Effectiveness of Respiratory Muscle Training for Pulmonary Function and Walking Ability in Patients with Stroke: A Systematic Review with Meta-Analysis

 ,
,  ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection
2.3. Data Extraction
2.4. Risk of Bias Assessment
2.5. Statistical Analysis
3. Results
3.1. Risk of Bias Assessment
3.2. Effect of Intervention: Pooled Estimates
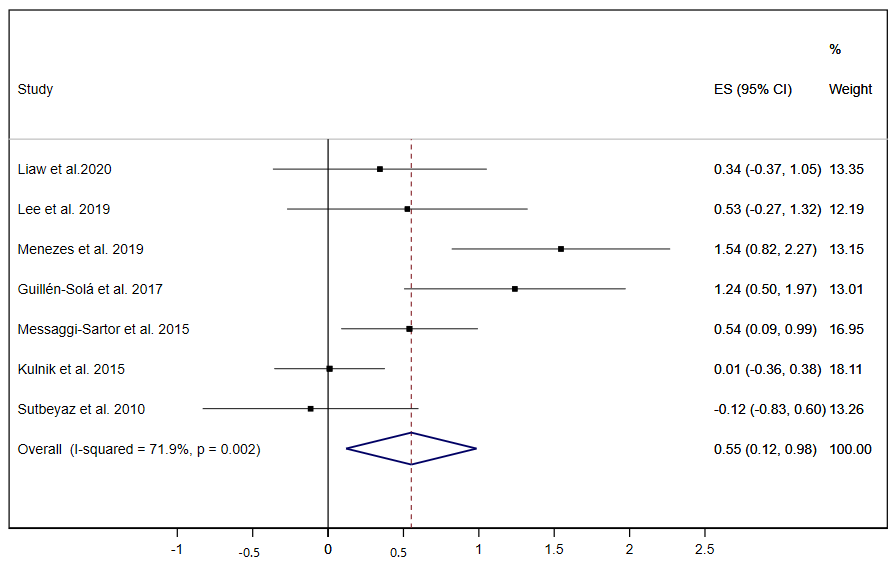
3.2.1. Pulmonary Function
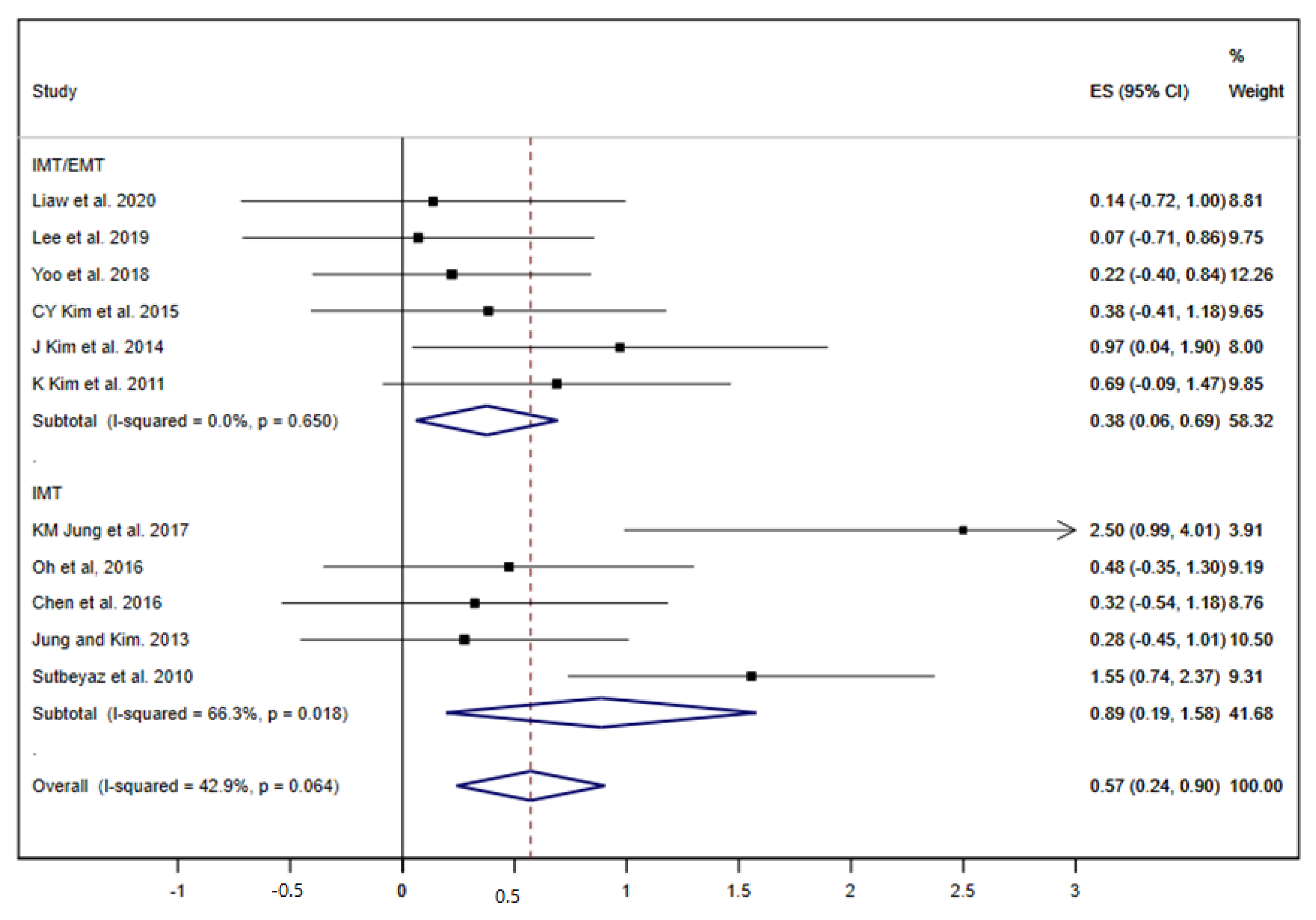
3.2.2. Functional Capacity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Hankey, G.J. Stroke. Lancet 2017, 389, 641–654. [Google Scholar] [CrossRef]
- Jandt, S.R.; Caballero, R.M.D.S.; Junior, L.A.F.; Dias, A.S. Correlation between trunk control, respiratory muscle strength and spirometry in patients with stroke: An observational study. Physiother. Res. Int. 2010, 16, 218–224. [Google Scholar] [CrossRef] [PubMed]
- Menezes, K.K.P.; Nascimento, L.R.; Ada, L.; Polese, J.C.; Avelino, P.R.; Teixeira-Salmela, L.F. Respiratory muscle training increases respiratory muscle strength and reduces respiratory complications after stroke: A systematic review. J. Physiother. 2016, 62, 138–144. [Google Scholar] [CrossRef] [Green Version]
- Polese, J.C.; Pinheiro, M.B.; Faria, C.D.C.M.; Britto, R.R.; Parreira, V.F.; Teixeira-Salmela, L.F. Strength of the respiratory and lower limb muscles and functional capacity in chronic stroke survivors with different physical activity levels. Braz. J. Phys. Ther. 2013, 17, 487–493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Battaglia, E.; Fulgenzi, A.; Ferrero, M.E. Rationale of the combined use of inspiratory and expiratory devices in improving maximal inspiratory pressure and maximal expiratory pressure of patients with chronic obstructive pulmonary disease. Arch. Phys. Med. Rehabil. 2009, 90, 913–918. [Google Scholar] [CrossRef] [PubMed]
- Forbes, S.; Game, A.; Syrotuik, D.; Jones, R.; Bell, G.J. The effect of inspiratory and expiratory respiratory muscle training in rowers. Res. Sports Med. 2011, 19, 217–230. [Google Scholar] [CrossRef] [PubMed]
- De Menezes, K.K.P.; Nascimento, L.R.; Avelino, P.R.; Alvarenga, M.T.M.; Teixeira-Salmela, L.F. Efficacy of interventions to improve respiratory function after stroke. Respir. Care 2018, 63, 920–933. [Google Scholar] [CrossRef]
- Gomes-Neto, M.; Saquetto, M.B.; Silva, C.M.; Carvalho, V.O.; Ribeiro, N.; Conceição, C.S. Effects of respiratory muscle training on respiratory function, respiratory muscle strength and exercise tolerance in post-stroke patients: A systematic review with meta-analysis. Arch. Phys. Med. Rehabil. 2016, 97, 1994–2001. [Google Scholar] [CrossRef]
- Xiao, Y.; Luo, M.; Wang, J.; Luo, H. Inspiratory muscle training for the recovery of function after stroke (Cochrane review). Cochrane Database Syst. Rev. 2012, 5. [Google Scholar] [CrossRef]
- Martín-Valero, R.; Almeida, M.D.L.C.; Casuso-Holgado, M.J.; Heredia-Madrazo, A. Systematic Review of Inspiratory Muscle Training after Cerebrovascular Accident. Respir. Care 2015, 60, 1652–1659. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- Higgins, J.P.; Thomas, S.J.; Page, M.J.; Elbers, R.G.; Sterne, J.A.C. Chapter 8: Assessing risk of bias in a randomized trial. In Cochrane Handbook for Systematic Reviews of Interventions Version 60 (Updated July 2019): Cochrane; Higgins, J.P., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- Olivo, S.A.; Macedo, L.; Gadotti, I.C.; Fuentes, J.; Stanton, T.R.; Magee, D.J. Scales to Assess the Quality of Randomized Controlled Trials: A Systematic Review. Phys. Ther. 2008, 88, 156–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M.R. Reliability of the PEDro Scale for Rating Quality of Randomized Controlled Trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, S.B. Estimating Effect Sizes From Pretest-Posttest-Control Group Designs. Organ. Res. Methods 2007, 11, 364–386. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Li, T.; Deeks, J.J. Chapter 6: Choosing effect measures and computing estimates of effect. In Cochrane Handbook for Systematic Reviews of Interventions Version 60 (Updated July 2019): Cochrane; Higgins, J.P., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- Liaw, M.Y.; Hsu, C.H.; Leong, C.P.; Liao, C.Y.; Wang, L.Y.; Lu, C.H.; Lin, M.C. Respiratory muscle training in stroke patients with respiratory muscle weakness, dysphagia, and dysarthria—A prospective randomized trial. Medicine (Baltimore) 2020, 99, e19337. [Google Scholar] [CrossRef]
- Lee, K.; Park, D.; Lee, G. Progressive Respiratory Muscle Training for Improving Trunk Stability in Chronic Stroke Survivors: A Pilot Randomized Controlled Trial. J. Stroke Cerebrovasc. Dis. 2019, 28, 1200–1211. [Google Scholar] [CrossRef]
- De Menezes, K.K.P.; Nascimento, L.R.; Ada, L.; Avelino, P.R.; Polese, J.C.; Alvarenga, M.T.M.; Barbosa, M.H.; Teixeira-Salmela, L.F. High-Intensity Respiratory Muscle Training Improves Strength and Dyspnea Poststroke: A Double-Blind Randomized Trial. Arch. Phys. Med. Rehabil. 2018, 100, 205–212. [Google Scholar] [CrossRef]
- Cho, J.E.; Lee, H.J.; Kim, M.K.; Lee, W.H. The improvement in respiratory function by inspiratory muscle training is due to structural muscle changes in patients with stroke: A randomized controlled pilot trial. Top. Stroke Rehabil. 2017, 25, 37–43. [Google Scholar] [CrossRef]
- Yoo, H.J.; Pyun, S.B. Efficacy of Bedside Respiratory Muscle Training in Patients with Stroke: A Randomized Controlled Trial. Am. J. Phys. Med. Rehabil. 2018, 97, 691–697. [Google Scholar] [CrossRef]
- Lee, H.J.; Kang, T.W.; Kim, B.R. Effects of diaphragm and deep abdominal muscle exercise on walking and balance ability in patients with hemiplegia due to stroke. J. Exerc. Rehabil. 2018, 14, 648–653. [Google Scholar] [CrossRef]
- Jung, K.M.; Bang, D.H. Effect of inspiratory muscle training on respiratory capacity and walking ability with subacute stroke patients: A randomized controlled pilot trial. J. Phys. Ther. Sci. 2017, 29, 336–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, N.J.; Na, S.S.; Kim, S.K.; Hwangbo, G. The effect of the inspiratory muscle training on functional ability in stroke patients. J. Phys. Ther. Sci. 2017, 29, 1954–1956. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oh, D.; Kim, G.; Lee, W.; Shin, M.M.S. Effects of inspiratory muscle training on balance ability and abdominal muscle thickness in chronic stroke patients. J. Phys. Ther. Sci. 2016, 28, 107–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guillen-Sola, A.; Sartor, M.M.; Soler, N.B.; Duarte, E.; Barrera, M.C.; Marco, E. Respiratory muscle strength training and neuromuscular electrical stimulation in subacute dysphagic stroke patients: A randomized controlled trial. Clin. Rehabil. 2016, 31, 761–771. [Google Scholar] [CrossRef]
- Chen, P.C.; Liaw, M.Y.; Wang, L.Y.; Tsai, Y.C.; Hsin, Y.J.; Chen, Y.C. Inspiratory muscle training in stroke patients with congestive heart failure A CONSORT-compliant prospective randomized single-blind controlled trial. Medicine 2016, 95, e4856. [Google Scholar] [CrossRef]
- Messaggi-Sartor, M.; Guillen-Sola, A.; Depolo, M.; Duarte, E.; Rodríguez, D.A.; Barrera, M.-C.; Barreiro, E.; Escalada, F.; Orozco-Levi, M.; Marco, E. Inspiratory and expiratory muscle training in subacute stroke: A randomized clinical trial. Neurology 2015, 85, 564–572. [Google Scholar] [CrossRef]
- Kulnik, S.T.; Birring, S.S.; Moxham, J.; Rafferty, G.F.; Kalra, L. Does Respiratory Muscle Training Improve Cough Flow in Acute Stroke? Pilot Randomized Controlled Trial. Stroke 2015, 46, 447–453. [Google Scholar] [CrossRef] [Green Version]
- Kim, C.Y.; Lee, J.S.; Kim, H.D.; Kim, I.S. Effects of the combination of respiratory muscle training and abdominal drawing-in maneuver on respiratory muscle activity in patients with post-stroke hemiplegia: A pilot randomized controlled trial. Top. Stroke Rehabil. 2015, 22, 262–270. [Google Scholar] [CrossRef]
- Yim, J.; Kim, J.; Park, J. Effects of Respiratory Muscle and Endurance Training Using an Individualized Training Device on the Pulmonary Function and Exercise Capacity in Stroke Patients. Med. Sci. Monit. 2014, 20, 2543–2549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, J.-H.; Kim, N.-S. Effects of Inspiratory Muscle Training on Diaphragm Thickness, Pulmonary Function, and Chest Expansion in Chronic Stroke Patients. J. Korean Soc. Phys. Med. 2013, 8, 59–69. [Google Scholar] [CrossRef] [Green Version]
- Britto, R.R.; Rezende, N.R.; Marinho, K.C.; Torres, J.L.; Parreira, V.F.; Teixeira-Salmela, L.F. Inspiratory Muscular Training in Chronic Stroke Survivors: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2011, 92, 184–190. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Fell, D.W.; Lee, J.H. Feedback Respiratory Training to Enhance Chest Expansion and Pulmonary Function in Chronic Stroke: A Double-Blind, Randomized Controlled Study. J. Phys. Ther. Sci. 2011, 23, 75–79. [Google Scholar] [CrossRef] [Green Version]
- Sutbeyaz, S.T.; Koseoglu, F.; Inan, L.; Coskun, O. Respiratory muscle training improves cardiopulmonary function and exercise tolerance in subjects with subacute stroke: A randomized controlled trial. Clin. Rehabil. 2010, 24, 240–250. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Sutton, A.J.; Ioannidis, J.P.A.; Terrin, N.; Jones, D.R.; Lau, J.; Carpenter, J.R.; Rücker, G.; Harbord, R.; Schmid, C.H.; et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ 2011, 343, d4002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lanini, B.; Gigliotti, F.; Coli, C.; Bianchi, R.; Pizzi, A.; Romagnoli, I.; Grazzini, M.; Stendardi, L.; Scano, G. Dissociation between respiratory effort and dyspnoea in a subset of patients with stroke. Clin. Sci. 2002, 103, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pollock, R.D.; Rafferty, G.F.; Moxham, J.; Kalra, L.; Rafferty, G.F. Respiratory Muscle Strength and Training in Stroke and Neurology: A Systematic Review. Int. J. Stroke 2012, 8, 124–130. [Google Scholar] [CrossRef]
- De Almeida, I.C.L.; Clementino, A.C.C.R.; Rocha, E.H.T.; Brandão, D.C.; De Andrade, A.D. Effects of hemiplegy on pulmonary function and diaphragmatic dome displacement. Respir. Physiol. Neurobiol. 2011, 178, 196–201. [Google Scholar] [CrossRef] [Green Version]
- Tomczak, C.R.; Jelani, A.; Haennel, R.G.; Haykowsky, M.; Welsh, R.; Manns, P. Cardiac Reserve and Pulmonary Gas Exchange Kinetics in Patients With Stroke. Stroke 2008, 39, 3102–3106. [Google Scholar] [CrossRef] [Green Version]
- Schünemann, H.J.; Vist, G.E.; Higgins, J.P.; Santesso, N.; Deeks, J.J.; Glasziou, P.; Akl, E.A.; Guyatt, G.H. Interpreting results and drawing conclusions. In Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Chichester, UK, 2019; pp. 403–431. [Google Scholar]
- Reyes, A.; Ziman, M.; Nosaka, K.; Nosaka, K. Respiratory Muscle Training for Respiratory Deficits in Neurodegenerative Disorders. Chest 2013, 143, 1386–1394. [Google Scholar] [CrossRef]
- Field, M.J.; Gebruers, N.; Shanmuga Sundaram, T.; Nicholson, S.; Mead, G. Physical Activity after Stroke: A Systematic Review and Meta-Analysis. ISRN Stroke 2013, 2013, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Michaelsen, S.M.; Ovando, A.C.; Romaguera, F.; Ada, L. Effect of Backward Walking Treadmill Training on Walking Capacity after Stroke: A Randomized Clinical Trial. Int. J. Stroke 2014, 9, 529–532. [Google Scholar] [CrossRef] [PubMed]
- Sulter, G.; Steen, C.; De Keyser, J. Use of the Barthel index and modified Rankin scale in acute stroke trials. Stroke 1999, 30, 1538–1541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blum, L.; Korner-Bitensky, N. Usefulness of the Berg Balance Scale in Stroke Rehabilitation: A Systematic Review. Phys. Ther. 2008, 88, 559–566. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Country | Participants/Mean Age | Inclusion/Exclusion Criteria | Intervention | Control | Study Outcomes |
|---|---|---|---|---|---|---|
| Liaw et al., 2020 [19] | Taiwan | n = 31 GI: 15 GC: 16 38.7% men 62.8 years | Inclusion: Aged 35 to 80 years with unilateral stroke > 6 months, respiratory muscle weakness, dysphagia, or dysarthria. Exclusion: Increased intracranial pressure, uncontrolled hypertension, decompensated heart failure, unstable angina, recent myocardial infarction, complicated arrhythmias, pneumothorax, bullae/blebs in the preceding 3 months, severe cognitive function or infection, recurrent stroke, brain stem stroke, and aphasia. | IMT load was 30%–60% of MIP (6 sets of 5 repetitions). EMT load was 15%–75% of MEP (5 sets of 5 breaths). Session: IMT and EMT, 1 to 2 times per day, 5 days a week for 6 weeks, 1 to 2 min between each set. Device: Dofin Breathing Trainer (DT 11 or DT 14). RHB program as CG. | RHB program: postural training, breathing control, improving cough technique, checking chest wall mobility, fatigue management, orofacial exercises, thermal tactile stimulation, Mendelsohn maneuvering, effort swallowing, or supra-glottic maneuver. | -FEV1 -MEP -MIP -MBI -Dyspnea -FVC |
| Lee et al., 2019 [20] | Seoul, Korea | n = 25 GI: 13 GC: 12 48% men 59.1 years | Inclusion: Stroke over 6 months, MMSE > 24, no facial palsy and receptive aphasia, and no prior thoracic or abdominal surgery. Exclusion: Medications for neuromuscular control or that provoke drowsiness, significant disability prior to stroke as evidenced by a score >3 on MRS, restrictive lung disease, TIS <10, and musculoskeletal problems in the pelvis or spine. | IMT/EMT at 30% of the resistance intensity on the first day of the week. Session: 10–15 times, 5 set for 20 min in a session and resting time of 30–60 s between each set. Trunk stabilization exercises: 40 min, 3 times a week for 6 weeks. Device: Threshold PEP; Threshold IMT-Respironics. RHB program as CG. | Conventional physical and occupational therapy conducted for 30 min, 2 times a day, and 6 times per week. Trunk stabilization exercises: 40 min, 3 times a week for 6 weeks. | -FEV1 -MEP -MIP -PEF |
| Menezes et al., 2019 [21] | Brazil | n = 38 GI: 19 GC: 19 50% men 63.5 years | Inclusion: Adults > 20 years, stroke > 3 months and < 5 years, MIP < 80 cm H2O or MEP < 90 cm H2O (respiratory muscle weakness), and not undertook any respiratory training. Exclusion: Patients with cognitive deficits, facial palsy, and/or any conditions. | Home based IMT/EMT. Session: 40 min/day (two 20 min sessions), 7 times/ week, over 8 weeks. Each 20-min session: 4 min sets of training, followed by 1 min rest. Load: 50% MIP/MEP Device: Orygen-dual valve. | Sham respiratory training without any resistance and progression. | -MIP -MEP -Dyspnea -6-MWT |
| Cho et al., 2018 [22] | Korea | n = 25 GI: 12 GC: 13 52% men 49.5 years | Inclusion: Adults > 20 years, stroke > 3 months, MIP < 70% of those predicted when adjusted for age and sex, had and were able to give informed consent and follow study procedures. Exclusion: Patients with facial palsy, myocardial infarction or acute heart failure within 3 months, pulmonary disease, neurological conditions or medications that interfere with neuromuscular control. | Hospital IMT. Session: 3 sets of 30 breaths, with a 1-min rest in between the sets. 5 days a week, for 6 weeks. Load: 30% MIP readjusted weekly. Device: PowerBreath K5. RHB program as CG. | RHB program: muscle strengthening exercises, Bobath therapy, gait training, and stair climbing training for 60 min/day, 5 days per week, for 6 weeks. | -MIP -Fatigue -6-MWT |
| Yoo et al., 2018 [23] | Seoul, Korea | n = 40 GI: 20 GC: 20 65% men 61 years | Inclusion: Adults >18 years; first episode of stroke within 3 months; moderate to severe stroke impairment; understand instructions and follow the study program. Exclusion: Persistent cardiopulmonary disease, coexisting brain disorders, uncontrolled hypertension, severe facial palsy or other oropharyngeal structural abnormality, severe oral apraxia, and tracheostomy. | Bedside IMT/EMT. Session: 10 min of breath stacking exercise + 10 min IMT + 10 min EMT; with a 5-min interval before each exercise. Twice/day for 7 days/week for a 3-wk period. Device: A flow-oriented incentive spirometer (Hyupsung) for IMT; Acapella vibratory PEP for EMT. RHB program as CG. | Conventional stroke RHB program: motion exercises, muscle strengthening, gait training, fine motor exercises, and activity of daily living training. It was performed for 30 min, twice a day 5 days a week, for 3 weeks. | -FVC -FEV1 -PEF -MBI -BBS |
| Lee et al., 2018 [24] | Jeonju, Korea | n = 20 GI: 10 GC: 10 50% men 60 years | Inclusion: Patients with hemiplegia due to stroke, 50–70 years, diagnosed 1–2 year previously, could perform 10-m walking independently and walk within 5–60 sec, ability to understand and follow the indication of the researcher. Exclusion: NA | Load of IMT: 50% of MIP increasing repetitions each week. Session: 20 min of IMT and 20 min of bracing exercise for 6 weeks and 5 days per week. Bracing exercise holding the pressometer at 40 mmHg. Device: POWERbreath for IMT. RHB program as CG. | Traditional exercise to enhance trunk control ability and included a stretching exercise for trunk flexibility, for 6 weeks, 5 days per week, once for 40 min. | -6-MWT -BBS |
| KM Jung, 2017 [25] | Korea | n = 12 GI: 6 GC: 6 41.6% men 61.7 years | Inclusion: Hemiparesis due to stroke, event occurring <6 months previously, ability to use a cycle ergometer, no restriction in lung function and no neurologic, orthopedic, or unstable cardiac condition, and ability to walk 100 m. Exclusion: Comorbidities or disabilities that would preclude study, and any uncontrolled health condition for which exercise is contraindicated. | Session: IMT 6 sets of 5 min each for 30 min a day, 5 times a week, for 4 weeks. Load: IMT at 30% MIP. Device: Threshold IMT. Moreover, traditional physical therapy and occupational therapy. | A self-selective intensity exercise with an ergonomic cycle for 30 min a day, five times a week, for four weeks. | -FVC -FEV1 -6-MWT |
| NJ Jung, 2017 [26] | Daegu, Korea | n = 20 GI: 10 GC: 10 NA | Inclusion: Stroke 6 months or longer; had no visual field defect and auditory sense; Scored at least 24 on the K-MMSE; independent sitting and gait; had no pulmonary embolus; no orthopedic problem, or unstable cardiac condition; had not undergone chest or abdominal surgery. Exclusion: NA | Session: 2 sets of 10 times IMT, taking a break of 10 s between each set. 5 times a week, for 6 weeks. Load of IMT: 80% of MIP Device: Respifit-S. Neuro Developmental Treatment as CG. | Neuro developmental treatment physical therapy for 30 min per time, 3 times a week, for 6 weeks. | -6-MWT |
| Guillen-Sola et al., 2017 [28] | Spain | n = 50 GI1: 16 GI2: 16 GC: 18 51.3% men 69.0 years | Inclusion: Subacute ischemic stroke within 1 to 3 weeks of inclusion and dysphagia. Exclusion: History of previous neurological diseases and/or cognitive impairment | Session: IMT/EMT, 5 sets of 10 breaths followed by 1 min of unloaded recovery breathing off the device. Twice a day, 5 days per week for 3 weeks, with the assistance of a therapist. Load: 30% of MIP/MEP and increased weekly at intervals of 10 cm H2O. Device: Orygen dual valve. RHB program as CG. | RHB program: Physical, occupational and speech therapy targeting specific impairments in mobility, activities of daily living, swallowing and communication skills. | -MIP -MEP |
| Oh et al., 2016 [27] | Korea | n = 23 GI: 11 GC: 12 56.5% men 70.6 years | Inclusion: Unilateral stroke occurred 6 months prior to the study the ability to perform breathing training for 30 min or longer; no sight impairment; modified Ashworth scale (MAS) score for upper and low extremities < 2; and MMSE-K score > 24. Exclusion: NA | Session: 15 times per set, 10 sets. Warm-up and cool-down exercises twice in each set, with a rest time of 60 s. 20 min per day, 3 times per week for 6 weeks. Load: IMT resistance 30% MIP. Device: n/A. RHB program as CG. | RHB program: 20-min session, 3 times/week, for 6 weeks. General breathing exercises, abdominal strengthening exercises, and general physical therapy. | -FVC -FEV1 -PEF -BBS |
| Chen et al., 2016 [29] | Taiwan | n = 21 GI: 11 GC: 10 38.1% men 65.5 years | Inclusion: Adults 20–85 years with congestive heart failure and stroke. Exclusion: MIP ≥70% predicted MIP, could not tightly place the lips over a mouthpiece, recent acute exacerbation of COPD, pneumothorax or large bullae on chest radiography, long-term use of oxygen therapy, recent lung surgery marked osteoporosis, unstable angina, decompensated CHF, or arrhythmia. | Session: IMT with a load of 30% of MIP (adjusted by 2 cm H2O/week), for 30 min, 5 times/week, for 10 weeks. Device: Respironics. RHB program as CG. | Conventional stroke RHB program, 5 days/week for 10 weeks. | -FVC -FEV1 -Dyspnea -MBI |
| Messaggi-Sartor et al., 2015 [30] | Spain | n = 77 GI: 39 GC: 38 57.8% men 66.5 years | Inclusion: Adults, first-ever ischemic stroke, time since stroke < 3 weeks, hemiparesis in upper or lower limb, and gave informed consent and followed study procedures. Exclusion: Cardiopulmonary disease, neurologic condition other than stroke, significant alcohol abuse, medical treatment with potential effect on muscle structure and function. | IMT/EMT with workload of 30% MIP/MEP. Session: 5 sets of 10 repetitions followed by 1–2 min of unloaded recovery, twice a day, 5 days per week, for 3 weeks. 15–20 breaths/min Device: Orygen-Dual valve. | RHB program: physical, occupational, and speech therapy sessions (3 h per day, 5 days a week, for 3 weeks). Sham IEMT without load and progression. | -MIP -MEP |
| Kulnik et al., 2015 [31] | United Kingdom | n = 82 GI1: 27 GI2:26 GC:25 57.3% men 64.4 years | Inclusion: Adults, < 2 weeks of stroke, 5–25 score in NIHSS, ability to give informed consent and follow study procedures. Exclusion: Blood pressure > 180/100 mmHg, angina, myocardial infarction, or acute heart failure within 3 months, pulmonary disease; and neurological conditions other than stroke. | EMT (GI1) and IMT (GI2) Session: 5 sets of 10 breaths each, with 1-min rests between sets. Load was 50% of MIP or MEP. These pressures were reassessed, and resistance readjusted weekly. Device: Respironics | Sham training: without load and progression. | -MIP -MEP |
| CY Kim et al., 2015 [32] | Germany | n = 37 GI1: 15 GI2: 13 GC: 12 45.94% men 59.1 years | Inclusion: Ischemic or hemorrhagic post-stroke hemiparesis; K-MMSE ≥ 26. Exclusion: Previous musculoskeletal abnormalities, confusion, neurological disorders, significant perceptual, cognitive, or communication impairments, COPD, and asthma. | Session: IMT/EMT 5 sets (10 repetitions/set), 1-min of rest after each set. 30 supervised sessions (5 × 15 min/week, 6 weeks). Device: Tri-ball Incentive Spirometer. RHB program as CG. | RHB program: stretching exercises of the limbs, therapist-guided techniques for facilitating the normal movement pattern. 1 h, 5 times a week. | -FEV1 -FVC |
| J Kim et al., 2014 [33] | Korea | n = 20 GI: 10 GC: 10 54 years | Inclusion: Hemiparesis due to stroke in previous 6 months, capable of comprehending commands and walking for at least 6 min with/without assistive device, had no previous cardiovascular or respiratory problems, no medications that would influence the metabolic or cardiorespiratory responses to exercise, no previous exercise training ventilator muscles and no bone deformities of the chest or spine. Exclusion: NA | Session: IMT/EMT during 20 min. Individually loaded and set to the breathing capacity of each patient. Device: Respifit-S. | Conventional exercise treatments for 30 min (including joint mobility, eccentric contraction, muscle strengthening, and walking exercise) followed by a 10-min rest. Full body workout machine for 20 min. 3 times/week, for 4 weeks. | -FEV1 -PEF -6-MWT -Dyspnea |
| Jung and Kim, 2013 [34] | Korea | n = 29 GI: 15 GC: 14 58.6% men 59 years | Inclusion: Hemiplegia secondary to stroke > 6 months and were undergoing general physical therapy. Exclusion: Innate thorax deformity, rib fracture, or had a disease related to lungs, kidneys, the endocrine system, orthopedics, or rheumatology. | Session: IMT with a load of 30% of MIP (adjusted gradually). 20 min, 3 times/week, for 6 weeks. Device: Respironics | Nothing | -FVC -FEV1 -PEF |
| Britto et al., 2011 [35] | Brazil | n = 21 GI: 9 GC: 9 52% men 54 years | Inclusion: Adults > 20 years; hemiparesis due to stroke, MIP < 90%; no facial palsy, able to use a cycle ergometer, had no restrictions in lung function and no neurologic, orthopedic, or unstable cardiac conditions, nonsmokers, showed no receptive aphasia, and had not undergone thoracic or abdominal surgery. Exclusion: Patients unable to perform the tests and used medications that could interfere with neuromuscular control or cause drowsiness. | Session: IMT 30 min, 5 times/week, for 8 weeks. Each session was divided into 6 series of 5 min each, with a 1-min rest interval between series. IMT with a load of 30% of MIP (adjusted every 2 weeks, according the new MIP value). Device: Threshold IMT. | Sham respiratory training. | -MIP |
| K Kim et al., 2011 [36] | Korea, Daegu | n = 27 GI: 13 GC: 14 37% men 57 years | Inclusion: Stroke occurred greater than 6 months ago. Exclusion: Pulmonary disorders, severe aphasia, and impairment of cognitive function. | Session: IMT/EMT, 30 min, 3 times/week, for 4 weeks. Load: 50–60% of VC and low frequency (12–13 breaths/ minute). Device: SpiroTiger. RHB program as CG. | Conventional stroke physical therapy program (30 min, 3 times/week, for 4 weeks). | -FVC -FEV1 -PEF |
| Sutbeyaz et al., 2010 [37] | Turkey | n = 45 GI1: 15 GI2: 15 GC: 15 53.3% men 61.8 years | Inclusion: Unilateral stroke with hemiparesis in previous 12 months, enough unilateral upper torso and extremity nerve function and strength to accomplish arm crank ergometry, ability to understand and follow simple verbal instructions, no previous history of cardiovascular or respiratory problems, no medication that would influence metabolic or cardiorespiratory responses to exercise. Exclusion: Chronic pulmonary and/or cardiac disease, clinical signs of cardiac and/or respiratory disease, impaired level of consciousness and evidence of gross cognitive impairment. | Session: 2 sets/day of 15 min each, six times a week, for 6 weeks. Load of IMT starting at a load of 40% MIP. It was gradually increased, 5–10% each session, to 60% of MIP as tolerated. Device: Threshold IMT. RHB program as CG. | Conventional stroke rehabilitation program, 5 days a week for 6 weeks. | -FVC -FEV1 -PEF -MIP -MEP -Dyspnea |
| Study | Random Allocation | Concealed Allocation | Baseline Similarity | Subject Blinding | Therapist Blinding | Assessor Blinding | <15% Dropouts | Intention to-Treat Analysis | Between-Group Difference Reported | Point Estimate, Variability Reported | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Liaw et al., 2020 [19] | Y | Y | Y | N | Y | N | N | Y | Y | Y | 7 |
| Lee et al., 2019 [20] | Y | Y | Y | N | N | Y | N | N | Y | Y | 6 |
| Menezes et al., 2019 [21] | Y | Y | Y | Y | N | N | Y | Y | Y | Y | 8 |
| Cho et al., 2018 [22] | Y | Y | Y | N | N | Y | N | N | Y | Y | 6 |
| Yoo et al., 2018 [23] | Y | N | Y | N | N | N | Y | N | Y | Y | 5 |
| Lee et al., 2018 [24] | Y | N | Y | N | N | N | N | N | Y | Y | 4 |
| KM Jung et al., 2017 [25] | Y | Y | Y | N | N | N | Y | N | Y | Y | 6 |
| NJ Jung et al., 2017 [26] | Y | N | N | N | N | N | N | N | Y | Y | 3 |
| Guillen-Sola et al., 2017 [28] | Y | N | Y | N | N | Y | N | Y | Y | Y | 6 |
| Oh et al., 2016 [27] | Y | N | Y | N | N | N | Y | N | Y | Y | 5 |
| Chen et al., 2016 [29] | Y | N | Y | N | N | Y | N | N | Y | Y | 5 |
| Messagi-Sartor et al., 2015 [30] | Y | Y | Y | Y | N | Y | N | Y | Y | Y | 8 |
| Kulnik et al., 2015 [31] | Y | Y | Y | N | N | Y | N | Y | Y | Y | 7 |
| CY Kim et al., 2015 [32] | Y | N | Y | N | N | Y | N | N | Y | Y | 5 |
| J Kim et al., 2014 [33] | Y | N | Y | N | N | N | N | N | Y | Y | 4 |
| Jung and Kim 2013 [34] | Y | N | Y | N | N | N | N | N | Y | Y | 4 |
| Britto et al., 2011 [35] | Y | Y | Y | N | N | Y | Y | N | Y | Y | 7 |
| K Kim et al., 2011 [36] | Y | N | Y | Y | N | Y | N | N | Y | Y | 6 |
| Sutbeyaz et al., 2010 [37] | Y | Y | Y | N | N | Y | Y | N | Y | Y | 7 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pozuelo-Carrascosa, D.P.; Carmona-Torres, J.M.; Laredo-Aguilera, J.A.; Latorre-Román, P.Á.; Párraga-Montilla, J.A.; Cobo-Cuenca, A.I. Effectiveness of Respiratory Muscle Training for Pulmonary Function and Walking Ability in Patients with Stroke: A Systematic Review with Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 5356. https://doi.org/10.3390/ijerph17155356
Pozuelo-Carrascosa DP, Carmona-Torres JM, Laredo-Aguilera JA, Latorre-Román PÁ, Párraga-Montilla JA, Cobo-Cuenca AI. Effectiveness of Respiratory Muscle Training for Pulmonary Function and Walking Ability in Patients with Stroke: A Systematic Review with Meta-Analysis. International Journal of Environmental Research and Public Health. 2020; 17(15):5356. https://doi.org/10.3390/ijerph17155356
Chicago/Turabian StylePozuelo-Carrascosa, Diana P., Juan Manuel Carmona-Torres, José Alberto Laredo-Aguilera, Pedro Ángel Latorre-Román, Juan Antonio Párraga-Montilla, and Ana Isabel Cobo-Cuenca. 2020. "Effectiveness of Respiratory Muscle Training for Pulmonary Function and Walking Ability in Patients with Stroke: A Systematic Review with Meta-Analysis" International Journal of Environmental Research and Public Health 17, no. 15: 5356. https://doi.org/10.3390/ijerph17155356