Emotional and Behavioral Consequences of the COVID-19 Pandemic: The Role of Health Anxiety, Intolerance of Uncertainty, and Distress (In)Tolerance


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedure
2.2. Measures
2.3. Statistical Analyses
3. Results
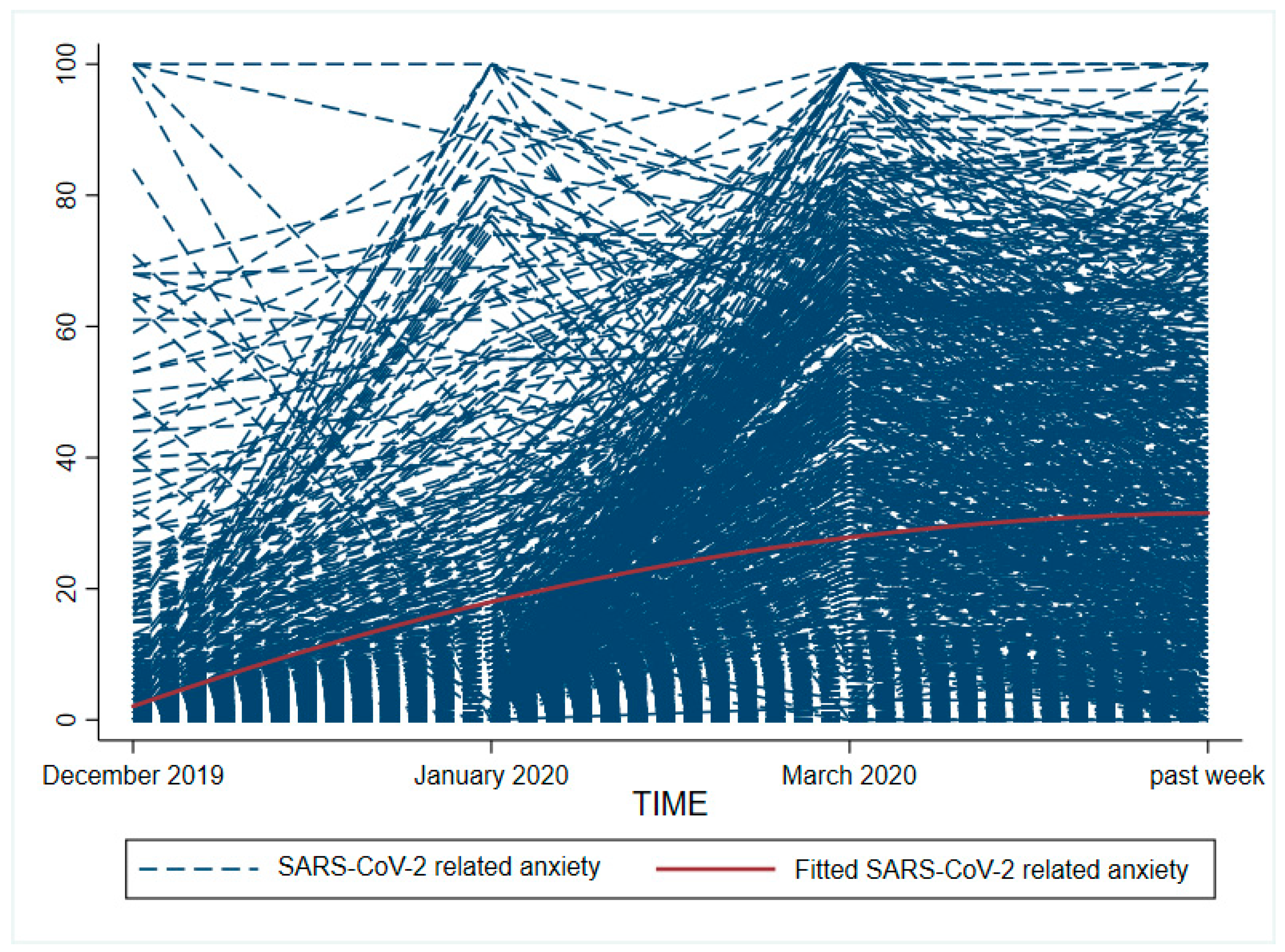
3.1. Course of Health Anxiety and SARS-CoV-2 Related Anxiety
3.2. Comparison of Behavior in Relation to SARS-CoV-2 and to Other Diseases/Viruses
3.3. Prediction of SARS-CoV-2 Related Anxiety during the COVID-19 Pandemic
3.4. Comparison of the Effect of Pre-Existing Health Anxiety on Anxiety in Relation to SARS-CoV-2 and to Other Severe Diseases
3.5. Prediction of SARS-CoV-2 Related Behavior in the Context of the COVID-19 Pandemic and Comparison with Behavior in Relation to Other Severe Diseases/Viruses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, M.Z.; Ahmed, O.; Aibao, Z.; Hanbin, S.; Siyu, L.; Ahmad, A. Epidemic of COVID-19 in China and associated Psychological Problems. Asian J. Psychiatr. 2020, 51, 102092. [Google Scholar] [CrossRef] [PubMed]
- Mazza, C.; Ricci, E.; Biondi, S.; Colasanti, M.; Ferracuti, S.; Napoli, C.; Roma, P. A Nationwide Survey of Psychological Distress among Italian People during the COVID-19 Pandemic: Immediate Psychological Responses and Associated Factors. Int. J. Environ. Res. Public Health 2020, 17, 3165. [Google Scholar] [CrossRef] [PubMed]
- González-Sanguino, C.; Ausín, B.; ÁngelCastellanos, M.; Saiz, J.; López-Gómez, A.; Ugidos, C.; Muñoz, M. Mental Health Consequences during the Initial Stage of the 2020 Coronavirus Pandemic (COVID-19) in Spain. Brain Behav. Immun. 2020. [Google Scholar] [CrossRef]
- Cénat, J.M.; Felix, N.; Blais-Rochette, C.; Rousseau, C.; Bukaka, J.; Derivois, D.; Noorishad, P.-G.; Birangui, J.-P. Prevalence of mental health problems in populations affected by the Ebola virus disease: A systematic review and meta-analysis. Psychiatry Res. 2020, 289, 113033. [Google Scholar] [CrossRef]
- Jones, J.H.; Salathé, M. Early assessment of anxiety and behavioral response to novel swine-origin influenza A(H1N1). PLoS ONE 2009, 4, e8032. [Google Scholar] [CrossRef]
- Goodwin, R.; Gaines, S.O.; Myers, L.; Neto, F. Initial psychological responses to swine flu. Int. J. Behav. Med. 2011, 18, 88–92. [Google Scholar] [CrossRef]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.W.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef]
- Ferguson, E. A taxometric analysis of health anxiety. Psychol. Med. 2009, 39, 277–285. [Google Scholar] [CrossRef]
- Warwick, H.M.; Salkovskis, P.M. Hypochondriasis. Behav. Res. Ther. 1990, 28, 105–117. [Google Scholar] [CrossRef]
- Witthöft, M.; Kerstner, T.; Ofer, J.; Mier, D.; Rist, F.; Diener, C.; Bailer, J. Cognitive Biases in Pathological Health Anxiety. Clin. Psychol. Sci. 2016, 4, 464–479. [Google Scholar] [CrossRef] [Green Version]
- Barsky, A.J.; Wyshak, G. Hypochondriasis and somatosensory amplification. Br. J. Psychiatry 1990, 157, 404–409. [Google Scholar] [CrossRef] [PubMed]
- Jungmann, S.M.; Witthöft, M. Health anxiety, cyberchondria, and coping in the current COVID-19 pandemic: Which factors are related to coronavirus anxiety? J. Anxiety Disord. 2020, 73, 102239. [Google Scholar] [CrossRef] [PubMed]
- Asmundson, G.J.G.; Taylor, S. How health anxiety influences responses to viral outbreaks like COVID-19: What all decision-makers, health authorities, and health care professionals need to know. J. Anxiety Disord. 2020, 71, 102211. [Google Scholar] [CrossRef]
- Bacon, A.M.; Corr, P.J. Coronavirus (COVID-19) in the United Kingdom: A personality-based perspective on concerns and intention to self-isolate. Br. J. Health Psychol. 2020. [Google Scholar] [CrossRef]
- Mertens, G.; Gerritsen, L.; Duijndam, S.; Salemink, E.; Engelhard, I.M. Fear of the coronavirus (COVID-19): Predictors in an online study conducted in March 2020. J. Anxiety Disord. 2020, 74, 102258. [Google Scholar] [CrossRef]
- Gallagher, M.W.; Zvolensky, M.J.; Long, L.J.; Rogers, A.H.; Garey, L. The Impact of Covid-19 Experiences and Associated Stress on Anxiety, Depression, and Functional Impairment in American Adults. Cognit. Ther. Res. 2020, 1–9. [Google Scholar] [CrossRef]
- Lee, S.A.; Jobe, M.C.; Mathis, A.A.; Gibbons, J.A. Incremental validity of coronaphobia: Coronavirus anxiety explains depression, generalized anxiety, and death anxiety. J. Anxiety Disord. 2020, 74, 102268. [Google Scholar] [CrossRef]
- Taylor, S.; Landry, C.A.; Paluszek, M.M.; Fergus, T.A.; McKay, D.; Asmundson, G.J.G. COVID stress syndrome: Concept, structure, and correlates. Depress. Anxiety 2020. [Google Scholar] [CrossRef]
- Taylor, S.; Landry, C.A.; Paluszek, M.M.; Fergus, T.A.; McKay, D.; Asmundson, G.J.G. Development and initial validation of the COVID Stress Scales. J. Anxiety Disord. 2020, 72, 102232. [Google Scholar] [CrossRef]
- Newby, J.M.; Hobbs, M.J.; Mahoney, A.E.J.; Wong, S.K.; Andrews, G. DSM-5 illness anxiety disorder and somatic symptom disorder: Comorbidity, correlates, and overlap with DSM-IV hypochondriasis. J. Psychosom. Res. 2017, 101, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.; Landry, C.A.; Paluszek, M.M.; Asmundson, G.J.G. Reactions to COVID-19: Differential Predictors of Distress, Avoidance, and Disregard for Social Distancing. J. Affect. Disord. 2020. [Google Scholar] [CrossRef] [PubMed]
- Seale, H.; Heywood, A.E.; Leask, J.; Sheel, M.; Thomas, S.; Durrheim, D.N.; Bolsewicz, K.; Kaur, R. COVID-19 is rapidly changing: Examining public perceptions and behaviors in response to this evolving pandemic. PLoS ONE 2020, 15. [Google Scholar] [CrossRef] [PubMed]
- Bish, A.; Michie, S. Demographic and attitudinal determinants of protective behaviours during a pandemic: A review. Br. J. Health Psychol. 2010, 15, 797–824. [Google Scholar] [CrossRef] [PubMed]
- Scherr, C.L.; Jensen, J.D.; Christy, K. Dispositional pandemic worry and the health belief model: Promoting vaccination during pandemic events. J. Public Health (Oxf.) 2017, 39, e242–e250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaygisiz, U.; Gaygisiz, E.; Ozkan, T.; Lajunen, T. Individual differences in behavioral reactions to H1N1 during a later stage of the epidemic. J. Infect. Public Health 2012, 5, 9–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liao, Q.; Cowling, B.J.; Lam, W.W.T.; Ng, D.M.W.; Fielding, R. Anxiety, worry and cognitive risk estimate in relation to protective behaviors during the 2009 influenza A/H1N1 pandemic in Hong Kong: Ten cross-sectional surveys. BMC Infect. Dis. 2014, 14, 169. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.A.; Crunk, E.A. Fear and Psychopathology During the COVID-19 Crisis: Neuroticism, Hypochondriasis, Reassurance-Seeking, and Coronaphobia as Fear Factors. Omega (Westport) 2020, 30222820949350. [Google Scholar] [CrossRef]
- Carleton, R.N. Into the unknown: A review and synthesis of contemporary models involving uncertainty. J. Anxiety Disord. 2016, 39, 30–43. [Google Scholar] [CrossRef] [Green Version]
- Greco, V.; Roger, D. Uncertainty, stress, and health. Pers. Individ. Dif. 2003, 34, 1057–1068. [Google Scholar] [CrossRef]
- Dugas, M.J.; Hedayati, M.; Karavidas, A.; Buhr, K.; Francis, K.; Phillips, N.A. Intolerance of Uncertainty and Information Processing: Evidence of Biased Recall and Interpretations. Cogn. Ther. Res. 2005, 29, 57–70. [Google Scholar] [CrossRef]
- San Martín, C.; Jacobs, B.; Vervliet, B. Further characterization of relief dynamics in the conditioning and generalization of avoidance: Effects of distress tolerance and intolerance of uncertainty. Behav. Res. Ther. 2020, 124, 103526. [Google Scholar] [CrossRef] [PubMed]
- Rosen, N.O.; Knäuper, B. A little uncertainty goes a long way: State and trait differences in uncertainty interact to increase information seeking but also increase worry. Health Commun. 2009, 24, 228–238. [Google Scholar] [CrossRef] [PubMed]
- Fergus, T.A.; Bardeen, J.R. Anxiety sensitivity and intolerance of uncertainty: Evidence of incremental specificity in relation to health anxiety. Pers. Individ. Dif. 2013, 55, 640–644. [Google Scholar] [CrossRef]
- Fetzner, M.G.; Asmundson, G.J.G.; Carey, C.; Thibodeau, M.A.; Brandt, C.; Zvolensky, M.J.; Carleton, R.N. How do elements of a reduced capacity to withstand uncertainty relate to the severity of health anxiety? Cogn. Behav. Ther. 2014, 43, 262–274. [Google Scholar] [CrossRef]
- Deacon, B.; Abramowitz, J.S. Is Hypochondriasis Related to Obsessive-Compulsive Disorder, Panic Disorder, or Both? An Empirical Evaluation. J. Cogn. Psychother. 2008, 22, 115–127. [Google Scholar] [CrossRef]
- Abramowitz, J.S.; Deacon, B.J.; Valentiner, D.P. The Short Health Anxiety Inventory: Psychometric Properties and Construct Validity in a Non-clinical Sample. Cognit. Ther. Res. 2007, 31, 871–883. [Google Scholar] [CrossRef]
- Taha, S.; Matheson, K.; Anisman, H. H1N1 was not all that scary: Uncertainty and stressor appraisals predict anxiety related to a coming viral threat. Stress Health 2014, 30, 149–157. [Google Scholar] [CrossRef]
- Taha, S.; Matheson, K.; Cronin, T.; Anisman, H. Intolerance of uncertainty, appraisals, coping, and anxiety: The case of the 2009 H1N1 pandemic. Br. J. Health Psychol. 2014, 19, 592–605. [Google Scholar] [CrossRef]
- Satici, B.; Saricali, M.; Satici, S.A.; Griffiths, M.D. Intolerance of Uncertainty and Mental Wellbeing: Serial Mediation by Rumination and Fear of COVID-19. Int. J. Ment. Health Addict. 2020, 1–12. [Google Scholar] [CrossRef]
- Tull, M.T.; Barbano, A.C.; Scamaldo, K.M.; Richmond, J.R.; Edmonds, K.A.; Rose, J.P.; Gratz, K.L. The prospective influence of COVID-19 affective risk assessments and intolerance of uncertainty on later dimensions of health anxiety. J. Anxiety Disord. 2020, 75, 102290. [Google Scholar] [CrossRef] [PubMed]
- Rettie, H.; Daniels, J. Coping and tolerance of uncertainty: Predictors and mediators of mental health during the COVID-19 pandemic. Am. Psychol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Simons, J.S.; Gaher, R.M. The Distress Tolerance Scale: Development and Validation of a Self-Report Measure. Motiv. Emot. 2005, 29, 83–102. [Google Scholar] [CrossRef]
- Keough, M.E.; Riccardi, C.J.; Timpano, K.R.; Mitchell, M.A.; Schmidt, N.B. Anxiety symptomatology: The association with distress tolerance and anxiety sensitivity. Behav. Ther. 2010, 41, 567–574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hunt, C.; Cooper, S.E.; Hartnell, M.P.; Lissek, S. Distraction/Suppression and Distress Endurance diminish the extent to which generalized conditioned fear is associated with maladaptive behavioral avoidance. Behav. Res. Ther. 2017, 96, 90–105. [Google Scholar] [CrossRef]
- Fergus, T.A.; Bardeen, J.R.; Orcutt, H.K. Examining the Specific Facets of Distress Tolerance That Are Relevant to Health Anxiety. J. Cogn. Psychother. 2015, 29, 32–44. [Google Scholar] [CrossRef]
- Liu, C.H.; Zhang, E.; Wong, G.T.F.; Hyun, S.; Hahm, H.C. Factors associated with depression, anxiety, and PTSD symptomatology during the COVID-19 pandemic: Clinical implications for U.S. young adult mental health. Psychiatry Res. 2020, 290, 113172. [Google Scholar] [CrossRef]
- Robert Koch Institut. Daily Status Report of the RKI on the Coronavirus-Disease-2019 (COVID-19) 20.04.2020—Updated Status for Germany. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Situationsberichte/2020-04-20-de.pdf?__blob=publicationFile (accessed on 2 October 2020).
- Robert Koch Institut. Daily Status Report of the RKI on the Coronavirus-Disease-2019 (COVID-19) 15.05.2020—Updated Stand. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Situationsberichte/2020-05-15-de.pdf?__blob=publicationFile (accessed on 2 October 2020).
- Salkovskis, P.M.; Rimes, K.A.; Warwick, H.M.C.; Clark, D.M. The Health Anxiety Inventory: Development and validation of scales for the measurement of health anxiety and hypochondriasis. Psychol. Med. 2002, 32, 843–853. [Google Scholar] [CrossRef]
- Bailer, J.; Rist, F.; Müller, T.; Mier, D.; Diener, C.; Ofer, J.; Fenske, S.; Witthöft, M. Erfassung von Krankheitsangst mit dem Short Health Anxiety Inventory. Verhaltenstherapie Verhaltensmedizin 2013, 34, 378–398. [Google Scholar]
- Weck, F.; Brehm, U.; Schermelleh-Engel, K. Entwicklung und Validierung eines Fragebogens zur Erfassung von hypochondrischem Sicherheitsverhalten. Zeitschrift für Klinische Psychologie und Psychotherapie 2012, 41, 271–281. [Google Scholar] [CrossRef]
- Gerlach, A.L.; Andor, T.; Patzelt, J. Die Bedeutung von Unsicherheitsintoleranz für die Generalisierte Angststörung Modellüberlegungen und Entwicklung einer deutschen Version der Unsicherheitsintoleranz-Skala. Zeitschrift für Klinische Psychologie und Psychotherapie 2008, 37, 190–199. [Google Scholar] [CrossRef]
- Buhr, K.; Dugas, M.J. The intolerance of uncertainty scale: Psychometric properties of the English version. Behav. Res. Ther. 2002, 40, 931–945. [Google Scholar] [CrossRef]
- Freeston, M.H.; Rheaume, J.; Letarte, H.; Dugas, M.J.; Ladouceur, R. Why do people worry? Pers. Individ. Dif. 1994, 17, 791–802. [Google Scholar] [CrossRef]
- McHugh, R.K.; Otto, M.W. Refining the measurement of distress intolerance. Behav. Ther. 2012, 43, 641–651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reiss, S.; Peterson, R.A.; Gursky, D.M.; McNally, R.J. Anxiety sensitivity, anxiety frequency and the prediction of fearfulness. Behav. Res. Ther. 1986, 24, 1–8. [Google Scholar] [CrossRef]
- Harrington, N. The Frustration Discomfort Scale: Development and psychometric properties. Clin. Psychol. Psychother. 2005, 12, 374–387. [Google Scholar] [CrossRef]
- Schmidt, N.B.; Richey, J.A.; Fitzpatrick, K.K. Discomfort intolerance: Development of a construct and measure relevant to panic disorder. J. Anxiety Disord. 2006, 20, 263–280. [Google Scholar] [CrossRef]
- Otto, J.; Linden, M. Die deutsche Übersetzung der Distress-Intoleranz-Skala. Verhaltenstherapie 2019, 29, 108–112. [Google Scholar] [CrossRef]
- Singer, J.D.; Willett, J.B. Applied Longitudinal Data Analysis: Modeling Change and Event Occurence; Oxford University Press: New York, NY, USA, 2003. [Google Scholar]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Press: New York, NY, USA, 2017. [Google Scholar]
- Robert Koch Institut. Nowcasting und R-Schätzung: Schätzung der aktuellen Entwicklung der SARS-CoV-2-Epidemie in Deutschland. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Projekte_RKI/Nowcasting.html (accessed on 2 October 2020).
- Liao, Q.; Wu, P.; Wing Tak Lam, W.; Cowling, B.J.; Fielding, R. Trajectories of public psycho-behavioural responses relating to influenza A(H7N9) over the winter of 2014-15 in Hong Kong. Psychol. Health 2019, 34, 162–180. [Google Scholar] [CrossRef]
- Cheng, C.; Cheung, M.W.L. Psychological responses to outbreak of severe acute respiratory syndrome: A prospective, multiple time-point study. J. Pers. 2005, 73, 261–285. [Google Scholar] [CrossRef]
- Balkhi, F.; Nasir, A.; Zehra, A.; Riaz, R. Psychological and Behavioral Response to the Coronavirus (COVID-19) Pandemic. Cureus 2020, 12, e7923. [Google Scholar] [CrossRef] [PubMed]
- Creed, F.; Barsky, A. A systematic review of the epidemiology of somatisation disorder and hypochondriasis. J. Psychosom. Res. 2004, 56, 391–408. [Google Scholar] [CrossRef]
- Mitchell, M.A.; Riccardi, C.J.; Keough, M.E.; Timpano, K.R.; Schmidt, N.B. Understanding the associations among anxiety sensitivity, distress tolerance, and discomfort intolerance: A comparison of three models. J. Anxiety Disord. 2013, 27, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, A.; Zvolensky, M.J.; Vujanovic, A.A.; Moos, R. Integrating anxiety sensitivity, distress tolerance, and discomfort intolerance: A hierarchical model of affect sensitivity and tolerance. Behav. Ther. 2009, 40, 291–301. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| M | SD | N | % | |
|---|---|---|---|---|
| Anxiety related to SARS-CoV-2 (0–100) | ||||
| December 2019 a | 4.44 | 11.97 | ||
| January 2020 a | 10.93 | 19.37 | ||
| March 2020 a | 34.90 | 27.97 | ||
| past week | 29.20 | 25.37 | ||
| Anxiety related to other severe diseases (0–100) | ||||
| December 2019 a | 12.21 | 18.86 | ||
| January 2020 a | 13.19 | 20.16 | ||
| March 2020 a | 13.24 | 19.70 | ||
| past week | 13.22 | 19.81 | ||
| Health anxiety (SHAI) pre COVID-19 b | ||||
| total (0–54) | 14.00 | 7.13 | ||
| subscale “health anxiety” (0–42) | 11.08 | 5.97 | ||
| subscale “negative consequences of illness” (0–12) | 2.92 | 1.97 | ||
| Health anxiety (SHAI) during COVID-19 | ||||
| total (0–54) | 17.16 | 8.45 | ||
| subscale “health anxiety” (0–42) | 13.88 | 7.04 | ||
| subscale “negative consequences of illness” (0–12) | 3.29 | 2.18 | ||
| Hypochondriacal safety behavior (QSBH) pre COVID-19 c | ||||
| subscale “reassurance” (original version) (0–32) | 9.88 | 4.92 | ||
| subscale “avoidance” (original version) (0–32) | 11.26 | 6.77 | ||
| subscale “reassurance” (shortened version) (0–20) | 6.33 | 3.39 | ||
| subscale “avoidance” (shortened version) (0–20) | 4.56 | 4.29 | ||
| Hypochondriacal safety behavior (QSBH) during COVID-19 | ||||
| subscale “reassurance”—SARS-CoV-2 (0–20) | 6.53 | 3.75 | ||
| subscale “reassurance”—other severe diseases (0–20) | 5.90 | 3.53 | ||
| subscale “avoidance”—SARS-CoV-2 (0–20) | 4.36 | 4.20 | ||
| subscale “avoidance”—other severe diseases (0–20) | 4.17 | 4.49 | ||
| Preventive behavior pre COVID-19 d | ||||
| total (0–16) | 4.70 | 3.12 | ||
| Buying or using toiletries (e.g., disinfectants) | 1.21 | 1.08 | ||
| Washing hands | 2.33 | 1.10 | ||
| Buying or using respiratory masks | 0.30 | 0.85 | ||
| Avoiding places | 0.85 | 1.11 | ||
| Preventive behavior during COVID-19 | ||||
| total—SARS-CoV-2 (0–16) | 10.75 | 3.50 | ||
| total—other infections (0–16) | 5.24 | 3.45 | ||
| Buying or using toiletries (e.g., disinfectants)—SARS-CoV-2 | 2.26 | 1.23 | ||
| Buying or using toiletries (e.g., disinfectants)—other infections | 1.36 | 1.21 | ||
| Washing hands—SARS-CoV-2 | 3.35 | 0.84 | ||
| Washing hands—other infections | 2.35 | 1.19 | ||
| Buying or using respiratory masks—SARS-CoV-2 | 2.48 | 1.29 | ||
| Buying or using respiratory masks—other infections | 0.41 | 0.92 | ||
| Avoiding places—SARS-CoV-2 | 2.66 | 1.25 | ||
| Avoiding places—other infections | 1.11 | 1.25 | ||
| Most feared disease at the moment | ||||
| Infection with SARS-CoV-2 (incl. COVID-19) | 292 | 32.90 | ||
| Cancer | 107 | 12.10 | ||
| Mental disorders | 93 | 10.50 | ||
| Cardiovascular diseases | 63 | 7.10 | ||
| Respiratory diseases | 15 | 1.70 | ||
| Neurological diseases | 14 | 1.60 | ||
| Injuries/poisoning | 7 | 0.80 | ||
| Other infections | 3 | 0.30 | ||
| Others | 22 | 2.50 | ||
| No disease | 271 | 30.60 | ||
| Intolerance of uncertainty (IU-18) | ||||
| total (18–90) | 47.39 | 14.82 | ||
| subscale “reduced ability to act due to IU” (6–30) | 14.13 | 5.71 | ||
| subscale “burden due to IU” (6–30) | 16.64 | 5.61 | ||
| subscale “vigilance due to IU” (6–30) | 16.62 | 5.37 | ||
| Distress intolerance (Distress intolerance scale) | ||||
| total (10–50) | 24.63 | 9.34 |
| Reassurance Behavior | Avoidance Behavior | Preventive Behavior | |||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SARS-CoV-2 | Other Diseases | SARS-CoV-2 | Other Diseases | SARS-CoV-2 | Other Viruses | ||||||||||||||||||||||
| M | SD | M | SD | BCa 99% CI | |t| | df | p | d | M | SD | M | SD | BCa 99% CI | |t| | df | p | d | M | SD | M | SD | BCa 99% CI | |t| | df | p | d | |
| Female | 6.63 | 3.75 | 6.00 | 3.52 | [0.33, 0.91] | 5.56 | 694 | <0.001 | 0.17 | 4.45 | 4.21 | 4.10 | 4.38 | [0.03, 0.67] | 2.76 | 694 | 0.01 | 0.08 | 15.03 | 3.29 | 9.36 | 3.42 | [5.33, 6.01] | 42.20 | 694 | <0.001 | 1.69 |
| Male | 6.22 | 3.75 | 5.53 | 3.54 | [0.06, 1.35] | 2.99 | 187 | 0.003 | 0.19 | 3.96 | 4.12 | 4.43 | 4.87 | [−1.02, 0.24] | 1.68 | 187 | 0.10 | 0.10 | 13.77 | 4.03 | 8.86 | 3.51 | [4.18, 5.60] | 18.33 | 187 | <0.001 | 1.29 |
| Young | 6.15 | 3.57 | 5.53 | 3.48 | [0.23, 1.01] | 4.09 | 404 | <0.001 | 0.18 | 4.28 | 4.21 | 3.07 | 3.88 | [0.76, 1.66] | 6.91 | 404 | <0.001 | 0.30 | 14.63 | 3.33 | 8.98 | 3.49 | [5.20, 6.10] | 33.55 | 404 | <0.001 | 1.66 |
| Middle | 6.91 | 3.91 | 6.24 | 3.64 | [0.22, 1.11] | 4.03 | 344 | <0.001 | 0.18 | 4.59 | 4.44 | 4.99 | 4.95 | [−0.85, 0.08] | 2.22 | 344 | 0.03 | 0.08 | 14.64 | 3.75 | 9.54 | 3.56 | [4.59, 5.61] | 24.79 | 344 | <0.001 | 1.40 |
| Old | 6.72 | 3.78 | 6.11 | 3.29 | [0.01, 1.26] | 2.52 | 136 | 0.01 | 0.17 | 3.99 | 3.45 | 5.34 | 4.22 | [−2.01, −0.72] | 5.48 | 136 | <0.001 | 0.34 | 15.36 | 3.31 | 9.28 | 2.93 | [5.31, 6.82] | 20.87 | 136 | <0.001 | 1.94 |
| Parameter | Estimate | SE | p | |
|---|---|---|---|---|
| Fixed effects | ||||
| Initial level | b0 | 1.93 | 0.62 | 0.002 |
| Time a | b1 | 18.33 | 0.91 | <0.001 |
| Time 2 a | b2 | −2.96 | 0.29 | <0.001 |
| Health anxiety b | b3 | −0.07 | 0.09 | 0.46 |
| Health anxiety b × Time a | b4 | 1.10 | 0.14 | <0.001 |
| Health anxiety b × Time2 a | b5 | −0.18 | 0.04 | <0.001 |
| Intolerance of uncertainty | b6 | −0.01 | 0.06 | 0.83 |
| Intolerance of uncertainty × Time a | b7 | 0.02 | 0.09 | 0.85 |
| Intolerance of uncertainty × Time2 a | b8 | 0.01 | 0.03 | 0.68 |
| Distress intolerance | b9 | 0.04 | 0.09 | 0.64 |
| Distress intolerance × Time a | b10 | −0.06 | 0.14 | 0.68 |
| Distress intolerance × Time 2 a | b11 | 0.01 | 0.04 | 0.77 |
| Random effects | ||||
| Variance initial level | b0i | 38.60 | 9.65 | <0.001 |
| Variance quadratic slope (Time 2 a) | b1i | 1.51 | 0.39 | <0.001 |
| Covariance initial level−quadratic slope (Time 2 a) | 7.58 | |||
| Goodness-of-fit | ||||
| Akaike information criterion | AIC | 30,988.22 | ||
| Bayesian information criterion | BIC | 31,087.01 | ||
| Reassurance Behavior | Avoidance Behavior | Preventive Behavior | ||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SARS-CoV-2 | Other Diseases | SARS-CoV-2 | Other Diseases | SARS-CoV-2 | Other Diseases | |||||||||||||||||||
| b | 99% CI [LL, UL] | p | b | 99% CI [LL, UL] | p | b | 99% CI [LL, UL] | p | b | 99% CI [LL, UL] | p | b | 99% CI [LL, UL] | p | b | 99% CI [LL, UL] | p | |||||||
| HA pre | −0.001 | −0.05 | 0.05 | 0.96 | 0.004 | −0.03 | 0.04 | 0.80 | 0.004 | −0.05 | 0.06 | 0.85 | 0.02 | −0.02 | 0.06 | 0.24 | 0.06 | 0.01 | 0.11 | 0.005 | 0.02 | −0.02 | 0.05 | 0.30 |
| DI a | 0.04 | −0.01 | 0.08 | 0.03 | 0.03 | 0.01 | 0.06 | 0.003 | 0.07 | 0.02 | 0.12 | 0.001 | 0.04 | 0.002 | 0.08 | 0.01 | 0.02 | −0.03 | 0.06 | 0.31 | 0.03 | −0.01 | 0.06 | 0.11 |
| IU b | 0.01 | −0.01 | 0.04 | 0.23 | −0.004 | −0.02 | 0.01 | 0.55 | 0.004 | −0.03 | 0.04 | 0.74 | −0.005 | −0.03 | 0.02 | 0.55 | 0.02 | −0.01 | 0.04 | 0.12 | 0.01 | −0.02 | 0.03 | 0.36 |
| HA pre x DI a | −0.003 | −0.01 | 0.004 | 0.32 | −0.001 | −0.01 | 0.004 | 0.61 | 0.001 | −0.01 | 0.01 | 0.76 | <0.001 | −0.005 | 0.004 | 0.98 | −0.004 | −0.01 | 0.002 | 0.11 | 0.001 | −0.01 | 0.01 | 0.80 |
| HA pre x IU b | 0.003 | −0.001 | 0.01 | 0.09 | 0.001 | −0.001 | 0.004 | 0.18 | −0.002 | −0.01 | 0.003 | 0.29 | <0.001 | −0.003 | 0.003 | 0.89 | 0.001 | −0.003 | 0.004 | 0.74 | <0.001 | -0.004 | 0.003 | 0.79 |
| Behavior pre c | 0.59 | 0.49 | 0.69 | <0.001 | 0.82 | 0.75 | 0.89 | <0.001 | 0.50 | 0.42 | 0.59 | <0.001 | 0.88 | 0.82 | 0.93 | <0.001 | 0.40 | 0.32 | 0.49 | <0.001 | 0.72 | 0.63 | 0.81 | <0.001 |
| R2 | 0.35 | 0.68 | 0.34 | 0.76 | 0.18 | 0.46 | ||||||||||||||||||
| Reassurance Behavior | Avoidance Behavior | Preventive Behavior | ||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SARS-CoV-2 | Other Diseases | SARS-CoV-2 | Other Diseases | SARS-CoV-2 | Other Diseases | |||||||||||||||||||
| b | 99% CI [LL, UL] | p | b | 99% CI [LL, UL] | p | b | 99% CI [LL, UL] | p | b | 99% CI [LL, UL] | p | b | 99% CI [LL, UL] | p | b | 99% CI [LL, UL] | p | |||||||
| HA during | 0.14 | 0.10 | 0.19 | <0.001 | 0.06 | 0.03 | 0.09 | <0.001 | 0.002 | −0.05 | 0.05 | 0.94 | 0.03 | −0.01 | 0.06 | 0.08 | 0.15 | 0.11 | 0.20 | <0.001 | 0.05 | 0.01 | 0.09 | 0.002 |
| DI a | 0.003 | −0.03 | 0.04 | 0.81 | 0.02 | −0.004 | 0.05 | 0.04 | 0.07 | 0.02 | 0.12 | 0.001 | 0.03 | 0.002 | 0.07 | 0.01 | −0.01 | -0.05 | 0.04 | 0.65 | 0.01 | −0.02 | 0.05 | 0.30 |
| IU b | −0.01 | −0.04 | 0.01 | 0.28 | -0.01 | −0.03 | 0.005 | 0.07 | 0.004 | −0.03 | 0.04 | 0.79 | −0.01 | −0.03 | 0.01 | 0.41 | −0.004 | -0.03 | 0.02 | 0.69 | 0.001 | −0.02 | 0.03 | 0.88 |
| HA during x DI a | 0.001 | −0.004 | 0.01 | 0.72 | 0.001 | −0.004 | 0.005 | 0.66 | 0.001 | −0.01 | 0.01 | 0.70 | 0.001 | −0.004 | 0.01 | 0.51 | −0.002 | -0.01 | 0.003 | 0.43 | 0.002 | −0.004 | 0.01 | 0.51 |
| HA during x IU b | 0.001 | −0.003 | 0.004 | 0.65 | 0.001 | −0.002 | 0.003 | 0.63 | −0.001 | −0.005 | 0.003 | 0.63 | <0.001 | −0.003 | 0.003 | 0.96 | −0.001 | -0.005 | 0.002 | 0.30 | −0.001 | −0.004 | 0.003 | 0.61 |
| Behavior pre c | 0.47 | 0.37 | 0.57 | <0.001 | 0.77 | 0.70 | 0.85 | <0.001 | 0.50 | 0.42 | 0.59 | <0.001 | 0.87 | 0.81 | 0.93 | <0.001 | 0.36 | 0.28 | 0.45 | <0.001 | 0.70 | 0.62 | 0.79 | <0.001 |
| R2 | 0.42 | 0.70 | 0.34 | 0.76 | 0.25 | 0.47 | ||||||||||||||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sauer, K.S.; Jungmann, S.M.; Witthöft, M. Emotional and Behavioral Consequences of the COVID-19 Pandemic: The Role of Health Anxiety, Intolerance of Uncertainty, and Distress (In)Tolerance. Int. J. Environ. Res. Public Health 2020, 17, 7241. https://doi.org/10.3390/ijerph17197241
Sauer KS, Jungmann SM, Witthöft M. Emotional and Behavioral Consequences of the COVID-19 Pandemic: The Role of Health Anxiety, Intolerance of Uncertainty, and Distress (In)Tolerance. International Journal of Environmental Research and Public Health. 2020; 17(19):7241. https://doi.org/10.3390/ijerph17197241
Chicago/Turabian StyleSauer, Karoline S., Stefanie M. Jungmann, and Michael Witthöft. 2020. "Emotional and Behavioral Consequences of the COVID-19 Pandemic: The Role of Health Anxiety, Intolerance of Uncertainty, and Distress (In)Tolerance" International Journal of Environmental Research and Public Health 17, no. 19: 7241. https://doi.org/10.3390/ijerph17197241