
A Model of the Effects of Parental Illness on Youth Adjustment and Family Functioning: The Moderating Effects of Psychological Flexibility on Youth Caregiving and Stress

 ,
,  ,
,  ,
,  ,
, 
Abstract
:1. Introduction
1.1. Illness Severity and Youth Adjustment and Family Functioning
1.2. Mediators of the Effects of Parental Illness on Youth Adjustment and Family Functioning
1.3. Psychological Flexibility as Moderator of the Effects of Parental Illness on Youth Adjustment and Family Functioning
1.4. The Present Study
2. Materials and Methods
2.1. Participants and Recruitment Procedure
2.2. Measures
2.2.1. Demographic Characteristics
2.2.2. Parental Illness Severity
2.2.3. Youth Caregiving
2.2.4. Youth Stress
2.2.5. Psychological Flexibility
2.2.6. Youth Adjustment—Internalizing and Externalizing Problems
2.2.7. Youth Adjustment—Psychological Wellbeing
2.2.8. Family Functioning
2.3. Data Analysis Approach
3. Results
3.1. Participant Characteristics
3.2. Path Analyses
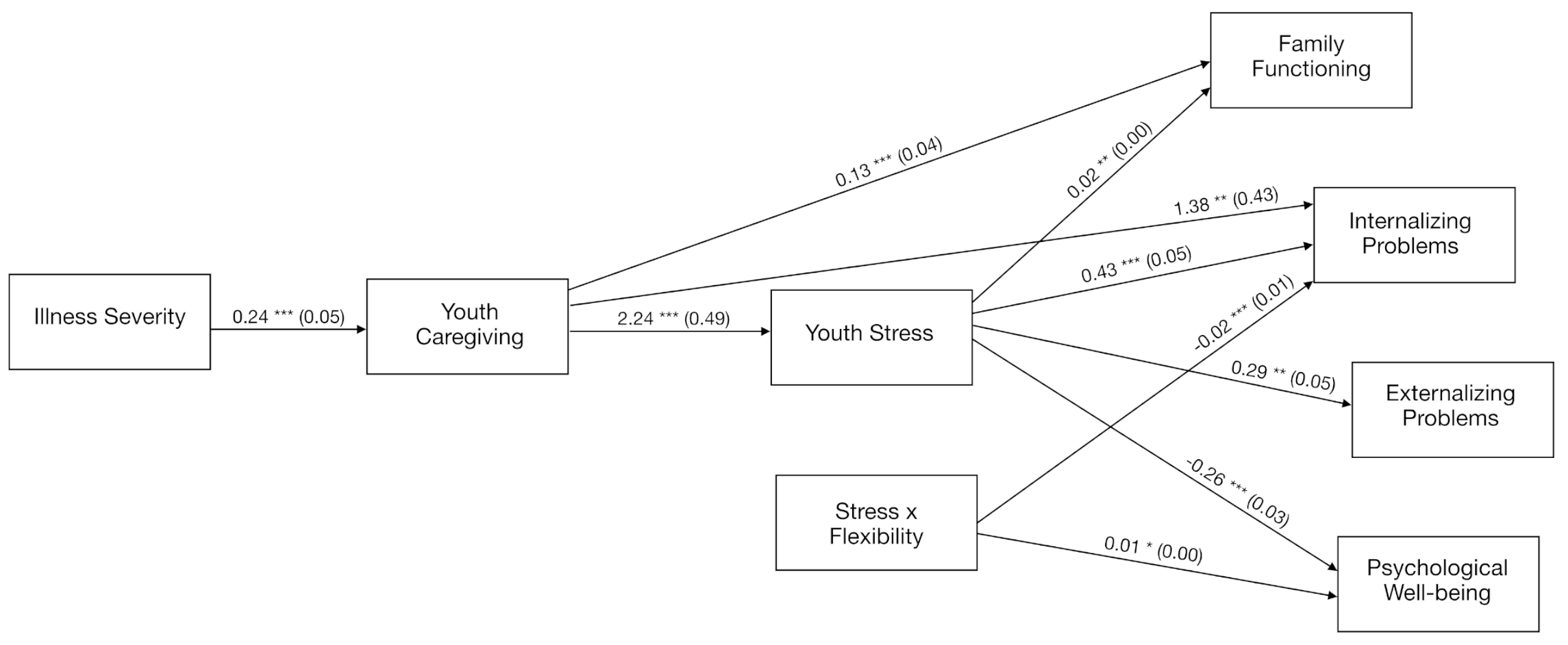
3.2.1. Serial Mediation of Youth Caregiving and Stress on the Link between Parental Illness and Youth Adjustment and Family Functioning
3.2.2. Moderated Mediation: The Buffering Effects of Psychological Flexibility through Youth Caregiving and Stress
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Robison, O.M.; Inglis, G.; Egan, J. The health, well-being and future opportunities of young carers: A population approach. Public Health 2020, 185, 139–143. [Google Scholar] [CrossRef]
- Worsham, N.L.; Compas, B.E.; Ey, S. Children’s coping with parental illness. In Handbook of Children’s Coping; Wolchik, S.A., Sandler, I.N., Eds.; Issues in Clinical Child Psychology; Springer: Boston, MA, USA, 1997; pp. 195–213. [Google Scholar]
- Morley, D.; Li, X.; Jenkinson, C. (Eds.) Children and Young People’s Response to Parental Illness: A Handbook of Assessment and Practice; CRC Press: Boca Raton, FL, USA; London, UK; New York, NY, USA, 2016. [Google Scholar]
- World Health Organization. Noncommunicable Diseases: Progress Monitor 2020. Available online: https://www.who.int/publications/i/item/ncd-progress-monitor-2020 (accessed on 21 October 2020).
- Armistead, L.; Klein, K.; Forehand, R. Parental physical illness and child functioning. Clin. Psychol. Rev. 1995, 15, 409–422. [Google Scholar] [CrossRef]
- Hagen, K.A.; Hilsen, M.; Kallander, E.K.; Ruud, T. Health-related quality of life (HRQoL) in children of ill or substance abusing parents: Examining factor structure and sub-group differences. Qual. Life Res. 2019, 28, 1063–1073. [Google Scholar] [CrossRef] [PubMed]
- Korneluk, Y.G.; Lee, C.M. Children’s adjustment to parental physical illness. Clin. Child Fam. Psychol. Rev. 1998, 1, 179–193. [Google Scholar] [CrossRef] [PubMed]
- Landi, G.; Andreozzi, M.S.; Pakenham, K.I.; Grandi, S.; Tossani, E. Psychosocial adjustment of young offspring in the context of parental type 1 and type 2 diabetes: A systematic review. Diabet. Med. 2020, 37, 1103–1113. [Google Scholar] [CrossRef] [PubMed]
- Pakenham, K.I.; Cox, S. The nature of caregiving in children of a parent with multiple sclerosis from multiple sources and the associations between caregiving activities and youth adjustment overtime. Psychol. Health 2012, 27, 324–346. [Google Scholar] [CrossRef] [Green Version]
- Pakenham, K.I.; Cox, S. Test of a model of the effects of parental illness on youth and family functioning. Health Psychol. 2012, 31, 580–590. [Google Scholar] [CrossRef] [Green Version]
- Pakenham, K.I.; Cox, S. Comparisons between youth of a parent with MS and a control group on adjustment, caregiving, attachment and family functioning. Psychol. Health 2014, 29, 1–15. [Google Scholar] [CrossRef]
- Pakenham, K.I.; Cox, S. The effects of parental illness and other ill family members on the adjustment of children. Ann. Behav. Med. 2014, 48, 424–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pakenham, K.I.; Cox, S. The effects of parental illness and other ill family members on youth caregiving experiences. Psychol. Health 2015, 30, 857–878. [Google Scholar] [CrossRef] [Green Version]
- Pakenham, K.I.; Chiu, J.; Bursnall, S.; Cannon, T. Relations between social support, appraisal and coping and both positive and negative outcomes in young carers. J. Health Psychol. 2007, 12, 89–102. [Google Scholar] [CrossRef]
- Sieh, D.S.; Meijer, A.M.; Oort, F.J.; Visser-Meily, J.M.A.; Van der Leij, D.A.V. Problem behavior in children of chronically ill parents: A meta-analysis. Clin. Child Fam. Psychol. Rev. 2010, 13, 384–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elliott, L.; Thompson, K.A.; Fobian, A.D. A systematic review of somatic symptoms in children with a chronically ill family member. Psychosom. Med. 2020, 82, 366–376. [Google Scholar] [CrossRef] [PubMed]
- Ireland, M.J.; Pakenham, K.I. Youth adjustment to parental illness or disability: The role of illness characteristics, caregiving, and attachment. Psychol. Health Med. 2010, 15, 632–645. [Google Scholar] [CrossRef] [PubMed]
- Sieh, D.S.; Visser-Meily, J.M.; Oort, F.J.; Meijer, A.M. The diurnal salivary cortisol pattern of adolescents from families with single, ill and healthy parents. J. Psychosom. Res. 2012, 72, 288–292. [Google Scholar] [CrossRef] [Green Version]
- Patterson, J.M.; Garwick, A.W. The impact of chronic illness on families: A family systems perspective. Ann. Behav. Med. 1994, 16, 131–142. [Google Scholar] [CrossRef]
- Sieh, D.S.; Dikkers, A.L.C.; Visser-Meily, J.M.A.; Meijer, A.M. Stress in adolescents with a chronically ill parent: Inspiration from Rolland’s family systems-illness model. J. Dev. Phys. Disabil. 2012, 24, 591–606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedersen, S.; Revenson, T.A. Parental illness, family functioning, and adolescent well-being: A family ecology framework to guide research. J. Fam. Psychol. 2005, 19, 404–419. [Google Scholar] [CrossRef]
- Sieh, D.S.; Oort, F.J.; Visser-Meily, J.M.A.; Meijer, A.M. Mediators for internalizing problems in adolescents of parents with chronic medical condition. J. Dev. Phys. Disabil. 2014, 26, 67–82. [Google Scholar] [CrossRef]
- Compas, B.E.; Worsham, N.L.; Epping-Jordan, J.E.; Grant, K.E.; Mireault, G.; Howell, D.C.; Malcarne, V.L. When mom or dad has cancer: Markers of psychological distress in cancer patients, spouses, and children. Health Psychol. 1994, 13, 507–515. [Google Scholar] [CrossRef] [PubMed]
- Compas, B.E.; Worsham, N.L.; Ey, S.; Howell, D.C. When mom or dad has cancer: II. Coping, cognitive appraisals, and psychological distress in children of cancer patient. Health Psychol. 1996, 15, 167–175. [Google Scholar] [CrossRef] [PubMed]
- Pakenham, K.I.; Bursnall, S.; Chiu, J.; Cannon, T.; Okochi, M. The psychosocial impact of caregiving on young people who have a parent with an illness or disability: Comparisons between young caregivers and noncaregivers. Rehabil. Psychol. 2006, 51, 113–126. [Google Scholar] [CrossRef]
- Steele, R.G.; Tripp, G.; Kotchick, B.A.; Summers, P.; Forehand, R. Family members’ uncertainty about parental chronic illness: The relationship of hemophilia and HIV infection to child functioning. J. Pediatr. Psychol. 1997, 22, 577–591. [Google Scholar] [CrossRef] [Green Version]
- Chikhradze, N.; Knecht, C.; Metzing, S. Young carers: Growing up with chronic illness in the family—A systematic review 2007–2017. J. Compassionate Health Care 2017, 4, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Joseph, S.; Kendall, C.; Toher, D.; Sempik, J.; Holland, J.; Becker, S. Young carers in England: Findings from the 2018 BBC survey on the prevalence and nature of caring among young people. Child Care Health Dev. 2019, 45, 606–612. [Google Scholar] [CrossRef]
- Aldridge, J.; Becker, S. Children as carers: The impact of parental illness and disability on children’s caring roles. J. Fam. Ther. 1999, 21, 303–320. [Google Scholar] [CrossRef]
- Early, L.; Cushway, D.; Cassidy, T. Perceived stress in young carers: Development of a measure. J. Child Fam. Stud. 2006, 15, 165–176. [Google Scholar] [CrossRef]
- Hayes, S.C.; Strosahl, K.D.; Wilson, K.G. Acceptance and Commitment Therapy. An Experiential Approach to Behavior Change, 2nd ed.; The Guildford Press: New York, NY, USA, 2012. [Google Scholar]
- Kashdan, T.B.; Rottenberg, J. Psychological flexibility as a fundamental aspect of health. Clin. Psychol. Rev. 2010, 30, 865–878. [Google Scholar] [CrossRef] [Green Version]
- Gloster, A.T.; Meyer, A.H.; Lieb, R. Psychological flexibility as a malleable public health target: Evidence from a representative sample. J. Contextual. Behav. Sci. 2017, 6, 166–171. [Google Scholar] [CrossRef] [Green Version]
- Moyer, D.N.; Sandoz, E.K. The role of psychological flexibility in the relationship between parent and adolescent distress. J. Child Fam. Stud. 2015, 24, 1406–1418. [Google Scholar] [CrossRef]
- Fonseca, S.; Trindade, I.A.; Mendes, A.L.; Ferreira, C. The buffer role of psychological flexibility against the impact of major life events on depression symptoms. Clin. Psychol. 2020, 24, 82–90. [Google Scholar] [CrossRef]
- Darlington, R.B.; Hayes, A.F. Detecting and Managing Irregularities in Regression Analysis and Linear Models: Concepts, Applications, and Implementation; Guilford: New York, NY, USA, 2017; pp. 479–518. [Google Scholar]
- Cox, S.; Pakenham, K.I. Confirmatory factor analysis and invariance testing of the Young Carer of Parents Inventory (YCOPI). Rehabil. Psychol. 2014, 59, 439–452. [Google Scholar] [CrossRef] [Green Version]
- Landi, G.; Boccolini, G.; Giovagnoli, S.; Pakenham, K.I.; Grandi, S.; Tossani, E. Validation of the Italian Young Carer of Parents Inventory-Revised (YCOPI-R). Disabil. Rehabil. 2020, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Landi, G.; Pakenham, K.I.; Crocetti, E.; Grandi, S.; Tossani, E. Examination of the tripartite model of youth caregiving in the context of parental illness. Psychol. Health 2021, 1–22. [Google Scholar] [CrossRef]
- Pakenham, K.I.; Cox, S. Effects of benefit finding, social support and caregiving on youth adjustment in a parental illness context. J. Child Fam. Stud. 2018, 27, 2491–2506. [Google Scholar] [CrossRef]
- De Bruin, E.I.; Sieh, D.S.; Zijlstra, B.J.; Meijer, A.M. Chronic childhood stress: Psychometric properties of the chronic stress questionnaire for children and adolescents (CSQ-CA) in three independent samples. Child Indic. Res. 2018, 11, 1389–1406. [Google Scholar] [CrossRef] [Green Version]
- Schweiger, M.; Ristallo, A.; Oppo, A.; Pergolizzi, F.; Presti, G.; Moderato, P. Ragazzi in lotta con emozioni e pensieri: La validazione della versione italiana dellʼAvoidance and Fusion Questionnaire for Youth (I-AFQ-Y). Psicot. Cognit. Comport. 2017, 23, 141–162. [Google Scholar]
- Greco, L.A.; Lambert, W.; Baer, R.A. Psychological inflexibility in childhood and adolescence: Development and evaluation of the Avoidance and Fusion Questionnaire for Youth. Psychol. Assess. 2008, 20, 93–102. [Google Scholar] [CrossRef]
- Livheim, F.; Tengström, A.; Bond, F.W.; Andersson, G.; Dahl, J.; Rosendahl, I. Psychometric properties of the Avoidance and Fusion Questionnaire for Youth: A psychological measure of psychological inflexibility in youth. J. Contextual. Behav. Sci. 2016, 5, 103–110. [Google Scholar] [CrossRef] [Green Version]
- Frigerio, A.; Cattaneo, C.; Cataldo, M.; Schiatti, A.; Molteni, M.; Battaglia, M. Behavioral and emotional problems among Italian children and adolescents aged 4 to 18 years as reported by parents and teachers. Eur. J. Psychol. Assess. 2004, 20, 124–133. [Google Scholar] [CrossRef]
- Achenbach, T.M.; Rescorla, L.A. Manual for ASEBA School-Age Forms & Profiles; University of Vermont, Research Center for Children, Youth, & Families: Burlington, VT, USA, 2001. [Google Scholar]
- Lum, J.J.; Phares, V. Assessing the emotional availability of parents. J. Psychopathol. Behav. Assess. 2005, 27, 211–226. [Google Scholar] [CrossRef]
- Kidscreen Group Europe. The KIDSCREEN Questionnaires: Quality of Life Questionnaires for Children and Adolescents; Pabst Science Publishers: Lengerich, Germany, 2006. [Google Scholar]
- Ravens-Sieberer, U.; Auquier, P.; Erhart, M.; Gosch, A.; Rajmil, L.; Bruil, J.; Power, M.; Duer, W.; Cloetta, B.; Czemy, L.; et al. The KIDSCREEN-27 quality of life measure for children and adolescents: Psychometric results from a cross-cultural survey in 13 European countries. Qual. Life Res. 2007, 16, 1347–1356. [Google Scholar] [CrossRef] [PubMed]
- Sepke, M.; Ferentzi, H.; Disselhoff, V.S.U.; Albert, W. Exploring the developmental tasks of emerging adults after paediatric heart transplantation: A cross-sectional case control study. BMJ Open 2018, 8, e022461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grandi, S.; Fabbri, S.; Scortichini, S.; Bolzani, R. Italian validation of the Family Assessment Device (FAD). Riv. Psichiat. 2007, 42, 114–122. [Google Scholar]
- Epstein, N.B.; Baldwin, L.M.; Bishop, D.S. The McMaster family assessment device. J. Marital. Fam. Ther. 1983, 9, 171–180. [Google Scholar] [CrossRef]
- Akister, J.; Stevenson-Hinde, J. Identifying families at risk: Exploring the potential of the McMaster Family Assessment Device. J. Fam. Ther. 1991, 13, 411–421. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach, 2nd ed.; Guilford Press: New York, NY, USA, 2018. [Google Scholar]
- Hayes, A.F. An index and test of linear moderated mediation. Multivar. Behav. Res. 2015, 50, 1–22. [Google Scholar] [CrossRef]
- Jansen, J.E.; Haahr, U.H.; Lyse, H.G.; Pedersen, M.B.; Trauelsen, A.M.; Simonsen, E. Psychological flexibility as a buffer against caregiver distress in families with psychosis. Front. Psychol. 2017, 8, 1625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muris, P.; Meesters, C.; Herings, A.; Jansen, M.; Vossen, C.; Kersten, P. Inflexible youngsters: Psychological and psychopathological correlates of the Avoidance and Fusion Questionnaire for youths in nonclinical Dutch adolescents. Mindfulness 2017, 8, 1381–1392. [Google Scholar] [CrossRef] [Green Version]
- Gloster, A.T.; Walder, N.; Levin, M.; Twohig, M.; Karekla, M. The empirical status of Acceptance and Commitment Therapy: A review of meta-analyses. J. Contextual. Behav. Sci. 2020, 18, 181–192. [Google Scholar] [CrossRef]
- Livheim, F.; Hayes, L.; Ghaderi, A.; Magnusdottir, T.; Högfeldt, A.; Rowse, J.; Turner, S.; Hayes, S.C.; Tengström, A. The effectiveness of Acceptance and Commitment Therapy for adolescent mental health: Swedish and Australian pilot outcomes. J. Child Fam. Stud. 2015, 24, 1016–1030. [Google Scholar] [CrossRef]
- Kishita, N.; Contreras, M.L.; West, J.; Mioshi, E. Exploring the impact of carer stressors and psychological inflexibility on depression and anxiety in family carers of people with dementia. J. Contextual. Behav. Sci. 2020, 17, 119–125. [Google Scholar] [CrossRef]
- Han, A.; Yuen, H.K.; Jenkins, J. Acceptance and commitment therapy for family caregivers: A systematic review and meta-analysis. J. Health Psychol. 2020, 26, 82–102. [Google Scholar] [CrossRef] [PubMed]
- Pakenham, K.I. Effects of Acceptance and Commitment Therapy (ACT) training on clinical psychology trainee stress, therapist skills and attributes, and ACT processes. Clin. Psychol. Psychother. 2015, 22, 647–655. [Google Scholar] [CrossRef]
- Pakenham, K.I.; Stafford-Brown, J. Postgraduate clinical psychology students’ perceptions of an Acceptance and Commitment Therapy stress management intervention and clinical training. Clin. Psychol. 2013, 17, 56–66. [Google Scholar] [CrossRef]
- Puolakanaho, A.; Lappalainen, R.; Lappalainen, P.; Muotka, J.S.; Hirvonen, R.; Eklund, K.M.; Ahonen, T.P.S.; Kiuru, N. Reducing stress and enhancing academic buoyancy among adolescents using a brief web-based program based on acceptance and commitment therapy: A randomized controlled trial. J. Youth Adolesc. 2019, 48, 287–305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Räsänen, P.; Lappalainen, P.; Muotka, J.; Tolvanen, A.; Lappalainen, R. An online guided ACT intervention for enhancing the psychological wellbeing of university students: A randomized controlled clinical trial. Behav. Res. Ther. 2016, 78, 30–42. [Google Scholar] [CrossRef] [PubMed]
- Stafford-Brown, J.; Pakenham, K.I. The effectiveness of an ACT informed intervention for managing stress and improving therapist qualities in clinical psychology trainees. J. Clin. Psychol. 2012, 68, 513–592. [Google Scholar] [CrossRef]
- Viskovich, S.; Pakenham, K.I. Pilot evaluation of a web-based acceptance and commitment therapy program to promote mental health skills in university students. J. Clin. Psychol. 2018, 74, 2047–2069. [Google Scholar] [CrossRef] [Green Version]
- Viskovich, S.; Pakenham, K.I. Randomized controlled trial of a web-based Acceptance and Commitment Therapy (ACT) program to promote mental health in university students. J. Clin. Psychol. 2020, 76, 929–951. [Google Scholar] [CrossRef] [PubMed]
- Giovannetti, A.M.; Quintas, R.; Tramacere, I.; Giordano, A.; Confalonieri, P.; Messmer Uccelli, M.; Solari, A.; Pakenham, K.I. A resilience group training program for people with MS: Results of a pilot single-blind randomized controlled trial and nested qualitative study. PLoS ONE 2020, 15, e0231380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryan, A.; Pakenham, K.I.; Burton, N. A pilot evaluation of a group acceptance and commitment therapy (ACT)-informed resilience training program for people with diabetes. Aust. Psychol. 2020, 55, 196–207. [Google Scholar] [CrossRef]
- Hawkes, A.L.; Pakenham, K.I.; Chambers, S.K.; Patrao, T.A.; Courneya, K.S. Effects of a multiple health behavior change intervention for colorectal cancer survivors on psychosocial outcomes and quality of life: A randomised controlled trial. Ann. Behav. Med. 2014, 48, 359–370. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| % | M (SD) | Range | |
|---|---|---|---|
| Sample characteristics | |||
| Age in years | 17.71 (3.61) | 11–24 | |
| Gender: male | 40.8 | ||
| Currently studying | 83.9 | ||
| Current part-time job | 29.0 | ||
| Family size | 4.04 (1.14) | 2–8 | |
| Single-parent family | 6.2 | ||
| Descriptive data for study variables | |||
| Illness Severity | 2.62 (0.83) | 1–5 | |
| Youth Caregiving | 1.50 (0.78) | 0–3.86 | |
| Stress | 42.45 (8.01) | 21–60 | |
| Psychological Flexibility | 22.88 (5.71) | 5–32 | |
| Internalizing Problems | 15.52 (9.76) | 0–42 | |
| Externalizing Problems | 10.04 (6.48) | 0–34 | |
| Psychological Wellbeing | 26.01 (5.02) | 8–35 | |
| Family Functioning | 1.93 (0.55) | 1–4 |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |
|---|---|---|---|---|---|---|---|---|
| 1. Illness Severity | − | |||||||
| 2. Youth Caregiving | 0.24 ** | − | ||||||
| 3. Stress | 0.10 * | 0.24 ** | − | |||||
| 4. Psychological Flexibility | −0.07 | −0.22 ** | −0.51 ** | − | ||||
| 5. Internalizing Problems | 0.12 * | 0.29 ** | 0.56 ** | −0.59 ** | − | |||
| 6. Externalizing Problems | 0.10 | 0.18 ** | 0.45 ** | −0.43 ** | 0.55 ** | − | ||
| 7. Psychological Wellbeing | −0.11 * | −0.14 ** | −0.52 ** | 0.52 ** | −0.66 ** | −0.35 ** | − | |
| 8. Family Functioning | 0.23 ** | 0.20 ** | 0.37 ** | −0.32 ** | 0.49 ** | 0.39 ** | −0.49 ** | − |
| 9. Gender (0 = female) | −0.08 | −0.02 | −0.32 ** | 0.14 ** | −0.27 ** | 0.04 | 0.21 ** | −0.11 * |
| 10. Age | 0.16 ** | 0.10 | 0.16 ** | 0.03 | 0.01 | 0.01 | −0.16 ** | 0.13 * |
| Youth Caregiving (M1) | Youth Stress (M2) | Internalizing Problems (Y1) | Externalizing Problems (Y2) | Psychological Wellbeing (Y3) | Family Functioning (Y4) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Coeff. (SE) | 95% CI | Coeff. (SE) | 95% CI | Coeff. (SE) | 95% CI | Coeff. (SE) | 95% CI | Coeff. (SE) | 95% CI | Coeff. (SE) | 95% CI | |
| Illness Severity (X) | 0.244 ***, | 0.139, | 0.038 | −1.007, | 0.212 | −0.664, | 0.507, | −0.279, | −0.280 | −0.816, | 0.047 | −0.021, |
| (0.054) | 0.350 | (0.531) | 1.083 | (0.446) | 1.089 | (0.400) | 1.292 | (0.273) | 0.256 | (0.035) | 0.115 | |
| Youth Caregiving (M1) | 2.242 *** | 1.272, | 1.375 *** | 0.535, | 0.325, | −0.428, | 0.236, | −0.278, | 126 ***, | 0.054, | ||
| (0.494) | 3.213 | (0.427) | 2.216 | (0.383) | 1.079 | (0.261) | 0.750 | 0.036 | 0.197 | |||
| Youth Stress (M2) | 0.433 ***, | 0.332, | 0.291 **, | 0.201, | −0.263 ***, | −0.324, | 0.018 **, | 0.010, | ||||
| (0.051) | 0.533 | (0.046) | 0.381 | (0.031) | −0.202 | (0.004) | 0.026 | |||||
| Psychological Flexibility (W) | −0.738, | −0.874, | −0.293, | −0.415, | 0.256, | 0.172, | −0.014, | −0.025, | ||||
| (0.069) | −0.601 | (0.062) | −0.171 | (0.042) | 0.339 | (0.006) | 0.003 | |||||
| Interaction (M2 × W) | −0.023 ***, | −0.037, | 0.006, | −0.007, | 0.011 *, | 0.002, | 0.000, | −0.001, | ||||
| (0.007) | −0.010 | (0.006) | 0.018 | (0.004) | 0.019 | (0.001) | (0.001) | |||||
| Gender (U1) | 0.001, | −0.154, | −5.061 ***, | −6.557, | −1.792 **, | −3.121, | 2.495 ***, | 1.304, | 0.242 | −0.571, | 0.015, | −0.093 |
| (0.079) | 0.155 | (0.761) | −3.566 | (0.676) | −0.463 | (0.606) | 3.687 | (0.414) | 1.055 | (0.055) | (0.123) | |
| Age (U2) | 0.013, | −0.008, | 0.288 **, | 0.082, | −0.201 *, | −0.376, | −0.109, | −0.266, | −0.121 *, | −0.228, | 0.008, | −0.006, |
| (0.011) | 0.034 | (0.105) | 0.493 | 0.089 | −0.027 | (0.08) | 0.048 | (0.054) | −0.014 | (0.007) | 0.022 | |
| R2 = 0.061 *** | R2 = 0.172 *** | R2 = 0.611 *** | R2 = 0.290 *** | R2 = 0.449 *** | R2 = 0.197 *** | |||||||
| F(3, 383) = 8.235 | F(4, 382) = 19.806 | F(7, 379) = 84.912 | F(7, 379) = 22.159 | F(7, 379) = 44.074 | F(7, 379) = 13.296 | |||||||
| Index of Moderated Mediation | Coeff. (SE) | 95% CI | Coeff. (SE) | 95% CI | Coeff. (SE) | 95% CI | Coeff. (SE) | 95% CI | ||||
| Moderation of the serial indirect effect through Caregiving (M1) and Stress (M2) | −0.013, | 0.025, | 0.003, | −0.005, | 0.006, | 0.000, | −0.000, | −0.001, | ||||
| (0.006) | −0.004 | (0.004) | 0.012 | (0.005) | 0.008 | 0.000 | 0.001 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Landi, G.; Pakenham, K.I.; Benassi, M.; Giovagnoli, S.; Tossani, E.; Grandi, S. A Model of the Effects of Parental Illness on Youth Adjustment and Family Functioning: The Moderating Effects of Psychological Flexibility on Youth Caregiving and Stress. Int. J. Environ. Res. Public Health 2021, 18, 4902. https://doi.org/10.3390/ijerph18094902
Landi G, Pakenham KI, Benassi M, Giovagnoli S, Tossani E, Grandi S. A Model of the Effects of Parental Illness on Youth Adjustment and Family Functioning: The Moderating Effects of Psychological Flexibility on Youth Caregiving and Stress. International Journal of Environmental Research and Public Health. 2021; 18(9):4902. https://doi.org/10.3390/ijerph18094902
Chicago/Turabian StyleLandi, Giulia, Kenneth Ian Pakenham, Mariagrazia Benassi, Sara Giovagnoli, Eliana Tossani, and Silvana Grandi. 2021. "A Model of the Effects of Parental Illness on Youth Adjustment and Family Functioning: The Moderating Effects of Psychological Flexibility on Youth Caregiving and Stress" International Journal of Environmental Research and Public Health 18, no. 9: 4902. https://doi.org/10.3390/ijerph18094902