, K.; Steen, N.; McColl, E.; Eccles, M.; Shiels, C.; Hewison, J.; Hutchinson, A. The Diabetes Health Profile (DHP): A new instrument for assessing the psychosocial profile of insulin requiring patients—Development and psychometric evaluation. Qual. Life Res. 1996, 5, 242–254. [Google Scholar] [CrossRef] [PubMed]
- Polonsky, W.H.; Anderson, B.J.; Lohrer, P.A.; Welch, G.; Jacobson, A.M.; Aponte, J.E.; Schwartz, C.E. Assessment of diabetes-related distress. Diabetes Care 1995, 18, 754–760. [Google Scholar] [CrossRef] [PubMed]
- Toobert, D.J.; Hampson, S.E.; Glasgow, R.E. The summary of diabetes self-care activities measure: Results from 7 studies and a revised scale. Diabetes Care 2000, 23, 943–950. [Google Scholar] [CrossRef] [PubMed]
- Stetson, B.; Schlundt, D.; Rothschild, C.; Floyd, J.E.; Rogers, W.; Mokshagundam, S.P. Development and validation of The Personal Diabetes Questionnaire (PDQ): A measure of diabetes self-care behaviors, perceptions and barriers. Diabetes Res. Clin. Pract. 2011, 91, 321–332. [Google Scholar] [CrossRef] [PubMed]
- Caro-Bautista, J.; Martín-Santos, F.J.; Morales-Asencio, J.M. Systematic review of the psychometric properties and theoretical grounding of instruments evaluating self-care in people with type 2 Diabetes Mellitus. J. Adv. Nurs. 2014, 70, 1209–1227. [Google Scholar] [CrossRef] [PubMed]
- Jia, Y.; Huang, H.; Gagnier, J.J. A systematic review of measurement properties of patient-reported outcome measures for use in patients with foot or ankle diseases. Qual. Life Res. 2017, 26, 1969–2010. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef]
- Terwee, C.B.; Jansma, E.P.; Riphagen, I.I.; De Vet, H.C.W. Development of a methodological PubMed search filter for finding studies on measurement properties of measurement instruments. Qual. Life Res. 2009, 18, 1115–1123. [Google Scholar] [CrossRef] [Green Version]
- Prinsen, C.A.C.; Mokkink, L.B.; Bouter, L.M.; Alonso, J.; Patrick, D.L.; de Vet, H.C.W.; Terwee, C.B. COSMIN guideline for systematic reviews of patient-reported outcome measures. Qual. Life Res. 2018, 27, 1147–1157. [Google Scholar] [CrossRef] [Green Version]
- Mokkink, L.B.; Terwee, C.B.; Patrick, D.L.; Alonso, J.; Stratford, P.W.; Knol, D.L.; Bouter, L.M.; De Vet, H.C.W. The COSMIN checklist for assessing the methodological quality of studies on measurement properties of health status measurement instruments: An international Delphi study. Qual. Life Res. 2010, 19, 539–549. [Google Scholar] [CrossRef] [PubMed]
- Terwee, C.B.; Mokkink, L.B.; Knol, D.L.; Ostelo, R.W.J.G.; Bouter, L.M.; De Vet, H.C.W. Rating the methodological quality in systematic reviews of studies on measurement properties: A scoring system for the COSMIN checklist. Qual. Life Res. 2012, 21, 651–657. [Google Scholar] [CrossRef] [PubMed]
- Terwee, C.B.; Bot, S.D.M.; de Boer, M.R.; van der Windt, D.A.W.M.; Knol, D.L.; Dekker, J.; Bouter, L.M.; de Vet, H.C.W. Quality criteria were proposed for measurement properties of health status questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Vileikyte, L.; Peyrot, M.; Bundy, C.; Rubin, R.R.; Leventhal, H.; Mora, P.; Shaw, J.E.; Baker, P.; Boulton, A.J. The Development and Validation of a Neuropathy- and Foot Ulcer—Specific. Diabetes Care 2003, 26, 2549–2555. [Google Scholar] [CrossRef] [PubMed]
- Victorson, D.; Cavazos, J.E.; Holmes, G.L.; Reder, A.T.; Wojna, V.; Nowinski, C.; Miller, D.; Buono, S.; Mueller, A.; Moy, C.; et al. Validity of the Neurology Quality-of-Life (Neuro-QoL) measurement system in adult epilepsy. Epilepsy Behav. 2015, 31, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Xie, G.; Chen, L.; Yang, S.; Tao, J.; Chan, C.C.H.; Heinemann, A.W.; Cella, D.; Lai, J.S.; Correia, H.; Wong, A.W.K. Simplified Chinese translation of 13 adult item banks from the Quality of Life in Neurological Disorders (Neuro-QoL). BMC Health Serv. Res. 2018, 18, 825. [Google Scholar] [CrossRef] [PubMed]
- Xavier, A.T.; Foss, M.C.; Marques Junior, W.; dos Santos, C.B.; Onofre, P.T.B.N.; Pace, A.E. Cultural adaptation and validation of the Neuropathy- and Foot Ulcer—Specific Quality of Life instrument (NeuroQol) for Brazilian Portuguese—Phase 1. Rev. Lat. Am. Enfermagem 2011, 19, 1352–1361. [Google Scholar] [CrossRef] [PubMed]
- Bann, C.M.; Fehnel, S.E.; Gagnon, D.D. Development and Validation of the Diabetic Foot Ulcer Scale-Short Form (DFS-SF). Pharmacoeconomics 2003, 21, 1277–1290. [Google Scholar] [CrossRef] [PubMed]
- Kontodimopoulos, N.; Veniou, A.; Tentolouris, N.; Niakas, D. Validity and reliability of the Greek version of the Diabetic Foot Ulcer Scale—Short Form (DFS-SF). Hormones 2016, 15, 394–403. [Google Scholar] [CrossRef]
- Macioch, T.; Sobol, E.; Krakowiecki, A.; Mrozikiewicz-Rakowska, B.; Kasprowicz, M.; Hermanowski, T. Health related quality of life in patients with diabetic foot ulceration—Translation and Polish adaptation of Diabetic Foot Ulcer Scale short form. Health Qual. Life Outcomes 2017, 15, 1–8. [Google Scholar] [CrossRef]
- Chin, Y.F.; Huang, T.T. Development and validation of a diabetes foot self-care behavior scale. J. Nurs. Res. 2013, 21, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Price, P.; Harding, K. Cardiff wound impact schedule: The development of a condition-specific questionnaire to assess health-related quality of life in patients with chronic wounds of the lower limb. Int. Wound J. 2004, 1, 10–17. [Google Scholar] [CrossRef]
- Jaksa, J.P.; Mahoney, L.J. Quality of life in patients with diabetic foot ulcers: Validation of the Cardiff Wound Impact Schedule in a Canadian population. Int. Wound J. 2010, 7, 502–507. [Google Scholar] [CrossRef] [PubMed]
- Kateel, R.; Augustine, A.J.; Ullal, S.; Prabhu, S.; Bhat, R.; Adhikari, P. Development and validation of health related quality of life questionnaire (Indian scenario) in diabetic foot ulcer patients. Diabetes Metab. Syndr. Clin. Res. Rev. 2017, 11, S651–S653. [Google Scholar] [CrossRef] [PubMed]
- Fagerdahl, A.M.; Boström, L.; Ulfvarson, J.; Bergström, G.; Ottosson, C. Translation and validation of the wound-specific quality of life instrument Cardiff Wound Impact Schedule in a Swedish population. Scand. J. Caring Sci. 2014, 28, 398–404. [Google Scholar] [CrossRef] [PubMed]
- Dhawan, V.; Spratt, K.F.; Pinzur, M.S.; Baumhauer, J.; Rudicel, S.; Saltzman, C.L. Reliability of AOFAS diabetic foot questionnaire in Charcot arthropathy: Stability, internal consistency, and measurable difference. Foot Ankle Int. 2005, 26, 717–731. [Google Scholar] [CrossRef] [PubMed]
- Van Lieshout, E.M.M.; De Boer, A.S.; Meuffels, D.E.; Den Hoed, P.T.; Van Der Vlies, C.H.; Tuinebreijer, W.E.; Verhofstad, M.H.J. American Orthopaedic Foot and Ankle Society (AOFAS) Ankle-Hindfoot Score: A study protocol for the translation and validation of the Dutch language version. BMJ Open 2017, 7, e012884. [Google Scholar] [CrossRef] [PubMed]
- Kostuj, T.; Krummenauer, F.; Schaper, K.; Stief, F.; Zettersten, K.; Baums, M.H.; Meurer, A.; Lieske, S. Analysis of agreement between the German translation of the American Foot and Ankle Society’s Ankle and Hindfoot Scale (AOFAS-AHS) and the Foot Function Index in its validated German translation by Naal et al. (FFI-D). Arch. Orthop. Trauma Surg. 2014, 134, 1205–1210. [Google Scholar] [CrossRef]
- Rodrigues, R.C.; Masiero, D.; Mizusaki, J.M.; Imoto, A.M.; Peccin, M.S.; Cohen, M.; Alloza, J.F.M. Translation, Cultural Adaptation and Validation of the “American Orthopaedic Foot and Ankle Society’s (Aofas) Ankle-Hindfoot Scale”. Acta Ortop. Bras. 2008, 16, 107–111. [Google Scholar] [CrossRef]
- Sayyed-Hosseinian, S.H.; Hassankhani, G.G.; Bagheri, F.; Alavi, N.; Shojaie, B.; Mousavian, A. Validation of the Persian Version of the American Orthopedic Foot and Ankle Society Score (AOFAS) Questionnaire. Arch. Bone Jt. Surg. 2018, 233, 233–239. [Google Scholar]
- Analay Akbaba, Y.; Celik, D.; Ogut, R.T. (Trans.) Cross-Cultural Adaptation, Reliability, and Validity of Turkish Version of the American Orthopaedic Foot and Ankle Society Ankle-Hindfoot Scale. J. Foot Ankle Surg. 2016, 55, 1139–1142. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.L.; Hutt, D.M.; Wukich, D.K. Validity of the Foot and Ankle Ability Measure (FAAM) in Diabetes Mellitus. Foot Ankle Int. 2009, 30, 297–302. [Google Scholar] [CrossRef] [PubMed]
- Moreira, T.S.; Magalhães, L.D.C.; Silva, R.D.; Martin, R.R.L.; Resende, M.A. Translation, cross-cultural adaptation and validity of the Brazilian version of the Foot and Ankle Ability Measure questionnaire. Disabil. Rehabil. 2016, 38, 2479–2490. [Google Scholar] [CrossRef] [PubMed]
- González-Sánchez, M.; Li, G.Z.; Ruiz Muñoz, M.; Cuesta-Vargas, A.I. Foot and ankle ability measure to measure functional limitations in patients with foot and ankle disorders: A Chinese cross-cultural adaptation and validation. Disabil. Rehabil. 2017, 39, 2182–2189. [Google Scholar] [CrossRef] [PubMed]
- Weel, H.; Zwiers, R.; Azim, D.; Sierevelt, I.N.; Haverkamp, D.; van Dijk, C.N.; Kerkhoffs, G.M.M.J. Validity and reliability of a Dutch version of the Foot and Ankle Ability Measure. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 1348–1354. [Google Scholar] [CrossRef] [PubMed]
- Borloz, S.; Crevoisier, X.; Deriaz, O.; Ballabeni, P.; Martin, R.L.; Luthi, F. Evidence for validity and reliability of a french version of the FAAM. BMC Musculoskelet. Disord. 2011, 12, 40. [Google Scholar] [CrossRef]
- Bizjak, G. Report Information from ProQuest. Art Persuas. 2014. [Google Scholar] [CrossRef]
- Sartorio, F.; Vercelli, S.; Bravini, E.; Bargeri, S.; Moroso, M.; Plebani, G.; Ferriero, G. Foot and ankle ability measure: Cross-cultural translation and validation of the Italian version of the ADL module (FAAM-I/ADL). Med. Lav. 2014, 105, 357–365. [Google Scholar]
- Uematsu, D.; Suzuki, H.; Sasaki, S.; Nagano, Y.; Shinozuka, N.; Sunagawa, N.; Fukubayashi, T. Evidence of validity for the Japanese version of the foot and ankle ability measure. J. Athl. Train. 2015, 50, 65–70. [Google Scholar] [CrossRef]
- Mazaheri, M.; Salavati, M.; Negahban, H.; Sohani, S.M.; Taghizadeh, F.; Feizi, A.; Karimi, A.; Parnianpour, M. Reliability and validity of the Persian version of Foot and Ankle Ability Measure (FAAM) to measure functional limitations in patients with foot and ankle disorders. Osteoarthr. Cartil. 2010, 18, 755–759. [Google Scholar] [CrossRef] [Green Version]
- Arunakul, M.; Arunakul, P.; Suesiritumrong, C.; Angthong, C.; Chernchujit, B. Validity and Reliability of Thai Version of the Foot and Ankle Ability Measure (FAAM) Subjective Form. J. Med. Assoc. Thai. 2015, 98, 561–567. [Google Scholar] [PubMed]
- Çelik, D.; Malkoç, M.; Martin, R.R. Evidence for reliability, validity and responsiveness of Turkish Foot and Ankle Ability Measure (FAAM). Rheumatol. Int. 2016, 36, 1469–1476. [Google Scholar] [CrossRef] [PubMed]
- Cervera-Garvi, P.; Ortega-Avila, A.B.; Morales-Asencio, J.M.; Cervera-Marin, J.A.; Martin, R.R.; Gijon-Nogueron, G. Cross-cultural adaptation and validation of Spanish version of The Foot and Ankle Ability Measures (FAAM-Sp). J. Foot Ankle Res. 2017, 10, 39. [Google Scholar] [CrossRef] [PubMed]
- Bergin, S.M.; Brand, C.A.; Colman, P.G.; Campbell, D.A. A questionnaire for determining prevalence of diabetes related foot disease (Q-DFD): Construction and validation. J. Foot Ankle Res. 2009, 2, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Castillo-Tandazo, W.; Flores-Fortty, A.; Feraud, L.; Tettamanti, D. Spanish translation, cross-cultural adaptation, and validation of the Questionnaire for Diabetes-Related Foot Disease (Q-DFD). Vasc. Health Risk Manag. 2013, 9, 501–508. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.H.; Lin, L.Y.; Cheng, C.P.; Hsu, M.T.; Kao, C.C. The psychometric testing of the diabetes health promotion self-care scale. J. Nurs. Res. 2012, 20, 122–130. [Google Scholar] [CrossRef] [PubMed]
- García-Inzunza, J.A.; Valles-Medina, A.M.; Muñoz, F.A.; Delgadillo-Ramos, G.; Compean-Ortiz, L.G. Validity of the Mexican version of the combined Foot Care Confidence/Foot-Care Behavior scale for diabetes. Rev. Panam. Salud Publ. 2015, 3838, 35–41. [Google Scholar]
- Navarro-Flores, E.; Morales-Asencio, J.M.; Cervera-Marín, J.A.; Labajos-Manzanares, M.T.; Gijon-Nogueron, G. Development, validation and psychometric analysis of the diabetic foot self-care questionnaire of the University of Malaga, Spain (DFSQ-UMA). J. Tissue Viability 2015, 24, 24–34. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, A.F.B.; Laurindo, I.M.M.; Rodrigues, P.T.; Ferraz, M.B.; Kowalski, S.C.; Tanaka, C. Brazilian version of the foot health status questionnaire (FHSQ-BR): Cross-cultural adaptation and evaluation of measurement properties. Clinics 2008, 63, 595–600. [Google Scholar] [CrossRef] [PubMed]
- Cuesta-Vargas, A.; Bennett, P.; Jimenez-Cebrian, A.M.; Labajos-Manzanares, M.T. The psychometric properties of the Spanish version of the Foot Health Status Questionnaire. Qual. Life Res. 2013, 22, 1739–1743. [Google Scholar] [CrossRef]
- Bennett, P.; Patterson, C.; Wearing, S.; Baglioni, T. Development and validation of a questionnaire designed to measure foot-health status. J. Am. Podiatr. Med. Assoc. 1998, 88, 419–428. [Google Scholar] [CrossRef] [PubMed]
- Landorf, K.B.; Keenan, A.M. An evaluation of two foot-specific, health-related quality-of-life measuring instruments. Foot Ankle Int. 2002, 23, 538–546. [Google Scholar] [CrossRef] [PubMed]
- Bennett, P.J.; Patterson, C.; Dunne, M.P. Health-related quality of life following podiatric surgery. J. Am. Podiatr. Med. Assoc. 2001, 91, 164–173. [Google Scholar] [CrossRef] [PubMed]
- Walmsley, S.; Williams, A.E.; Ravey, M.; Graham, A. The rheumatoid foot: A systematic literature review of patient-reported outcome measures. J. Foot Ankle Res. 2010, 3, 12. [Google Scholar] [CrossRef]
- Sierevelt, I.N.; Zwiers, R.; Schats, W.; Haverkamp, D.; Terwee, C.B.; Nolte, P.A.; Kerkhoffs, G.M.M.J. Measurement properties of the most commonly used Foot- and Ankle-Specific Questionnaires: The FFI, FAOS and FAAM. A systematic review. Knee Surg. Sport. Traumatol. Arthrosc. 2018, 26, 2059–2073. [Google Scholar] [CrossRef] [PubMed]
- Van Der Leeden, M.; Steultjens, M.P.M.; Terwee, C.B.; Rosenbaum, D.; Turner, D.; Woodburn, J.; Dekker, J. A systematic review of instruments measuring foot function, foot pain, and foot-related disability in patients with rheumatoid arthritis. Arthritis Care Res. 2008, 59, 1257–1269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenhalgh, J. The applications of PROs in clinical practice: What are they, do they work, and why? Qual. Life Res. 2009, 18, 115–123. [Google Scholar] [CrossRef]


{kind=link}
| Acronym | Full Title | Author | Country |
|---|---|---|---|
| NeuroQol | Neuropathy Quality of Life Instrument | Loretta Vileikyte et al. | UK and USA |
| DFS-SF | Diabetic Foot Ulcer Scale–Short Form | Carla M. Bann et al. | USA |
| CWIS | Cardiff Wound Impact Schedule | Patricia Price and Keith Harding | UK |
| AOFAS-DFQ | American Orthopaedic Foot and Ankle Society | Vibhu Dhawan et al. | USA |
| FAAM | Foot and Ankle Ability Measure | RobRoy L. Martin et al. | USA |
| Q-DFD | Questionnaire for Diabetes Related Foot Disease | Shan M Bergin et al. | Australia |
| DHPSC | Diabetes Health Promotion Self-Care Scale | Ruey-Hsia Wang et al. | Taiwan |
| FCBS | Foot Self-Care Behavior Scale | Yen-Fan Chin and Tzu-Ting Huang | Taiwan |
| DFSQ-UMA | Diabetic Foot Self-care Questionnaire of University of Malaga | Emmanuel Navarro et al. | Spain |
| HRQLQDFU | Health Related Quality of Life Questionnaire in Diabetic Foot Ulcer Patients | Ramya Kateel et al. | India |
| FHSQ | Foot Health Status Questionnaire | Patricia Palomo-López et al. | Spain |
| Year | Dimensions and Number of Items | Population Used for Validation | Psychometric Properties | Cross-Cultural Adaptation | |
|---|---|---|---|---|---|
| NeuroQoL [25] | 2003 | 6 dimensions: painful symptoms and paresthesia, symptoms of reduced/lost feeling in the feet, diffuse sensory motor symptoms, limitations in daily activities, interpersonal problems and emotional burden 28 items | 418 patients with diabetic peripheral neuropathy n: 296 male (70.8%) n: 122 female (29.2%) Mean age: 61.76 years | - Internal consistency: Cronbach’s alpha (0.86–0.95) | Spanish [26], Chinese [27], Brazilian [28] |
| DFS-SF [29] | 2003 | 6 dimensions: leisure, physical health, dependence/daily life, negative emotions, worried about ulcers/feet, bothered by ulcer care 29 items | 218 (diabetic with foot ulcer) and 108 (placebo) patients: n: 241male (74%) n: 85 female (26%) Age 27–87 years | - Internal consistency: Cronbach’s alpha (0.74–0.94) | Greek [30], Polish [31], Chinese [32] |
| CWIS [33] | 2004 | 3 dimensions: physical symptoms and daily living, social life and well-being 26 items + overall and individual rating of HRQoL | 87 with leg ulceration and 48 with diabetic foot ulceration n: 74 male (55%) n: 61 female (45%) Mean age 65.9 years (43–85.5) | Canadian [34], Chinese [34], French, German, English (US) [34], Sinhala [35], Swedish [36], Brazilian [34] | |
| AOFAS-DFQ [37] | 2005 | 6 dimensions: general health, care, worry, sleep, emotion and physicality. | 57 patients diagnosed with Charcot arthropathy n: 25 male (57.8%) n: 33 female (42.2%) Mean age: 57.5 years (37.7–80.6) | - Test-retest 0.77 | Dutch [38], German [39], Italian [40], Persian [41], Turkish [42] |
| FAAM [43] | 2009 | 2 dimensions: activities of daily living and sports 21 + 8 items | 83 patients with diabetes and foot and ankle problems n: 45 male (54%) n: 38 female (46%) Mean age: 60.3 years (21–93) | Brazilian [44], Chinese [45], Dutch [46], French [47], German [48], Italian [49], Japanese [50], Persian [51], Thai [52], Turkish [53], Spanish [54] | |
| Q-DFD [55] | 2009 | 5 dimensions: peripheral neuropathy, peripheral vasculopathy, foot ulceration, amputation and foot deformity 12 items | 31 patients with diabetes n:15 male (48%) n: 16 female (52%) Mean age: 64 years (45–80) | Spanish [56] | |
| DHPSC [57] | 2012 | 7 dimensions: interpersonal relationships, diet, blood glucose self-monitoring, personal health responsibility, exercise, adherence to the recommended regimens, and foot care 26 items | 489 patients with Type II diabetes n: 243 male (49.7%) n: 246 female (50.3%) Mean age: 58.1 years | - Internal consistency: Cronbach’s alpha 0.88 - Reliability: ICC 0.94 - Floor and ceiling effects: 4.59% | |
| FCBS [58] | 2013 | 1 dimension 7 items | 295 patients with diabetes n: 151 male (51.2%) n: 144 female (48.8%) Mean age: 66.93 years | -Internal consistency: Cronbach’s alpha 0.73 - Reliability: test-retest 0.92 | Mexican [58] |
| DFSQ-UMA [59] | 2015 | 3 dimensions: self-care, foot care, and footwear and socks 16 items | 209 with diabetes (48 type I and 161 type II) n: 101 male (48%) n: 108 female (52%) Mean age: 57.78 years (male) and 64.66 years (female) | - Internal consistency: Chronbach’s alpha 0.89 - Reliability: ICC 0.89–0.92 | |
| HRQLQDFU [35] | 2017 | 6 dimensions: physical health, daily activity, social, physical symptoms, emotional and financial 20 items | 10 patients with diabetic foot ulcers n: 7 male (70%) n: 3 female (30%) Mean age: 65 years | - Internal consistency: Cronbach’s alpha 0.86 | |
| FHSQ [5] | 2018 | 8 dimensions: foot pain, foot function, footwear, general foot health, general health, social capacity, physical activity, and vigour 17 items | 62 patients (31 type I and 31 type II) n:22 male (35.5%) n: 40 females (64.5%) Mean age: 59 years (30–86) | - Internal consistency: Cronbach’s alpha 0.89–0.95 - Reliability: ICC 0.74–0.92 | Brazilian [60], Spanish [61] |
| Content Validity | Internal Consistency | Criterion Validity | Construct Validity | Reproduci bility Agreement | Reproduci bility Reliability | Responsiveness | Floor and Ceiling Effects | Interpretability | Final Assessment | |
|---|---|---|---|---|---|---|---|---|---|---|
| NeuroQol | + | + | - | - | ? | ? | 0 | - | ? | |
| DFS-SF | + | + | - | ? | ? | - | ? | 0 | 0 | |
| CWIS | + | - | - | - | ? | ? | ? | 0 | ? | |
| AOFAS-DFQ | + | - | ? | ? | 0 | + | ? | ? | ? | |
| FAAM | + | 0 | - | ? | 0 | 0 | 0 | 0 | ? | |
| Q-DFD | + | 0 | 0 | ? | ? | - | 0 | 0 | 0 | |
| DHPSC | + | + | - | - | 0 | + | 0 | + | ? | √ |
| FCBS | + | + | - | - | 0 | + | ? | 0 | ? | |
| DFSQ-UMA | + | + | - | - | ? | + | 0 | ? | ? | |
| HRQLQDFU | + | + | 0 | 0 | 0 | ? | 0 | 0 | 0 | |
| FHSQ | + | + | 0 | ? | 0 | + | 0 | 0 | ? |
| Structural Validity | Internal Consistency | Reliability | Measurement Error | Hypothesis Testing for Construct Validity | Cross-cultural Validity | Criterion Validity | Responsiveness | |
|---|---|---|---|---|---|---|---|---|
| NeuroQol | ? | + | ? | ? | + | - | - | + |
| DFS-SF | ? | + | - | ? | + | ? | - | + |
| CWIS | ? | + | ? | ? | + | ? | - | + |
| AOFAS-DFQ | ? | - | + | ? | ? | + | ? | ? |
| FAAM | - | ? | ? | ? | + | + | - | + |
| Q-DFD | - | ? | - | ? | ? | ? | ? | ? |
| DHPSC | ? | + | + | ? | + | ? | - | + |
| FCBS | - | + | + | ? | + | - | - | + |
| DFSQ-UMA | ? | + | + | ? | ? | - | - | ? |
| HRQLQDFU | - | + | ? | ? | ? | ? | ? | ? |
| FHSQ | - | + | + | ? | + | + | ? | + |
| BOX AInternal Consistency | BOX BReliability | BOX CMeasurement Error | BOX DContent Validity | BOX EStructural Validity | BOX FHypothesis Testing | BOX GCross-cultural Validity | BOX HCriterion Validity | BOX IResponsiveness | |
|---|---|---|---|---|---|---|---|---|---|
| DHPSC | EXCELLENT | POOR | POOR | EXCELLENT | POOR | FAIR | - | POOR | POOR |
| FCBS | EXCELLENT | GOOD | POOR | EXCELLENT | POOR | FAIR | - | POOR | POOR |
| FHSQ | FAIR | POOR | POOR | POOR | POOR | POOR | - | POOR | POOR |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ortega-Avila, A.B.; Cervera-Garvi, P.; Ramos-Petersen, L.; Chicharro-Luna, E.; Gijon-Nogueron, G. Patient-Reported Outcome Measures for Patients with Diabetes Mellitus Associated with Foot and Ankle Pathologies: A Systematic Review. J. Clin. Med. 2019, 8, 146. https://doi.org/10.3390/jcm8020146
Ortega-Avila AB, Cervera-Garvi P, Ramos-Petersen L, Chicharro-Luna E, Gijon-Nogueron G. Patient-Reported Outcome Measures for Patients with Diabetes Mellitus Associated with Foot and Ankle Pathologies: A Systematic Review. Journal of Clinical Medicine. 2019; 8(2):146. https://doi.org/10.3390/jcm8020146
Chicago/Turabian StyleOrtega-Avila, Ana Belen, Pablo Cervera-Garvi, Laura Ramos-Petersen, Esther Chicharro-Luna, and Gabriel Gijon-Nogueron. 2019. "Patient-Reported Outcome Measures for Patients with Diabetes Mellitus Associated with Foot and Ankle Pathologies: A Systematic Review" Journal of Clinical Medicine 8, no. 2: 146. https://doi.org/10.3390/jcm8020146