
COVID-19 Isolation in Healthy Population in Israel: Challenges in Daily Life, Mental Health, Resilience, and Quality of Life

Abstract
:1. Introduction
2. Materials and Methods
3. Results
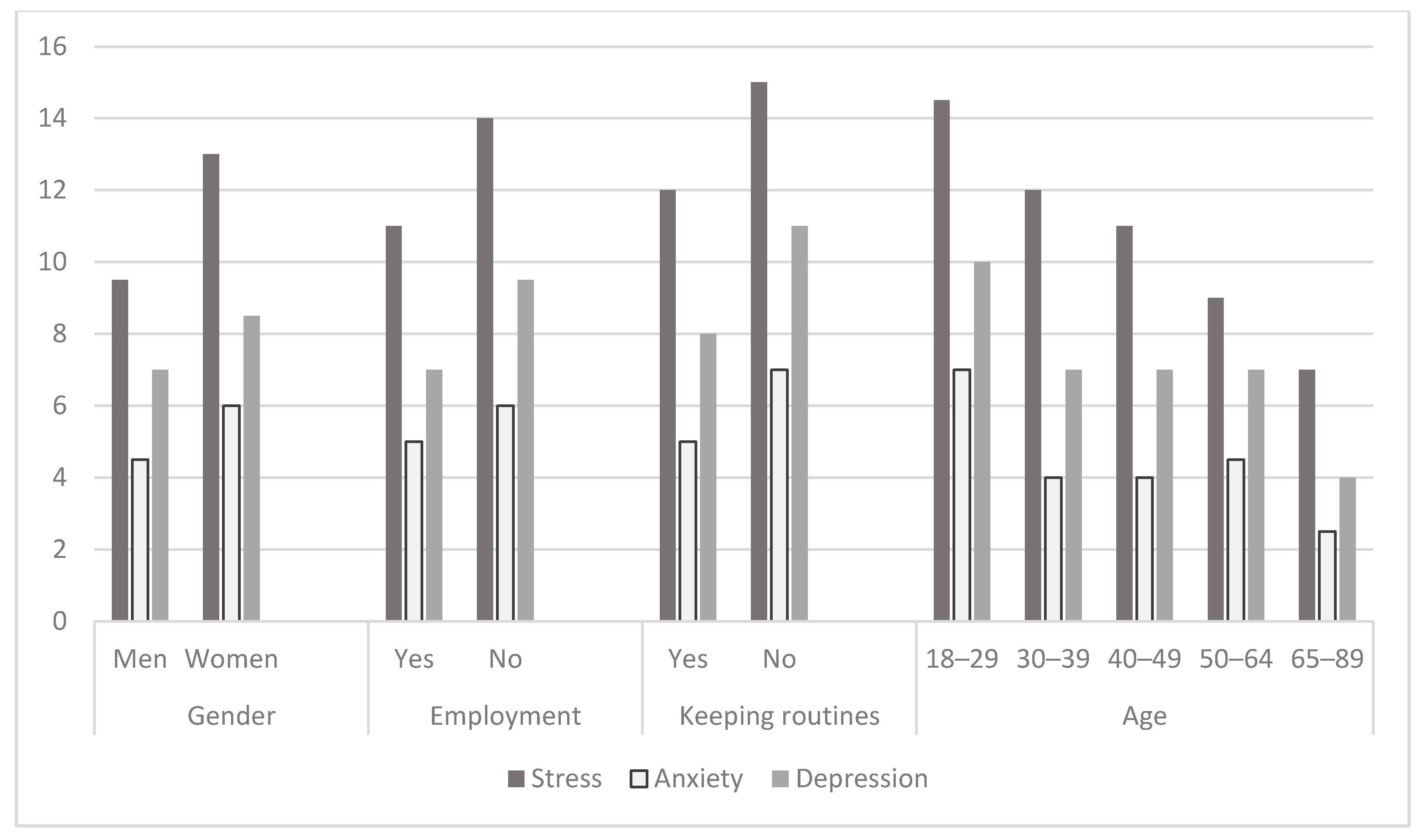
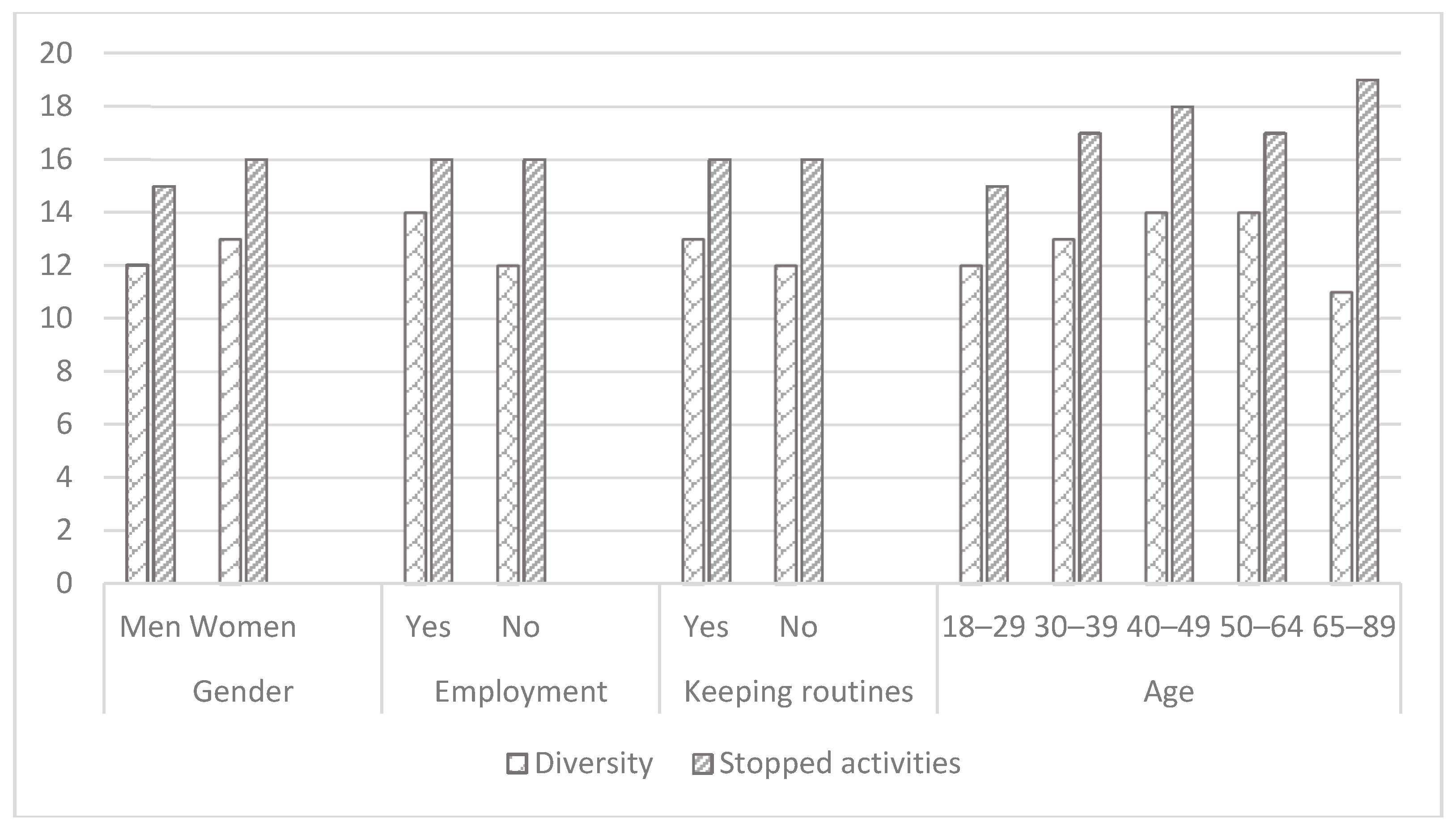
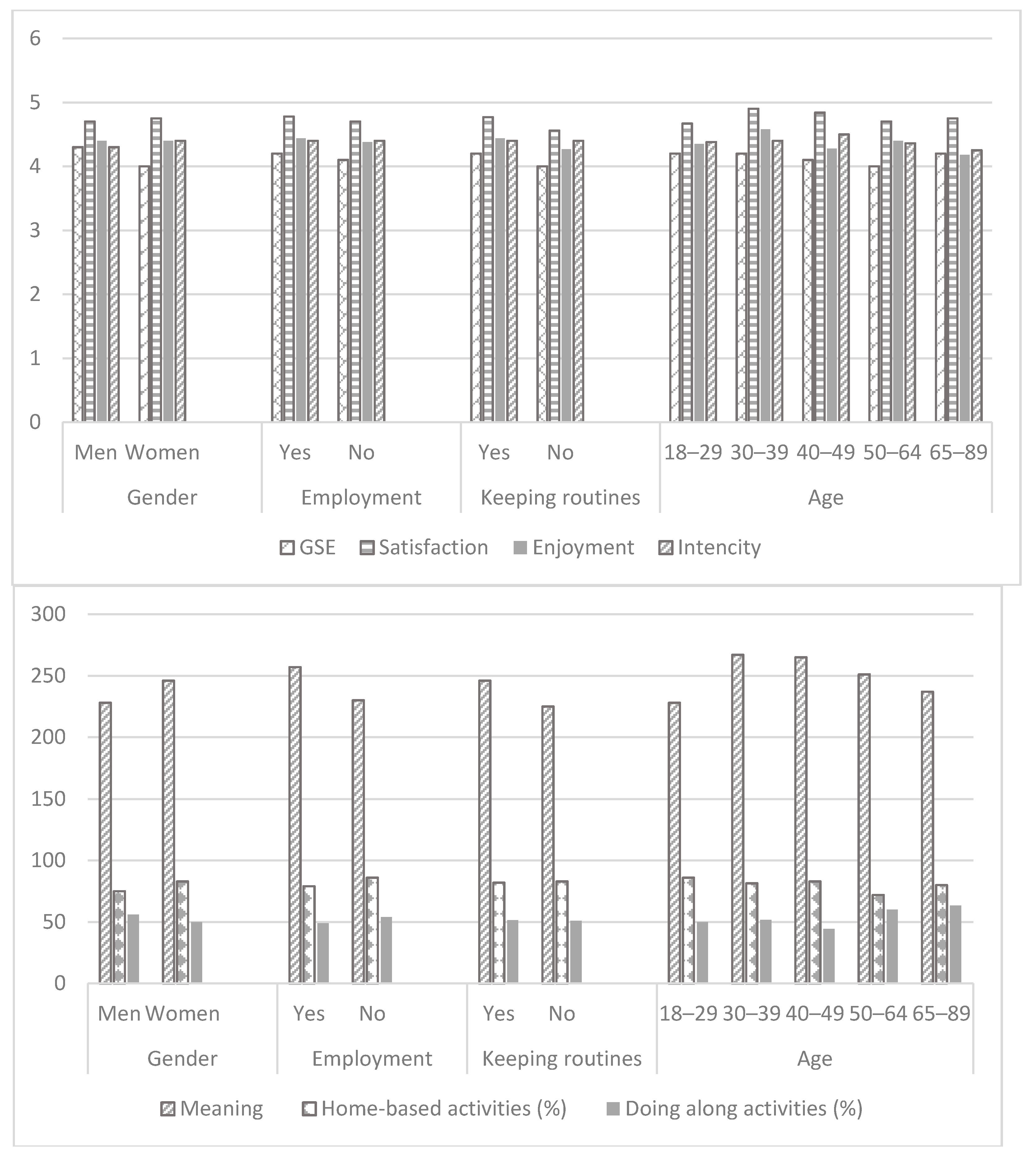
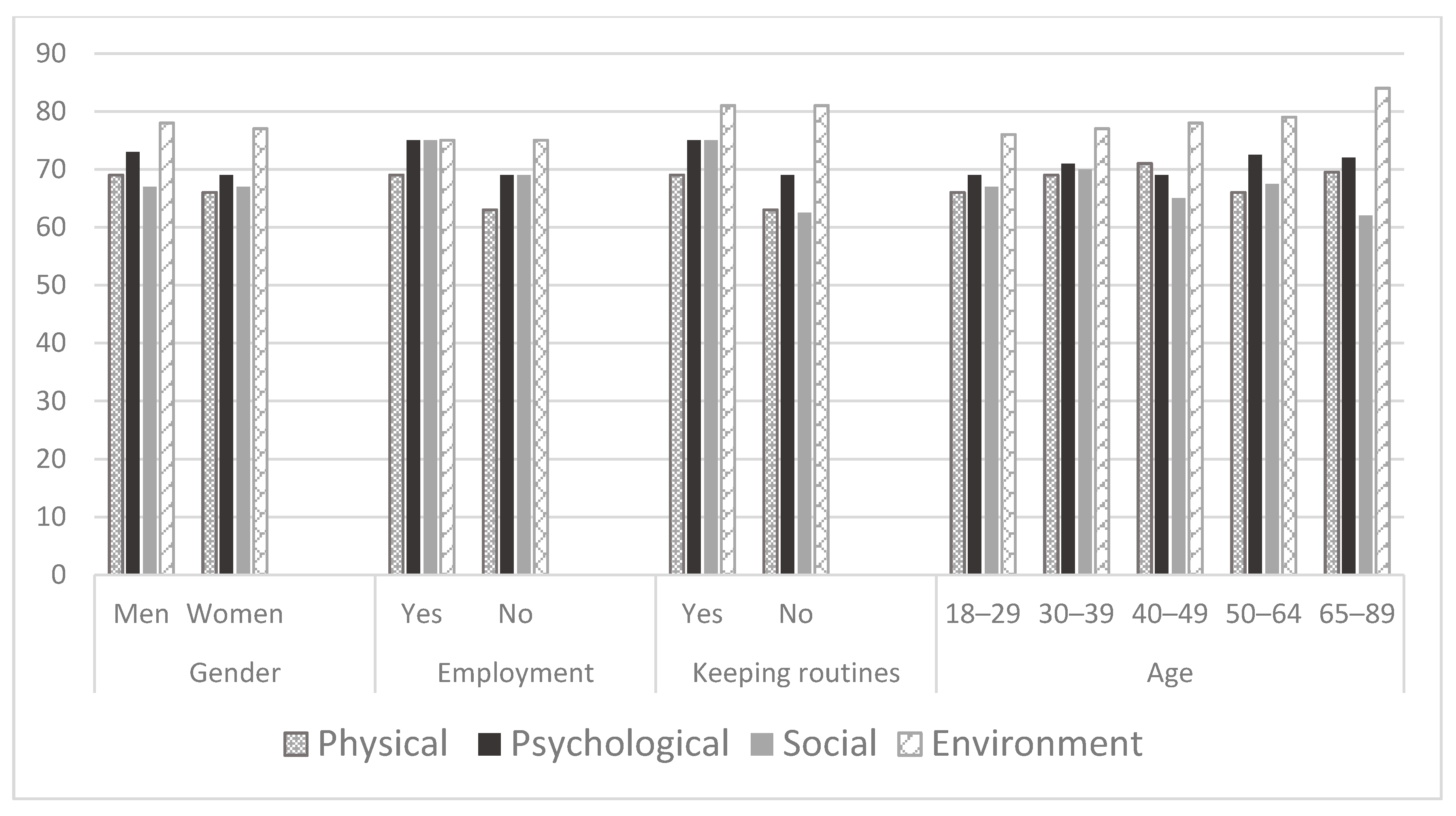
3.1. Descriptive Analysis
3.2. Analysis of Differences
3.3. Correlational Analysis
3.4. Regression Analysis
3.5. Mediation Analysis
4. Discussion
4.1. Psychological Distress and Loneliness
4.2. Participation in Daily Life
4.3. Quality of Life
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vahia, I.V.; Blazer, D.G.; Smith, G.S.; Karp, J.F.; Steffens, D.C.; Forester, B.P.; Tampi, R.; Agronin, M.; Jeste, D.V.; Reynolds, C.F., III. COVID-19, mental health and aging: A need for new knowledge to bridge science and service. Am. J. Geriat. Psychiat. 2020, 28, 695–697. [Google Scholar] [CrossRef]
- Tucci, V.; Moukaddam, N.; Meadows, J.; Shah, S.; Galwankar, S.C.; Kapur, G.B. The forgotten plague: Psychiatric manifestations of ebola, zika, and emerging infectious diseases. J. Glob. Infect. Dis. 2017, 9, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Marijon, E.; Karam, N.; Jost, D.; Perrot, D.; Frattini, B.; Derkenne, C.; Sharifzadehgan, A.; Waldmann, V.; Beganton, F.; Narayanan, K.; et al. Out-of-hospital cardiac arrest during the COVID-19 pandemic in Paris, France: A population-based, observational study. Lancet Pub. Health 2020, 2667, e437–e443. [Google Scholar] [CrossRef]
- Ornell, F.; Schuch, J.B.; Sordi, A.O.; Kessler, F.H.P. “Pandemic fear” and COVID-19: Mental health burden and strategies. Braz. J. Psychiat. 2020, 42, 232–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morens, D.; Fauci, A. Emerging infectious diseases: Threats to human health and global stability. PLoS Pathog. 2013, 9, e1003467. [Google Scholar] [CrossRef] [Green Version]
- Reardon, S. Ebola’s mental-health wounds linger in Africa. Nature 2015, 519, 13–14. [Google Scholar] [CrossRef]
- Shigemura, J.; Ursano, R.J.; Morganstein, J.C.; Kurosawa, M.; Benedek, D.M. Public responses to the novel 2019 coronavirus (2019-nCoV) in Japan: Mental health consequences and target populations. Psychiat. Clin. Neurosci. 2020, 74, 281–282. [Google Scholar] [CrossRef]
- World Health Organization. International Classification of Functioning, Disability and Health (2001); World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- World Health Organization. WHOQOL-BREF: Introduction, Administration, Scoring and Generic Version of the Assessment: Field trial Version, December 1996; World Health Organization: Geneva, Switzerland, 1996. [Google Scholar]
- Brown, D.S.; Thompson, W.W.; Zack, M.M.; Arnold, S.E.; Barile, J.P. Associations between health-related quality of life and mortality in older adults. Prev. Sci. 2015, 16, 21–30. [Google Scholar] [CrossRef] [Green Version]
- Barbisch, D.; Koenig, K.; Shih, F. Is there a case for quarantine? Perspectives from SARS to Ebola. Disaster Med. Public 2015, 9, 547–553. [Google Scholar] [CrossRef] [Green Version]
- Stankovska, G.; Memedi, I.; Dimitrovski, D. Coronavirus COVID-19 disease, mental health and psychosocial support. Soc. Regist. 2020, 4, 33–48. [Google Scholar] [CrossRef]
- Cellini, N.; Canale, N.; Mioni, G.; Costa, S. Changes in sleep pattern, sense of time and digital media use during COVID-19 lockdown in Italy. J. Sleep Res. 2020, e13074. [Google Scholar] [CrossRef] [PubMed]
- American Occupational Therapy Association. Occupational Therapy Practice Framework: Domain and Process (3rd Editon). Am. J. Occup. Ther. 2014, 68 (Suppl. 1), S1–S48. [Google Scholar]
- Bell, L. Storytelling for Social Justice: Connecting Narrative and the Arts in Antiracist Teaching, 2nd ed.; Routledge: New York, NY, USA, 2020; pp. 44–66. [Google Scholar]
- Fong, E.; Ooka, E. Patterns of participation in informal social activities among Chinese immigrants in Toronto. Int. Mig. Rev. 2006, 40, 348–374. [Google Scholar] [CrossRef]
- Hamermesh, D.; Trejo, S. How do immigrants spend their time? The process of assimilation. J. Popul. Econ. 2013, 26, 507–530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pudaric, S.; Sundquist, J.; Johansson, S. Country of birth, instrumental activities of daily living, self-rated health and mortality: A Swedish population-based survey of people aged 55–74. Soc. Sci. Med. 2003, 56, 2493–2503. [Google Scholar] [CrossRef]
- Lades, L.; Laffan, K.; Daly, M.; Delaney, L. Daily emotional well-being during the COVID-19 pandemic. Br. J. Health Psychol. 2020, 1–37. [Google Scholar] [CrossRef]
- Trzebiński, J.; Cabański, M.; Czarnecka, J. Reaction to the COVID-19 pandemic: The influence of meaning in life, life satisfaction, and assumptions on world orderliness and positivity. J. Loss Trauma 2020, 25, 544–557. [Google Scholar] [CrossRef]
- Zaharieva, R. The Dangers of Social Isolation during a Pandemic. COVID-19. Available online: https://epha.org/the-dangers-of-social-isolation-during-a-pandemic/ (accessed on 5 December 2020).
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (covid-19) epidemic among the general population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [Green Version]
- Evans, I.E.; Martyr, A.; Collins, R.; Brayne, C.; Clare, L. Social isolation and cognitive function in later life: A systematic review and meta-analysis. J. Alzheimer’s Dis 2019, 70, S119–S144. [Google Scholar] [CrossRef] [Green Version]
- Gerino, E.; Rollè, L.; Sechi, C.; Brustia, P. Loneliness, resilience, mental health, and quality of life in old age: A structural equation odel. Front. Psychol. 2017, 8, 2003. [Google Scholar] [CrossRef]
- Hawkley, L.; Capitanio, J. Perceived social isolation, evolutionary fitness and health outcomes: A lifespan approach. Philos. Trans. R. Soc. B 2015, 370, 20140114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valtorta, N.; Kanaan, M.; Gilbody, S.; Hanratty, B. Loneliness and social isolation as risk factors for coronary heart disease and stroke: Systematic review and meta-analysis of longitudinal observational studies. Heart 2016, 102, 1009–1016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engelhardt, H.; Buber, I.; Skirbekk, V.; Prskawetz, A. Social involvement, behavioral risks and cognitive functioning among the aged. Ageing Soc. 2010, 30, 779–809. [Google Scholar] [CrossRef]
- Tomioka, K.; Kurumatani, N.; Hosoi, H. Social participation and cognitive decline among community-dwelling older adults: A community-based longitudinal study. J. Gerontol. B 2018, 73, 799–806. [Google Scholar] [CrossRef] [Green Version]
- Schwarzer, R.; Warner, L. Perceived self-efficacy and its relationship to resilience. In Resilience in Children, Adolescents, and Adults; Prince-Embury, S., Saklofske, D., Eds.; Springer: New York, NY, USA, 2013; pp. 139–150. [Google Scholar]
- Jarus, T.; Barnea, R.N.; Waserlauf, L.; Burtz, S.; Yakoel, I.; Gal-On, L.; Grinbaum, S. The development of the Israeli Adults Assessment of Participation. Isr. J. Occup. Ther. 2005, 15, H93–H111. [Google Scholar]
- Henry, J.; Crawford, J. The short-form version of the Depression Anxiety Stress Scales (DASS-21): Construct validity and normative data in a large non-clinical sample. Brit. J. Clin. Psychol. 2005, 44, 227–239. [Google Scholar] [CrossRef] [Green Version]
- Russell, D.; Peplau, L.; Cutrona, C. The revised UCLA Loneliness Scale: Concurrent and discriminant validity evidence. J. Personal. Soc. Psychol. 1980, 39, 472–480. [Google Scholar] [CrossRef]
- Chavis, D.; Lee, K.; Acosta, J. The Sense of Community (SCI) Revised: The Reliability and Validity of the SCI-2. In Proceedings of the 2nd International Community Psychology Conference, Lisboa, Portugal, 4 June 2008. [Google Scholar]
- Chen, G.; Gully, S.; Eden, D. Validation of a new general self-efficacy scale. Organ. Res. Methods 2011, 4, 62–83. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.; Xu, H.; Wu, B. Gender differences in quality of life among community-dwelling older adults in low-and middle-income countries: Results from the Study on global AGEing and adult health (SAGE). BMC Public Health 2020, 20, 114. [Google Scholar] [CrossRef] [Green Version]
- Evans, J.; Repper, J. Employment, social inclusion and mental health. J. Psychiatr. Ment. Health Nurs. 2000, 7, 15–24. [Google Scholar] [CrossRef]
- Hawthorne, G.; Herrman, H.; Murphy, B. Interpreting the WHOQOL-BREF: Preliminary population norms and effect sizes. Soc. Indic. Res. 2006, 77, 37–59. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention, Corona Virus Disease 2019 (2020). Available online: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/older-adults.html (accessed on 20 November 2020).
- Mynard L Normal Life Has been Disrupted: Managing the Disruption Caused by COVID-19. Occupational Therapy Australia. Available online: https://otaus.com.au/publicassets/af469002-6f6a-ea11-9404-005056be13b5/OT%20Guide%20COVID-19%20March%202020.pdf (accessed on 20 November 2020).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gender | Employment Status | Risk Groups | Communication | Keeping Daily Routines | Age | |
|---|---|---|---|---|---|---|
| DASS | ||||||
| Depression | Z = −2.2 p = 0.03 | Z = −3.8 p = 0.001 | Z = −1.77 p > 0.05 | Z = −0.86 p > 0.05 | Z = −3.26 p = 0.001 | H(4) = 22.3 p = 0.001 |
| Anxiety | Z = −2.57 p = 0.01 | Z = −4.1 p = 0.001 | Z = −0.7 p > 0.05 | Z = −1.1 p > 0.05 | Z = −1.08 p > 0.05 | H(4) = 20.3 p = 0.001 |
| Stress | Z = −4.3 p = 0.001 | Z = −3.98 p = 0.001 | Z = −3.3 p = 0.001 | Z = −0.032 p >0.05 | Z = −2 p = 0.042 | H(4) = 29.8 p = 0.001 |
| UCLA | Z = −1.5 p > 0.05 | Z = −2.4 p = 0.018 | Z = −0.35 p > 0.05 | Z = −0.99 p > 0.05 | Z = −2.67 p = 0.008 | H(4) = 1.1 p > 0.05 |
| Sense of Community Index | ||||||
| Reinforcement of needs | Z = −1.9 p > 0.05 | Z = −0.15 p > 0.05 | Z = −0.5 p > 0.05 | Z = −0.17 p > 0.05 | Z = −0.46 p > 0.05 | H(4) = 6 p > 0.05 |
| Membership | Z = −0.04 p > 0.05 | Z = −0.18 p > 0.05 | Z = −0.28 p > 0.05 | Z = −0.26 p > 0.05 | Z = −0.37 p > 0.05 | H(4) = 3.3 p > 0.05 |
| Influence | Z = −0.5 p > 0.05 | Z = −0.46 p > 0.05 | Z = −0.02 p > 0.05 | Z = −0.78 p > 0.05 | Z = −0.04 p > 0.05 | H(4) = 3.4 p > 0.05 |
| Shared Emotional Connection | Z = −1.17 p > 0.05 | Z = −0.43 p > 0.05 | Z = −0.57 p > 0.05 | Z = −0.64 p > 0.05 | Z = −0.37 p > 0.05 | H(4) = 3.2 p > 0.05 |
| GSE | Z = −1.2 p > 0.05 | Z = −2.4 p = 0.017 | Z = −0.79 p > 0.05 | Z = −1.47 p > 0.05 | Z = −3.3 p = 0.001 | H(4) = 6.9 p > 0.05 |
| Adults Subjective Assessment of Participation | ||||||
| Diversity | Z = −2.1 p = 0.039 | Z = −3.78 p = 0.001 | Z = −0.68 p > 0.05 | Z = −0.02 p > 0.05 | Z = −3.55 p = 0.001 | H(4) = 23.75 p = 0.001 |
| Stopped activities | Z = −2.4 p = 0.017 | Z = −0.33 p > 0.05 | Z = −1.9 p > 0.05 | Z = −0.28 p > 0.05 | Z = −0.31 p > 0.05 | H(4) = 30.69 p = 0.001 |
| Intensity | t(568) = −1.44 p > 0.05 | t(569) = 0.09 p > 0.05 | t(569) = −0.77 p > 0.05 | t(569) = 1.52 p > 0.05 | t(569) = −0.59 p > 0.05 | F(4) = 1.74 p > 0.05 |
| Meaning | Z = −3.1 p = 0.003 | Z = −4.3 p = 0.001 | Z = −0.69 p >0.05 | Z = −0.11 p >0.05 | Z = −3.45 p = 0.001 | H(4) = 29.3 p = 0.001 |
| Enjoyment | t(568) = −0.4 p > 0.05 | t(569) = 1.65 p > 0.05 | t(569) = 2 p = 0.044 | t(569) = 1.73 p > 0.05 | t(569) = −2.3 p = 0.024 | F(4) = 4.65 p = 0.001 |
| Satisfaction | t(568) = −1.16 p > 0.05 | t(569) = 2.06, p = 0.04 | t(569) = −0.57 p > 0.05 | t(569) = 0.85 p > 0.05 | t(569) = −2.55 p = 0.011 | F(4) = 2.11 p > 0.05 |
| Activities at home (%) | Z = −3.6 p = 0.001 | Z = −4.3 p = 0.001 | Z = −1.19 p > 0.05 | Z = −0.35 p > 0.05 | Z = −0.92 p > 0.05 | H(4) = 21.6 p = 0.001 |
| Activities alone (%) | Z = −2.5 p = 0.012 | Z = −2.84 p = 0.01 | Z = −2 p = 0.041 | Z = −2 p = 0.045 | Z = −0.56 p > 0.05 | H(4) = 16.85 p = 0.002 |
| WHOQOL-BREF | ||||||
| Physical | Z = −2.28 p = 0.024 | Z = −6.34 p = 0.001 | Z = −1.65 p > 0.05 | Z = −2.54 p = 0.011 | Z = −2.2 p = 0.022 | H(4) = 5.4 p > 0.05 |
| Psychological | Z = −2.33 p = 0.017 | Z = −2.78 p = 0.005 | Z = −0.87 p > 0.05 | Z = −0.27 p > 0.05 | Z = −2.5 p = 0.013 | H(4) = 3.68 p > 0.05 |
| Social | Z = −0.015 p > 0.05 | Z = −2.4 p = 0.015 | Z = −1.04 p > 0.05 | Z = −0.13 p > 0.05 | Z = −3.2 p = 0.001 | H(4) = 3.4 p >0.05 |
| Environmental | Z = −0.81 p > 0.05 | Z = −3 p = 0.003 | Z = −0.29 p > 0.05 | Z = −0.35 p > 0.05 | Z = −0.73 p > 0.05 | H(4) = 10 p = 0.04 |
| WHOQOL-BREF | GSE | DASS | UCLA | Sense of Community Index | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Physical | Psychological | Social | Environmental | Stress | Anxiety | Depression | Reinforcement of Needs | Membership | Influence | Shared Emot. Connect | |||||
| GSE | r | 0.294 ** | 0.484 ** | 0.330 ** | 0.379 ** | ||||||||||
| p | 0.000 | 0.000 | 0.000 | 0.000 | |||||||||||
| DASS | Stress | r | −0.49 ** | −0.6 ** | −0.42 ** | −0.44 ** | −0.29 ** | ||||||||
| p | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | ||||||||||
| Anxiety | r | −0.42 ** | −0.53 ** | −0.39 ** | −0.40 ** | −0.27 ** | 0.73 ** | ||||||||
| p | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | |||||||||
| Depression | r | −0.49 ** | −0.72 ** | −0.48 ** | −0.49 ** | −0.41 ** | 0.76 ** | 0.72 ** | |||||||
| p | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | ||||||||
| UCLA | r | −0.32 ** | −0.51 ** | −0.54 ** | −0.44 ** | −0.39 ** | 0.43 ** | 0.44 ** | 0.56 ** | ||||||
| p | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | |||||||
| Sense of Community Index | Reinforcement of needs | r | 0.14 ** | 0.22 ** | 0.22 ** | 0.23 ** | 0.18 ** | −0.11 * | −0.10 * | −0.17 ** | −0.32 ** | ||||
| p | 0.001 | 0.000 | 0.000 | 0.000 | 0.000 | 0.012 | 0.014 | 0.000 | 0.000 | ||||||
| Membership | r | 0.11 ** | 0.2 ** | 0.16 ** | 0.21 ** | 0.16 ** | −0.06 | −0.05 | −0.11 ** | −0.21 ** | 0.82 ** | ||||
| p | 0.008 | 0.000 | 0.000 | 0.000 | 0.000 | 0.140 | 0.228 | 0.007 | 0.000 | 0.000 | |||||
| Influence | r | 0.11 * | 0.12 ** | 0.11 ** | 0.17 ** | 0.11 ** | −0.01 | −0.01 | −0.06 | −0.19 ** | 0.79 ** | 0.87 ** | |||
| p | 0.012 | 0.004 | 0.009 | 0.000 | 0.007 | 0.895 | 0.813 | 0.131 | 0.000 | 0.000 | 0.000 | ||||
| Shared Emot. Connect | r | 0.10 * | 0.13 ** | 0.14 ** | 0.17 ** | 0.11 ** | −0.02 | −0.02 | −0.07 | −0.17 ** | 0.8 ** | 0.84 ** | 0.89 ** | ||
| p | 0.017 | 0.001 | 0.001 | 0.000 | 0.009 | 0.669 | 0.663 | 0.080 | 0.000 | 0.000 | 0.000 | 0.000 | |||
| Age | r | 0.05 | 0.09 * | 0.01 | 0.16 ** | −0.06 | −0.23 ** | −0.15 ** | −0.19 ** | −0.02 | 0.03 | 0.04 | 0.01 | 0.04 | |
| p | 0.256 | 0.028 | 0.824 | 0.000 | 0.168 | 0.000 | 0.000 | 0.000 | 0.729 | 0.470 | 0.354 | 0.809 | 0.325 | ||
| Adults Subjective Assessment of Participation | Diversity | r | 0.08 | 0.1 * | 0.00 | 0.08 | 0.05 | 0.00 | −0.02 | −0.07 | −0.09 * | 0.06 | 0.05 | 0.09 * | 0.07 |
| p | 0.061 | 0.020 | 0.992 | 0.073 | 0.201 | 0.983 | 0.569 | 0.114 | 0.035 | 0.176 | 0.275 | 0.035 | 0.103 | ||
| Stopped activities | r | −0.09 * | −0.03 | 0.02 | −0.08 * | 0.07 | 0.08 | 0.12 ** | 0.03 | 0.01 | 0.16 ** | 0.16 ** | 0.16 ** | 0.14 ** | |
| p | 0.041 | 0.499 | 0.729 | 0.046 | 0.08 | 0.061 | 0.003 | 0.552 | 0.768 | 0.000 | 0.000 | 0.000 | 0.001 | ||
| Intensity | r | 0.05 | 0.08 | 0.10 * | 0.02 | 0.16 ** | 0.00 | 0.01 | −0.05 | −0.08 | 0.07 | 0.08 | 0.05 | 0.09 * | |
| p | 0.212 | 0.058 | 0.013 | 0.700 | 0.000 | 0.992 | 0.853 | 0.238 | 0.060 | 0.089 | 0.063 | 0.285 | 0.042 | ||
| Meaning | r | 0.1 * | 0.17 ** | 0.1 * | 0.1* | 0.18 ** | 0.00 | −0.02 | −0.11 ** | −0.2 ** | 0.13** | 0.12 ** | 0.14 ** | 0.14 ** | |
| p | 0.018 | 0.000 | 0.013 | 0.015 | 0.000 | 0.967 | 0.689 | 0.007 | 0.000 | 0.002 | 0.006 | 0.001 | 0.001 | ||
| Enjoyment | r | 0.25 ** | 0.31 ** | 0.25 ** | 0.16 ** | 0.22 ** | −0.14 ** | −0.12 ** | −0.21 ** | −0.21 ** | 0.21 ** | 0.17 ** | 0.15 ** | 0.18 ** | |
| p | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.001 | 0.004 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | ||
| Satisfaction | r | 0.27 ** | 0.37 ** | 0.37 ** | 0.23 ** | 0.28 ** | −0.22 ** | −0.22 ** | −0.29 ** | −0.35 ** | 0.17 ** | 0.14 ** | 0.1 * | 0.14 ** | |
| p | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.002 | 0.012 | 0.001 | ||
| Activities at home (%) | r | −0.1 * | −0.06 | 0.04 | −0.07 | 0.02 | 0.09 * | 0.04 | 0.05 | 0.02 | −0.06 | −0.06 | −0.02 | −0.07 | |
| p | 0.016 | 0.152 | 0.384 | 0.079 | 0.567 | 0.043 | 0.309 | 0.208 | 0.634 | 0.155 | 0.175 | 0.569 | 0.085 | ||
| Activities alone (%) | r | −0.07 | −0.03 | −0.13 ** | −0.04 | −0.03 | −0.03 | 0.02 | 0.06 | 0.11 ** | −0.1 * | −0.04 | −0.09 * | −0.05 | |
| p | 0.097 | 0.466 | 0.001 | 0.301 | 0.502 | 0.508 | 0.612 | 0.170 | 0.006 | 0.015 | 0.312 | 0.026 | 0.216 | ||
| WHOQOL-BREF Domains | B | St Error B | β | p Value |
|---|---|---|---|---|
| Physical | ||||
| DASS-Depression | −0.422 | 0.118 | −0.201 | 0.000 |
| DASS-Stress | −0.491 | 0.093 | −0.285 | 0.000 |
| ASAP-Enjoyment | 4.149 | 1.091 | 0.138 | 0.000 |
| ASAP-Number of stopped activities | −0.365 | 0.132 | −0.098 | 0.006 |
| General Self Efficacy | 3.015 | 1.169 | 0.100 | 0.010 |
| SCI-Influence subscale | 0.268 | 0.136 | 0.070 | 0.049 |
| Psychological | ||||
| DASS-Depression | −0.867 | 0.078 | −0.489 | 0.000 |
| DASS-Stress | −0.199 | 0.060 | −0.136 | 0.001 |
| ASAP-Satisfaction | 3.558 | 0.729 | 0.140 | 0.000 |
| General Self Efficacy Scale | 4.941 | 0.773 | 0.193 | 0.000 |
| SCI-Membership subscale | 0.268 | 0.093 | 0.079 | 0.004 |
| Social | ||||
| DASS-Depression | −0.152 | 0.066 | −0.129 | 0.022 |
| DASS-Stress | −0.142 | 0.050 | −0.146 | 0.005 |
| UCLA Loneliness scale | −0.381 | 0.048 | −0.330 | 0.000 |
| ASAP-Satisfaction | 3.221 | 0.602 | 0.190 | 0.000 |
| ASAP-Percent of activities done along | −0.039 | 0.014 | −0.092 | 0.006 |
| Environment | ||||
| DASS-Depression | −0.326 | 0.121 | −0.158 | 0.007 |
| DASS-Stress | −0.233 | 0.090 | −0.137 | 0.010 |
| General Self Efficacy | 6.040 | 1.154 | 0.203 | 0.000 |
| ASAP-Number of stopped activities | −0.492 | 0.131 | −0.134 | 0.000 |
| SCI-Membership subscale | 0.481 | 0.139 | 0.122 | 0.001 |
| UCLA Loneliness scale | −0.373 | 0.086 | −0.185 | 0.000 |
| Age | 0.163 | 0.048 | 0.124 | 0.001 |
| Mediator | Regression Weight | SE | p | |
|---|---|---|---|---|
| Physical | Number of stopped activities | |||
| DASS-Stress | −0.016 | 0.01 | 0.015 | |
| GSE | −0.321 | 0.164 | 0.048 | |
| SCI-Influence | −0.051 | 0.026 | 0.004 | |
| Enjoyment with participation | ||||
| DASS-Depression | −0.042 | 0.018 | 0.004 | |
| GSE | 0.646 | 0.274 | 0.002 | |
| SCI-Influence | 0.068 | 0.03 | 0.001 | |
| Psychological | Satisfaction with participation | |||
| DASS-Depression | −0.048 | 0.018 | 0.001 | |
| GSE | 0.651 | 0.213 | 0.001 | |
| SCI-Membership | 0.034 | 0.02 | 0.06 | |
| Social relationship | Satisfaction with participation | |||
| DASS-Depression | −0.028 | 0.013 | 0.013 | |
| UCLA Loneliness Scale | −0.059 | 0.015 | 0.001 | |
| Percent of activities done along | ||||
| DASS-Depression | −0.013 | 0.009 | 0.046 | |
| DASS-Stress | 0.015 | 0.008 | 0.005 | |
| UCLA Loneliness Scale | −0.013 | 0.007 | 0.01 | |
| Environment | Number of stopped activities | |||
| DASS-Stress | −0.037 | 0.015 | 0.001 | |
| GSE | −0.422 | 0.205 | 0.008 | |
| SCI-Membership | −0.072 | 0.033 | 0.001 | |
| age | −0.038 | 0.012 | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lipskaya-Velikovsky, L. COVID-19 Isolation in Healthy Population in Israel: Challenges in Daily Life, Mental Health, Resilience, and Quality of Life. Int. J. Environ. Res. Public Health 2021, 18, 999. https://doi.org/10.3390/ijerph18030999
Lipskaya-Velikovsky L. COVID-19 Isolation in Healthy Population in Israel: Challenges in Daily Life, Mental Health, Resilience, and Quality of Life. International Journal of Environmental Research and Public Health. 2021; 18(3):999. https://doi.org/10.3390/ijerph18030999
Chicago/Turabian StyleLipskaya-Velikovsky, Lena. 2021. "COVID-19 Isolation in Healthy Population in Israel: Challenges in Daily Life, Mental Health, Resilience, and Quality of Life" International Journal of Environmental Research and Public Health 18, no. 3: 999. https://doi.org/10.3390/ijerph18030999