
Does EMDR Therapy Have an Effect on Memories of Emotional Abuse, Neglect and Other Types of Adverse Events in Patients with a Personality Disorder? Preliminary Data


Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Assessment
2.2.1. General Assessment
2.2.2. Memories of Adverse Events
2.3. Outcome Measures
2.3.1. Psychological Symptoms
2.3.2. Psychological Functioning
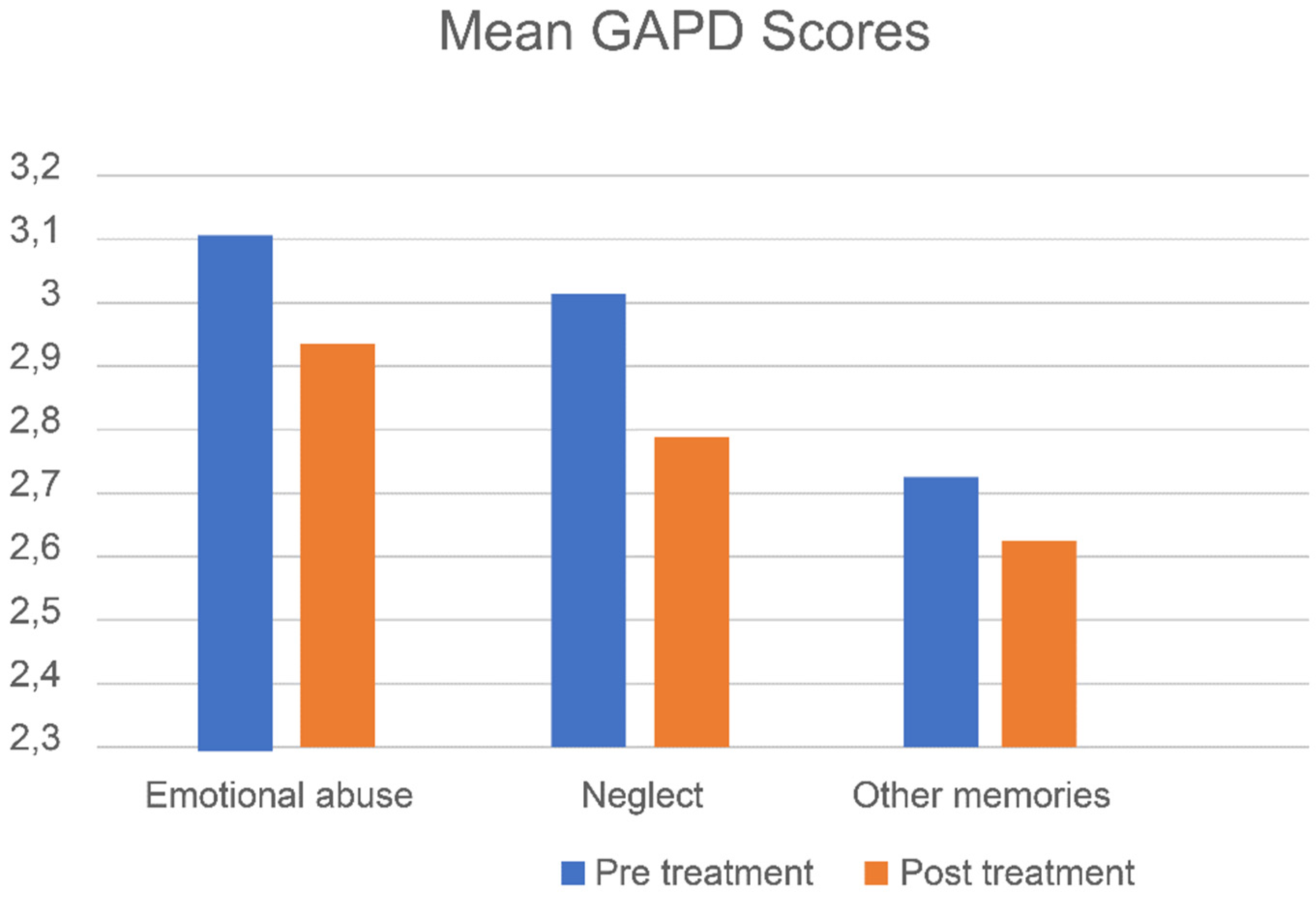
2.3.3. Personality Dysfunctioning
2.4. Treatment and Treatment Training
3. Statistical Analysis
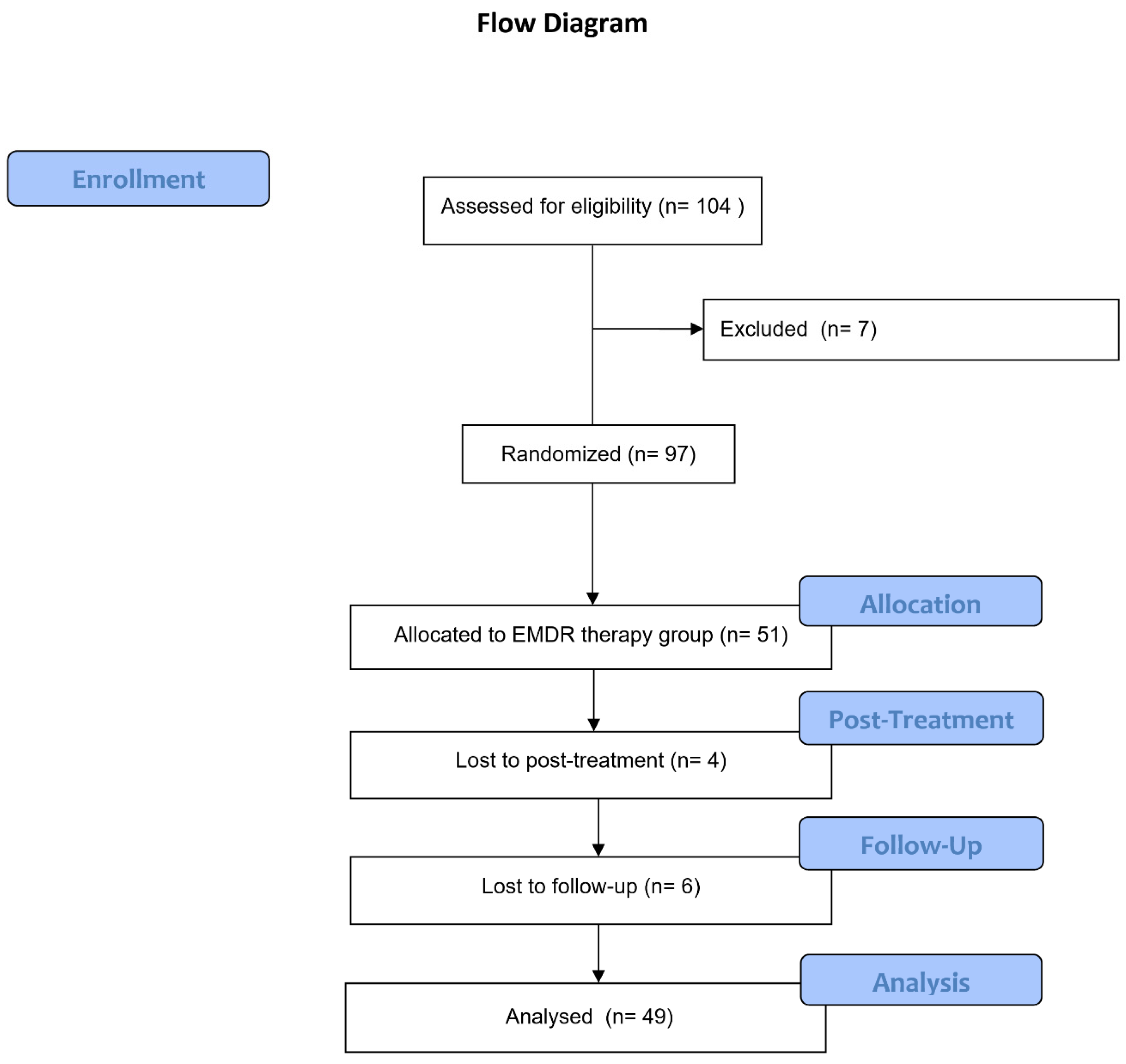
4. Results
4.1. Sample Characteristics and Types of Memories
4.2. Effects of Treatment
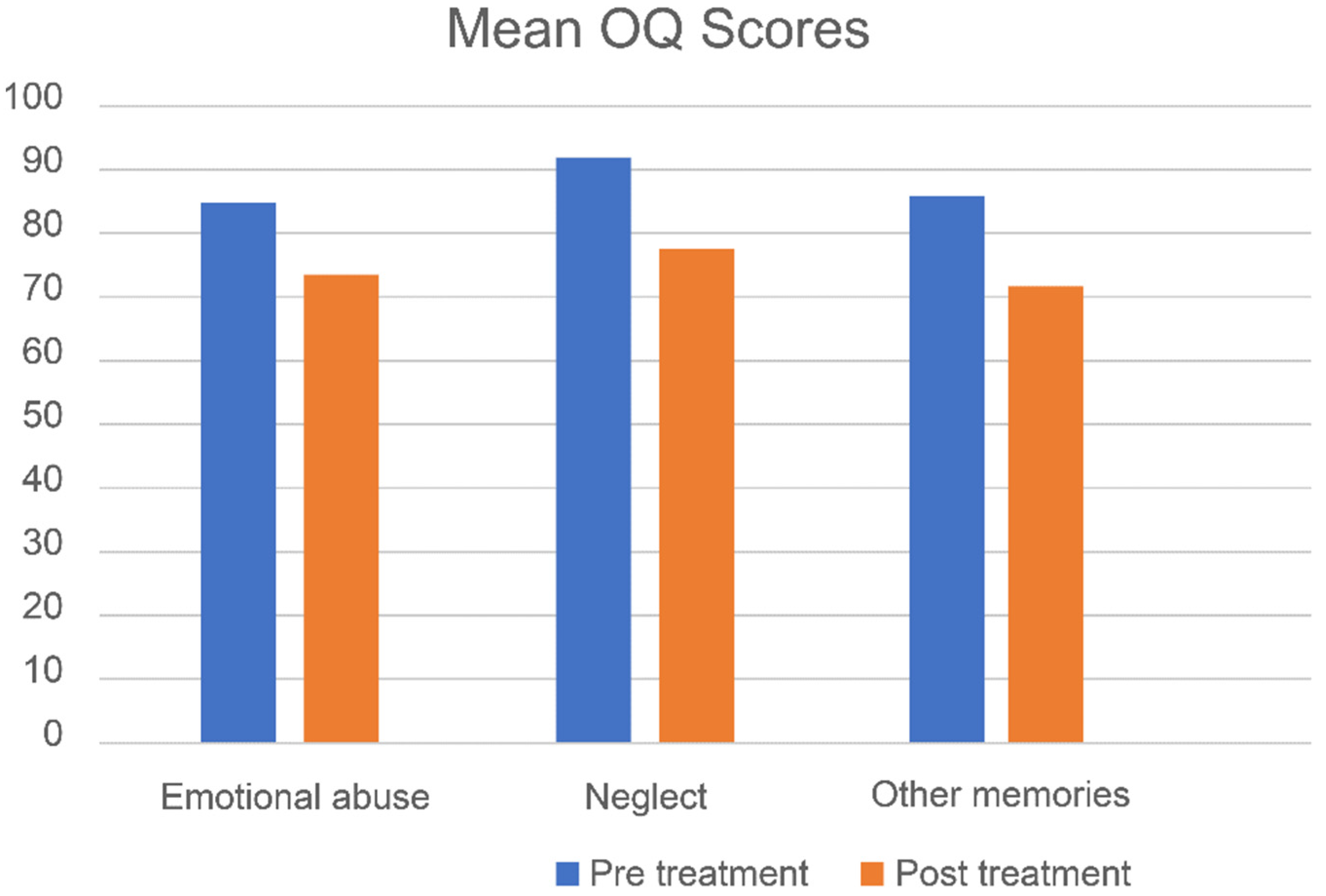
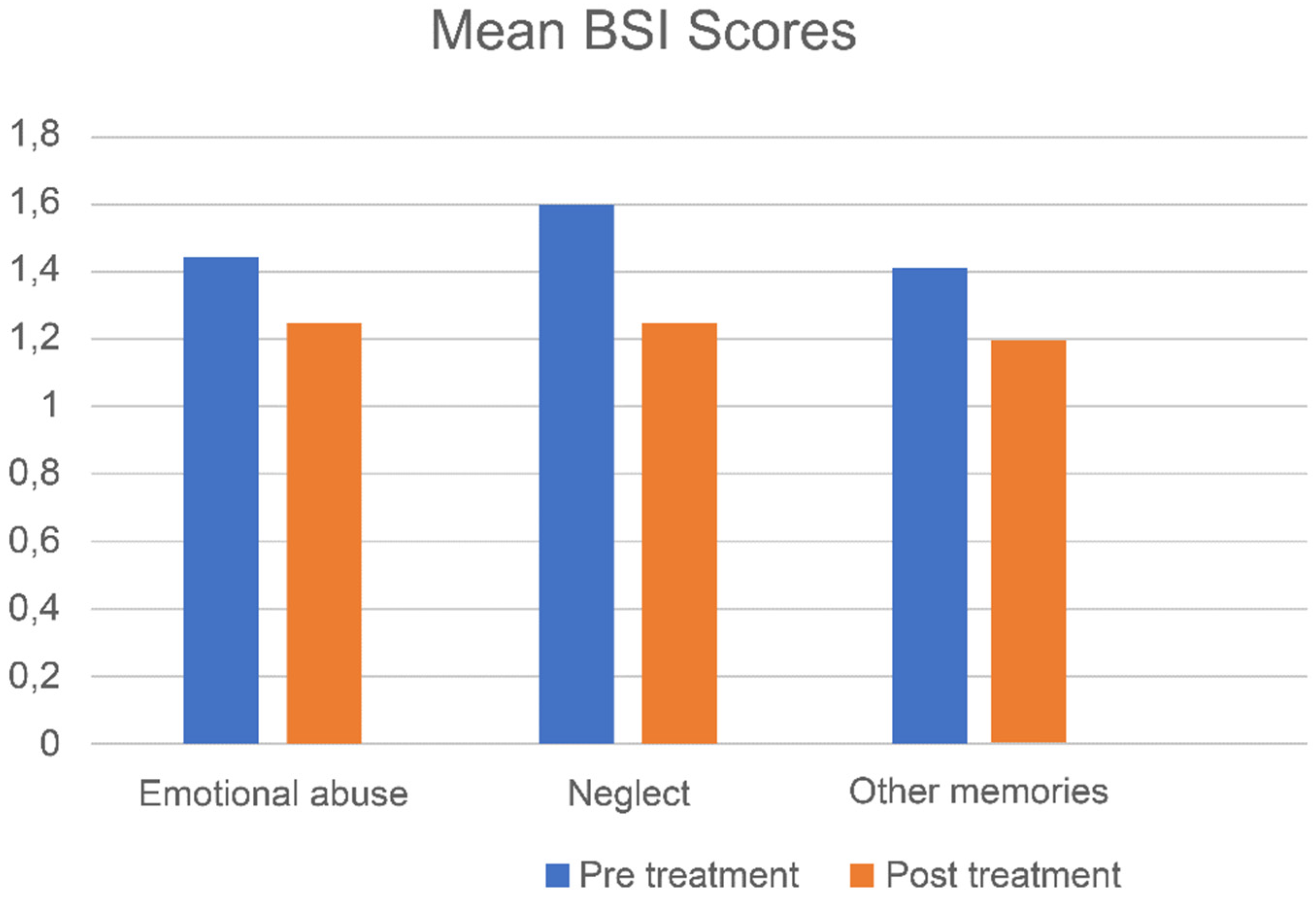
4.2.1. Overall Treatment Effects
4.2.2. Memories of Emotional Abuse
4.2.3. Memories of Emotional Neglect
4.2.4. Other Adverse Memories
4.2.5. Differences among the Three Memory Types
4.2.6. Results at 3-Month Follow-Up
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lobbestael, J.; Arntz, A.; Bernstein, D.P. Disentangling the relationship between different types of childhood maltreatment and personality disorders. J. Personal. Disord. 2010, 24, 285–295. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.G.; Cohen, P.; Chen, H.; Kasen, S.; Brook, J.S. Parenting behaviors associated with risk for offspring personality disorder during adulthood. Arch. Gen. Psychiatry 2006, 63, 579–587. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.G.; Smailes, E.M.; Cohen, P.; Brown, J.; Bernstein, D.P. Associations between four types of childhood neglect and personality disorder symptoms during adolescence and early adulthood: Findings of a community-based longitudinal study. J. Personal. Disord. 2000, 14, 171–187. [Google Scholar] [CrossRef]
- Grover, K.E.; Carpenter, L.L.; Price, L.H.; Gagne, G.G.; Mello, A.F.; Mello, M.F.; Tyrka, A.R. The relationship between childhood abuse and adult personality disorder symptoms. J. Personal. Disord. 2007, 21, 442–447. [Google Scholar] [CrossRef] [Green Version]
- Burns, E.E.; Jackson, J.L.; Harding, H.G. Child maltreatment, emotion regulation, and posttraumatic stress: The Impact of Emotional Abuse. J. Aggress. Maltreatment Trauma 2010, 19, 801–819. [Google Scholar] [CrossRef]
- Niemantsverdriet, M.B.A.; Slotema, C.W.; Blom, J.D.; Franken, I.H.; Hoek, H.W.; Sommer, I.E.C.; van der Gaag, M. Hallucinations in borderline personality disorder: Prevalence, characteristics and associations with comorbid symptoms and disorders. Sci. Rep. 2017, 7, 13920. [Google Scholar] [CrossRef] [Green Version]
- Voestermans, D.; Eikelenboom, M.; Rullmann, J.; Wolters-Geerdink, M.; Draijer, N.; Smit, J.H.; Thomaes, K.; van Marle, H.J. The Association Between Childhood Trauma and Attachment Functioning in Patients With Personality Disorders. J. Personal. Disord. 2020, 35, 554–572. [Google Scholar] [CrossRef] [Green Version]
- Seo, J.; Choi, J.Y. Social defeat as a mediator of the relationship between childhood trauma and paranoid ideation. Psychiatry Res. 2018, 260, 48–52. [Google Scholar] [CrossRef] [PubMed]
- Kuo, J.R.; Khoury, J.E.; Metcalfe, R.; Fitzpatrick, S.; Goodwill, A. An examination of the relationship between childhood emotional abuse and borderline personality disorder features: The role of difficulties with emotion regulation. Child Abus. Negl. 2015, 39, 147–155. [Google Scholar]
- Bovin, M.J.; Wolf, E.J.; Resick, P.A. Longitudinal associations between posttraumatic stress disorder severity and personality disorder features among female rape survivors. Front. Psychiatry 2017, 8, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Markowitz, J.C.; Petkova, E.; Biyanova, T.; Ding, K.; Suh, E.J.; Neria, Y. Exploring personality diagnosis stability following acute psychotherapy for chronic posttraumatic stress disorder. Depress. Anxiety 2015, 32, 919–926. [Google Scholar] [CrossRef] [Green Version]
- Slotema, C.W.; Wilhelmus, B.; Arends, L.R.; Franken, I.H. Psychotherapy for posttraumatic stress disorder in patients with borderline personality disorder: A systematic review and meta-analysis of its efficacy and safety. Eur. J. Psychotraumatol. 2020, 11, 1796188. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Pub.: Arlington, VA, USA, 2013. [Google Scholar]
- Staring, A.B.P.; Van den Berg, D.P.G.; Cath, D.C.; Schoorl, M.; Engelhard, I.M.; Korrelboom, C.W. Self-esteem treatment in anxiety: A randomized controlled crossover trial of Eye Movement Desensitization and Reprocessing (EMDR) versus Competitive Memory Training (COMET) in patients with anxiety disorders. Behav. Res. Ther. 2016, 82, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Littel, M.; Remijn, M.; Tinga, A.M.; Engelhard, I.M.; van den Hout, M.A. Stress enhances the memory-degrading effects of eye movements on emotionally neutral memories. Clin. Psychol. Sci. 2017, 5, 316–324. [Google Scholar] [CrossRef]
- van den Hout, M.A.; Engelhard, I.M. How does EMDR work? J. Exp. Psychopathol. 2012, 3, 724–738. [Google Scholar] [CrossRef] [Green Version]
- Battle, C.L.; Shea, M.T.; Johnson, D.M.; Yen, S.; Zlotnick, C.; Zanarini, M.C.; Sanislow, C.A.; Skodol, A.E.; Gunderson, J.G.; Grilo, C.M.; et al. Childhood maltreatment associated with adult personality disorders: Findings from the Collaborative Longitudinal Personality Disorders Study. J. Personal. Disord. 2004, 18, 193–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hafkemeijer, L.; de Jongh, A.; van der Palen, J.; Starrenburg, A. Eye movement desensitization and reprocessing (EMDR) in patients with a personality disorder. Eur. J. Psychotraumatol. 2020, 11, 1838777. [Google Scholar] [CrossRef] [PubMed]
- Grossman, F.K.; Spinazzola, J.; Zucker, M.; Hopper, E. Treating adult survivors of childhood emotional abuse and neglect: A new framework. Am. J. Orthopsychiatry 2017, 87, 86. [Google Scholar] [CrossRef]
- First, M.B.; Williams, J.B.; Karg, R.S.; Spitzer, R.L. Structured Clinical Interview for DSM-5 Disorders—Clinical Version (SCID-5-CV); American Psychiatric Association: Arlington, VA, USA, 2016. [Google Scholar]
- Sheehan, D.V.; Lecrubier, Y.; Sheehan, K.H.; Janavs, J.; Weiller, E.; Keskiner, A.; Schinka, J.; Knapp, E.; Sheehan, M.F.; Dunbar, G.C. The validity of the mini international neuropsychiatric interview (MINI) according to the SCID-P and its reliability. Eur. Psychiatry 1997, 12, 232–241. [Google Scholar] [CrossRef]
- De Jongh, A.; Ten Broeke, E.; Meijer, S. Two method approach: A case conceptualization model in the context of EMDR. J. EMDR Pract. Res. 2010, 4, 12–21. [Google Scholar] [CrossRef]
- De Beurs, E.; Zitman, F. De brief symptom inventory (BSI). In De Betrouwbaarheid en Validiteit van een Handzaam Alternatief Voor de SCL-90; Leids Universitair Medisch Centrum: Leiden, The Netherlands, 2005. [Google Scholar]
- Akhavan Abiri, F.; Shairi, M.R. Validity and Reliability of Symptom Checklist-90-Revised (SCL-90-R) and Brief Symptom Inventory-53 (BSI-53). Clin. Psychol. Personal. 2020, 17, 169–195. [Google Scholar]
- Lambert, M.J.; Finch, A.E. The Outcome Questionnaire. In The Use of Psychological Testing for Treatment Planning and Outcomes Assessment, 2nd ed.; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 1999; pp. 831–869. [Google Scholar]
- De Jong, K.; Nugter, M.A.; Polak, M.G.; Wagenborg, J.E.; Spinhoven, P.; Heiser, W.J. The outcome questionnaire (OQ-45) in a Dutch population: A cross-cultural validation. Int. J. Theory Pract. 2007, 14, 288–301. [Google Scholar] [CrossRef]
- Livesley, W.J.V. General Assessment of Personality Disorder (GAPD); Department of Psychiatry, University of British Columbia: Vancouver, BC, Canada, 2006. [Google Scholar]
- Berghuis, H. General Assessment of Personality Disorder (GAPD); Version 2007; Symfora Groep: Amersfoort, The Netherlands, 2007. [Google Scholar]
- Shapiro, F. Eye Movement Desensitization and Reprocessing: Basic Principles, Protocols and Procedures, 3rd ed.; Guilford Press: New York, NY, USA, 2018. [Google Scholar]
- De Jongh, A.; Ten Broeke, E. Handboek EMDR: Een Geprotocolleerde Behandelmethode voor de Gevolgen van Psychotrauma (Handbook EMDR: A Protocolled Treatment for the Consequences of Psychotrauma); Swets & Zeitlinger: Lisse, The Netherlands, 2012. [Google Scholar]
- Ziegler, A. Generalized Estimating Equations, 1st ed.; Springer: New York, NY, USA, 2011. [Google Scholar]
- Lambert, M.J. Bergin and Garfield’s Handbook of Psychotherapy and Behavior Change; John Wiley & Sons: New York, NY, USA, 2013. [Google Scholar]
- Leichsenring, F.; Rabung, S. Long-term psychodynamic psychotherapy in complex mental disorders: Update of a meta-analysis. Br. J. Psychiatry 2011, 199, 15–22. [Google Scholar] [CrossRef] [Green Version]
- de Jongh, A.; Amann, B.L.; Hofmann, A.; Farrell, D.; Lee, C.W. The status of EMDR therapy in the treatment of posttraumatic stress disorder 30 years after its introduction. J. EMDR Pract. Res. 2019, 13, 261–269. [Google Scholar] [CrossRef]
- Doering, S.; Ohlmeier, M.-C.; De Jongh, A.; Hofmann, A.; Bisping, V. Efficacy of a trauma-focused treatment approach for dental phobia: A randomized clinical trial. Eur. J. Oral. Sci. 2013, 121, 584–593. [Google Scholar] [CrossRef] [PubMed]
- Gauhar, Y.W.M. The efficacy of EMDR in the treatment of depression. J. EMDR Pract. Res. 2016, 10, 59–69. [Google Scholar] [CrossRef]
- De Jongh, A.; Ernst, R.; Marques, L.; Hornsveld, H. The impact of eye movements and tones on disturbing memories involving PTSD and other mental disorders. J. Behav. Ther. Exp. Psychiatry 2013, 44, 477–483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gold, S.D.; Marx, B.P.; Soler-Baillo, J.M.; Sloan, D.M. Is life stress more traumatic than traumatic stress? J. Anxiety Disord. 2005, 19, 687–698. [Google Scholar] [CrossRef] [PubMed]
- Mol, S.S.; Arntz, A.; Metsemakers, J.F.; Dinant, G.J.; Vilters-Van Montfort, P.A.; Knottnerus, J.A. Symptoms of post-traumatic stress disorder after non-traumatic events: Evidence from an open population study. Br. J. Psychiatry 2005, 186, 494–499. [Google Scholar] [CrossRef]
- Anders, S.L.; Frazier, P.A.; Frankfurt, S.B. Variations in Criterion A and PTSD rates in a community sample of women. J. Anxiety Disord. 2011, 25, 176–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | EMDR Group |
|---|---|
| Mean age (years) | 33.9 (range 18–64) |
| Gender | |
| Male | 17 (33.3%) |
| Female | 32 (66.7%) |
| Personality cluster | |
| B | 13 (29.4%) |
| C | 20 (32.2%) |
| OS | 16 (31.4%) |
| DSM-5 personality classification | |
| Borderline PD | 12 (25.5%) |
| Avoidant PD | 12 (25.5%) |
| Histrionic PD | - |
| Narcistic PD | - |
| PD OS | 19 (37.3%) |
| Obsessive compulsive PD | 6 (11.8%) |
| Dependent PD | - |
| Types of memories | |
| Emotional abuse | 11 (22.4%) |
| Neglect | 24 (49%) |
| Other memories | 13 (26.5%) |
| Effect Size d at Post-Treatment | Effect Size d from PT to 3 Months FU | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| n | BL Score Mean (SD) | PT Score Mean (SD) | 3-Month Follow-Up Mean (SD) | d | CI Interval | d | CI Interval | p-Value (GEE) of the Difference over Time | |
| Total sample | |||||||||
| OQ-45 | 49 | 87.15 (21.11) | 74.35 (23.86) | 69.07 (27.60) | 0.57 | 0.16–0.97 | 0.20 | −0.19–0.60 | <0.001 |
| BSI | 49 | 1.48 (0.74) | 1.23 (0.67) | 1.06 (0.68) | 0.35 | −0.05–0.75 | 0.25 | −0.15–0.64 | <0.001 |
| Type of memory | |||||||||
| OQ-45 | |||||||||
| Neglect | 24 | 91.61 (17.68) | 77.66 (18.26) | 75.99 (24.24) | 0.78 | 0.18–1.35 | 0.08 | −0.49–0.64 | <0.001 |
| Emotional abuse | 11 | 84.55 (20.39) | 73.27 (17.54) | 63.78 (28.27) | 0.59 | −0.28–1.42 | 0.40 | −0.46–1.23 | 0.005 |
| Other | 13 | 85.31 (20.09) | 72.12 (28.55) | 67.43 (23.59) | 0.53 | −0.26–1.30 | 0.18 | −0.60–0.94 | <0.001 |
| BSI | |||||||||
| Neglect | 24 | 1.58 (0.66) | 1.25 (0.66) | 1.22 (0.76) | 0.52 | −0.06–1.09 | 0.05 | −0.51–0.62 | 0.018 |
| Emotional abuse | 11 | 1.44 (0.71) | 1.25 (0.57) | 0.99 (0.59) | 0.29 | −0.56–1.12 | 0.46 | −0.41–1.29 | <0.001 |
| Other | 13 | 1.41 (0.68) | 1.20 (0.71) | 0.98 (0.63) | 0.31 | −0.47–1.07 | 0.33 | −0.46–1.09 | 0.002 |
| Fixed Effects OQ-45 | Fixed Effects BSI | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Est/Beta | SE | 95% CI | Wald Chi-Square | p | Est/Beta | SE | 95% CI | Wald Chi-Square | p | |
| Intercept | 85.31 | 5.57 | 74.39–96.23 | 234.32 | <0.001 | 1.4 | 0.19 | 1.04–1.79 | 1.78 | <0.001 |
| Neglect | 6.3 | 6.64 | −6.71–19.31 | 0.90 | 0.343 | 0.17 | 0.23 | −0.29–0.63 | 0.53 | 0.465 |
| EA | 0.76 | 8.30 | −17.03–15.50 | 0.08 | 0.927 | 0.03 | 0.29 | −0.53–0.59 | 0.01 | 0.922 |
| Post-treatment | −13.19 | 4.50 | −22.00–4.38 | 8.60 | 0.003 | −0.22 | 0.10 | −0.42–0.01 | 4.29 | 0.038 |
| Neglect Post-treatment | −0.775 | 5.18 | −10.90–9.40 | 0.02 | 0.884 | −0.12 | 0.16 | −0.42–0.19 | 0.55 | 0.458 |
| EA Post-treatment | 1.92 | 6.06 | −9.96–13.79 | 0.10 | 0.752 | 0.03 | 0.14 | −0.24–0.29 | 0.04 | 0.852 |
| Follow-up | −17.88 | 4.46 | 26.62–9.13 | 16.05 | 0.000 | −0.43 | 0.13 | −0.69–−0.18 | 10.93 | 0.001 |
| Neglect Follow-up | 2.26 | 6.31 | −10.11–14.64 | 0.13 | 0.720 | 0.07 | 0.20 | −0.32–0.46 | 0.11 | 0.738 |
| EA Follow-up | 2.89 | 7.97 | −18.51–12.72 | 0.13 | 0.716 | −0.02 | 0.18 | −0.37–0.32 | 0.02 | 0.901 |
| Model Fit | Model Fit | |||||||||
| QIC | 60,424.259 | 72.171 | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hafkemeijer, L.; Starrenburg, A.; van der Palen, J.; Slotema, K.; de Jongh, A. Does EMDR Therapy Have an Effect on Memories of Emotional Abuse, Neglect and Other Types of Adverse Events in Patients with a Personality Disorder? Preliminary Data. J. Clin. Med. 2021, 10, 4333. https://doi.org/10.3390/jcm10194333
Hafkemeijer L, Starrenburg A, van der Palen J, Slotema K, de Jongh A. Does EMDR Therapy Have an Effect on Memories of Emotional Abuse, Neglect and Other Types of Adverse Events in Patients with a Personality Disorder? Preliminary Data. Journal of Clinical Medicine. 2021; 10(19):4333. https://doi.org/10.3390/jcm10194333
Chicago/Turabian StyleHafkemeijer, Laurian, Annemieke Starrenburg, Job van der Palen, Karin Slotema, and Ad de Jongh. 2021. "Does EMDR Therapy Have an Effect on Memories of Emotional Abuse, Neglect and Other Types of Adverse Events in Patients with a Personality Disorder? Preliminary Data" Journal of Clinical Medicine 10, no. 19: 4333. https://doi.org/10.3390/jcm10194333