Adverse Childhood Experiences and Psychological Well-Being in Chinese College Students: Mediation Effect of Mindfulness



Abstract
:1. Introduction
2. Conceptual Framework and Hypotheses
2.1. Psychological Well-Being (PWB)
2.2. ACEs and Mindfulness
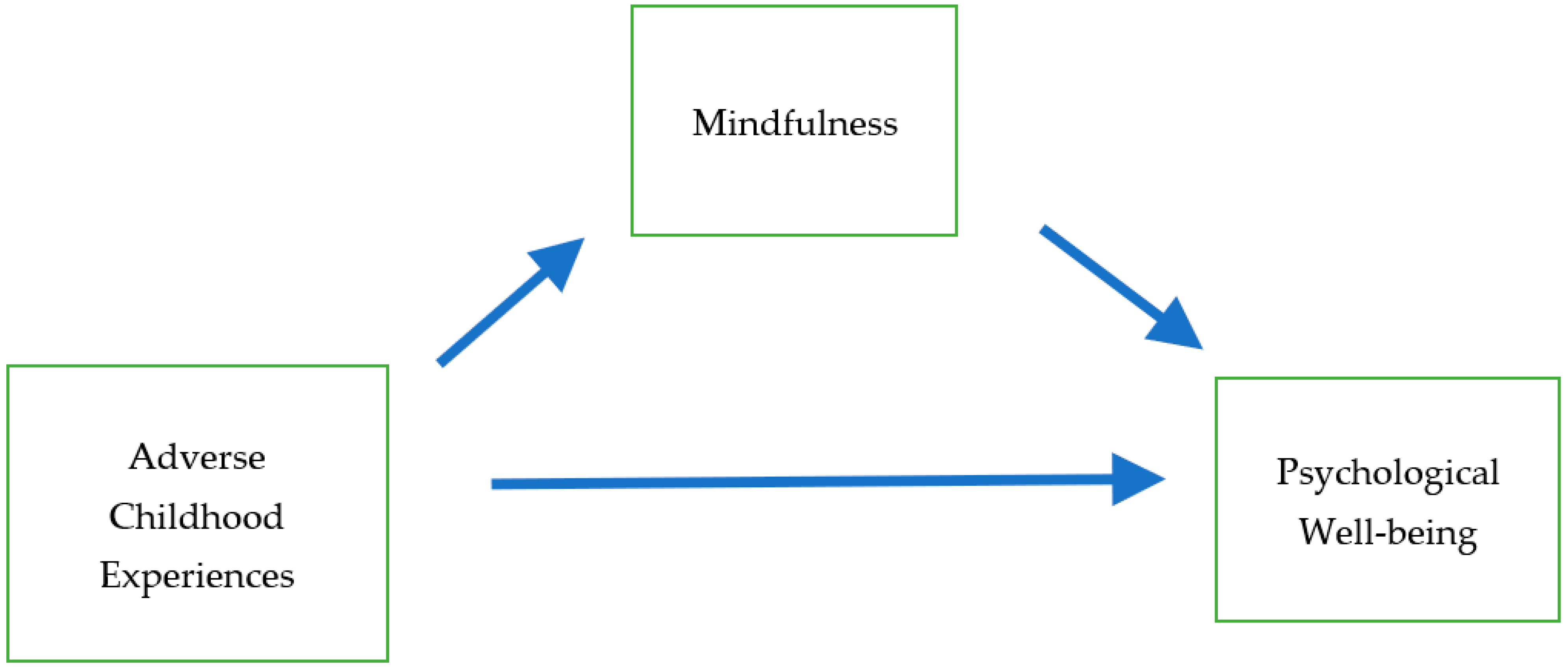
2.3. Conceptual Framework: ACEs, Mindfulness, and PWB
2.4. Hypotheses
3. Data and Method
3.1. Sample and Procedure
3.2. Measures
3.3. Analytical Strategy
4. Results
4.1. Descriptive Statistics
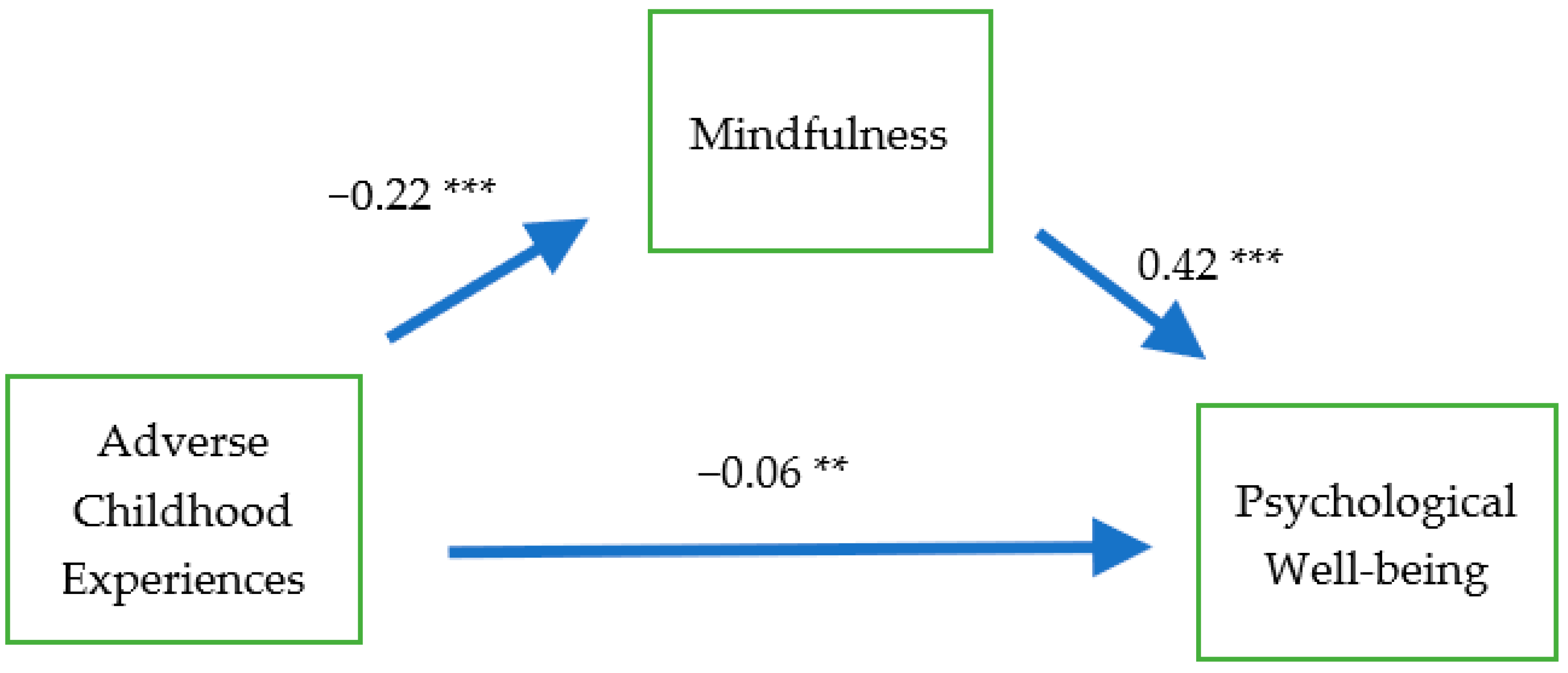
4.2. SEM Analyses
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lyubomirsky, S.; King, L.; Diener, E. The benefits of frequent positive affect: Does happiness lead to success? Psychol. Bull. 2005, 131, 803–855. Available online: https://www.apa.org/pubs/journals/releases/bul-1316803.pdf (accessed on 12 November 2020).
- Staudinger, U.M.; Fleeson, W.; Baltes, P.B. Predictors of subjective physical health and global well-being: Similarities and differences between the United States and Germany. J. Personal. Soc. Psychol. 1999, 76, 305–319. [Google Scholar] [CrossRef]
- Pressman, S.D.; Jenkins, B.N.; Moskowitz, J.T. Positive affect and health: What do we know and where next should we go? Annu. Rev. Psychol. 2019, 70, 627–650. [Google Scholar] [CrossRef] [PubMed]
- Ryff, C.D. Psychological well-being revisited: Advances in the science and practice of eudaimonia. Psychother. Psychosom. 2014, 83, 10–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, S.-T. Generativity in later life: Perceived respect from younger generations as a determinant of goal disengagement and psychological well-being. J. Gerontol. B Psychol. Sci. Soc. Sci. 2009, 64B, 45–54. [Google Scholar] [CrossRef] [Green Version]
- McLaughlin, K.A.; Green, J.G.; Gruber, M.J.; Sampson, N.A.; Zaslavsky, A.; Kessler, R.C. Childhood adversities and first onset of psychiatric disorders in a national sample of US adolescents. Arch. Gen. Psychiatry 2012, 69, 1151–1160. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Fang, S. Adolescents’ mindfulness and psychological distress: The mediating role of emotion regulation. Front. Psychol. 2019, 10, 1358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mosley-Johnson, E.; Garacci, E.; Wagner, N.; Mendez, C.; Williams, J.S.; Egede, L.E. Assessing the relationship between adverse childhood experiences and life satisfaction, psychological well-being, and social well-being: United States Longitudinal Cohort 1995–2014. Qual. Life Res. 2019, 28, 907–914. [Google Scholar] [CrossRef]
- McElroy, S.; Hevey, D. Relationship between adverse early experiences, stressors, psychosocial resources and wellbeing. Child Abus. Negl. 2014, 38, 65–75. [Google Scholar] [CrossRef]
- Merrick, M.T.; Ports, K.A.; Ford, D.C.; Afifi, T.O.; Gershoff, E.T.; Grogan-Kaylor, A. Unpacking the impact of adverse childhood experiences on adult mental health. Child Abus. Negl. 2017, 69, 10–19. [Google Scholar] [CrossRef]
- Nurius, P.S.; Green, S.; Logan-Greene, P.; Boria, S. Life course pathways of adverse childhood experiences toward adult psychological well-being: A stress process analysis. Child Abus. Negl. 2015, 45, 143–153. [Google Scholar] [CrossRef] [Green Version]
- Parto, M.; Besharat, M.A. Mindfulness, psychological well-being and psychological distress in adolescents: Assessing the mediating variables and mechanisms of autonomy and self-regulation. Procedia Soc. Behav. Sci. 2011, 30, 578–582. [Google Scholar] [CrossRef] [Green Version]
- Elmore, A.L.; Crouch, E.; Chowdhury, M.A.K. The interaction of adverse childhood experiences and resiliency on the outcome of depression among children and youth 8–17 years old. Child Abus. Negl. 2020, 107, 104616. [Google Scholar] [CrossRef]
- Arnett, J.J. Emerging adulthood: What is it, and what is it good for? Child Dev. Perspect. 2007, 1, 68–73. [Google Scholar] [CrossRef] [Green Version]
- Arnett, J.J. Emerging adulthood: A theory of development from the late teens through the twenties. Am. Psychol. 2000, 55, 469–480. [Google Scholar] [CrossRef] [PubMed]
- Costa, H.; Ripoll, P.; Sánchez, M.; Carvalho, C. Emotional intelligence and self-efficacy: Effects on psychological well-being in college students. Span. J. Psychol. 2013, 16, E50. [Google Scholar] [CrossRef]
- Li, H.; Meng, L.; Shi, X.; Wu, B. Does attending elite colleges pay in China? J. Comp. Econ. 2012, 40, 78–88. [Google Scholar] [CrossRef]
- Long, M.C. College quality and early adult outcomes. Econ. Educ. Rev. 2008, 27, 588–602. [Google Scholar] [CrossRef]
- Marginson, S. Higher education, economic inequality and social mobility: Implications for emerging East Asia. Int. J. Educ. Dev. 2017, 63, 4–11. [Google Scholar] [CrossRef]
- Ryff, C.D.; Singer, B. Psychological well-being: Meaning, measurement, and implications for psychotherapy research. Psychother. Psychosom. 1996, 65, 14–23. [Google Scholar] [CrossRef]
- Ryff, C.D.; Keyes, C.L.M. The structure of psychological well-being revisited. J. Personal. Soc. Psychol. 1995, 69, 719–727. [Google Scholar] [CrossRef]
- Ryff, C.D. Challenges and Opportunities at The Interface of Aging, Personality, And Well-Being. In Handbook of Personality: Theory and Research; John, O.P., Robins, R.W., Pervin, L.A., Eds.; Guilford Press: New York, NY, USA, 2008; pp. 399–418. [Google Scholar]
- Shields, M.A.; Price, S.W. Exploring the economic and social determinants of psychological well-being and perceived social support in England. J. R. Stat. Soc. Ser. A 2005, 168, 513–538. Available online: https://www.jstor.org/stable/3559837 (accessed on 12 November 2020).
- Steptoe, A. Happiness and health. Annu Rev. Public Health 2019, 40, 339–359. [Google Scholar] [CrossRef] [Green Version]
- Abbott, R.A.; Croudace, T.J.; Ploubidis, G.B.; Kuh, D.; Richards, M.; Huppert, F.A. The relationship between early personality and midlife psychological well-being: Evidence from a UK birth cohort study. Soc. Psychiatry Psychiatr Epidemiol. 2008, 43, 679–687. [Google Scholar] [CrossRef] [Green Version]
- Vohs, K.D.; Baumeister, R.F. Understanding Self-Regulation: An Introduction. In Handbook of Self-Regulation: Research, Theories, and Applications; Baumeister, R.F., Vohs, K.D., Eds.; Guilford Press: New York, NY, USA, 2004; pp. 1–9. [Google Scholar]
- Williams, L.; Gatt, J.; Hatch, A.; Palmer, D.; Nagy, M.; Rennie, C.; Cooper, N.J.; Morris, C.; Grieve, S.; Dobson-Stone, C.; et al. The INTEGRATE model of emotion, thinking and self regulation: An application to the “paradox of aging”. J. Integr. Neurosci. 2008, 7, 367–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fomina, T.; Burmistrova-Savenkova, A.; Morosanova, V. Self-regulation and psychological well-being in early adolescence: A two-wave longitudinal study. Behav. Sci. 2020, 10, 67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, C.L.; Edmondson, D.; Lee, J. Development of self-regulation abilities as predictors of psychological adjustment across the first year of college. J. Adult Dev. 2012, 19, 40–49. [Google Scholar] [CrossRef]
- Giluk, T.L. Mindfulness, Big Five personality, and affect: A meta-analysis. Personal. Individ. Differ. 2009, 47, 805–811. [Google Scholar] [CrossRef]
- Kaunhoven, R.J.; Dorjee, D. How does mindfulness modulate self-regulation in pre-adolescent children? An integrative neurocognitive review. Neurosci. Biobehav. Rev. 2017, 74, 163–184. [Google Scholar] [CrossRef]
- Carlson, J.S.; Yohannan, J.; Darr, C.L.; Turley, M.R.; Larez, N.A.; Perfect, M.M. Prevalence of adverse childhood experiences in school-aged youth: A systematic review (1990–2015). Int. J. Sch. Educ. Psychol. 2020, 8, 2–23. [Google Scholar] [CrossRef]
- Center for Disease Control and Prevention (CDC). About the CDC-Kaiser ACE Study. Available online: https://www.cdc.gov/violenceprevention/aces/about.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fviolenceprevention%2Facestudy%2Fabout.html (accessed on 16 October 2020).
- Felitti, V.J.; Anda, R.F.; Nordenberg, D.; Williamson, D.F.; Spitz, A.M.; Edwards, V.; Koss, M.P.; Marks, J.S. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The Adverse Childhood Experiences (ACE) Study. Am. J. Prev. Med. 1998, 14, 245–258. [Google Scholar] [CrossRef]
- Crandall, A.; Broadbent, E.; Stanfill, M.; Magnusson, B.M.; Novilla, M.L.B.; Hanson, C.L.; Barnes, M.D. The influence of adverse and advantageous childhood experiences during adolescence on young adult health. Child Abus. Negl. 2020, 108, 1–9. [Google Scholar] [CrossRef]
- Isohookana, R.; Riala, K.; Hakko, H.; Räsänen, P. Adverse childhood experiences and suicidal behavior of adolescent psychiatric inpatients. Eur. Child Adolesc. Psychiatry 2013, 22, 13–22. [Google Scholar] [CrossRef]
- Zhang, L.; Mersky, J.P.; Topitzes, J. Adverse childhood experiences and psychological well-being in a rural sample of Chinese young adults. Child Abus. Negl. 2020, 108, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Brown, D.W.; Anda, R.F.; Felitti, V.J.; Edwards, V.J.; Malarcher, A.M.; Croft, J.B.; Giles, W.H. Adverse childhood experiences are associated with the risk of lung cancer: A prospective cohort study. BMC Public Health 2010, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gilbert, L.K.; Breiding, M.J.; Merrick, M.T.; Thompson, W.W.; Ford, D.C.; Dhingra, S.S.; Parks, S.E. Childhood adversity and adult chronic disease: An update from ten states and the District of Columbia, 2010. Am. J. Prev. Med. 2015, 48, 345–349. [Google Scholar] [CrossRef] [PubMed]
- Schütze, I.; Geraedts, K.; Leeners, B. The association between adverse childhood experiences and quality of partnership in adult women. Child Abus. Negl. 2020, 108, 1–11. [Google Scholar] [CrossRef]
- Bishop, S.R.; Lau, M.; Shapiro, S.; Carlson, L.; Anderson, N.D.; Carmody, J.; Segal, Z.V.; Abbey, S.; Speca, M.; Velting, D.; et al. Mindfulness: A proposed operational definition. Clin. Psychol. Sci. Pract. 2004, 11, 230–241. [Google Scholar] [CrossRef]
- Reina, C.S.; Kudesia, R.S. Wherever you go, there you become: How mindfulness arises in everyday situations. Organ. Behav. Hum. Decis. Process. 2020, 159, 78–96. [Google Scholar] [CrossRef]
- Herman, J.L. Trauma and Recovery; Basic Books: New York, NY, USA, 1992. [Google Scholar]
- Herrenkohl, T.I.; Hong, S.; Klika, J.B.; Herrenkohl, R.C.; Russo, M.J. Developmental impacts of child abuse and neglect related to adult mental health, substance use, and physical health. J. Fam. Violence 2013, 28, 191–199. [Google Scholar] [CrossRef]
- Weder, N.; Zhang, H.; Jensen, K.; Yang, B.Z.; Simen, A.; Jackowski, A.; O’Loughlin, K. Child abuse, depression, and methylation in genes involved with stress, neural plasticity, and brain circuitry. J. Am. Acad. Child Adolesc. Psychiatry 2014, 53, 417–424. [Google Scholar] [CrossRef] [Green Version]
- Anda, R.F.; Felitti, R.F.; Walker, J.; Whitfield, C.; Bremner, D.J.; Perry, B.D.; Dube, R.; Giles, W.H. The enduring effects of childhood abuse and related experiences: A convergence of evidence from neurobiology and epidemiology. Eur. Arch. Psychiatr. Clin. Neurosci. 2006, 256, 174–186. [Google Scholar] [CrossRef] [PubMed]
- Caballero, C.; Scherer, E.; West, M.R.; Mrazek, M.D.; Gabrieli, C.F.; Gabrieli, J.D. Greater Mindfulness is Associated with Better Academic Achievement in Middle School. Mind Brain Educ. 2019, 13, 157–166. [Google Scholar] [CrossRef]
- Lu, S.; Huang, C.; Rios, J. Mindfulness and academic performance: An example of migrant children in China. Child Youth Serv. Rev. 2017, 82, 53–59. [Google Scholar] [CrossRef]
- Klingbeil, D.A.; Renshaw, T.L.; Willenbrink, J.B.; Copek, R.A.; Chan, K.T.; Haddock, A.; Yassine, J.; Clifton, J. Mindfulness-based interventions with youth: A comprehensive meta-analysis of group-design studies. J. Sch. Psychol. 2017, 63, 77–103. [Google Scholar] [CrossRef] [PubMed]
- Schonert-Reichl, K.A.; Lawlor, M.S. The effects of a mindfulness-based education program on pre-and early adolescents’ well-being and social and emotional competence. Mindfulness 2010, 1, 137–151. [Google Scholar] [CrossRef]
- Huang, C.-C.; Chen, Y.; Greene, L.; Cheung, S.; Wei, Y. Resilience and emotional and behavioral problems of adolescents in China: Effects of a short-term and intensive mindfulness and life skills training. Child Youth Serv. Rev. 2019, 100, 291–297. [Google Scholar] [CrossRef]
- van de Weijer-Bergsma, E.; Formsma, A.R.; de Bruin, E.I.; Bögels, S.M. The effectiveness of mindfulness training on behavioral problems and attentional functioning in adolescents with ADHD. J. Child Fam. Stud. 2012, 21, 775–787. [Google Scholar] [CrossRef] [Green Version]
- Hollis-Walker, L.; Colosimo, K. Mindfulness, self-compassion, and happiness in non-meditators: A theoretical and empirical examination. Personal. Individ. Differ. 2011, 50, 222–227. [Google Scholar] [CrossRef]
- Lovallo, W.R. Early life adversity reduces stress reactivity and enhances impulsive behavior: Implications for health behaviors. Int. J. Psychophysiol. 2013, 90, 8–16. [Google Scholar] [CrossRef] [Green Version]
- Nagel, K.E.; Dearth-Wesley, T.; Herman, A.N.; Smith, H.G.; Gandica, R.G.; Golden, L.H.; Weil, H.F.C.; Whitaker, R.C. The association between dispositional mindfulness and glycemic control in type 1 diabetes during early adulthood: Differences by age and adverse childhood experiences. Pediatr. Diabetes. 2020, 21, 681–691. [Google Scholar] [CrossRef]
- Voith, L.A.; Russell, K.; Lee, H.; Anderson, R.E. Adverse childhood experiences, trauma symptoms, mindfulness, and intimate partner violence: Therapeutic implications for marginalized men. Fam. Process. 2020, 59, 1588–1607. [Google Scholar] [CrossRef] [PubMed]
- Brett, E.I.; Espeleta, H.C.; Lopez, S.V.; Leavens, E.L.; Leffingwell, T.R. Mindfulness as a mediator of the association between adverse childhood experiences and alcohol use and consequences. Addict. Behav. 2018, 84, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Emirtekin, M.; Balta, S.; Kircaburun, K.; Griffiths, M.D. Childhood emotional abuse and cyberbullying perpetration among adolescents: The mediating role of trait mindfulness. Int. J. Ment. Health Addict. 2020, 18, 1548–1559. [Google Scholar] [CrossRef] [Green Version]
- Whitaker, R.; Dearth-Wesley, T.; Gooze, R.; Becker, B.; Gallagher, K.; McEwen, B. Adverse childhood experiences, dispositional mindfulness, and adult health. Prev. Med. 2014, 67, 147–153. [Google Scholar] [CrossRef]
- Brown, K.W.; West, A.M.; Loverich, T.M.; Biegel, G.M. Assessing adolescent mindfulness: Validation of an Adapted Mindful Attention Awareness Scale in adolescent normative and psychiatric populations. Psychol. Assess. 2011, 23, 1023–1033. [Google Scholar] [CrossRef] [Green Version]
- Deng, Y.Q.; Li, S.; Tang, Y.Y.; Zhu, L.H.; Ryan, R.; Brown, K. Psychometric properties of the Chinese translation of the mindful attention awareness scale (MAAS). Mindfulness 2011, 3, 10–14. [Google Scholar] [CrossRef]
- Gunzler, D.; Chen, T.; Wu, P.; Zhang, H. Introduction to mediation analysis with structural equation modeling. Shanghai Arch. Psychiatry 2013, 25, 390–394. [Google Scholar] [CrossRef]
- Klainin-Yobas, P.; Cho, M.A.; Creedy, D. Efficacy of mindfulness-based interventions on depressive symptoms among people with mental disorders: A meta-analysis. Int. J. Nurs. Stud. 2011, 49, 109–121. [Google Scholar] [CrossRef]
- Zoogman, S.; Goldberg, S.B.; Hoyt, W.T.; Miller, L. Mindfulness Interventions with Youth: A Meta-Analysis. Mindfulness 2014, 6, 290–302. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. Full Catastrophe Living: Using the Wisdom of your Body and Mind to Face Stress, Pain, and Illness; Delacourt: New York, NY, USA, 1990. [Google Scholar]
- Kabat-Zinn, J. Mindfulness-based interventions in context: Past, present, and future. Clin. Psychol. Sci. Pract. 2003, 10, 144–156. [Google Scholar] [CrossRef]
- Shapero, B.G.; Greenberg, J.; Pedrelli, P.; de Jong, M.; Desbordes, G. Mindfulness-based interventions in psychiatry. Focus 2018, 16, 32–39. [Google Scholar] [CrossRef]
- Canby, N.K.; Cameron, I.M.; Calhoun, A.T.; Buchanan, G.M. A brief mindfulness intervention for healthy college students and its effects on psychological distress, self-control, meta-mood, and subjective vitality. Mindfulness 2015, 6, 1071–1081. [Google Scholar] [CrossRef]
- Mermelstein, L.C.; Garske, J.P. A brief mindfulness intervention for college student binge drinkers: A pilot study. Psychol. Addict. Behav. 2015, 29, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Parcover, J.; Coiro, M.J.; Finglass, E.; Barr, E. Effects of a brief mindfulness based group intervention on college students. J. Coll. Stud. Psychother. 2017, 32, 312–329. [Google Scholar] [CrossRef]
- Cheung, S.; Xie, X.; Huang, C.-C. Mind over matter: Mindfulness, income, resilience, and life quality of vocational high school students in China. Int. J. Environ. Res. Public Health 2020, 17, 5701. [Google Scholar] [CrossRef]
- Schwartz, S.J.; Petrova, M. Prevention science in emerging adulthood: A field coming of age. Prev. Sci. 2019, 20, 305–309. [Google Scholar] [CrossRef] [Green Version]
- Baer, R.A.; Smith, G.T.; Lykins, E.; Button, D.; Krietemeyer, J.; Sauer, S.; Walsh, E.; Duggan, D.; Williams, J.M.G. Construct validity of the Five Facet mindfulness Questionnaire in mediating and nonmediating samples. Assessment 2008, 15, 329–342. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Mean (S.D.) | 1 | 2 | 3 | |
|---|---|---|---|---|
| 1. Psychological Wellbeing [24–121] | 81.75 (12.29) | --- | ||
| 2. Mindfulness [15–90] | 59.61 (10.84) | 0.44 *** | --- | |
| 3. Adverse Childhood Experiences [0–10] | 0.69 (1.28) | −0.15 *** | −0.22 *** | --- |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, C.-C.; Tan, Y.; Cheung, S.P.; Hu, H. Adverse Childhood Experiences and Psychological Well-Being in Chinese College Students: Mediation Effect of Mindfulness. Int. J. Environ. Res. Public Health 2021, 18, 1636. https://doi.org/10.3390/ijerph18041636
Huang C-C, Tan Y, Cheung SP, Hu H. Adverse Childhood Experiences and Psychological Well-Being in Chinese College Students: Mediation Effect of Mindfulness. International Journal of Environmental Research and Public Health. 2021; 18(4):1636. https://doi.org/10.3390/ijerph18041636
Chicago/Turabian StyleHuang, Chien-Chung, Yuanfa Tan, Shannon P. Cheung, and Hongwei Hu. 2021. "Adverse Childhood Experiences and Psychological Well-Being in Chinese College Students: Mediation Effect of Mindfulness" International Journal of Environmental Research and Public Health 18, no. 4: 1636. https://doi.org/10.3390/ijerph18041636