
Understanding How and Why Alcohol Interventions Prevent and Reduce Problematic Alcohol Consumption among Older Adults: A Systematic Review

 ,
,
Abstract
:1. Introduction
Objectives
2. Materials and Methods
2.1. Realist Evaluation Approach
2.2. Search Strategy
2.3. Inclusion Criteria
2.4. Study Selection
2.5. Data Extraction and Analysis
3. Results
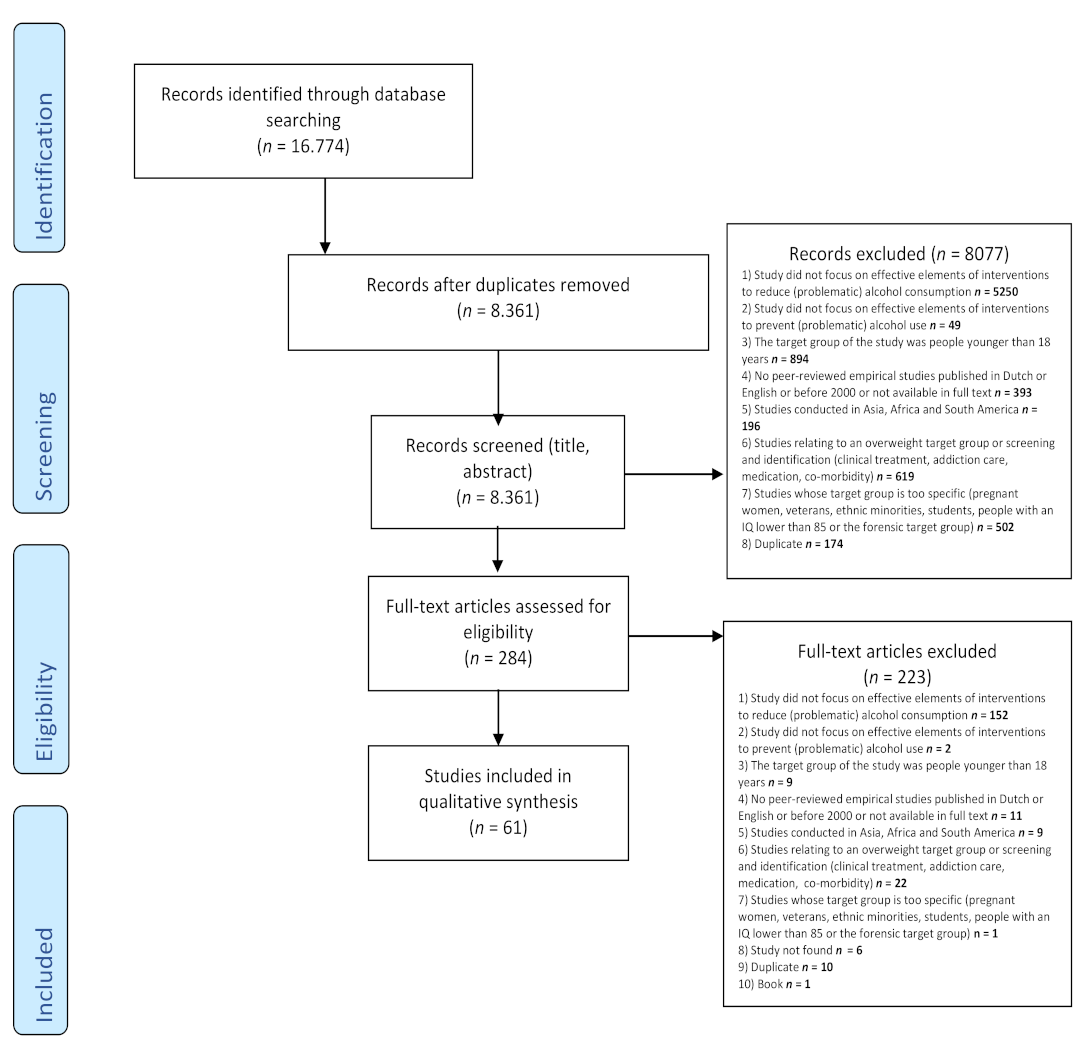
3.1. Study Selection and Characteristics

{kind=link}
| A. Context (C) 1: Therapist—In-Person—Individual | How | Why | ||||
|---|---|---|---|---|---|---|
| Author; Country | Participants; Age Mean (SD) | Method | Intervention or Aim | Intervention Elements (E) 2 and Outcome (O) 4 | Mechanisms (M) 3 and Outcome (O) 4 | Study Quality (MMAT) |
| Andréasson et al. (2002); SE [45] | N = 93; >18+ years Mean age 50.2 years (Not given) | Quantitative randomized controlled trial | Intervention: Treatment of alcohol-related problems with cognitive behavioral therapy and motivation enhancement Control: One assessment session; one session of feedback/advice, guided by the same motivation enhancement principles; and a 24-page self-help manual | Intervention: Four treatment sessions on cognitive behavioral therapy and motivation enhancement (E) → alcohol reduction (O) → reduction in the number of drinking days (O) Control: (1) One session of feedback/advice, guided by the same motivation enhancement principles (E) → reduction of alcohol (O) | Not studied | 3 |
| Baumann et al. (2015); DK [46] | N = 9415; 30–60 years Intervention: mean age 46.1 (7.9) Control: mean age 45.7 (9.8) | Quantitative randomized controlled trial | Intervention 1A: Screening, risk assessment and individual lifestyle counselling; participants at high risk of ischemic heart disease were also offered group-based counselling Intervention 1B: High-risk people in the intervention group were offered group-based counselling on smoking cessation or on diet and physical activity Control: No intervention | Intervention 1A: Sessions were conducted by a nurse, dietitian or doctor (E) trained in motivational interviewing (E) → greater reductions in binge drinking during the 5 years of intervention (O) Intervention 1B: Additionally, high-risk people in the intervention group were offered group-based counselling on smoking cessation or on diet and physical activity (E) → reported greater reductions in binge drinking during the 5 years of intervention (O) | Not studied | 4 |
| Connors et al. (2016); USA [47] | N = 63; 18 and 65 years Mean age 48.27 (10.64) | Quantitative non-randomized | Aim: Examined therapeutic alliance. Participants seeking treatment for an alcohol use disorder received 12 weeks of cognitive behavioral therapy (CBT) for alcohol dependence and completed weekly assessments of the alliance | Not studied | (1) Higher therapeutic alliance scores (M) (2) achieved though therapist and patient collaboration in the identification of additional sessions as judged best to meet the patient’s clinical needs (M) → fewer drinking days (O) in the period until the next treatment session → fewer heavy drinking days in the period until the next treatment session (O) | 5 |
| Csillik et al. (2022); FR [48] | N = 45 >18+ years Mean age: 44.6, (11.6) | Randomized controlled trial | Intervention: The efficacy of three MI intervention plans using a randomized matched pre-test/post-test design spanning a 10-week period | Intervention: Five individual face-to-face motivational interview (E) sessions conducted over a ten-week period → reduction of alcohol consumption (O) | Not studied | 3 |
| Ilgen et al. (2006); USA [49] | N = 785; Age not specified Mean age not specified | Quantitative randomized | Aim: Investigated whether a positive therapeutic relation is particularly beneficial for patients entering alcohol use disorder treatment with low motivation Intervention: Project MATCH. Patients were randomly assigned to twelve-step facilitation, cognitive behavioral coping skills or motivational enhancement therapy | Not studied | (1) High-quality therapeutic relationship (M) was more strongly associated with → reductions in alcohol use (O) among patients with (2) low motivation (M) than among those with high motivation | 5 |
| Karno et al. (2002); USA [50] | N = 47: Age not specified Mean age 38.8 | Quantitative non-randomized | Aim: Examined the effects of interactions between patient attributes and therapist interventions on alcoholism treatment outcome. The partners of these patients participated in treatment but were not a focus of this study Intervention: Psychotherapy session from either cognitive behavioral or family systems therapy | Intervention: cognitive behavioral therapy (E) → had significantly better drinking outcomes (O) than family systems therapy (E) | (1) Use of interventions early in treatment that emphasized emotional experiences (M) → less alcohol consumption (O) (2) The relationships between emotional distress and therapist focus on affect (M) and patient reaction and therapist directness (M) → were important predictors of alcohol use (O) during the maintenance phase of treatment | 4 |
| Kavanagh and Connolly (2009); AUS [51] | N = 204; Age 19–80 years Mean age 47.8 (10.8) | Quantitative randomized controlled trial | Intervention: General practitioners (GPs) received a letter providing a summary of baseline assessments plus standard guidelines on management of alcohol disorders in general practice. They were informed of their patients’ progress. Participants received information about alcohol’s effect, a self-help booklet and self-monitoring forms Control group: Received information about alcohol’s effects, a self-help booklet and self-monitoring forms. Posted self-monitoring forms each fortnight and received letters that summarized progress, encouraging continued self-monitoring and self-monitoring forms | Intervention: GPs receiving information about the alcohol behavior of patients (E) and at monthly intervals over the following 6 months, an update about their patients’ progress (E) → drank on fewer days (O) | Not studied | 5 |
| Khan et al. (2013); UK [52] | N = 141; >18+ years Mean age not specified | Quantitative non-randomized | Aim: Possible benefits of offering a brief alcohol intervention within community pharmacies Intervention: Hazardous drinkers received a full brief intervention from the pharmacist based on the Feedback, Listen, Advice, Goals and Strategies (FLAGS) technique | Intervention: (1) Full brief intervention given by the pharmacist (E) based on the Feedback, Listen, Advice, Goals and Strategies technique (E) and (2) an alcohol unit wheel calculator (E), (3) a “Units and You” booklet (E) and a leaflet with contact details of local and national specialist alcohol services (E) → reduction in the number of drinking days reported by hazardous drinkers (O) → a highly significant reduction in the number of alcohol units consumed by hazardous drinkers (O) | Not studied | 4 |
| *Kiluk et al. (2016); USA [53] | N = 68; >18+ Mean age 42.7 (1.9) | Quantitative randomized controlled trial | Intervention 1: Treatment as usual plus on-site access to computerized cognitive behavioral therapy targeting alcohol use Intervention 2: Computerized cognitive behavioral therapy plus brief weekly clinical monitoring Intervention 3: On-site access to computerized cognitive behavioral therapy targeting alcohol use Control: Treatment as usual | Intervention 1: Weekly group or individual motivational psychotherapy delivered by masters-level counsellors at the outpatient facility (E) → lower alcohol consumption (O) Intervention 2: Computerized cognitive behavioral therapy plus brief weekly clinical monitoring (E) → reduction of alcohol consumption (O) Control: (1) Weekly group or individual motivational psychotherapy (E) → reduction alcohol use (O) | Not studied | 4 |
| Kingree and Thompson (2011); USA [54] | N = 268; >18+ years Mean age not specified | Quantitative non-randomized | Intervention 1: Assessed participation in meetings Intervention 2: Having a sponsor | Intervention 1: Not effective Intervention 2: Having a sponsor (E) → subsequent abstinence from alcohol (O) | Not studied | 4 |
| Mowbray (2013); USA [55] | N = 271; >18+ years Mean age 44.6 | Quantitative non-randomized | Aim: Could setting drinking goals be a mechanism of change Intervention 1: Classic abstinence-based treatment models Intervention 2: A drinking programme that helped individuals to reduce, but not to stop, their drinking | Interventions (1) Individuals with abstinence as a drinking goal (E) → significantly increased abstinent days (O) → significantly fewer heavy drinking days (O) | Not studied | 4 |
| Nielsen and Nielsen (2018); DK [56] | N = 276; Intervention: mean age 42.6 Control: mean age 40.3 | Quantitative non-randomized | Intervention: (1) All patients in the intervention received a single motivational session after assessment and before treatment assignment; (2) patients were allocated to one of the four treatments by the actuarial matching system described above, without discretion for clinical judgement Control: Treatment based on clinician judgement | Intervention: A single motivational session after assessment and before treatment assignment (E) → significantly more likely to complete treatment and show a greater reduction in drinking (O) | Not studied | 3 |
| Orford et al. (2006); UK [57] | N = 211; Age not specified Mean age 42 years | Qualitative interviews | Aim: To develop a model of change during and following professional treatment (social behavior and network therapy and motivational enhancement therapy) for drinking problems, grounded in clients’ accounts Intervention 1: Three sessions of motivational enhancement therapy over 12 weeks Intervention 2: Eight sessions of social behavior and network therapy over 12 weeks | Intervention 1: Not studied Intervention 2: Not studied | (1) Thinking differently (M) (2) Family and friends support (M) (3) Acting differently (M) (4) Treatment delivers new insights (5) Down to me: clients often expressed the view that change was self-directed (M) (6) Seeing the benefits (M) (7) Catalyst (M) is a simple summary of a set of processes that were talked about at greater length by clients during pre-treatment interviews → less alcohol consumption (O) | 5 |
| Orford et al. (2009); UK [58] | N = 397; Age not specified | Qualitative interviews | Aim: Social treatment (social behavior and network therapy and motivational enhancement therapy) to explore the factors to which clients attributed positive changes that might have occurred in their drinking Intervention 1: Three sessions of motivational enhancement therapy over 12 weeks Intervention 2: Eight sessions of social behavior and network therapy over 12 weeks | Intervention 1: Not studied Intervention 2: Not studied | (1) Involvement of other people (excluding therapists or other professionals) in supporting own behavior change by attending treatment sessions or in any other way (M) (2) Communicating better and more openly (M) (3) Awareness of, and thinking about, the consequences of drinking (M) (4) Feedback of results from assessment (M) (5) Thinking about what is important in life (M) → change in drinking (O) | 5 |
| Richardson et al. (2011) NZ [59] | N = 125; 17–59 years Mean age 37.6 (10.4) | Quantitative randomized controlled trial | Intervention 1: Motivational enhancement therapy: four sessions Intervention 2: Non-directive reflective listening: four sessions Control: No sessions | Intervention 1: No significant effect Intervention 2: No significant effect Control: No significant effect | Therapeutic alliance (M) was significantly higher for clients who attended all four sessions (E) More therapeutic alliance because of more attendance (M) → more abstinent days (O) | 3 |
| Team UR (2005); UK [60] | N = 742;> 16+ Mean age 41.6 (10.1) | Quantitative randomized controlled trial | Intervention 1: Social behavior and network therapy: three 50-min sessions over eight to 12 weeks to help clients build social networks Intervention 2: Motivational enhancement therapy comprised three 50-min sessions over eight to 12 weeks, combining counselling in the motivational style with objective feedback | Intervention 1: Network therapy to build social networks (E) → reduction of alcohol (O) Intervention 2: (1) Counselling in the motivational (E) style and (2) including “significant others” in only the first session to provide only confirmatory information (E) → reduction of alcohol (O) | Not studied | 3 |
| * Walitzer and Dermen (2004); USA [61] | N = 64; Male clients mean age of 42.0 years (11.3); Spouses mean age of 39.3 years (9.6). | Quantitative randomized controlled trial | Intervention 1: Treatment for problem drinkers only Intervention 2: Couples’ alcohol-focused treatment Intervention 3: Couples’ alcohol-focused treatment + behavioral couple therapy | Intervention 1: Specific strategies for changing drinking patterns and informational lectures on current alcohol and other health-related topics (E) → less alcohol consumption (O) Intervention 2: Not applicable see C. Context: therapist—in-person—relatives Intervention 3: Not applicable see C. Context: therapist—in-person—relatives | Not studied | 4 |
| Wiprovnick et al. (2015); USA [42] | N = 59; Age not specified Mean age 40.25 (11.79) | Quantitative randomized controlled trial | Intervention 1: Goal of moderation and a detailed structural personalized feedback module Intervention 2: Relational motivational interviewing without directive elements consisting of the non-directive elements of motivational interviewing, including therapist stance (warmth, genuineness, egalitarianism), emphasis on client responsibility for change and avoidance of MI-inconsistent behaviors, such as advising and confronting | Intervention 1: Not studied Intervention 2: Not studied | The change in therapeutic bond (E) and empathic resonance (M) from Week 1 to Week 8 was → significant in predicting drinking outcomes (O) → and decreased alcohol use at the end of treatment for participants in both conditions (O) | 2 |
| B. Context: Therapist—Not-in-Person—Individual | ||||||
| Author; Country | Participants; Age | Method | Intervention or Aim | Intervention Elements (E) 2 and Outcome (O) 4 | Mechanisms (M) 3 and Outcome (O) 4 | Study Quality (MMAT) |
| Best et al. (2015); USA [62] | N = 22; >18+ Mean age 43.1 (12.9) | Quantitative descriptive | Intervention: A 24-h, 7-days-a-week, free, anonymous state-wide telephone counselling, information and referral service for people who use alcohol and other drugs | Intervention: (1) Over the telephone; (2) practice elements were presented in the manual alongside a spatial representation through a cognitive (node-link) mapping exercise. After the initial session, the participants were posted a copy of the workbook containing node-link maps, drink diaries and information connected to each of the relevant modules (E) → reduction in drinking (O) | Not studied | 3 |
| Bischof et al. (2008); DE [63] | N = 408; 18–64 years Intervention 1: mean age 36.8 (13.2) Intervention 2: mean age 36.8 (13.5) Control mean age 35.9 (13.7) | Quantitative randomized controlled trial | Intervention 1: Stepped-care participants received computerized feedback and a maximum of three brief counselling sessions based on motivational interviewing and behavioral change counselling. All counselling sessions were conducted by telephone Intervention 2: Full-care participants received computerized feedback and simultaneously received brief counselling sessions conducted by trained psychologists based on motivational interviewing and containing structured elements of behavioral change counselling. Counselling sessions were conducted by telephone Control group: Participants received roughly half of the number of intervention in minutes compared with full-care participants | Both interventions: (1) Received computerized feedback (E) and (2) a maximum of three brief counselling sessions based on motivational interviewing and behavioral change counselling. (3) All counselling sessions were conducted by telephone (E) → reduction in drinking (O) Control group: No significant effect | Not studied | 3 |
| Blankers et al., (2011); NL [64] | N = 205; 18–65 years Mean age 42.2 (9.7) | Quantitative randomized controlled trial | Intervention 1: No-therapist-involved web-based intervention: fully automated, self-guided treatment programme Intervention 2: Therapist-involved web-based intervention: synchronous online therapy including up to seven synchronous text-based chat therapy sessions. Before each chat session, the participant worked on a homework assignment. There was no other kind of contact between participants and therapists | Intervention 1: (1) Feedback about alcohol consumption is provided with interactive graphs and table (E) → reducing alcohol (O) Intervention 2: (1) Online therapy (E); (2) seven synchronous text-based chat therapy sessions (E). (3) Before each chat session, the participant worked on a homework assignment (E) → reduction of alcohol consumption (O) | Not studied | 4 |
| Brown et al. (2007); USA [65] | N = 897; 21–59 years Mean age not specified | Quantitative randomized controlled trial | Intervention: Motivational telephone calls: an adaptation of motivational interviewing administered over up to six telephone sessions Control: Received a four-page pamphlet on healthy lifestyles. One page was devoted to each of four topics: tobacco, diet, exercise and alcohol | Intervention: (1) Motivational telephone calls bolstered with summary letters (E) → significantly reduced drinking for male primary-care patients with alcohol abuse or dependence who are not necessarily seeking assistance for their drinking (O) Control: Four-page information pamphlet on healthy lifestyles (E) → reduction in alcohol consumption in women (O) | Not studied | 4 |
| Clifford et al. (2007); USA [66] | N = 235;> 18+ years Mean age 40.01 (10.00) | Quantitative randomized controlled trial | Intervention 1: Frequent comprehensive (FC) quarterly in-person follow-up interviews interspersed with monthly telephone interviews for a period of 12 months after participants’ treatment programme intake interview session. The content of the FC interviews covered the following areas: drinking and drug-taking behaviors; alcohol- and other drug-related negative consequences; medical and psychiatric status; psychological, social and cohabitation/marital relationships; and occupational functioning Intervention 2: Frequent brief (FB) quarterly in-person follow-up interviews interspersed with monthly telephone interviews for a period of 12 months after respondents’ treatment programme intake interview session. However, before the final 12-month, in-person interview, interviews were limited to addressing alcohol and other drug-taking behaviors Intervention 3: Infrequent comprehensive (IC) interviews only at the baseline and 6- and 12-month research assessment interviews. The content of the assessment battery was identical to that of the FC condition Intervention 4: Infrequent brief (IB) in-person follow-up interviews (i.e., only two, at 6 and 12 months) and a 6-month interview limited to the assessment of alcohol and other drug-taking behaviors | For all interventions: Follow-up contact after treatment with the study participants, even if brief in nature (E) → less alcohol consumption (O) FC and IC: (1) More follow-up contact after treatment for study participants (2) in-person (E) (3) or by telephone (E) → less alcohol consumption (O) | Not studied | 5 |
| Ettner et al. (2014); USA [39] | N = 1168; Age above 60 years Mean age 71 | Quantitative randomized controlled trial | Intervention: Project SHARE (Senior Health and Alcohol Risk Education), which included personalized reports, educational materials, drinking diaries, physician advice during office visits and telephone counselling Control group: Care as usual | Intervention: (1) Mailed a personalized patient report (E); (2) an educational booklet on alcohol and aging (E); (3) via telephone, a health educator contacted intervention patients three times. During these calls, the health educator answered questions about the written materials and gave feedback → at-risk drinkers reduced (O) → less alcohol consumption (O) → older adults were more likely to have discussed their alcohol use with a physician (O) | Not studied | 5 |
| Postel et al. (2015); NL [67] | N = 144; >18+ 22–66 years Mean age 45.8 | Quantitative non-randomized | Intervention: A 3-month web-based alcohol treatment programme using intensive, asynchronous (non-simultaneous) therapeutic support at a 9-month follow-up assessment | Intervention: The web-based treatment programme consisted of (1) a structured two-part online treatment programme (E); (2) the participant and the therapist communicated asynchronously via the Internet (intensive asynchronous therapeutic) (E) → reduction in the number of drinks per week (O) | Not studied | 4 |
| C. Context: Therapist—In-Person—Relatives | ||||||
| Author; Country | Participants; Age Mean (SD) | Method | Intervention or Aim | Intervention Elements (E) 2 and Outcome (O) 4 | Mechanisms (M) 3 and Outcome (O) 4 | Study Quality (MMAT) |
| Doyle et al. (2003); IE [68] | N = 67; Age not specified Mean not specified | Quantitative non-randomized | Intervention: Community-based 10-week programme involved weekly separate and conjoint group therapy for problem drinkers and their families | (1) Clients and their families attended psychoeducational lectures (E) and (2) films on addiction and recovery (E) → abstinent (O) or drinking moderately (O) | Not studied | 4 |
| McCrady et al. (2002); USA [69] | N = 68; Age not specified Mean age 39.4 (10.3) | Quantitative non-randomized | Intervention: Alcohol behavioral couple therapy (ABCT) model; three primary domains are assumed to be related to alcohol consumption: (a) individual factors related to the drinker’s alcohol consumption, (b) the quality and nature of the spouse’s responses to alcohol-related situations and (c) the nature and quality of the couple’s marital interactions | Intervention: Greater spousal use of problem solving and social support to deal with problems and less use of self-blame, wishful thinking and avoidance → less intense drinking during treatment (O) | Intervention: (1) The quality of the pre-treatment marital relationship (M) → men’s ability to remain abstinent (O) (2) The degree of the respondents’ marital happiness immediately after treatment (M) → predicted the intensity of their drinking (O) | 4 |
| McCrady et al. (2009); USA [70] | N = 102; Age not specified Intervention 1: mean age 44.78 (9.14) Intervention 2: mean age 45.31 (9.31) | Quantitative randomized controlled trial | Intervention 1: Alcohol behavioral couple therapy (ABCT) manual-guided, 20-session outpatient cognitive behavioral therapies with an explicit goal of abstinence from alcohol; all sessions included both partners | Intervention 1: (1) Sessions included both partners in all sessions (E) and (2) included self-monitoring, functional analysis of drinking and coping skills to avoid alcohol and deal with other life problems (E) resulting in more days abstinent (O) → fewer days heavy drinking (O) | Intervention 1: Interventions to teach the partner to support abstinence and to decrease attention to drinking and interventions to improve the couple’s relationship, including reciprocity enhancement, communication and problem solving (M) → more days abstinent (O) → fewer days heavy drinking (O) | 4 |
| Rentscher et al. (2017); USA [71] | N = 33; Age not specified Mean age 39.2 (10.2) | Quantitative non-randomized | Aim: Investigating pronoun use prior to and during two couple-focused interventions for problematic alcohol use: cognitive behavioral therapy and family systems therapy | Intervention: Not studied | Spouse we-talk (M) → associated with successful treatment outcomes (O) | 3 |
| Schumm et al. (2014); USA [72] | N = 105; 18–65 years Mean age women 44.42 (8.08) men 47.68 (8.40) | Quantitative randomized controlled trial | Intervention 1: BCT (behavioral couple therapy) sessions attended together by the woman and her partner Control: IBT (individually-based therapy) for women | Intervention: (1) 13 BCT sessions attended together by the woman and her partner (E) (2) to build support for abstinence and improve relationship functioning (E); (3) completion of a daily “trust discussion” in which the patient states an intent to stay abstinent that day and the spouse expresses support for the patient’s efforts (E) → more abstinent days during treatment and during the 12-month follow-up (O) | Intervention: (1) Teaching partners to decrease behaviors that may trigger or enable substance use (M); and (2) helping the couple to decrease the patient’s exposure to alcohol and drugs by removing alcohol from the home and avoiding or managing alcohol-related family and social gatherings (M) → more abstinent days during treatment and during the 12-month follow-up (O) | 3 |
| Vedel et al. (2008); NL [73] | N = 64; Age not specified Mean age 45.5 (11.34) | Quantitative randomized controlled trial | Intervention 1: Behavioral couples therapy Intervention 2: Cognitive behavioral therapy | Intervention 1: (1) Individual couple sessions (E); (2) 10 sessions (E); (3) 90 min (E) → reduction in drinking (O) Intervention 2: Cognitive behavioral therapy (1) emphasizes overcoming skill deficits and aims to increase the person’s ability to detect and cope with high-risk situations that commonly precipitate relapse (E) → reduction of drinking (O) | Not studied | 4 |
| * Walitzer and Dermen (2004); USA [61] | N = 64; Age not specified Male clients mean age 42.0 (11.3); Spouses mean age of 39.3 (9.6). | Quantitative randomized controlled trial | Intervention 1: Treatment for problem drinkers only (PDO) Intervention 2: Couples’ alcohol-focused treatment; subjects were presented with specific strategies for changing drinking patterns; informational lectures on current alcohol and other health-related topics Intervention 3: Couples’ alcohol-focused treatment + behavioralcouple therapy; subjects were presented with specific strategies for changing drinking patterns | Intervention 1: Not applicable see A.Context (C) 1: therapist—in-person—individual Interventions 2 +3 (not specified): A significant increase was obtained in the frequency of drinking days (O) | Intervention 2: Treatment material for the alcohol-focused spouse involvement component, presented in conjunction with the client’s drinking reduction strategies, consisted of specific strategies designed to increase spouse behaviors supportive of drinking reduction and to support the problem drinker’s independence and autonomy (M) → reduction in alcohol use (absent and light drinking days) (O) → reduction in heavy drinking days (O) Intervention 3: BCT consisted of a series of treatment components designed to equip each couple with a variety of skills and techniques (a) to increase cohesion and the positive aspects of their marriage and (b) to enhance communication and conflict resolution skills (M) → reduction in alcohol use (absent and light drinking days) (O) → reduction in heavy drinking days (O) | 4 |
| D. Context: Therapist—In-Person—Group Component | ||||||
| Bamford et al. (2003); UK [74] | N = 124; 21–64 years Mean age 41 | Quantitative non-randomized | Intervention: Short 6-week intervention that focused on psycho-educational materials on physical and mental complications | Intervention: (1) Focused on psycho-educational materials on physical and mental complications (E); (2) coping with family problems and mistrust (E); (3) visitors’ groups, in which patients who had made positive changes to their drinking described their experiences (E) and positive influences (E) and (4) spent less time on problem solving and managing low mood and anxiety → reduced drinking behavior (O) | Not studied | 4 |
| Brown (2007); CA [75] | N = 76; Age not specified Intervention: mean age 41.0 (9.9) Control: mean age 33.2 (8.7) | Quantitative non-randomized | Intervention: Brief, four-session group-adapted motivational interviewing (GAMI) Control: Standard care (SC) | Intervention: (1) Standardized, four-session group treatment (E) (2) in a brief, four-session GAMI intervention (E) → alcohol reduction (O) | Intervention: (1) Targeting rapid internally motivated change (M); (2) all sessions were conducted using the specific communication style and strategies associated with motivational interviewing (M) → alcohol reduction (O) | 5 |
| Gómez- Recasens et al. (2018) ES [76] | N = 1103; >18+ years Mean age 42.48 (10.44)> | Quantitative non-randomized | Intervention: To promote health and prevent alcohol and drug consumption in the workplace, emphasizing (1) health promotion and health monitoring, which included (a) alcohol and drug awareness and (b) the evaluation and monitoring of alcohol and drug consumption through a semi-structured interview designed to assess risky consumption; urine tests aimed at detecting alcohol, cannabis and cocaine use; an Alcotest based on expired air to test for the recent consumption of alcohol and a saliva exam to test for the recent consumption of six drugs; and (2) secondary prevention if risky consumption was identified | (1) Awareness (E), (2) information (E), (3) training (E), (4) participation in a workshop outside work (E), (5) evaluation and health surveillance (E), (6) medical examination (E), (7) brief intervention (E), (8) personalized advice (E), (9) personalized follow-up (E), referral to the centre for the attention and monitoring of drug addictions (E) → reduced risky alcohol consumption (O) | Not studied | 4 |
| Hagger et al. (2011); UK [77] | N = 281; 18–65 years Mean age 35.65, (12.44) | Quantitative randomized controlled trial | Intervention: Mental simulation manipulation in pen-and-paper form after receiving information about reducing alcohol consumption and questionnaire measures Control: Received identical measures and information about alcohol consumption | Intervention: (1) Mental simulation exercise (E) (2) about alcohol intake (E) and (3) health benefits of keeping alcohol intake within guidelines limits (E) → consuming fewer unit of alcohol during the 4-week follow-up period (O) Control: Effect not studied | Not studied | 4 |
| Reynolds and Bennett (2015); USA [78] | N = 1510; >18+ years Mean age not specified | Quantitative randomized controlled trial | Intervention 1: The Team Awareness Program: (1) peer referral and (2) team building: 4-h on-the-job classroom training sessions that encouraged healthy lifestyles and the seeking of professional help Intervention 2: The Choices in Health Promotion Program delivered various health topics based on a needs assessment: 4-h on-the-job classroom training sessions that encouraged healthy lifestyles and the seeking of professional help | Intervention 1: (1) Relevance (E); (2) team ownership of policy (E); (3) understanding tolerance (E); (4) communication (E); (5) support and encourage help (E) → reduced monthly alcohol intake (O)Intervention 2: (1) 4-hour programme developed based on needs assessment (E), (2) goal setting (E) and (3) choice components (E) → reduced monthly alcohol intake (O) | Not studied | 3 |
| Toft et al. (2009); DK [79] | N = 9.415; 30, 35, 40, 45, 50, 55 and 60 years Majority of individuals at the age of 40 to 50 years | Quantitative randomized controlled trial | Intervention 1 (Low risk): Each participant had a lifestyle consultation focusing on smoking, physical activity, diet and alcohol Intervention 2 (High risk): Each participant had a lifestyle consultation focusing on smoking, physical activity, diet and alcohol. The individually counselled high-risk individuals were offered group counselling on diet and exercise or smoking | Intervention 1: (1) Each participant had a lifestyle consultation focusing on smoking, physical activity, diet and alcohol (E) → men decreased their alcohol intake (O) → less binge drinking in both men and woman (O) Intervention 2: (1) Each participant had a lifestyle consultation focusing on smoking, physical activity, diet and alcohol (E); (2) the individual counselling high-risk individuals were offered group counselling on diet and exercise or smoking; (3) the relatives of the participants were offered the chance to participate in one of the meetings (E) → men decreased their alcohol intake (O) → less binge drinking in both men and women (O) | Not studied | 4 |
| E. Context: No Therapist—Not In-Person—Individual | ||||||
| Author; Country | Participants; Age Mean (SD) | Method | Intervention or Aim | Intervention Elements (E) 2 and Outcome (O) 4 | Mechanisms (M) 3 and Outcome (O) 4 | Study Quality (MMAT) |
| Augsburger et al. (2021); EE [80] | N = 589 >18+ years Mean age: 37.86 (11.16) | Randomized controlled trial | Intervention: To estimate the efficacy of an on-line self-help intervention to reduce problem drinking at thepopulation level | Intervention: 10 modules based on principles of cognitive–behavioral therapy and motivational interviewing (E). Access to a website with a self-test including personalized normative feedback (E) and information for standard alcohol treatment. Control: access to a help-page received PNF on a self-test for alcohol consumption (E) and furtherinformation together with contact details for treatment options → reduction of alcohol consumption (O) | Not studied | 3 |
| Baumann et al. (2017); DE [81] | N = 1282; 18–64 years Mean age 30.1 (11.1) | Quantitative randomized controlled trial | Intervention 1: Brief intervention tailored to the motivational stage (ST) Intervention 2: Brief non-stage tailored intervention (NST) Control: Assessment only (AO) | Intervention 1: (1) Individualized computer-generated feedback letters in comparison to other persons at the same stage of change and feedback on intrapersonal changes by comparing the participant’s current and previous data (E); (2) the letters referred to particular pages in the accompanying stage-matched manual for further information) → only persons with daily low use benefitted from intervention (O) → more change of being abstinent after 15 months (O) Intervention 2: Individualized computer-generated feedback letters in comparison to other persons at the same stage of change and feedback on intrapersonal changes by comparing the participant’s current and previous data (E) → only persons with daily low use benefitted from intervention (O) → more chance of being abstinent after 15 months (O) Control: No effect given | Not studied | 4 |
| Bagnardi et al. (2011); I [82] | N = 6026; >15+ Mean age not specified | Quantitative non-randomized | Intervention (coordinated community-based intervention): Informing residents about and committing them to the project, brochures, alcohol-free parties, public events promoting a healthy lifestyle, news about the project in local newspapers educating at schools, religious and sporting facilities, meetings with parents/teachers, driving schools, physicians, police forces and volunteers and meetings and alcohol-free events at centres for older adults | Intervention: (1) Informing residents about and committing them to the project (E), brochures (E), alcohol-free parties (E), public events promoting a healthy lifestyle (E), news about the project in local newspapers (E); (2) educating at schools, religious and sporting facilities (E), meetings with parents/teachers, driving schools, physicians, police forces and volunteers (E) and meetings and alcohol-free events at centres for older adults (E) → reduced alcohol consumption (O) | Not studied | 3 |
| Blankers et al., (2011); NL [64] | N = 205; 18–65 years Mean age 42.2 (9.7). | Quantitative randomized controlled trial | Intervention 1: No-therapist-involved web-based intervention: fully automated, self-guided treatment programme Intervention 2: Therapist-involved web-based intervention: synchronous online therapy including up to seven synchronous text-based chat therapy sessions. Before each chat session, the participant worked on a homework assignment. There was no other kind of contact between participants and therapists | Intervention 1: Feedback about alcohol consumption was provided with interactive graphs and table (E) → reducing alcohol conspumtion (O) Intervention 2: (1) Online therapy (E), (2) seven synchronous text-based chat therapy sessions (E), (3) before each chat session, the participant worked on a homework assignment (E) → reduction of alcohol consumption (O) | Not studied | 4 |
| Connors et al. (2017); USA [83] | N = 111; Age not specified Woman: mean age 46.99 (11.79) Men: mean age 15.54 (2.70) | Quantitative randomized controlled trial | Intervention 1: Bibliotherapy (a self-directed manual) alone Intervention 2: Bibliotherapy with one telephone-administered motivational interview Intervention 3: Bibliotherapy with one telephone-administered motivational interview and six biweekly telephone (50 min) therapy sessions | Intervention 1: (1) 122-page self-directed manual (E) (2) focused on self-awareness of drinking behavior, identifying danger signals regarding problem drinking situations, developing strategies for reducing alcohol intake and reducing risks associated with drinking that does occur → fewer heavy drinking days (O) → increased abstinent and light drinking days (O) Intervention 2: Bibliotherapy with one telephone-administered motivational interview of 60 min (E) → increased abstinent and light drinking days (O) Intervention 3: Bibliotherapy (E) with one telephone-administered motivational interview (E) and six biweekly telephone (50 min) therapy sessions (E) → increased abstinent and light drinking days (O) | Not studied | 4 |
| Cunningham et al. (2001); CA [84] | N = 449; Age not specified Intervention: mean age 41.0 (10.8) Control group: 38.8 (10.5) | Quantitative non-randomized | Intervention: Brief self-help booklet provided at assessment for alcohol treatment | Intervention: (1) Self-help booklet (E); (2) perspective of encouraging the individuals to consider the costs of their drinking, to motivate them to want to change and to take the next step towards change (E) → drinking on fewer days (O) → and drinking less on each occasion (O) | Not studied | 4 |
| Cunningham et al. (2009); CA [85] | N = 185; Age not specified Mean age 40.1 (13.4) | Quantitative randomized controlled trial | Intervention (internet personalized alcohol feedback): After completing a brief online assessment, participants received a ‘Personalized Drinking Profile’ Control: Sent a list of the informational components that could be included in a computerized summary for drinkers | Intervention: (1) Participants received a ‘Personalized Drinking Profile’ (E); the core element was normative feedback pie charts that compare the participant’s drinking with that of others of the same age, sex and country of origin (E) → less alcohol consumption (O) | Not studied | 4 |
| Cunningham et al. (2014); CA [86] | N = 741; >19+ years Mean age 29.8 (9.7) | Quantitative randomized controlled trial | Intervention 1: The normative feedback component of the Check Your Drinking Screener (a personalized feedback intervention) Intervention 2: Personalized feedback information of the Check Your Drinking Screener Intervention 3: The full Check Your Drinking Screener intervention, both the normative feedback and other personalized feedback components. Control: No intervention | Intervention 1: No significant effect Intervention 2: (1) Personalized feedback information (E) → reduction in the number of drinks in a typical week (O) Intervention 3: (1) Both the normative feedback (E) and other personalized feedback components (E) → reduction in the number of drinks in a typical week (O) | Not studied | 4 |
| Dulin et al. (2014); USA [87] | N = 28; 18–45 years Mean age 33.6 years, (6.5) | Quantitative descriptive | Intervention: Smartphone-based intervention: stepwise approach to providing the information and interventions to the client; enhancement of motivation for change by providing assessment feedback and immediate coping strategies | Intervention: (1) Enhancement of motivation for change by providing assessment feedback (E); fewer heavy drinking days (O) → fewer drinks per day (O) | Intervention: (1) Enhanced awareness, i.e., “it helped me to keep track” and “the reports made me realize how much I was drinking and what were my triggers” → fewer heavy drinking days (O) → fewer drinks per day (O) | 4 |
| Fink et al. (2005); USA [40] | N = 711; >65+ Mean age 75.6 | Quantitative randomized controlled trial | Intervention 1: Combined report intervention: participants and their GPs received a personalized report of their drinking risks and education Intervention 2: Patient report intervention: only participants received a personalized report of their drinking, risk and education Control: Minimal assessments | Interventions 1 and 2: (1) Personalized reports of their drinking classification (E) and (2) educational information to patients (E) → reduction alcohol (O) | Not studied | 5 |
| Freyer-Adam et al. (2014); DE [43] | N = 1243; 18–64 years Control: mean age 30.1 (10.9) Intervention 1: mean age 29.5 (10.7) Intervention 2: mean age 30.6 (11.7) | Quantitative randomized controlled trial | Intervention 1: The stage tailored intervention: individualized computer-generated feedback letters and self-help manuals. Each text module was dependent on the current stage of change Intervention 2: The non-stage tailored intervention: individualized computer-generated feedback letters and self-help manuals | Intervention 1: (1) individualized computer-generated feedback letters (E); (2) each text module was dependent on the current stage of change (E); (3) the participant’s responses were compared with normative data of individuals at the same stage (E); (4) self-help manuals (E) → reduction of alcohol consumption in the short term (O) → reduction of alcohol consumption in the long term (O) Intervention 2: (1) Computer-generated feedback letters (E); (2) feedback was accompanied by information and/or advice; (E) (3) participants were encouraged to complete a when/where/how-to-change plan, introduced by gender-specific examples (E) → reduction in alcohol consumption in the short term (O) | Not studied | 2 |
| Giroux et al. (2014); USA [88] | N = 28; 22–45 years Mean age 33.6 (6.5) | Qualitative interviews | Intervention: Smartphone-based intervention: 10 psychoeducational modules and tools for change, which provided immediate coping strategies and monitoring functions for numerous alcohol-related issues | Intervention: Not studied | Smartphone-based intervention (1) raising awareness about drinking (M) → motivated to change their drinking (O) (2) teaching new skills that could be transferred to other areas of their life (M) → motivated to change their drinking (O) → (3) tracking progress related to their goals → motivation to continue engaging in non-drinking behavior (O) | 5 |
| Gonzalez and Dulin (2015); USA [89] | N = 60; >18+ years Intervention 1: mean age 33.57 (6.54) Intervention 2: mean age 34.30 (6.22) | Quantitative non-randomized | Intervention 1: Location-Based Monitoring and Intervention for Alcohol Use Disorder (LBMI-A): participants were provided with a customized LBMI-A-enabled smartphone. The LBMI-A provided seven psychoeducation modules or steps: (1) assessment and feedback, (2) high-risk locations for drinking, (3) selecting and using supportive people for change, (4) cravings and their management, (5) problem-solving skills, (6) communication and drink refusal skills and (7) pleasurable non-drinking activities. Following the completion of a step, an associated tool became available Intervention 2: The online Drinker’s Check-Up plus bibliotherapy (DCU+Bib): the DCU is an internet-based, brief motivation intervention that can be completed in less than one hour. It provides a comprehensive assessment of drinking and alcohol-related problems, objective and norm-based feedback, a decisional balance exercise to help resolve ambivalence about change, goal selection, brief development of a change plan and brief interventions to facilitate change | Intervention 1: (1) Seven psychoeducation modules (E); weekly feedback reports (E) → less alcohol consumption (O) → fewer heavy drinking days (O) Intervention 2: (1) Objective and norm-based feedback (E); (2) links to other online interventions and resources (E); (3) a 16-page booklet (E); (4) an accompanying web page that has additional interactive worksheets and modules for handling urges, drink refusal and recovering from a slip (E) → less alcohol consumption (O) → fewer heavy drinking days (O) | Not studied | 3 |
| Guillemont et al. (2017); FR [90] | N = 1147; >18+ years Mean age not specified | Quantitative randomized controlled trial | Intervention: The Alcoometre self-help web-based intervention delivers personalized normative feedback and some general information about alcohol Control: Were informed that their alcohol consumption was hazardous and were given information about hazardous drinking | Intervention: (1) Web-based intervention (E) delivers (2) personalized normative feedback (E) and (3) some general information about alcohol (E). (4) Participants can review their motivations and fears regarding reducing their alcohol intake (E), (5) set individual goals (E) and (6) monitor their progress via a consumption diary and other tools (E) → reduction in weekly alcohol intake (O) | Not studied | 3 |
| * Kiluk et al. (2016); USA [53] | N = 68; >18+ years Mean age 42.7 (11.9) | Quantitative randomized controlled trial | Intervention 1: Treatment as usual plus on-site access to computerized cognitive behavioral therapy targeting alcohol use Intervention 2: Computerized cognitive behavioral therapy plus brief weekly clinical monitoring Intervention 3: On-site access to computerized cognitive behavioral therapy targeting alcohol use Control: Treatment as usual | Intervention 1: Not applicable see C)1: therapist—_in-person—_individual Intervention 2: Not applicable see C)1: therapist—_in-person—_individual Intervention 3: On-site access to computerized cognitive behavioral therapy targeting alcohol use → reduction of alcohol consumption (O) Control: Not applicable | Not studied | 4 |
| Koffanus (2018); USA [91] | N = 40; >18+ years Intervention: mean age 46.6 (12.5) Control: mean age 45.2 (11.5) | Quantitative randomized controlled trial | Intervention: Breathalyser that allows remote, user-verified collection of a breath alcohol sample, text messaging and reloadable debit cards for remote delivery of incentives to evaluate a contingency management treatment for alcohol use disorder that can be delivered with no in-person contact | Intervention: (1) 21 consecutive days with three remote breathalyser screens per day (E); (2) participants self-reported their previous day’s alcohol use and current withdrawal symptoms daily in response to a text message and/or phone call (E); (3) participants chose these times each day with guidance from research staff (E). (4) Incentive payments (E) → less alcohol consumption per day | Not studied | 5 |
| Kuerbis et al. (2015); USA [41] | N = 86; >50+ years Mean age 64.7 (8.4) | Quantitative randomized controlled trial | Intervention: Brief mailed intervention with personalized mailed feedback outlining their specific risks associated with alcohol and educational booklets Control: No intervention | Intervention: (1) A personalized feedback report (E) and (2) two alcohol education booklets (E) → less at-risk drinking (O) | Not studied | 4 |
| Lockwood et al. (2020); UK [92] | N = 3057 (questionnaires) N = 14 (interviews) Age between 45–65 years | Mixed methods questionnaires and interviews | Aim: evaluate the impact of a “gain-framed”, multimedia campaign to encourage heavier drinking men aged 45–64 years to drink less. | Intervention: more aware of how much they routinely drink, and to make healthier choices. (1) Providing information about health consequences (E); providing information about emotional consequences (E); encouraging self-monitoring of behavior (E); encouraging self-monitoring of outcomes of behavior (E) and encouraging behavioral experiments (E). | Appreciated the friendly, non-threatening tone and that the message was straightforward (M), meaningful, achievable (M), and was gainframed—i.e., emphasised the benefits of drinking less rather than the harms of drinking too much (M) → reduction of alcohol consumption (O) | 4 |
| Moody et al. (2018); USA [93] | N = 36; 18–65 years Intervention: mean age 38.89 (11.58) Control: mean age 40.24 (12.91) | Quantitative non-randomized | Intervention: Two-week implementation intention interventions that linked high-risk situations with alternative responses Control: Two-week implementation intention interventions for selected situations and responses but did not link these together | Intervention: (1) Cut back on drinking over the following two weeks (E) (2) and fill in an “if–then” worksheet format. Response (linked high-risk situations with alternative responses) (E) → with a significant reduction in alcohol consumption when drinking was reported (O) → more abstinent days (O) Control: To try to cut back on drinking over the following two weeks (E) and (3) asked to select situations and responses but did not link these together (E) → more abstinent days (O) | Not studied | 3 |
| Nygaard (2001); DK [94] | N = 13; 35–45 years | Qualitative interviews | Intervention: The participants were asked to abstain from drinking alcohol for 6 weeks, during which period they were to maintain their “normal” social behavior and obligated to keep a diary of their experiences with abstinence | Intervention: (1) Abstain from drinking alcohol for 6 weeks (E), during which period participants were to maintain their “normal” social behavior (E) → the participants reporting the largest decrease in consumption were the persons reporting the highest initial consumption level (O) | Intervention: (1) Abstain from drinking alcohol for 6 weeks (E), during which period the participants were to maintain their “normal” social behavior (E), producing increased awareness of the role of alcohol in their lives (M). (2) Participants expressed more insights into their expectations of social gatherings and how to fulfil them (M) → the participants reporting the largest decrease in consumption were the persons reporting the highest initial consumption level (O). (3) More participants reported that they now made conscious decisions about their alcohol consumption prior to participating in a social gathering and that they would feel more comfortable complying with those decisions (M) → some started to drink at a slower pace, and others started bringing their own water bottles (O) | 3 |
| Van Lettow et al. (2015); NL [95] | N = 2634; Age not specified Mean age 37.03 (15.19) | Quantitative randomized controlled trial | Intervention 1: Drinktest (online personalized feedback intervention) plus prototype alteration (feedback regarding prototype alteration tailored to gender, drinking behavior (also including normative feedback), intentions, and prototypical self-characterization) Intervention 2: Drinktest (online personalized feedback intervention) plus cue reminder Intervention 3: Drinktest (online personalized feedback intervention) plus prototype alteration and cue reminder Control: Original Drinktest (1) received feedback tailored to demographic background (gender drinking behavior (also including normative feedback), intentions, and prototypical self-characterization), alcohol consumption and intentions to reduce drinking. These messages reflected on personal drinking levels in comparison with the Dutch norm and peers’ drinking behavior | Intervention 1: (1) Received feedback tailored to gender, drinking behavior (also including normative feedback) (E), intentions and prototypical self-characterization; (2) the prototype message reflected on characteristics that the participants evaluated as personally desirable or undesirable by evaluating themselves on 11 characteristics (E); (3) participants were encouraged to reduce their drinking to achieve their desired characteristics and, in turn, to be positively valued by peers (E); (4) then, participants were guided in their goal setting by selecting an action plan to achieve the desired characteristics (E) → reduction of alcohol consumption (O) Intervention 2: (1) Received feedback tailored to demographic background (gender), alcohol consumption and intentions to reduce drinking. These messages reflected on personal drinking levels in comparison with the Dutch norm and peers’ drinking behavior (E). Participants were guided in their goal setting by selecting an action plan to achieve the desired characteristics (E). (2) Feedback was provided that reflected on their action plans, explaining that a cue reminder may help them to remember their plans (E) (if made) and they received a free silicone bracelet by mail. If participants did not want to receive the bracelet, they were encouraged to select a piece of their own jewellery or another object of frequent use (E) → reduction of alcohol consumption (O) Intervention 3: (1) Drinktest plus prototype alteration, cue reminder and feedback tailored to gender, drinking behavior (also including normative feedback) (E), intentions and prototypical self-characterization. (2) The prototype message reflected on characteristics that the participants evaluated as personally desirable or undesirable by evaluating themselves on 11 characteristics (E); (3) participants were encouraged to reduce their drinking to achieve their desired characteristics and, in turn, to be positively valued by their peers (E). (4) Participants were guided in their goal setting by selecting an action plan to achieve the desired characteristics (E). (5) Feedback was provided that reflected on their action plans, explaining that a cue reminder may help them to remember their plans (E) (if made) and they received a free silicone bracelet by mail. If participants did not want to receive the bracelet, they were encouraged to select a piece of their own jewellery or another object of frequent use (E) → reduction of alcohol consumption (O) Control group: Original Drinktest: (1) received feedback tailored to demographic background (gender), alcohol consumption and intentions to reduce drinking. These messages reflected on personal drinking levels in comparison with the Dutch norm and peers’ drinking behavior → reduction in alcohol consumption (O) | Not studied | 3 |
| Tait et al. (2019); AUS [96] | N = 793; >18+ years Mean age 40.1 (10.0) | Quantitative randomized controlled trial | Intervention 1: Daybreak is a self-guided programme, accessible via mobile app and desktop with weekly check-ins and peer support. The Daybreak programme enables participants to connect with other users of the programme through a blog function Intervention 2: Daybreak + coaching: Daybreak and access to an online health coach between 7:00 and 19:00 on weekdays | Intervention 1: (1) Weekly check-ins: the programme includes self-reported questionnaires to encourage participants to undertake self-reflection to explore their intrinsic motivators for change (E) (2) Peer support: the programme enables participants to connect with other users of the programme through a blog function (E) → reduction of alcohol use (O)Intervention 2: No effective elements | Not studied | 3 |
| Zill et al. (2019); DE [97] | N = 608; >18+ years Intervention: mean age 40.4 (11.2) Control: mean age 40.7 (12.1) | Quantitative randomized controlled trial | Intervention: Vorvida: a German Internet intervention based on cognitive behavioral therapy (CBT) methods, which automatically tailors content to match individual user characteristics | Intervention: (1) Internet intervention based (E) on (2) cognitive behavioral therapy (E) methods, which (3) automatically tailors content to match individual user characteristics (E) → less alcohol consumption (O) → less binge drinking (O) | Not studied | 4 |
| F. Context: No Therapist—Not In-Person—Group Component | ||||||
| Author; Country | Participants; Age Mean (SD) | Method | Intervention or Aim | Intervention Elements (E) 2 and Outcome (O) 4 | Mechanisms (M) 3 and Outcome (O) 4 | Study Quality (MMAT) |
| Black et al. (2020); AUS [98] | N = 24 Age not specified Mean age: 42.42 (8.69) | Qualitative interviews | Aim: to inform recruitment and retention strategies by exploring users’ motivations and experiences in using a novel, Internet intervention, the Hello Sunday Morning (HSM) program. | Intervention: (1) Publicly set a personal goal to stop drinking or reduce consumption for a set period of time (E); (2) record their reflections and progress on blogs and social networks (E) → reduction of alcohol consumption (O) | Support and normalization: participants gained social support from other consumption (M), and their problems with alcohol and desire to seek help were normalized (M); (2b) goal setting and self-monitoring: setting goals (M) and monitoring progress provided participants with motivation and self-accountability (M) → reduction of alcohol consumption (O) | 5 |
| Haug et al. (2020); USA [99] | N = 57 Age 21–30, 31–40, 41–50, 51–60, 61 or older | Quantitative descriptive | Intervention: Self-guided alcohol Internet intervention that provides access to several different online social networks and is based on principles of harm reduction, cognitive-behavioral therapy (CBT), and relapse prevention | Intervention: Online mutual help program to change their alcohol drinking(E) cyber community (E), social networking (E), and self-help tools (E) → reduction of alcohol consumption (O) | consumption of more than one online activity (e.g., Facebook group plus online chat) (M) was associated with greater reductions in self-reported alcohol consumption (O) | 4 |
| Kirkman et al. (2018); AUS [44] | N = 1917; Age not specified Mean age 46 (11.71). | Quantitative non-randomized | Intervention Hello Sunday Morning (HSM): An Australian social media health promotion “movement” that asks participants to set a personal goal publicly to stop drinking or reduce their consumption, for a set period of time, and to record their reflections and progress on blogs and social networks | Intervention: (1) Publicly set a personal goal to stop drinking or reduce consumption for a set period of time (E); (2) record their reflections and progress on blogs and social networks (E) → reduction of alcohol use (O) | Not studied | 1 |
3.2. Themes
- A. Practitioner—in-person—individual
- Paying attention to drinking behavior
- The relationship between the patient and the therapist
- B. Practitioner—not in-person—individual
- Personal contact and feedback
- Online communication and feedback
- C. Practitioner—in-person—relatives
- The status of the relationship
- Teaching the partner to deal with drinking behavior
- D. Practitioner—in-person—group component
- Motivating to change lifestyle
- Motivating to change lifestyle delivered in a workplace setting
- E. No practitioner—not in-person—individual
- Web-based interventions
- Telephone based interventions
- F. No practitioner—not in-person—group component
4. Discussion
4.1. Limitations
4.1.1. Practical Implications
4.1.2. Scientific Recommendations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Global Status Report on Alcohol and Health; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- McGilton, K.S.; Vellani, S.; Yeung, L.; Chishtie, J.; Commisso, E.; Ploeg, J.; Andrew, M.K.; Ayala, A.P.; Gray, M.; Morgan, D.; et al. Identifying and understanding the health and social care needs of older adults with multiple chronic conditions and their caregivers: A scoping review. BMC Geriatr. 2018, 18, 231. [Google Scholar] [CrossRef] [PubMed]
- Stathokostas, L.; McDonald, M.W.; Little, R.M.D.; Paterson, D.H. Flexibility of Older Adults Aged 55–86 Years and the Influence of Physical Activity. J. Aging Res. 2013, 2013, 743843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, P.; Scafato, E.; Galluzzo, L. Alcohol and older people from a public health perspective. Ann. Ist. Super. Sanita 2012, 48, 232–247. [Google Scholar] [CrossRef] [PubMed]
- Breslow, R.A.; Castle, I.-J.P.; Chen, C.M.; Graubard, B.I. Trends in alcohol consumption among older Americans: National Health Interview Surveys, 1997 to 2014. Alcohol. Clin. Exp. Res. 2017, 41, 976–986. [Google Scholar] [CrossRef] [PubMed]
- Comijs, H.; Aartsen, M.; Visser, M.; Deeg, D. Alcohol consumption among persons aged 55+ in The Netherlands. Tijdschr. Voor Gerontol. Geriatr. 2012, 43, 115–126. [Google Scholar] [CrossRef]
- Immonen, S.; Valvanne, J.; Pitkälä, K.H. Older adults’ own reasoning for their alcohol consumption. Int. J. Geriatr. Psychiatry 2011, 26, 1169–1176. [Google Scholar] [CrossRef]
- Dare, J.; Wilkinson, C.; Allsop, S.; Waters, S.; McHale, S. Social engagement, setting and alcohol use among a sample of older Australians. Health Soc. Care Community 2014, 22, 524–532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, B.H.; Moore, A.A. Prevention and screening of unhealthy substance use by older adults. Clin. Geriatr. Med. 2018, 34, 117–129. [Google Scholar] [CrossRef]
- Han, B.H.; Moore, A.A.; Sherman, S.; Keyes, K.M.; Palamar, J.J. Demographic trends of binge alcohol use and alcohol use disorders among older adults in the United States, 2005–2014. Drug Alcohol Depend. 2017, 170, 198–207. [Google Scholar] [CrossRef] [Green Version]
- Emiliussen, J.; Andersen, K.; Nielsen, A.S. Why do some older adults start drinking excessively late in life? Results from an interpretative phenomenological study. Scand. J. Caring Sci. 2017, 31, 974–983. [Google Scholar] [CrossRef] [Green Version]
- Canham, S.L.; Mauro, P.M.; Kaufmann, C.N.; Sixsmith, A. Association of alcohol use and loneliness frequency among middle-aged and older adult drinkers. J. Aging Health 2016, 28, 267–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalousova, L.; Burgard, S.A. Unemployment, measured and perceived decline of economic resources: Contrasting three measures of recessionary hardships and their implications for adopting negative health behaviors. Soc. Sci. Med. 2014, 106, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Calvo, E.; Allel, K.; Staudinger, U.; Castillo-Carniglia, Á.; Medina, J.; Keyes, K.; Butler, R. Cross-Country differences in age trends in alcohol consumption among older adults: A cross-sectional study of individuals aged 50 years and older in 22 countries. Addiction 2020, 116, 1399–1412. [Google Scholar] [CrossRef] [PubMed]
- Heuberger, R.A. Alcohol and the older adult: A comprehensive review. J. Nutr. Elder. 2009, 28, 203–235. [Google Scholar] [CrossRef] [PubMed]
- Bates, M.E.; Bowden, S.C.; Barry, D. Neurocognitive impairment associated with alcohol use disorders: Implications for treatment. Exp. Clin. Psychopharmacol. 2002, 10, 193–212. [Google Scholar] [CrossRef]
- Stein, M.D.; Friedmann, P.D. Disturbed sleep and its relationship to alcohol use. Subst. Abus. 2005, 26, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Chakravorty, S.; Chaudhary, N.S.; Brower, K.J. Alcohol dependence and its relationship with insomnia and other sleep disorders. Alcohol. Clin. Exp. Res. 2016, 40, 2271–2282. [Google Scholar] [CrossRef]
- Bain, K.T. Management of chronic insomnia in elderly persons. Am. J. Geriatr. Pharmacother. 2006, 4, 168–192. [Google Scholar] [CrossRef]
- 2019 American Geriatrics Society Beers Criteria® Update Expert Panel. American Geriatrics Society 2019 Updated AGS Beers Criteria® for Potentially Inappropriate Medication Use in Older Adults. J. Am. Geriatr. Soc. 2019, 67, 674–694. [Google Scholar] [CrossRef]
- Meier, E.; Miller, M.B.; Lombardi, N.; Leffingwell, T. Assessment reactivity: A randomized controlled trial of alcohol-specific measures on alcohol-related behaviors. Addict. Behav. 2017, 67, 44–48. [Google Scholar] [CrossRef] [Green Version]
- Pozzato, G.; Moretti, M.; Franzin, F.; Crocè, L.S.; Lacchin, T.; Benedetti, G.; Sablich, R.; Stebel, M.; Campanacci, L. Ethanol metabolism and aging: The role of “first pass metabolism” and gastric alcohol dehydrogenase activity. J. Gerontol. A Biol. Sci. Med. Sci. 1995, 50, B135–B141. [Google Scholar] [CrossRef] [PubMed]
- Moore, A.A.; Whiteman, E.J.; Ward, K.T. Risks of combined alcohol/medication use in older adults. Am. J. Geriatr. Pharmacother. 2007, 5, 64–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- United Nations. World Population Ageing 2019; United Nations: New York, NY, USA, 2020. [Google Scholar]
- Beyer, F.R.; Campbell, F.; Bertholet, N.; Daeppen, J.B.; Saunders, J.B.; Pienaar, E.D.; Muirhead, C.R.; Kaner, E.F.S. The Cochrane 2018 review on brief interventions in primary care for Hazardous and harmful alcohol consumption: A distillation for clinicians and policy makers. Alcohol Alcohol. 2019, 54, 417–427. [Google Scholar] [CrossRef] [PubMed]
- Kaner, E.F.S.; Beyer, F.R.; Muirhead, C.; Campbell, F.; Pienaar, E.D.; Bertholet, N.; Daeppen, J.B.; Saunders, J.B.; Burnand, B. Effectiveness of brief alcohol interventions in primary care populations. Cochrane Database Syst. Rev. 2018, 2. [Google Scholar] [CrossRef] [Green Version]
- Barrio, P.; Gual, A. Patient-Centered care interventions for the management of alcohol use disorders: A systematic review of randomized controlled trials. Patient Prefer. Adherence 2016, 10, 1823–1845. [Google Scholar] [CrossRef] [Green Version]
- Sundström, C.; Blankers, M.; Khadjesari, Z. Computer-Based interventions for problematic alcohol use: A review of systematic reviews. Int. J. Behav. Med. 2017, 24, 646–658. [Google Scholar] [CrossRef] [Green Version]
- Fowler, L.A.; Holt, S.L.; Joshi, D. Mobile technology-based interventions for adult users of alcohol: A systematic review of the literature. Addict. Behav. 2016, 62, 25–34. [Google Scholar] [CrossRef]
- Törrönen, J.; Roumeliotis, F.; Samuelsson, E.; Kraus, L.; Room, R. Why are young people drinking less than earlier? Identifying and specifying social mechanisms with a pragmatist approach. Int. J. Drug Policy 2019, 64, 13–20. [Google Scholar] [CrossRef]
- Kraus, L.; Room, R.; Livingston, M.; Pennay, A.; Holmes, J.; Törrönen, J. Long waves of consumption or a unique social generation? Exploring recent declines in youth drinking. Addict. Res. Theory 2020, 28, 183–193. [Google Scholar] [CrossRef]
- Armstrong-Moore, R.; Haighton, C.; Davinson, N.; Ling, J. Interventions to reduce the negative effects of alcohol consumption in older adults: A systematic review. BMC Public Health 2018, 18, 302. [Google Scholar] [CrossRef]
- Kelly, S.; Olanrewaju, O.; Cowan, A.; Brayne, C.; Lafortune, L. Interventions to prevent and reduce excessive alcohol consumption in older people: A systematic review and meta-analysis. Age Ageing 2018, 47, 175–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pawson, R.; Tilley, N. Realistic Evaluation; SAGE: London, UK, 1997. [Google Scholar]
- Westhorp, G.; Prins, E.; Kusters, C.; Hultink, M.; Guijt, I.M.; Brouwers, J. Realist Evaluation: An Overview Report from an Expert Seminar with Dr. Gill Westhorp; Wageninen UR Centre for Development Innovation: Wageningen, The Netherlands, 2011. [Google Scholar]
- World Health Organization. World Report on Ageing and Health; World Health Organization: Luxembourg, 2015. [Google Scholar]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; Group, P.-P. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, Q.N.; Gonzalez-Reyes, A.; Pluye, P. Improving the usefulness of a tool for appraising the quality of qualitative, quantitative and mixed methods studies, the Mixed Methods Appraisal Tool (MMAT). J. Eval. Clin. Pract. 2018, 24, 459–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ettner, S.L.; Xu, H.; Duru, O.K.; Ang, A.; Tseng, C.H.; Tallen, L.; Barnes, A.; Mirkin, M.; Ransohoff, K.; Moore, A.A. The effect of an educational intervention on alcohol consumption, at-risk drinking, and health care utilization in older adults: The Project SHARE study. J. Stud. Alcohol Drugs 2014, 75, 447–457. [Google Scholar] [CrossRef] [Green Version]
- Fink, A.; Elliott, M.N.; Tsai, M.; Beck, J.C. An evaluation of an intervention to assist primary care physicians in screening and educating older patients who use alcohol. J. Am. Geriatr. Soc. 2005, 53, 1937–1943. [Google Scholar] [CrossRef]
- Kuerbis, A.N.; Yuan, S.E.; Borok, J.; LeFevre, P.M.; Kim, G.S.; Lum, D.; Ramirez, K.D.; Liao, D.H.; Moore, A.A. Testing the initial efficacy of a mailed screening and brief feedback intervention to reduce at-risk drinking in middle-aged and older adults: The comorbidity alcohol risk evaluation study. J. Am. Geriatr. Soc. 2015, 63, 321–326. [Google Scholar] [CrossRef]
- Wiprovnick, A.E.; Kuerbis, A.N.; Morgenstern, J. The effects of therapeutic bond within a brief intervention for alcohol moderation for problem drinkers. Psychol. Addict. Behav. 2015, 29, 129–135. [Google Scholar] [CrossRef]
- Freyer-Adam, J.; Baumann, S.; Schnuerer, I.; Haberecht, K.; Bischof, G.; John, U.; Gaertner, B. Does stage tailoring matter in brief alcohol interventions for job-seekers? A randomized controlled trial. Addiction 2014, 109, 1845–1856. [Google Scholar] [CrossRef]
- Kirkman, J.J.L.; Leo, B.; Moore, J.C. Alcohol consumption reduction among a web-based supportive community using the hello sunday morning blog platform: Observational study. J. Med. Internet Res. 2018, 20, e9605. [Google Scholar] [CrossRef]
- Andréasson, S.; Hansagi, H.; Österlund, B. Short-Term treatment for alcohol-related problems: Four-Session guided self-change versus one session of advice—A randomized, controlled trial. Alcohol 2002, 28, 57–62. [Google Scholar] [CrossRef]
- Baumann, S.; Toft, U.; Aadahl, M.; Jørgensen, T.; Pisinger, C. The long-term effect of a population-based life-style intervention on smoking and alcohol consumption. The Inter99 Study—A randomized controlled trial. Addiction 2015, 110, 1853–1860. [Google Scholar] [CrossRef] [PubMed]
- Connors, G.; Maisto, S.; Schlauch, R.; Dearing, R.; Prince, M.; Duerr, M. Therapeutic alliances predict session by session drinking behavior in the treatment of alcohol use disorders. J. Consult. Clin. Psychol. 2016, 84, 972. [Google Scholar] [CrossRef] [PubMed]
- Csillik, A.; Osin, E.; Meyer, T. Comparative Evaluation of Motivational Interviewing Components in Alcohol Treatment. J. Contemp. Psychother. 2022, 52, 55–65. [Google Scholar] [CrossRef]
- Ilgen, M.A.; McKellar, J.; Moos, R.; Finney, J.W. Therapeutic alliance and the relationship between motivation and treatment outcomes in patients with alcohol use disorder. J. Subst. Abuse Treat. 2006, 31, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Karno, M.P.; Beutler, L.E.; Harwood, T.M. Interactions between psychotherapy procedures and patient attributes that predict alcohol treatment effectiveness: A preliminary report. Addict. Behav. 2002, 27, 779–797. [Google Scholar] [CrossRef]
- Kavanagh, D.; Connolly, J.M. Mailed treatment to augment primary care for alcohol disorders: A randomised controlled trial. Drug Alcohol. Rev. 2009, 28, 73–80. [Google Scholar] [CrossRef]
- Khan, N.S.; Norman, I.J.; Dhital, R.; McCrone, P.; Milligan, P.; Whittlesea, C.M. Alcohol brief intervention in community pharmacies: A feasibility study of outcomes and customer experiences. Int. J. Clin. Pharm. 2013, 35, 1178–1187. [Google Scholar] [CrossRef]
- Kiluk, B.D.; Devore, K.A.; Buck, M.B.; Nich, C.; Frankforter, T.L.; LaPaglia, D.M.; Yates, B.T.; Gordon, M.A.; Carroll, K.M. Randomized Trial of Computerized Cognitive Behavioral Therapy for Alcohol Use Disorders: Efficacy as a Virtual Stand-Alone and Treatment Add-On Compared with Standard Outpatient Treatment. Alcohol. Clin. Exp. Res. 2016, 40, 1991–2000. [Google Scholar] [CrossRef] [Green Version]
- Kingree, J.B.; Thompson, M. Participation in Alcoholics Anonymous and post-treatment abstinence from alcohol and other drugs. Addict. Behav. 2011, 36, 882–885. [Google Scholar] [CrossRef]
- Mowbray, O.; Krentzman, A.R.; Bradley, J.C.; Cranford, J.A.; Robinson, E.A.; Grogan-Kaylor, A. The effect of drinking goals at treatment entry on longitudinal alcohol use patterns among adults with alcohol dependence. Drug Alcohol Depend. 2013, 132, 182–188. [Google Scholar] [CrossRef] [Green Version]
- Nielsen, A.S.; Nielsen, B. Improving Outpatient Alcohol Treatment Systems: Integrating Focus on Motivation and Actuarial Matching. Alcohol. Treat. Q. 2018, 36, 373–386. [Google Scholar] [CrossRef] [Green Version]
- Orford, J.; Hodgson, R.; Copello, A.; John, B.; Smith, M.; Black, R.; Fryer, K.; Handforth, L.; Alwyn, T.; Kerr, C.; et al. The clients’ perspective on change during treatment for an alcohol problem: Qualitative analysis of follow-up interviews in the UK Alcohol Treatment Trial. Addiction 2006, 101, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Orford, J.; Hodgson, R.; Copello, A.; Wilton, S.; Slegg, G. To what factors do clients attribute change? Content analysis of follow-up interviews with clients of the UK Alcohol Treatment Trial. J. Subst. Abuse Treat. 2009, 36, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Richardson, D.; Adamson, S.; Deering, D. The Role of Therapeutic Alliance in Treatment for People with Mild to Moderate Alcohol Dependence. Int. J. Ment. Health Addict. 2011, 10, 597–606. [Google Scholar] [CrossRef]
- UKATT Research Team. Effectiveness of treatment for alcohol problems: Findings of the randomised UK alcohol treatment trial (UKATT). BMJ 2005, 331, 541–544. [Google Scholar] [CrossRef] [Green Version]
- Walitzer, K.S.; Dermen, K.H. Alcohol-Focused spouse involvement and behavioral couples therapy: Evaluation of enhancements to drinking reduction treatment for male problem drinkers. J. Consult. Clin. Psychol. 2004, 72, 944–955. [Google Scholar] [CrossRef]
- Best, D.; Hall, K.; Guthrie, A.; Abbatangelo, M.; Hunter, B.; Lubman, D. Development and Implementation of a Structured Intervention for Alcohol Use Disorders for Telephone Helpline Services. Alcohol. Treat. Q. 2015, 33, 118–131. [Google Scholar] [CrossRef] [Green Version]
- Bischof, G.; Grothues, J.M.; Reinhardt, S.; Meyer, C.; John, U.; Rumpf, H.J. Evaluation of a telephone-based stepped care intervention for alcohol-related disorders: A randomized controlled trial. Drug Alcohol Depend. 2008, 93, 244–251. [Google Scholar] [CrossRef]
- Blankers, M.; Koeter, M.W.; Schippers, G.M. Internet therapy versus internet self-help versus no treatment for problematic alcohol use: A randomized controlled trial. J. Consult. Clin. Psychol. 2011, 79, 330–341. [Google Scholar] [CrossRef] [Green Version]
- Brown, R.; Saunders, L.; Bobula, J.; Mundt, M.; Koch, P. Randomized-Controlled Trial of a Telephone and Mail Intervention for Alcohol Use Disorders: Three-Month Drinking Outcomes. Alcohol. Clin. Exp. Res. 2007, 31, 1372–1379. [Google Scholar] [CrossRef]
- Clifford, P.R.; Maisto, S.A.; Davis, C.M. Alcohol treatment research assessment exposure subject reactivity effects: Part I. Alcohol use and related consequences. J. Stud. Alcohol Drugs 2007, 68, 519–528. [Google Scholar] [CrossRef] [PubMed]
- Postel, M.G.; ter Huurne, E.D.; de Haan, H.A.; van der Palen, J.; de Jong, C.A. A 9-month follow-up of a 3-month web-based alcohol treatment program using intensive asynchronous therapeutic support. Am. J. Drug Alcohol Abuse 2015, 41, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Doyle, M.; Carr, A.; Rowen, S.; Galvin, P.; Lyons, S.; Cooney, G. Family–Oriented treatment for people with alcohol problems in Ireland: A comparison of the effectiveness of residential and community–based programmes. J. Fam. Ther. 2003, 25, 15–40. [Google Scholar] [CrossRef] [Green Version]
- McCrady, B.S.; Hayaki, J.; Epstein, E.E.; Hirsch, L.S. Testing hypothesized predictors of change in conjoint behavioral alcoholism treatment for men. Alcohol. Clin. Exp. Res. 2002, 26, 463–470. [Google Scholar] [CrossRef]
- McCrady, B.S.; Epstein, E.E.; Cook, S.; Jensen, N.; Hildebrandt, T. A randomized trial of individual and couple behavioral alcohol treatment for women. J. Consult. Clin. Psychol. 2009, 77, 243–256. [Google Scholar] [CrossRef] [Green Version]
- Rentscher, K.E.; Soriano, E.C.; Rohrbaugh, M.J.; Shoham, V.; Mehl, M.R. Partner pronoun use, communal coping, and abstinence during couple-focused intervention for problematic alcohol use. Fam. Process 2017, 56, 348–363. [Google Scholar] [CrossRef]
- Schumm, J.A.; O’Farrell, T.J.; Kahler, C.W.; Murphy, M.M.; Muchowski, P. A randomized clinical trial of behavioral couples therapy versus individually based treatment for women with alcohol dependence. J. Consult. Clin. Psychol. 2014, 82, 993–1004. [Google Scholar] [CrossRef] [Green Version]
- Vedel, E.; Emmelkamp, P.M.; Schippers, G.M. Individual cognitive-behavioral therapy and behavioral couples therapy in alcohol use disorder: A comparative evaluation in community-based addiction treatment centers. Psychother. Psychosom. 2008, 77, 280–288. [Google Scholar] [CrossRef]
- Bamford, Z.; Booth, P.G.; McGuire, J.; Salmon, P. Treatment outcome following day care for alcohol dependency: The effects of reducing programme length. Health Soc. Care Community 2003, 11, 440–445. [Google Scholar] [CrossRef]
- Brown, T.G.; Dongier, M.; Latimer, E.; Legault, L.; Seraganian, P.; Kokin, M.; Ross, D. Group-Delivered Brief Intervention versus Standard Care for Mixed Alcohol/Other Drug Problems. Alcohol. Treat. Q. 2007, 24, 23–40. [Google Scholar] [CrossRef]
- Gómez-Recasens, M.; Alfaro-Barrio, S.; Tarro, L.; Llauradó, E.; Solà, R. A workplace intervention to reduce alcohol and drug consumption: A nonrandomized single-group study. BMC Public Health 2018, 18, 1281. [Google Scholar] [CrossRef] [PubMed]
- Hagger, M.S.; Lonsdale, A.; Chatzisarantis, N.L. Effectiveness of a brief intervention using mental simulations in reducing alcohol consumption in corporate employees. Psychol. Health Med. 2011, 16, 375–392. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, G.S.; Bennett, J.B. A cluster randomized trial of alcohol prevention in small businesses: A cascade model of help seeking and risk reduction. Am. J. Health Promot. 2015, 29, 182–191. [Google Scholar] [CrossRef]
- Toft, U.; Pisinger, C.; Aadahl, M.; Lau, C.; Linneberg, A.; Ladelund, S.; Kristoffersen, L.; Jørgensen, T. The impact of a population-based multi-factorial lifestyle intervention on alcohol intake: The Inter99 study. Prev. Med. 2009, 49, 115–121. [Google Scholar] [CrossRef]
- Augsburger, M.; Kaal, E.; Ülesoo, T.; Wenger, A.; Blankers, M.; Haug, S.; Ebert, D.D.; Riper, H.; Keough, M.; Noormets, H.; et al. Effects of a minimal-guided on-line intervention for alcohol misuse in Estonia: A randomized controlled trial. Addiction 2022, 117, 108–117. [Google Scholar] [CrossRef] [PubMed]
- Baumann, S.; Gaertner, B.; Haberecht, K.; Bischof, G.; John, U.; Freyer-Adam, J. Who benefits from computer-based brief alcohol intervention? Day-to-day drinking patterns as a moderator of intervention efficacy. Drug Alcohol Depend. 2017, 175, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Bagnardi, V.; Sorini, E.; Disalvatore, D.; Assi, V.; Corrao, G.; De Stefani, R. ‘Alcohol, Less is Better’ project: Outcomes of an Italian community-based prevention programme on reducing per-capita alcohol consumption. Addiction 2011, 106, 102–110. [Google Scholar] [CrossRef] [PubMed]
- Connors, G.J.; Walitzer, K.S.; Prince, M.A.; Kubiak, A. Secondary prevention of alcohol problems in rural areas using a bibliotherapy-based approach. J. Rural Ment. Health 2017, 41, 162–173. [Google Scholar] [CrossRef]
- Cunningham, J.A.; Sdao-Jarvie, K.; Koski-Jännes, A.; Breslin, F.C. Using self-help materials to motivate change at assessment for alcohol treatment. J. Subst. Abus. Treat. 2001, 20, 301–304. [Google Scholar] [CrossRef]
- Cunningham, J.A.; Wild, T.C.; Cordingley, J.; van Mierlo, T.; Humphreys, K. A randomized controlled trial of an internet-based intervention for alcohol abusers. Addiction 2009, 104, 2023–2032. [Google Scholar] [CrossRef]
- Cunningham, J.A.; Murphy, M.; Hendershot, C.S. Treatment dismantling pilot study to identify the active ingredients in personalized feedback interventions for hazardous alcohol use: Randomized controlled trial. Addict. Sci. Clin. Pract. 2014, 10, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dulin, P.L.; Gonzalez, V.M.; Campbell, K. Results of a pilot test of a self-administered smartphone-based treatment system for alcohol use disorders: Usability and early outcomes. Subst. Abus. 2014, 35, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Giroux, D.; Bacon, S.; King, D.K.; Dulin, P.; Gonzalez, V. Examining perceptions of a smartphone-based intervention system for alcohol use disorders. Telemed. J. E-Health 2014, 20, 923–929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonzalez, V.M.; Dulin, P.L. Comparison of a smartphone app for alcohol use disorders with an Internet-based intervention plus bibliotherapy: A pilot study. J. Consult. Clin. Psychol. 2015, 83, 335–345. [Google Scholar] [CrossRef] [PubMed]
- Guillemont, J.; Cogordan, C.; Nalpas, B.; Nguyen-Thanh, V.; Richard, J.B.; Arwidson, P. Effectiveness of a web-based intervention to reduce alcohol consumption among French hazardous drinkers: A randomized controlled trial. Health Educ. Res. 2017, 32, 332–342. [Google Scholar] [CrossRef]
- Koffarnus, M.N.; Bickel, W.K.; Kablinger, A.S. Remote Alcohol Monitoring to Facilitate Incentive-Based Treatment for Alcohol Use Disorder: A Randomized Trial. Alcohol. Clin. Exp. Res. 2018, 42, 2423–2431. [Google Scholar] [CrossRef] [Green Version]
- Lockwood, N.; de Visser, R.; Larsen, J. “Have a little less, feel a lot better”: Mixed-Method evaluation of an alcohol intervention. Addict. Behav. Rep. 2020, 12, 100306. [Google Scholar] [CrossRef]
- Moody, L.N.; Tegge, A.N.; Poe, L.M.; Koffarnus, M.N.; Bickel, W.K. To drink or to drink less? Distinguishing between effects of implementation intentions on decisions to drink and how much to drink in treatment-seeking individuals with alcohol use disorder. Addict. Behav. 2018, 83, 64–71. [Google Scholar] [CrossRef]
- Nygaard, P. Intervention in social networks: A new method in the prevention of alcohol-related problems. Addict. Res. Theory 2001, 9, 221–237. [Google Scholar] [CrossRef]
- Van Lettow, B.; de Vries, H.; Burdorf, A.; Boon, B.; van Empelen, P. Drinker prototype alteration and cue reminders as strategies in a tailored web-based intervention reducing adults’ alcohol consumption: Randomized controlled trial. J. Med. Internet Res. 2015, 17, e3551. [Google Scholar] [CrossRef] [Green Version]
- Tait, R.J.; Paz Castro, R.; Kirkman, J.J.L.; Moore, J.C.; Schaub, M.P. A digital intervention addressing alcohol use problems (the “Daybreak” program): Quasi-Experimental randomized controlled trial. J. Med. Internet Res. 2019, 21, e14967. [Google Scholar] [CrossRef] [PubMed]
- Zill, J.; Christalle, E.; Meyer, B.; Härter, M.; Dirmaier, J. The Effectiveness of an Internet Intervention Aimed at Reducing Alcohol Consumption in Adults. Dtsch. Aerzteblatt Online 2019, 116, 127. [Google Scholar] [CrossRef] [PubMed]
- Black, N.; Loomes, M.; Juraskova, I.; Johnston, I. Engagement in a Novel Internet Intervention for Alcohol Reduction: A Qualitative Study of User Motivations and Experiences. Cyberpsychol. Behav. Soc. Netw. 2020, 23, 225–233. [Google Scholar] [CrossRef] [PubMed]
- Haug, N.A.; Morimoto, E.E.; Lembke, A. Online mutual-help intervention for reducing heavy alcohol use. J. Addict. Dis. 2020, 38, 241–249. [Google Scholar] [CrossRef]
- McCrady, B.S. To have but one true friend: Implications for practice of research on alcohol use disorders and social network. Psychol. Addict. Behav. 2004, 18, 113–121. [Google Scholar] [CrossRef]
- Witkiewitz, K.; Marlatt, G.A. Relapse prevention for alcohol and drug problems: That was Zen, this is Tao. Am. Psychol. 2004, 59, 224–235. [Google Scholar] [CrossRef] [Green Version]
- Robinson, C.S.H.; Fokas, K.; Witkiewitz, K. Relationship between empathic processing and drinking behavior in project MATCH. Addict. Behav. 2018, 77, 180–186. [Google Scholar] [CrossRef]
- White, A.; Kavanagh, D.; Stallman, H.; Klein, B.; Kay-Lambkin, F.; Proudfoot, J.; Drennan, J.; Connor, J.; Baker, A.; Hines, E.; et al. Online Alcohol Interventions: A Systematic Review. J. Med. Internet Res. 2010, 12, e62. [Google Scholar] [CrossRef] [Green Version]
- Riper, H.; van Straten, A.; Keuken, M.; Smit, F.; Schippers, G.; Cuijpers, P. Curbing Problem Drinking with Personalized-Feedback Interventions: A Meta-Analysis. Am. J. Prev. Med. 2009, 36, 247–255. [Google Scholar] [CrossRef]
- Pinquart, M.; Sorensen, S. Influences on Loneliness in Older Adults: A Meta-Analysis. Basic Appl. Soc. Psychol. 2001, 23, 245–266. [Google Scholar] [CrossRef]
- Canham, S.L.; Mauro, P.M.; Kaufmann, C.N. Alcohol consumption and loneliness in mid- and late-life. Drug Alcohol Depend. 2015, 146, e238. [Google Scholar] [CrossRef]
- Purser, G.L. The Combined Effect of Functional Independence, Loneliness, and Social Engagement on Older Adult Drinking Levels. J. Soc. Work. Pract. Addict. 2020, 1–12. [Google Scholar] [CrossRef]

| Database | Limits |
|---|---|
| PsycINFO | Peer-reviewed journals, age group: adulthood 18+, English, Dutch, years 2000–2022 |
| Web of Science (WOS) | Articles, publication years 2000–2022, English, Dutch 1 |
| PubMed | Adult: 19+ years, 2 publication years 2000–2022, English, Dutch |
| CINAHL | Peer-reviewed, publication years 2000–2022, English, Dutch 1 |
| Group 1 Alcohol |
| alcohol or “alcohol consumption” |
| Group 2 Older adults |
| elder or elderly or senior or old or pension or retire or retirement or “later life” or geriatric or geriatrics or “older adults” or ageing or aging or gerontology or aged |
| Group 3 Reduction |
| intervention or treatment or reduction |
| Group 4 Prevention |
| prevent or prevention or preventing |
| Group 5 Not child |
| NOT child or “young adult” or teenage or adolescent |
| Search Questions | Groups of Keywords |
|---|---|
| What are the effective elements of interventions for the general population with regard to reducing (problematic) alcohol consumption? | 1 (title) and 3 (title) not 5 (only for WOS (topic) and CINAHL (title)) |
| What are the effective elements of interventions for older adults (55+) with regard to reducing (problematic) alcohol consumption? | 1 (title) and 2 (title) and 3 (PsycINFO (abstract), WOS (topic), PubMed (title/abstract), CINAHL (abstract)) |
| What are the effective elements of interventions for the general population with regard to the prevention of (problematic) alcohol consumption? | 1 (title) and 4 (title) not 5 (only for WOS (topic) and CINAHL (title)) |
| What are the effective elements of interventions for older adults (55+) with regard to the prevention of (problematic) alcohol consumption? | 1 (title) and 2 (title) and 4 (PsycINFO (abstract), WOS (topic), PubMed (title/abstract), CINAHL (abstract)) |
| Context | Element of Intervention (How) | Mechanism (Why) | Outcome |
|---|---|---|---|
| A. Practitioner—in-person—individual | Paying attention to drinking behavior
| Interventions make people think and act differently about alcohol consumption and seek help from family and friends | Less or no alcohol consumption |
The relationship between the patient and practitioner
| Patient and practitioner collaborate in the identification of additional sessions, judged best to meet the patient’s clinical needs and the relationship between the patient and the therapist improves | Less or no alcohol consumption | |
| B. Practitioner—not in-person—individual | Personal contact and feedback
| - | Less or no alcohol consumption |
Online communication and feedback
| |||
| C. Practitioner—in-person—relatives | The status of the relationship | - | Less or no alcohol consumption |
| Teaching the partner to deal with drinking behavior | When the non-drinking partner is taught to deal with the behavior of the drinking partner, this can lead to more understanding and support from the non-drinking partner for the drinking partner. | ||
| D. Practitioner—in-person—group component | Motivating to change lifestyle
| - | Less or no alcohol consumption |
Motivating to change lifestyle delivered in a workplace setting
| |||
| E. No practitioner—not in-person—individual. | Web based interventions
| - | Less or no alcohol consumption |
Telephone based interventions
| Mobile phone interventions could provide insight into how much someone drinks through the information provided and this leads to realization of their own drinking behavior | ||
| F. No practitioner—not in-person—group component | Intervention to abstinent people
| Intervention to abstinent people (with or without problematic drinking behavior (1) from drinking alcohol for a certain period or to drink less and (2) to share this experience with peers makes people aware of their alcohol consumption and reduces alcohol consumption. | Less or no alcohol consumption |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boumans, J.; van de Mheen, D.; Crutzen, R.; Dupont, H.; Bovens, R.; Rozema, A. Understanding How and Why Alcohol Interventions Prevent and Reduce Problematic Alcohol Consumption among Older Adults: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 3188. https://doi.org/10.3390/ijerph19063188
Boumans J, van de Mheen D, Crutzen R, Dupont H, Bovens R, Rozema A. Understanding How and Why Alcohol Interventions Prevent and Reduce Problematic Alcohol Consumption among Older Adults: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(6):3188. https://doi.org/10.3390/ijerph19063188
Chicago/Turabian StyleBoumans, Jogé, Dike van de Mheen, Rik Crutzen, Hans Dupont, Rob Bovens, and Andrea Rozema. 2022. "Understanding How and Why Alcohol Interventions Prevent and Reduce Problematic Alcohol Consumption among Older Adults: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 6: 3188. https://doi.org/10.3390/ijerph19063188