
The Relationship between Mindfulness and Emotional Intelligence as a Protective Factor for Healthcare Professionals: Systematic Review

 , , , , and
, , , , and
Abstract
:1. Introduction
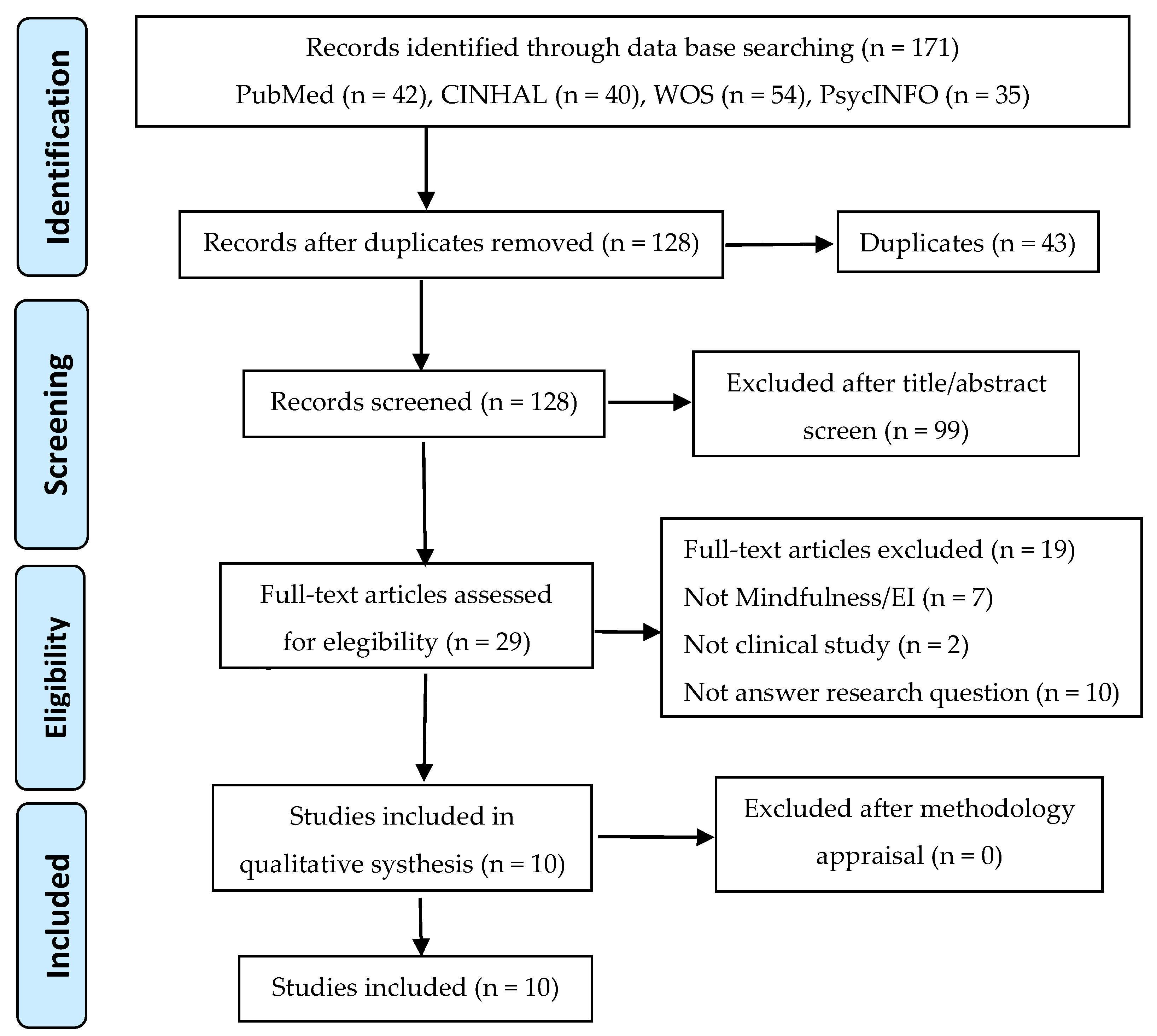
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Mayer, J.D.; Salovey, P.; Caruso, D.R.; Sitarenios, G. Emotional Intelligence as a Standard Intelligence. Emotion 2001, 1, 232–242. [Google Scholar] [CrossRef]
- Mayer, J.D.; Salovey, P.; Caruso, D.R.; Sitarenios, G. Measuring emotional intelligence with the MSCEIT V2.0. Emotion 2003, 3, 97–105. [Google Scholar] [CrossRef] [Green Version]
- Ruíz, V.M. Habilidades para la Vida: Una Propuesta de Formación Humana. Itiner. Educ. 2014, 28, 61. [Google Scholar] [CrossRef]
- Nightingale, S.; Spiby, H.; Sheen, K.; Slade, P. The Impact of Emotional Intelligence in Health Care Professionals on Caring Behaviour towards Patients in Clinical and Long-Term Care Settings: Findings from an Integrative Review. Int. J. Nurs. Stud. 2018, 80, 106–117. [Google Scholar] [CrossRef]
- Cox, K.M. Use of Emotional Intelligence to Enhance Advanced Practice Registered Nursing Competencies. J. Nurs. Educ. 2018, 57, 648–654. [Google Scholar] [CrossRef]
- Hutchinson, M.; Hurley, J.; Kozlowski, D.; Whitehair, L. The Use of Emotional Intelligence Capabilities in Clinical Reasoning and Decision-Making: A Qualitative, Exploratory Study. J. Clin. Nurs. 2018, 27, e600–e610. [Google Scholar] [CrossRef] [PubMed]
- Szczygiel, D.D.; Mikolajczak, M. Emotional Intelligence Buffers the Effects of Negative Emotions on Job Burnout in Nursing. Front. Psychol. 2018, 9, 2649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Looff, P.; Nijman, H.; Didden, R.; Embregts, P. Burnout Symptoms in Forensic Psychiatric Nurses and Their Associations with Personality, Emotional Intelligence and Client Aggression: A Cross-Sectional Study. J. Psychiatr. Ment. Health Nurs. 2018, 25, 506–516. [Google Scholar] [CrossRef]
- Molero Jurado, M.D.M.; Pérez-Fuentes, M.D.C.; Gázquez Linares, J.J.G.; Simón Márquez, M.D.M.; Martos Martínez, Á. Burnout Risk and Protection Factors in Certified Nursing Aides. Int. J. Environ. Res. Public Health 2018, 15, 1116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pérez-Fuentes, M.D.C.; Molero Jurado, M.D.M.; Gázquez Linares, J.J.; Oropesa Ruiz, N.F. The Role of Emotional Intelligence in Engagement in Nurses. Int. J. Environ. Res. Public Health 2018, 15, 1915. [Google Scholar] [CrossRef]
- Al-Hamdan, Z.; Oweidat, I.A.; Al-Faouri, I.; Codier, E. Correlating Emotional Intelligence and Job Performance Among Jordanian Hospitals’ Registered Nurses. Nurs. Forum 2017, 52, 12–20. [Google Scholar] [CrossRef]
- Beydler, K.W. The Role of Emotional Intelligence in Perioperative Nursing and Leadership: Developing Skills for Improved Performance. AORN J. 2017, 106, 317–323. [Google Scholar] [CrossRef]
- Sommaruga, M.; Casu, G.; Giaquinto, F.; Gremigni, P. Self-Perceived Provision of Patient Centered Care by Healthcare Professionals: The Role of Emotional Intelligence and General Self-Efficacy. Patient Educ. Couns. 2017, 100, 974–980. [Google Scholar] [CrossRef]
- Dafeeah, E.E.; Eltohami, A.A.; Ghuloum, S. Emotional Intelligence and Attitudes toward HIV/AIDS Patients among Healthcare Professionals in the State of Qatar. Int. Perspect. Psychol. Res. Pract. Consult. 2015, 4, 19–36. [Google Scholar] [CrossRef]
- Cassano, F.; Tamburrano, A.; Mellucci, C.; Galletti, C.; Damiani, G.; Laurenti, P. Evaluation of Emotional Intelligence among Master’s Degree Students in Nursing and Midwifery: A Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2020, 17, 6347. [Google Scholar] [CrossRef]
- del Carmen Giménez-Espert, M.; Valero-Moreno, S.; Prado-Gascó, V.J. Evaluation of Emotional Skills in Nursing Using Regression and QCA Models: A Transversal Study. Nurse Educ. Today 2019, 74, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Kim, S.; Byun, M.K. Emotional Distancing in Nursing: A Concept Analysis. Nurs. Forum 2020. [Google Scholar] [CrossRef]
- López-Cabarcos, M.Á.; López-Carballeira, A.; Ferro-Soto, C. The Role of Emotional Exhaustion among Public Healthcare Professionals. J. Health Organ. Manag. 2019, 33, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Xu, S.; Ouyang, X.; Shi, X.; Li, Y.; Chen, D.; Lai, Y.; Fan, F. Emotional Exhaustion and Sleep-Related Worry as Serial Mediators between Sleep Disturbance and Depressive Symptoms in Student Nurses: A Longitudinal Analysis. J. Psychosom. Res. 2020, 129. [Google Scholar] [CrossRef]
- Panari, C.; Caricati, L.; Pelosi, A.; Rossi, C. Emotional Exhaustion among Healthcare Professionals: The Effects of Role Ambiguity, Work Engagement and Professional Commitment. Acta Biomed. 2019, 90, 60–67. [Google Scholar] [CrossRef]
- Han, S.S.; Han, J.W.; An, Y.S.; Lim, S.H. Effects of Role Stress on Nurses’ Turnover Intentions: The Mediating Effects of Organizational Commitment and Burnout. Jpn. J. Nurs. Sci. 2015, 12, 287–296. [Google Scholar] [CrossRef]
- Yoon, J.D.; Rasinski, K.A.; Curlin, F.A. Conflict and Emotional Exhaustion in Obstetrician-Gynaecologists: A National Survey. J. Med. Ethics 2010, 36, 731–735. [Google Scholar] [CrossRef] [Green Version]
- Vásquez-Dextre, E.R. Mindfulness: Conceptos Generales, Psicoterapia y Aplicaciones Clínicas. Rev. Neuro Psiquiatr. 2016, 79, 42. [Google Scholar] [CrossRef]
- Zhou, B.; Wang, G.; Hong, Y.; Xu, S.; Wang, J.; Yu, H.; Liu, Y.; Yu, L. Mindfulness Interventions for Rheumatoid Arthritis: A Systematic Review and Meta-Analysis. Complementary Ther. Clin. Pract. 2020, 39, 101088. [Google Scholar] [CrossRef]
- Xie, C.; Dong, B.; Wang, L.; Jing, X.; Wu, Y.; Lin, L.; Tian, L. Mindfulness-Based Stress Reduction Can Alleviate Cancer- Related Fatigue: A Meta-Analysis. J. Psychosom. Res. 2020, 130, 109916. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Wang, H.; Luo, J.; Guo, Y.; Xie, Y.; Lei, B.; Wiley, J.; Whittemore, R. Factors Influencing the Effect of Mindfulness-Based Interventions on Diabetes Distress: A Meta-Analysis. BMJ Open Diabetes Res. Care 2019, 7, e000757. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simpson, R.; Simpson, S.; Ramparsad, N.; Lawrence, M.; Booth, J.; Mercer, S.W. Effects of Mindfulness-Based Interventions on Physical Symptoms in People with Multiple Sclerosis—A Systematic Review and Meta-Analysis. Mult. Scler. Relat. Disord. 2020, 38, 101493. [Google Scholar] [CrossRef]
- Xunlin, N.; Lau, Y.; Klainin-Yobas, P. The Effectiveness of Mindfulness-Based Interventions among Cancer Patients and Survivors: A Systematic Review and Meta-Analysis. Support. Care Cancer 2020, 28, 1563–1578. [Google Scholar] [CrossRef] [PubMed]
- Syed, I.U.B. Diet, physical activity, and emotional health: What works, what doesn’t, and why we need integrated solutions for total worker health. BMC Public Health 2020, 31, 152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pronk, N.P.; Katz, A.S.; Gallagher, J.; Austin, E.; Mullen, D.; Lowry, M.; Kottke, T.E. Adherence to optimal lifestyle behaviors is related to emotional health indicators among employees. Popul. Health Manag. 2011, 14, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Hunter, L. Making Time and Space: The Impact of Mindfulness Training on Nursing and Midwifery Practice. A Critical Interpretative Synthesis. J. Clin. Nurs. 2016, 25, 918–929. [Google Scholar] [CrossRef] [Green Version]
- Halm, M. The Role of Mindfulness in Enhancing Self-Care for Nurses. Am. J. Crit. Care 2017, 26, 344–348. [Google Scholar] [CrossRef]
- Burton, A.; Burgess, C.; Dean, S.; Koutsopoulou, G.Z.; Hugh-Jones, S. How Effective Are Mindfulness-Based Interventions for Reducing Stress Among Healthcare Professionals? A Systematic Review and Meta-Analysis. Stress Health 2017, 33, 3–13. [Google Scholar] [CrossRef]
- Ruiz-Fernández, M.D.; Ortíz-Amo, R.; Ortega-Galán, Á.M.; Ibáñez-Masero, O.; Rodríguez-Salvador, M.d.M.; Ramos-Pichardo, J.D. Mindfulness Therapies on Health Professionals. Int. J. Ment. Health Nurs. 2020, 29, 127–140. [Google Scholar] [CrossRef] [PubMed]
- Botha, E.; Gwin, T.; Purpora, C. The Effectiveness of Mindfulness Based Programs in Reducing Stress Experienced by Nurses in Adult Hospital Settings: A Systematic Review of Quantitative Evidence Protocol. JBI Database Syst. Rev. Implement. Rep. 2015, 13, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Gómez del Pulgar, E.; Meléndez Moreno, A. Mindfulness, Prevención y Control Del Síndrome de Desgaste Profesional En La Enfermería Española. Rev. Enferm. Trab. 2017, 7, 70–75. [Google Scholar]
- Suleiman-Martos, N.; Gomez-Urquiza, J.L.; Aguayo-Estremera, R.; Cañadas-De La Fuente, G.A.; de La Fuente-Solana, E.I.; Albendín-García, L. The Effect of Mindfulness Training on Burnout Syndrome in Nursing: A Systematic Review and Meta-analysis. J. Adv. Nurs. 2020, 76, 1124–1140. [Google Scholar] [CrossRef]
- Guillaumie, L.; Boiral, O.; Champagne, J. A Mixed-Methods Systematic Review of the Effects of Mindfulness on Nurses. J. Adv. Nurs. 2017, 73, 1017–1034. [Google Scholar] [CrossRef]
- Walker, M.; Mann, R.A. Exploration of Mindfulness in Relation to Compassion, Empathy and Reflection within Nursing Education. Nurse Educ. Today 2016, 40, 188–190. [Google Scholar] [CrossRef]
- van der Riet, P.; Levett-Jones, T.; Aquino-Russell, C. The Effectiveness of Mindfulness Meditation for Nurses and Nursing Students: An Integrated Literature Review. Nurse Educ. Today 2018, 65, 201–211. [Google Scholar] [CrossRef]
- Sumner, J. Reflection and Moral Maturity in a Nurse’s Caring Practice: A Critical Perspective. Nurs. Philos. 2010, 11, 159–169. [Google Scholar] [CrossRef] [PubMed]
- Solsona de la Serna, E.; Pujol, J.; Llistar, S.; Barbera, E.; Giménez, N. Técnicas Actorales e Inteligencia Emocional Para Profesionales de La Salud: Aprendizaje Transformacional. Index Enferm. 2015, 24, 240–244. [Google Scholar] [CrossRef]
- Codier, E.; Freitas, B.; Muneno, L. Developing Emotional Intelligence Ability in Oncology Nurses: A Clinical Rounds Approach. Oncol. Nurs. Forum 2013, 40, 22–29. [Google Scholar] [CrossRef]
- Bamberger, E.; Genizi, J.; Kerem, N.; Reuven-Lalung, A.; Dolev, N.; Srugo, I.; Rofe, A. A Pilot Study of an Emotional Intelligence Training Intervention for a Paediatric Team. Arch. Dis. Child. 2017, 102, 159–164. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015 Statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Eriksen, M.B.; Frandsen, T.F. The impact of patient, intervention, comparison, outcome (PICO) as a search strategy tool on literature search quality: A systematic review. J. Med. Libr. Assoc. 2018, 106, 420–431. [Google Scholar] [CrossRef] [PubMed]
- Carlock, D.; Anderson, J. Teaching and assessing the database searching skills of student nurses. Nurse Educ. 2007, 32, 251–255. [Google Scholar] [CrossRef] [PubMed]
- Urbizagástegui Alvarado, R. Synchronic study of literature obsolescence: The case of Lotka’s Law. Investig. Bibl. 2014, 28, 85–113. [Google Scholar]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetc, R.; Currie, M.; Lisy, K.; Qureshi, R.; Mattis, P.; et al. Chapter 7: Systematic Reviews of Etiology and Risk. In JBI Manual for Evidence Synthesis; JBI: Adelaide, Australia, 2020. [Google Scholar]
- Vongareesawat, C.; Thapinta, D.; Disayavanish, C.; Anders, R.L.; Tungpunkom, P. Effect of Insight Meditation on Enhancing Emotional Intelligence among Thai Psychiatric Nurses. Chiang Mai Univ. J. Nat. Sci. 2012, 11, 61–75. [Google Scholar]
- Snowden, A.; Stenhouse, R.; Duers, L.; Marshall, S.; Carver, F.; Brown, N.; Young, J. The Relationship between Emotional Intelligence, Previous Caring Experience and Successful Completion of a Pre-Registration Nursing/Midwifery Degree. J. Adv. Nurs. 2018, 74, 433–442. [Google Scholar] [CrossRef] [Green Version]
- Dubert, C.J.; Schumacher, A.M.; Locker, L.; Gutierrez, A.P.; Barnes, V.A. Mindfulness and Emotion Regulation among Nursing Students: Investigating the Mediation Effect of Working Memory Capacity. Mindfulness 2016, 7, 1061–1070. [Google Scholar] [CrossRef]
- Jacobs, I.; Wollny, A.; Sim, C.W.; Horsch, A. Mindfulness Facets, Trait Emotional Intelligence, Emotional Distress, and Multiple Health Behaviors: A Serial Two-Mediator Model. Scand. J. Psychol. 2016, 57, 207–214. [Google Scholar] [CrossRef]
- Orellana-Rios, C.L.; Radbruch, L.; Kern, M.; Regel, Y.U.; Anton, A.; Sinclair, S.; Schmidt, S. Mindfulness and Compassion-Oriented Practices at Work Reduce Distress and Enhance Self-Care of Palliative Care Teams: A Mixed-Method Evaluation of an “on the Job” Program. BMC Palliat. Care 2017, 17. [Google Scholar] [CrossRef]
- Kelm, D.J.; Ridgeway, J.L.; Gas, B.L.; Mohan, M.; Cook, D.A.; Nelson, D.R.; Benzo, R.P. Mindfulness Meditation and Interprofessional Cardiopulmonary Resuscitation: A Mixed-Methods Pilot Study. Teach. Learn. Med. 2018, 30, 433–443. [Google Scholar] [CrossRef]
- Lamothe, M.; McDuff, P.; Pastore, Y.D.; Duval, M.; Sultan, S. Developing Professional Caregivers’ Empathy and Emotional Competencies through Mindfulness-Based Stress Reduction (MBSR): Results of Two Proof-of-Concept Studies. BMJ Open 2018, 8, e018421. [Google Scholar] [CrossRef] [Green Version]
- Salvarani, V.; Rampoldi, G.; Ardenghi, S.; Bani, M.; Blasi, P.; Ausili, D.; di Mauro, S.; Strepparava, M.G. Protecting Emergency Room Nurses from Burnout: The Role of Dispositional Mindfulness, Emotion Regulation and Empathy. J. Nurs. Manag. 2019, 27, 765–774. [Google Scholar] [CrossRef] [PubMed]
- Salvarani, V.; Ardenghi, S.; Rampoldi, G.; Bani, M.; Cannata, P.; Ausili, D.; di Mauro, S.; Strepparava, M.G. Predictors of Psychological Distress amongst Nursing Students: A Multicenter Cross-Sectional Study. Nurse Educ. Pract. 2020, 44. [Google Scholar] [CrossRef] [PubMed]
- Xie, C.; Li, X.; Zeng, Y.; Hu, X. Mindfulness, Emotional Intelligence, and Occupational Burnout in Intensive Care Nurses: A Mediating Effect Model. J. Nurs. Manag. 2020. [Google Scholar] [CrossRef] [PubMed]
- Durlak, J.A.; Weissberg, R.P.; Dymnicki, A.B.; Taylor, R.D.; Schellinger, K.B. The Impact of Enhancing Students’ Social and Emotional Learning: A Meta-Analysis of School-Based Universal Interventions. Child. Dev. 2011, 82, 405–432. [Google Scholar] [CrossRef] [PubMed]
- Sharif, F.; Rezaie, S.; Keshavarzi, S.; Mansoori, P.; Ghadakpoor, S. Teaching Emotional Intelligence to Intensive Care Unit Nurses and Their General Health: A Randomized Clinical Trial. Int. J. Occup. Environ. Med. 2013, 4, 141–208. [Google Scholar]
- Crowne, K.A.; Young, T.M.; Goldman, B.; Patterson, B.; Krouse, A.M.; Proenca, J. Leading Nurses: Emotional Intelligence and Leadership Development Effectiveness. Leadersh. Health Serv. 2017, 30, 217–232. [Google Scholar] [CrossRef] [PubMed]
- Shahnavazi, M.; Parsa-Yekta, Z.; Yekaninejad, M.S.; Amaniyan, S.; Griffiths, P.; Vaismoradi, M. The Effect of the Emotional Intelligence Education Programme on Quality of Life in Haemodialysis Patients. Appl. Nurs. Res. 2018, 39, 18–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dugan, J.W.; Weatherly, R.A.; Girod, D.A.; Barber, C.E.; Tsue, T.T. A Longitudinal Study of Emotional Intelligence Training for Otolaryngology Residents and Faculty. JAMA Otolaryngol. Head Neck Surg. 2014, 140, 720–726. [Google Scholar] [CrossRef] [Green Version]
- Codier, E.; Kamikawa, C.; Kooker, B.M.; Shoultz, J. Emotional Intelligence, Performance, and Retention in Clinical Staff Nurses. Nurs. Adm. Q. 2009, 33, 310–316. [Google Scholar] [CrossRef] [PubMed]
- McConville, J.; McAleer, R.; Hahne, A. Mindfulness Training for Health Profession Students—The Effect of Mindfulness Training on Psychological Well-Being, Learning and Clinical Performance of Health Professional Students: A Systematic Review of Randomized and Non-Randomized Controlled Trials. Explor. J. Sci. Health 2017, 13, 26–45. [Google Scholar] [CrossRef] [PubMed]
- dos Santos, T.M.; Kozasa, E.H.; Carmagnani, I.S.; Tanaka, L.H.; Lacerda, S.S.; Nogueira-Martins, L.A. Positive Effects of a Stress Reduction Program Based on Mindfulness Meditation in Brazilian Nursing Professionals: Qualitative and Quantitative Evaluation. Explor. J. Sci. Health 2016, 12, 90–99. [Google Scholar] [CrossRef] [PubMed]
- Fortney, L.; Luchterhand, C.; Zakletskaia, L.; Zgierska, A.; Rakel, D. Abbreviated Mindfulness Intervention for Job Satisfaction, Quality of Life, and Compassion in Primary Care Clinicians: A Pilot Study. Ann. Fam. Med. 2013, 11, 412–420. [Google Scholar] [CrossRef]
- Delgado, C.; Upton, D.; Ranse, K.; Furness, T.; Foster, K. Nurses’ Resilience and the Emotional Labour of Nursing Work: An Integrative Review of Empirical Literature. Int. J. Nurs. Stud. 2017, 70, 71–88. [Google Scholar] [CrossRef]
- Badolamenti, S.; Sili, A.; Caruso, R.; Fida, R. What Do We Know about Emotional Labour in Nursing? A Narrative Review. Br. J. Nurs. 2017, 26, 48–55. [Google Scholar] [CrossRef] [Green Version]
- Wu, L.-F.; Chang, L.-F.; Hung, Y.-C.; Lin, C.; Tzou, S.-J.; Chou, L.-J.; Pan, H.-H. The Effect of Practice toward Do-Not-Resuscitate among Taiwanese Nursing Staff Using Path Modeling. Int. J. Environ. Res. Public Health 2020, 17, 6350. [Google Scholar] [CrossRef]
- Edward, K.L.; Hercelinskyj, G.; Giandinoto, J.A. Emotional Labour in Mental Health Nursing: An Integrative Systematic Review. Int. J. Ment. Health Nurs. 2017, 26, 215–225. [Google Scholar] [CrossRef]
- Melvin, C.S. Historical Review in Understanding Burnout, Professional Compassion Fatigue, and Secondary Traumatic Stress Disorder From a Hospice and Palliative Nursing Perspective. J. Hosp. Palliat. Nurs. 2015, 17, 1. [Google Scholar] [CrossRef]
- Karimi, L.; Leggat, S.G.; Donohue, L.; Farrell, G.; Couper, G.E. Emotional Rescue: The Role of Emotional Intelligence and Emotional Labour on Well-Being and Job-Stress among Community Nurses. J. Adv. Nurs. 2014, 70, 176–186. [Google Scholar] [CrossRef]
- Syed, I.U. Clearing the Smoke Screen: Smoking, Alcohol Consumption, and Stress Management Techniques among Canadian Long-Term Care Workers. Int. J. Environ. Res. Public Health 2020, 17, 6027. [Google Scholar] [CrossRef]
- Harlow, C. Role of Nature Therapy and Mindfulness for Resilience Among Rural Healthcare Providers. In Integrative Health Nursing Interventions for Vulnerable Populations; Vermeesch, A., Ed.; Springer: Berlin, Germany, 2021. [Google Scholar] [CrossRef]
- Rowe, A.C.; Shepstone, L.; Carnelley, K.B.; Cavanagh, K.; Millings, A. Attachment Security and Self-Compassion Priming Increase the Likelihood That First-Time Engagers in Mindfulness Meditation Will Continue with Mindfulness Training. Mindfulness 2016, 7, 642–650. [Google Scholar] [CrossRef]
- Gracia Gozalo, R.M.; Ferrer Tarrés, J.M.; Ayora Ayora, A.; Alonso Herrero, M.; Amutio Kareaga, A.; Ferrer Roca, R. Application of a Mindfulness Program among Healthcare Professionals in an Intensive Care Unit: Effect on Burnout, Empathy and Self-Compassion. Med. Intensiva 2019, 43, 207–216. [Google Scholar] [CrossRef] [PubMed]
- Germer, C.K.; Neff, K.D. Self-Compassion in Clinical Practice. J. Clin. Psychol. 2013, 69, 856–867. [Google Scholar] [CrossRef] [PubMed]
- Raab, K. Mindfulness, Self-Compassion, and Empathy Among Health Care Professionals: A Review of the Literature. J. Health Care Chaplain. 2014, 20, 95–108. [Google Scholar] [CrossRef] [PubMed]
- Mills, J.; Wand, T.; Fraser, J.A. Palliative Care Professionals’ Care and Compassion for Self and Others: A Narrative Review. Int. J. Palliat. Nurs. 2017, 23, 219–229. [Google Scholar] [CrossRef]
- Hart, P.L.; Brannan, J.D.; de Chesnay, M. Resilience in Nurses: An Integrative Review. J. Nurs. Manag. 2014, 22, 720–734. [Google Scholar] [CrossRef] [Green Version]
- Noble, H.; Reid, J.; Walsh, I.; Ellison, S.; McVeigh, C. Evaluating Mindfulness Training for Medical and PhD Nursing Students. Br. J. Nurs. 2019, 28, 798–802. [Google Scholar] [CrossRef] [PubMed]
- Kemper, K.J.; Mo, X.; Khayat, R. Are Mindfulness and Self-Compassion Associated with Sleep and Resilience in Health Professionals? J. Altern. Complementary Med. 2015, 21, 496–503. [Google Scholar] [CrossRef] [PubMed]
- Yu, F.; Raphael, D.; Mackay, L.; Smith, M.; King, A. Personal and Work-Related Factors Associated with Nurse Resilience: A Systematic Review. Int. J. Nurs. Stud. 2019, 93, 129–140. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Assessing Item | Vongareesawat et al. 2012 | Snowden et al. 2015 | Dubert et al. 2016 | Jacobs et al. 2016 | Orellana et al. 2017 | Kelm et al. 2018 | Lamothe et al. 2018 | Salvarani et al. 2019 | Salvarani et al. 2020 | Xie et al. 2020 |
|---|---|---|---|---|---|---|---|---|---|---|
| Were the criteria for inclusion in the sample clearly defined? | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Were the study subjects and the setting described in detail? | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Was the exposure measured in a valid and reliable way? | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Were objective, standard criteria used for measurement of the condition? | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Were confounding factors identified? | Y | Y | Y | Y | Y | Y | Y | Y | Y | N |
| Were strategies to deal with confounding factors stated? | Y | Y | N | Y | N | Y | N | N | Y | Y |
| Were the outcomes measured in a valid and reliable way? | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Was appropriate statistical analysis used? | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Overall appraisal | I | I | I | I | I | I | I | I | I | I |
| Authors Year Country | Design | Participants | Intervention | Variables (Assessment Tool) | Findings |
|---|---|---|---|---|---|
| Vongareesawat et al. [50] 2012. Thailand. | Pretest post-test (control group) | N = 26 psychiatric nurses | Mindfulness training 9 h/day 5 days/week 8 weeks | E Intelligence (TEISTTP) | EI scores significantly higher immediately after intervention (F = −2.13 p = 0.022) and at the one-month follow-up (F = −1.78 p = 0.044). |
| Snowden et al. [51] 2015. UK. | Cross-sectional | N = 870 nursing and midwifery students | Mindfulness training | E Intelligence (TEIQue, SEIS) | No significant differences in TEIQ-SF scores after mindfulness training (U = 22,980, z = 0.864, p = 0.388). Median SEIS significantly different according to mindfulness training (U = 25,115.5, z = 2.05, p = 0.039). |
| Dubert et al. [52] 2016. USA. | Cross-sectional | N = 80 nursing students | N/A | Dispositional mindfulnes (MAAS) E regulation (ERQ) | Positive correlation between MAAS and ERQ-R (r = 0.1905; p = 0.045). Direct effect with MAAS on ERQ-R (γ11 = 0.292 ± 0.158, p = 0.034) |
| Jacobs et al. [53] 2016. Germany. | Cross-sectional | N = 427 occupational therapists | N/A | Skills of mindfulness (KIMS) E Intelligence (TEIQue) | Trait E Intelligence correlated with skills of mindfulness observed (r = 0.19, p < 0.001), describe (r = 0.54, p < 0.001), act with awareness (r = 0.45, p < 0.001) and accept without judgment (r = 0.55, p < 0.001). Mindfulness facets explained 50.2% of variance of emotional intelligence [F(5,421) = 84.73, p < 0.001] |
| Orellana et al. [54] 2017. Germany. | Pretest post-test | N = 28 palliative healthcare professionals | Meditation training 2 h session 10 weeks | E regulation (ERSQ-27) Burnout (MBI) | E exhaustion decreased after meditation (t = −3.13, p < 0.005, d = 0.41) and E awareness increased (t = −2.87, p = 0.008, d = 0.45) as well as resilience (t = −2.47, p = 0.021, d = 0.43). E regulation skills increased but not significantly (t = −1.85, p > 0.05, d = 0.24). |
| Kelm et al. [55] 2018. USA. | Pretest post-test | N = 24 ICU health professionals | Mindfulness meditation 7 min twice/day or 14 min/day 4-week | CPR performance E intelligence (TEIQue) E balance (PANAS) | More positive E balance after intervention (Mean difference = 0.33, Cohen’s d = 0.43, p = 0.02). E intelligence improvement was not significant (Mean difference = 4, Cohen’s d = 0.28, p = 0.16). |
| Lamothe et al. [56] 2018. Canada. | Pretest post-test | N = 37 12 healthcare students 25 healthcare professionals | Mindfulness program 2 h/week 8 weeks 1 full-day retreat. | Dispositional mindfulness (MAAS) E competence (PEC, ERQ, GERT) E acceptance (AAQ-II) | Students showed significant differences after the program in E acceptance [d = 1.39; t(11) = 4.81, p < 0.001], emotion recognition [d = 1.20; t(11) = 4.14, p < 0.01], identifying own emotions [d = 0.77; t(11) = 2.67, p < 0.05], expressive suppression, [d = 0.73; t(11) = 2.53, p < 0.05]. |
| Salvarani et al. [57] 2019. Italy. | Cross-sectional | N = 97 emergency nurses | N/A | Dispositional mindfulness (FFMQ) Ability to regulate emotions (DERS) Burnout (MBI) | Significant negative correlation between E exhaustion and regulation of emotions and dimensions of FFQM (p < 0.05) FFMQ subscales explained the 23.6% of the E exhaustion variance |
| Salvarani et al. [58] 2020. Italy. | Cross-sectional | N = 622 nursing students | N/A | Dispositional mindfulness (FFMQ) Ability to regulate emotions (DERS) | Positive correlation between mindfulness and all dimensions of the ability to regulate emotions (p < 0.05). |
| Xie et al. [59] 2020. China. | Cross-sectional | N = 883 ICU nurses | N/A | Dispositional mindfulness (MAAS) E Intelligence (EI) Burnout (MBI) | Association between mindfulness, E intelligence, E exhaustion, depersonalization, and personal accomplishment (p < 0.001). E intelligence partially mediates the relationships between mindfulness and E exhaustion (total effect −0.492, p = 0.011) and depersonalization (total effect −0.633, p = 0.018). |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiménez-Picón, N.; Romero-Martín, M.; Ponce-Blandón, J.A.; Ramirez-Baena, L.; Palomo-Lara, J.C.; Gómez-Salgado, J. The Relationship between Mindfulness and Emotional Intelligence as a Protective Factor for Healthcare Professionals: Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 5491. https://doi.org/10.3390/ijerph18105491
Jiménez-Picón N, Romero-Martín M, Ponce-Blandón JA, Ramirez-Baena L, Palomo-Lara JC, Gómez-Salgado J. The Relationship between Mindfulness and Emotional Intelligence as a Protective Factor for Healthcare Professionals: Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(10):5491. https://doi.org/10.3390/ijerph18105491
Chicago/Turabian StyleJiménez-Picón, Nerea, Macarena Romero-Martín, José Antonio Ponce-Blandón, Lucia Ramirez-Baena, Juan Carlos Palomo-Lara, and Juan Gómez-Salgado. 2021. "The Relationship between Mindfulness and Emotional Intelligence as a Protective Factor for Healthcare Professionals: Systematic Review" International Journal of Environmental Research and Public Health 18, no. 10: 5491. https://doi.org/10.3390/ijerph18105491