A Comparison of the Effect of Two Types of Whole Body Vibration Platforms on Fibromyalgia. A Randomized Controlled Trial

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instruments and Procedure
Intervention Procedure
2.3. Self-Report Questionnaires
2.4. Sensitivity Measures
2.5. Motor Function Tasks
2.6. Static and Dynamic Balance
3. Results
3.1. Self-Report Questionnaires
3.2. Sensitivity Measures
3.3. Motor Function Tasks
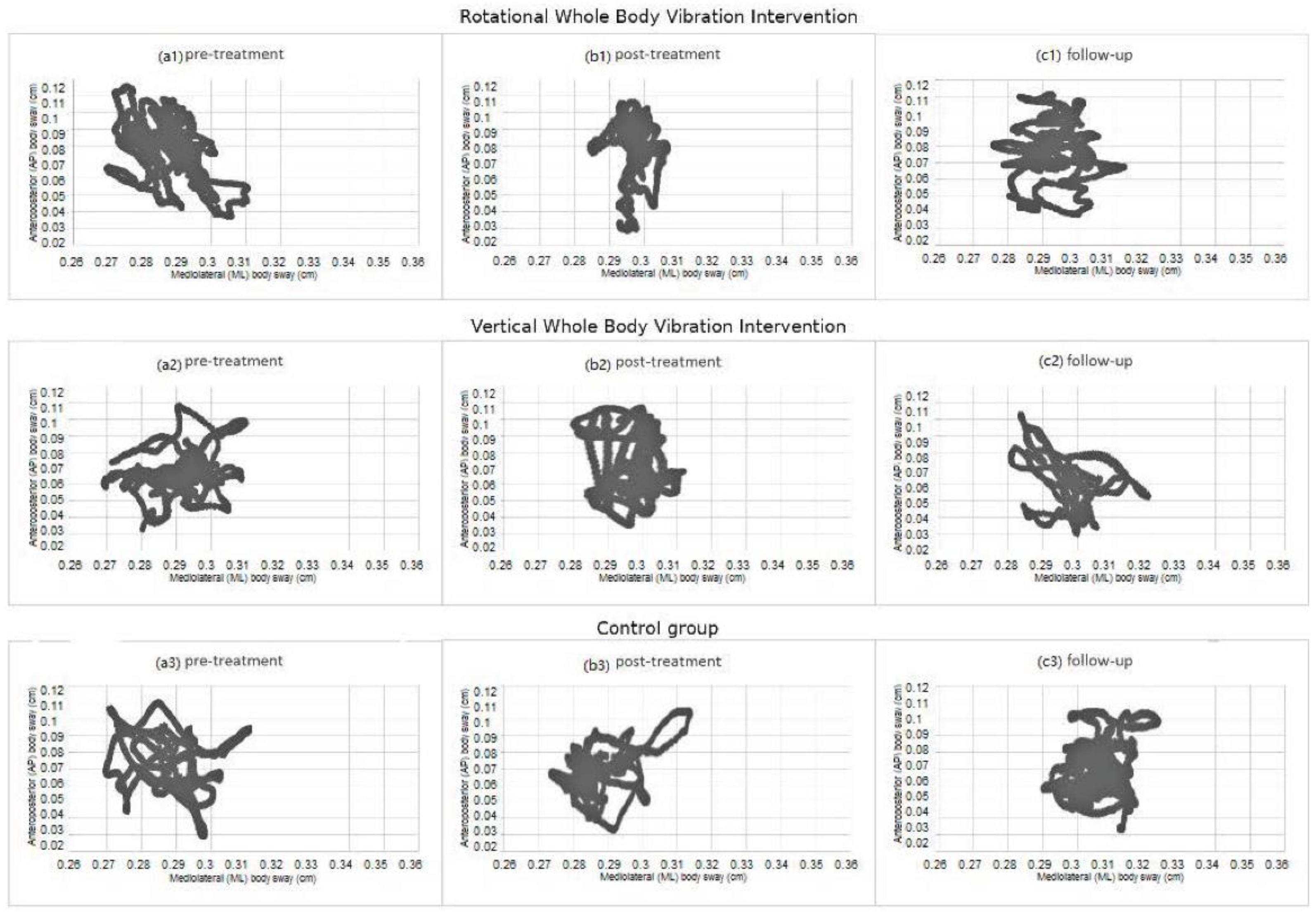
3.4. Static and Dynamic Balance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Häuser, W.; Katz, R.L.; Mease, P.J.; Russell, A.S.; Russell, I.J.; Walitt, B. 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin. Arthritis Rheum. 2016, 46, 319–329. [Google Scholar] [CrossRef] [PubMed]
- Mas, A.J.; Carmona, L.; Valverde, M.; Ribas, B. EPISER study group. Prevalence and impact of fibromyalgia on function and quality of life in individuals from the general population: Results from a nationwide study in Spain. Clin. Exp. Rheumatol. 2008, 26, 519–526. [Google Scholar]
- Martins, M.R.; Polvero, L.; Rocha, C.E.; Foss, M.H.; Santos, R. Uso de questionarios para avaliar a multidimensionalidade a qualidade de vida do fibromialgico. Rev. Bras. Reumatol. 2012, 52, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Mease, P.J.; Arnold, L.M.; Crofford, L.J.; Williams, D.A.; Russell, I.J.; Humphrey, L.; Abetz, L.; Martin, S.A. Identifying the clinical domains of fibromyalgia: Contributions from clinician and patient Delphi exercises. Arthritis Care Res. 2008, 39, 952–960. [Google Scholar] [CrossRef] [PubMed]
- Bosco, C.; Cardinale, M.; Tsarpela, O. Influence of vibration on mechanical power and electromyogram activity in human arm flexor muscles. Eur. J. Appl. Physiol. Occup. Physiol. 1999, 79, 306–311. [Google Scholar] [CrossRef]
- Park, Y.G.; Kwon, B.S.; Park, J.W.; Cha, D.Y.; Nam, K.Y.; Sim, K.B.; Chang, J.; Lee, H.J. Therapeutic effect of whole body vibration on chronic knee osteoarthritis. Ann. Rehabil. Med. 2013, 37, 505–515. [Google Scholar] [CrossRef]
- Rabini, A.; De Sire, A.; Marzetti, E.; Gimigliano, R.; Ferriero, G.; Piazzini, D.B.; Lolascon, G.; Gimigliano, F. Effects of focal muscle vibration on physical functioning in patients with knee osteoarthritis: A randomized controlled trial. Eur. J. Phys. Rehabil. Med. 2015, 51, 513–520. [Google Scholar] [PubMed]
- Zafar, H.; Alghadir, A.; Anwer, S.; Al-Eisa, E. Therapeutic effects of whole-body vibration training in knee osteoarthritis: A systematic review and meta-analysis. Arch Phys. Med. Rehabil. 2015, 96, 1525–1532. [Google Scholar] [CrossRef]
- Bokaeian, H.R.; Bakhtiary, A.H.; Mirmohammadkhani, M.; Moghimi, J. The effect of adding whole body vibration training to strengthening training in the treatment of knee osteoarthritis: A randomized clinical trial. J. Body Mov. Ther. 2016, 20, 334–340. [Google Scholar] [CrossRef]
- Sauni, R.; Paakkonen, R.; Virtema, P.; Toppila, E.; Uitti, J. Dose-response relationship between exposure to hand-arm vibration and health effects among metalworkers. Ann. Occup. Hyg. 2009, 53, 55–62. [Google Scholar]
- Kaeding, T.S.; Karch, A.; Schwarz, R.; Flor, T.; Wittke, T.C.; Kück, M.; Böselt, G.; Tegtbur, U.; Stein, L. Whole-body vibration training as a workplace-based sports activity for employees with chronic low-back pain. Scand. J. Med. Sci. Sports 2017, 27, 2027–2039. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Wang, W.; Zheng, J.; Chen, S.; Qiao, J.; Wang, X. Whole body vibration exercise for chronic musculoskeletal pain: A systematic review and meta-analysis of randomized controlled trials. Arch. Phys. Med. Rehabil. 2019, 100, 2167–2178. [Google Scholar] [CrossRef] [PubMed]
- Pel, J.J.; Bagheri, J.; van Dam, L.M.; van den Berg-Emons, H.J.; Horemans, H.L.; Stam, H.J.; van der Steen, J. Platform accelerations of three different whole-body vibration devices and the transmission of vertical vibrations to the lower limbs. Med. Eng. Phys. 2009, 31, 937–944. [Google Scholar] [CrossRef] [PubMed]
- Rauch, F.; Sievanen, H.; Boonen, S.; Cardinale, M.; Degens, H.; Felsenberg, D.; Roth, J.; Schoenau, E.; Verschueren, S.; Rittweger, J. International Society of Musculoskeletal and Neuronal Interactions. Reporting whole-body vibration intervention studies: Recommendations of the International Society of Musculoskeletal and Neuronal Interactions. J. Musculoskelet. Neuronal. Interact. 2010, 10, 193–198. [Google Scholar] [PubMed]
- Mannerkorpi, K.; Henriksson, C. Non-pharmacological treatment of chronic widespread musculoskeletal pain. Best Pract. Res. Clin. Rheumatol. 2007, 21, 513–534. [Google Scholar] [CrossRef]
- Kholvadia, A.; Baard, M. Whole body vibration improves body mass, flexibility and strength in previously sedentary adults. S. Afr. J. Sports Med. 2012, 24, 60–64. [Google Scholar] [CrossRef] [Green Version]
- Cardinale, M.; Lim, J. Electromyography activity of vastus lateralis muscle during whole-body vibrations of different frequencies. J. Strength Cond. Res. 2003, 17, 621–624. [Google Scholar] [PubMed] [Green Version]
- Abercromby, A.F.J.; Amonette, W.E.; Layne, C.S.; McFarlin, B.K.; Hinman, M.R.; Paloski, W.H. Variation in neuromuscular responses during acute whole-body vibration exercise. Med. Sci. Sports Exerc. 2007, 39, 16–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ritzmann, R.; Kramer, A.; Gruber, M.; Gollhofer, A.; Taube, W. EMG activity during whole body vibration: Motion artifacts or stretch reflexes? Eur. J. Appl. Physiol. 2010, 110, 143–151. [Google Scholar] [CrossRef] [Green Version]
- Bidonde, J.; Busch, A.J.; van der Spuy, I.; Tupper, S.; Kim, S.Y.; Boden, C. Whole body vibration exercise training for fibromyalgia. Cochrane Database Syst. Rev. 2017, 9, CD011755. [Google Scholar] [CrossRef]
- Gusi, N.; Parraca, J.A.; Olivares, P.R.; Leal, A.; Adsuar, J.C. Tilt vibratory exercise and the dynamic balance in fibromyalgia: A randomized controlled trial. Arthrit Care Res. 2010, 62, 1072–1078. [Google Scholar] [CrossRef]
- Sañudo, B.; Carrasco, L.; de Hoyo, M.; Oliva, A.; Rodríguez-Blanco, C. Changes in body balance and functional performance following whole-body vibration training in Patients with fibromyalgia syndrome: A randomized controlled trial. J. Rehabil. Med. 2013, 45, 678–684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alentorn-Geli, E.; Padilla, J.; Moras, G.; Lázaro, C.; Fernández-Solà, J. Six weeks of whole-body vibration exercise improves pain and fatigue in women with fibromyalgia. J. Altern. Complement. Med. 2008, 14, 975–981. [Google Scholar] [CrossRef] [Green Version]
- Collado-Mateo, D.; Adsuar, J.C.; Olivares, P.R.; Pozo-Cruz, B.D.; Parraca, J.A.; Pozo-Cruz, J.D.; Gusi, N. Effects of whole-body vibration therapy in patients with fibromyalgia: A systematic literature review. Evid. Based Complement. Alternat Med. 2015, 719082. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Busch, A.J.; van der Spuy, I.; Tupper, S.; Kim, S.Y.; Bidonde, J.; Overend, T.J. Whole body vibration exercise for fibromyalgia. Cochrane Database Syst. Rev. 2015, 6. [Google Scholar] [CrossRef]
- Chulvi-Medrano, I.; Sañudo, B.; Masia-Tortosa, L.; Marzo, M. The use of vibration platforms in fibromyalgia syndrome: Future prospects. J. Musculoskelet Pain 2013, 21, 165–172. [Google Scholar] [CrossRef]
- Rittweger, J.; Just, K.; Kautzsch, K.; Reeg, P.; Felsenberg, D. Treatment of chronic lower back pain with lumbar extension and whole-body vibration exercise: A randomized controlled trial. Spine 2002, 27, 1829–1834. [Google Scholar] [CrossRef]
- Spitzenpfeil, P.; Stritzker, M.; Kirchbichler, A.; Tusker, F.; Hartmann, U.; Hartard, H. Mechanical impacts to the human body by different vibration training devices. J. Biomech. 2006, 39, 196. [Google Scholar] [CrossRef]
- Monterde, S.; Salvat, I.; Montulls, S.; Fernández-Ballart, J. Validation of Fibromyalgia Impact Questionnaire. Rev. Esp. Reumatol. 2004, 31, 507–513. [Google Scholar]
- Stener-Victorin, E.; Lundeberg, T.; Kowalski, J.; Opdal, L.; Sjostrom, J.; Lundeberg, L. Perceptual matching for assessment of itch; reliability and responsiveness analyzed by a rank-invariant statistical method. J. Investig. Dermatol. 2003, 121, 1301–1305. [Google Scholar] [CrossRef] [Green Version]
- Mezzich, J.E.; Ruipérez, M.A.; Pérez, C.; Yoon, G.; Liu, J.; Mahmud, S. The Spanish version of the quality of life index: Presentation and validation. J. Nerv. Ment. Dis. 2000, 188, 301–305. [Google Scholar] [CrossRef]
- García-Palacios, A.; Herrero, R.; Vizcaíno, Y.; Belmonte, M.A.; Castilla, D.; Molinari, G.; Baños, R.M.; Botella, C. Integrating virtual reality with activity management for the treatment of fibromyalgia: Acceptability and preliminary efficacy. Clin. J. Pain 2015, 31, 564–572. [Google Scholar] [CrossRef] [Green Version]
- Kinser, A.M.; Sands, W.A.; Stone, M.H. Reliability and validity of a pressure algometer. J. Strength Cond. Res. 2009, 23, 312–314. [Google Scholar] [CrossRef]
- Arezzo, J.C.; Schaumburg, H.H.; Laudadio, C. The Vibratron: A simple device for quantitative evaluation of tactile/vibratory sense. Neurology 1985, 35, 169. [Google Scholar]
- Santo, A.S.E.; Mango, P.C.; Assumpçao, A.; Sauer, J.F.; Marques, A. Fibromyalgia: Is there association between balance and pain? A pilot study. Fisioter. Pesqui. 2014, 21, 27–33. [Google Scholar] [CrossRef]
- King, S.; Wessel, J.; Bhambhani, Y.; Maikala, R.; Sholter, D.; Maksymowych, W. Validity and reliability of the 6 minute walk in persons with fibromyalgia. J. Rheumatol. 1999, 26, 2233–2237. [Google Scholar]
- Costa, I.D.; Gamundí, A.; Miranda, J.G.; França, L.G.; De Santana, C.N.; Montoya, P. Altered functional performance in patients with fibromyalgia. Front. Hum. Neurosci. 2017, 11, 14. [Google Scholar] [CrossRef] [Green Version]
- Olivares, P.R.; Pérez-Sousa, M.A.; del Pozo-Cruz, B.; Delgado-Gil, S.; Domínguez-Muñoz, F.J.; Parraca, J.A. Fiabilidad de un test de rodilla en mujeres con fibromialgia mediante test-retest de 12 semanas. Rev. Colomb. Reumatol. 2014, 21, 70–75. [Google Scholar] [CrossRef]
- Khasnis, A.; Gokula, R. Romberg’s test. J. Postgrad Med. 2003, 49, 169. [Google Scholar] [PubMed]
- García-Pastor, C.; Álvarez, G.A. The Romberg test and Moritz Heinrich Romberg. Rev. Mex. Neuroci. 2014, 15, 31–35. [Google Scholar]
- Peña, N.; Credicio, B.C.; Nogueria, L.P.; Salles, R.M.; Souza, L.G.; Vale, M.; Cavalcanti, M.; Bomfim, J.P.; Vivas, J.G. Free instrument for measurements of motion. Rev. Bras. Ensino. Fís. 2013, 35, 1–5. [Google Scholar]
- Olivares, P.R.; Gusi, N.; Parraca, J.A.; Adsuar, J.C.; Del Pozo-Cruz, B. Tilting whole body vibration improves quality of life in women with fibromyalgia: A randomized controlled trial. J. Altern. Complement. Med. 2011, 17, 723–728. [Google Scholar] [CrossRef]
- Jones, K.D.; Horak, F.B.; Winters-Stone, K.; Irvine, J.M.; Bennet, R.M. Fibromyalgia is associated with impaired balance and falls. J. Clin. Rheumatol. 2009, 15, 16–21. [Google Scholar] [CrossRef] [Green Version]
- Melzack, R.; Wall, P.D. Mechanisms of pain: A new theory. Science 1965, 150, 971–979. [Google Scholar] [CrossRef]
- Rittweger, J. Vibration as an exercise modality: How it may work, and what its potential might be. Eur. J. Appl. Physiol. 2010, 108, 877–904. [Google Scholar] [CrossRef] [Green Version]
- Proske, U.; Gandevia, S.C. The proprioceptive senses: Their roles in signaling body shape, body position and movement, and muscle force. Physiol. Rev. 2012, 92, 1651–1697. [Google Scholar] [CrossRef] [PubMed]
- Hazell, T.J.; Jakobi, J.M.; Kenno, K.A. The effects of whole-body vibration on upper- and lower-body EMG during static and dynamic contractions. Appl. Physiol. Nutr. Metab. 2007, 32, 1156–1163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adsuar, J.C.; Del Pozo-Cruz, B.; Parraca, J.A.; Olivares, P.R.; Gusi, N. Whole body vibration improves the single-leg stance static balance in women with fibromyalgia: A randomized controlled trial. J. Sports Med. Phys. Fit. 2012, 52, 85–91. [Google Scholar]
- Marín, P.J.; Rhea, M.R. Effects of vibration training on muscle power: A meta-analysis. J. Strength Cond. Res. 2010, 24, 871–878. [Google Scholar] [CrossRef]
- Ritzmann, R.; Gollhofer, A.; Kramer, A. The influence of vibration type, frequency, body position and additional load on the neuromuscular activity during whole body vibration. Eur. J. Appl. Physiol. 2013, 113, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Pollock, R.D.; Woledge, R.C.; Mills, K.R.; Martin, F.C.; Di Newham, J. Muscle activity and acceleration during whole body vibration: Effect of frequency and amplitude. Clin. Biomech. 2010, 25, 840–846. [Google Scholar] [CrossRef]
- Aagaard, P. Training-induced changes in neural function. Exerc. Sport Sci. Rev. 2003, 31, 61–67. [Google Scholar] [CrossRef]
- Roelants, M.; Delecluse, C.; Verchueren, S.M. Whole-body-vibration training increases knee-extension strength and speed of movement in older women. J. Am. Geriatr. Soc. 2004, 52, 901–908. [Google Scholar] [CrossRef]
- Marín, P.J.; Bunker, D.; Rhea, M.R.; Ayllón, F.N. Neuromuscular activity during whole-body vibration of different amplitudes and footwear conditions: Implications for prescription of vibratory stimulation. J. Strength Cond. Res. 2009, 23, 2311–2316. [Google Scholar] [CrossRef]
- Zaidell, L.N.; Pollock, R.D.; James, D.C.; Bowtell, J.L.; Newham, D.J.; Sumners, D.P.; Mileva, K.N. Lower Body Acceleration and Muscular Responses to Rotational and Vertical Whole-Body Vibration at Different Frequencies and Amplitudes. Dose Response 2019, 17, 1. [Google Scholar] [CrossRef] [Green Version]
- Pollock, R.D.; Crewther, B.; Cronin, J.; Keogh, J. Gravitational forces and whole body vibration: Implications for prescription of vibratory stimulation. Phys. Ther. Sport 2004, 5, 37–43. [Google Scholar] [CrossRef]
- Nandi, T.; Fisher, B.E.; Hortobágyi, T.; Salem, G.J. Increasing mediolateral standing sway is associated with increasing corticospinal excitability, and decreasing M1 inhibition and facilitation. Gait Posture 2018, 60, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, S.; Günther, M. Human leg impact: Energy dissipation of wobbling masses. Arch. Appl. Mech. 2010, 81, 887–897. [Google Scholar] [CrossRef]
- Saffer, M.; Kiemel, T.; Jeka, J. Coherence analysis of muscle activity during quiet stance. Exp. Brain Res. 2008, 185, 215–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cochrane, D.J.; Loram, I.D.; Stannard, S.R.; Rittweger, J. Changes in joint angle, muscle-tendon complex length, muscle contractile tissue displacement, and modulation of EMG activity during acute whole-body vibration. Muscle Nerve 2009, 40, 420–429. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| CG (n = 20) | RWBV (n = 20) | VWBV (n = 20) | ||
|---|---|---|---|---|
| Mean ± sd | Mean ± sd | Mean ± sd | p | |
| Age (years) | 50.25 ± 8.53 | 52.30 ± 8.04 | 54.85 ± 8.62 | 0.23 |
| BMI | 23.34 ± 1.23 | 22.95 ± 1.30 | 24.21 ± 3.93 | 0.27 |
| Height (centimeters) | 169.15 ± 6.41 | 168.25 ± 6.35 | 166.90 ± 7.86 | 0.58 |
| Weight (kilograms) | 67.00 ± 7.46 | 65.05 ± 5.82 | 67.00 ± 7.43 | 0.59 |
| Pain duration (years) | 7.50 ± 3.22 | 6.75 ± 2.29 | 7.90 ± 2.82 | 0.42 |
| Dependent Variables | Vertical Group (n = 20) | Rotational Group (n = 20) | Control Group (n = 20) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Baseline | After | Follow-up | Baseline | After | Follow-up | Baseline | After | Follow-up | |
| Fibromyalgia Impact Questionnaire | 81.07 (77.74–84.39) | 77.68 (74.36–81.00) | 80.73 (77.22–84.24) | 81.87 (75.84–87.91) | 69.37 (62.24–76.50) | 81.00 (74.70–87.32) | 81.44 (78.30–84.58) | 81.72 (78.61–84.82) | 81.67 (78.63–84.71) |
| Visual Analogue Pain Scale | 7.72 (7.48–7.97) | 7.47 (7.19–7.76) | 7.77 (7.54–8.00) | 7.75 (7.54–7.96) | 7.12 (6.75–7.49) | 7.81 (7.55–8.07) | 7.80 (7.55–8.04) | 7.80 (7.55–8.04) | 7.78 (7.56–8.01) |
| Quality of Life Index | 3.80 (3.32–4.27) | 4.20 (3.81–4.59) | 3.85 (3.39–4.31) | 3.75 (3.35–4.15) | 5.00 (4.54–5.45) | 3.80 (3.33–4.27) | 3.85 (3.34–4.36) | 3.80 (3.33–4.27) | 3.75 (3.25–4.25) |
| Pressure pain sensitivity epicondyles | 21.45 (16.56–26.35) | 22.95 (17.99–27.92) | 21.65 (16.89–26.42) | 21.07 (17.16–24.98) | 29.81 (25.24–34.38) | 21.49 (17.65–25.32) | 21.90 (18.77–25.03) | 22.19 (19.25–25.13) | 22.04 (18.83–25.25) |
| Pressure pain sensitivity index fingers | 36.08 (28.92–43.24) | 38.36 (30.98–45.75) | 35.77 (28.51–43.02) | 35.33 (30.49–40.16) | 47.21 (43.19–51.22) | 35.81 (31.33–40.30) | 35.45 (29.24–41.66) | 35.32 (28.95–41.68) | 35.49 (29.25–41.73) |
| Vibration thresholds index fingers | 3.61 (3.11–4.12) | 3.40 (2.92–3.88) | 3.64 (3.14–4.13) | 3.52 (3.11–3.93) | 2.84 (2.48–3.21) | 3.57 (3.20–3.93) | 3.57 (3.32–3.82) | 3.52 (3.22–3.82) | 3.55 (3.26–3.85) |
| Vibration thresholds toes | 4.40 (3.89–4.90) | 4.28 (3.78–4.78) | 4.37 (3.86–4.87) | 4.37 (3.94–4.81) | 3.68 (3.30–4.07) | 4.43 (3.88–4.98) | 4.51 (4.27–4.74) | 4.50 (4.24–4.76) | 4.50 (4.25–4.75) |
| Berg Scale | 27.95 (25.79–30.11) | 29.60 (27.41–31.79) | 28.15 (26.11–30.19) | 27.00 (24.27–29.73) | 39.10 (36.81–41.39) | 27.25 (24.52–29.98) | 28.15 (26.68–29.62) | 28.45 (27.01–29.89) | 28.40 (26.94–29.86) |
| Six-minute walking test | 385.00 (353.15–416.85) | 394.25 (362.55–425.95) | 382.25 (349.86–414.64) | 365.00 (354.00–376.00) | 415.00 (402.76–427.24) | 358.75 (342.95–374.55) | 391.25 (369.35–413.15) | 387.75 (367.70–407.80) | 383.75 (364.79–402.71) |
| Isometric back muscle strength | 33.85 (31.30–36.40) | 35.70 (33.23–38.17) | 32.75 (30.04–35.46) | 33.40 (31.57–35.23) | 40.85 (38.07–43.63) | 33.45 (31.88–35.02) | 33.05 (30.64–35.46) | 32.85 (30.57–35.13) | 33.10 (29.85–36.35) |
| Mean sway velocity | 0.019 (0.014–0.023) | 0.013 (0.008–0.018) | 0.018 (0.013–0.023) | 0.017 (0.013–0.021) | 0.011 (0.008–0.013) | 0.016 (0.013–0.019) | 0.018 (0.013–0.021) | 0.017 (0.013–0.021) | 0.017 (0.015–0.020) |
| Mediolateral body sway | 0.016 (0.012–0.019) | 0.011 (0.007–0.015) | 0.014 (0.010–0.019) | 0.013 (0.008–0.018) | 0.004 (0.002–0.005) | 0.013 (0.006–0.021) | 0.014 (0.009–0.019) | 0.013 (0.008–0.017) | 0.012 (0.008–0.016) |
| Anteroposterior body sway | 0.013 (0.011–0.015) | 0.012 (0.009–0.014) | 0.013 (0.009–0.016) | 0.015 (0.012–0.017) | 0.013 (0.009–0.016) | 0.015 (0.011–0.019) | 0.013 (0.009–0.016) | 0.012 (0.008–0.016) | 0.012 (0.008–0.016) |
| Gait speed | 3.01 (2.57–3.45) | 3.48 (3.05–3.91) | 3.02 (2.53–3.51) | 2.99 (2.69–3.30) | 3.93 (3.40–4.44) | 3.19 (2.80–3.58) | 3.04 (2.58–3.49) | 3.02 (2.58–3.46) | 3.06 (2.55–3.57) |
| Stride length | 0.97 (0.83–1.13) | 1.00 (0.85–1.15) | 0.93 (0.80–1.06) | 0.88 (0.72–1.03) | 0.95 (0.82–1.08) | 0.93 (0.77–1.08) | 0.93 (0.77–1.10) | 1.13 (0.94–1.31) | 1.05 (0.88–1.22) |
| Percentage of time in the stance phase | 68.30 (65.53–71.07) | 67.41 (65.44–69.37) | 68.76 (66.35–71.16) | 64.75 (57.51–71.99) | 64.84 (60.84–68.85) | 67.56 (65.64–69.47) | 68.48 (65.04–71.91) | 67.56 (63.05–72.07) | 67.94 (64.59–71.29) |
| Percentage of time in the swing phase | 31.69 (28.92–34.47) | 32.59 (30.62–34.55) | 31.24 (28.84–33.64) | 31.77 (29.78–33.76) | 33.45 (31.68–35.22) | 32.44 (30.52–34.35) | 31.52 (28.08–34.95) | 33.93 (30.96–36.90) | 32.25 (28.85–35.65) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mingorance, J.A.; Montoya, P.; Vivas Miranda, J.G.; Riquelme, I. A Comparison of the Effect of Two Types of Whole Body Vibration Platforms on Fibromyalgia. A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 3007. https://doi.org/10.3390/ijerph18063007
Mingorance JA, Montoya P, Vivas Miranda JG, Riquelme I. A Comparison of the Effect of Two Types of Whole Body Vibration Platforms on Fibromyalgia. A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2021; 18(6):3007. https://doi.org/10.3390/ijerph18063007
Chicago/Turabian StyleMingorance, José Antonio, Pedro Montoya, José García Vivas Miranda, and Inmaculada Riquelme. 2021. "A Comparison of the Effect of Two Types of Whole Body Vibration Platforms on Fibromyalgia. A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 18, no. 6: 3007. https://doi.org/10.3390/ijerph18063007