Self-Perception of Dependence as an Indicator of Smartphone Addiction—Establishment of a Cutoff Point in the SPAI–Spain Inventory

 , , ,
, , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Data Collection Instrument
2.3. Data Analysis
3. Results
3.1. Characteristics of the Studied Population
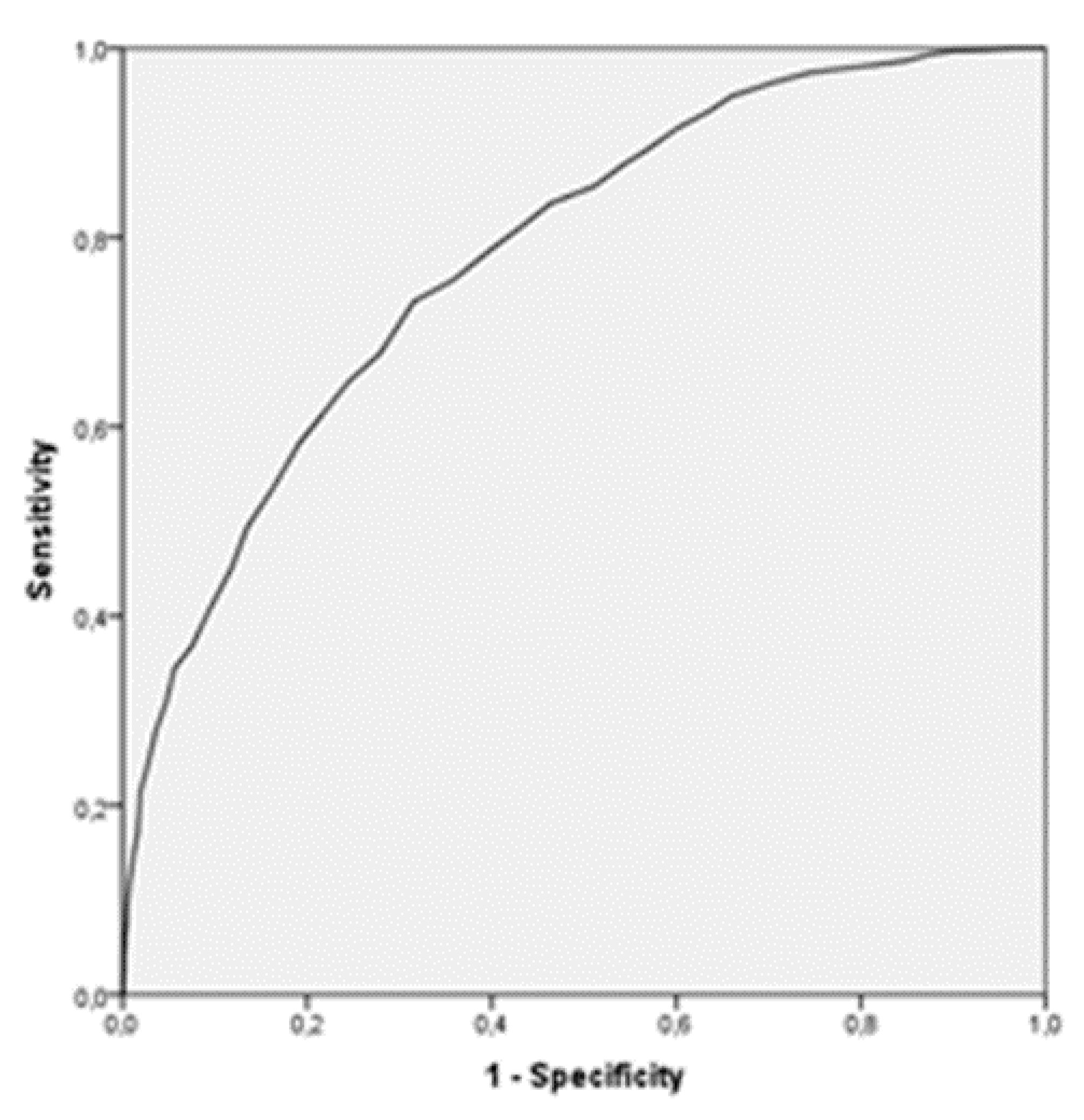
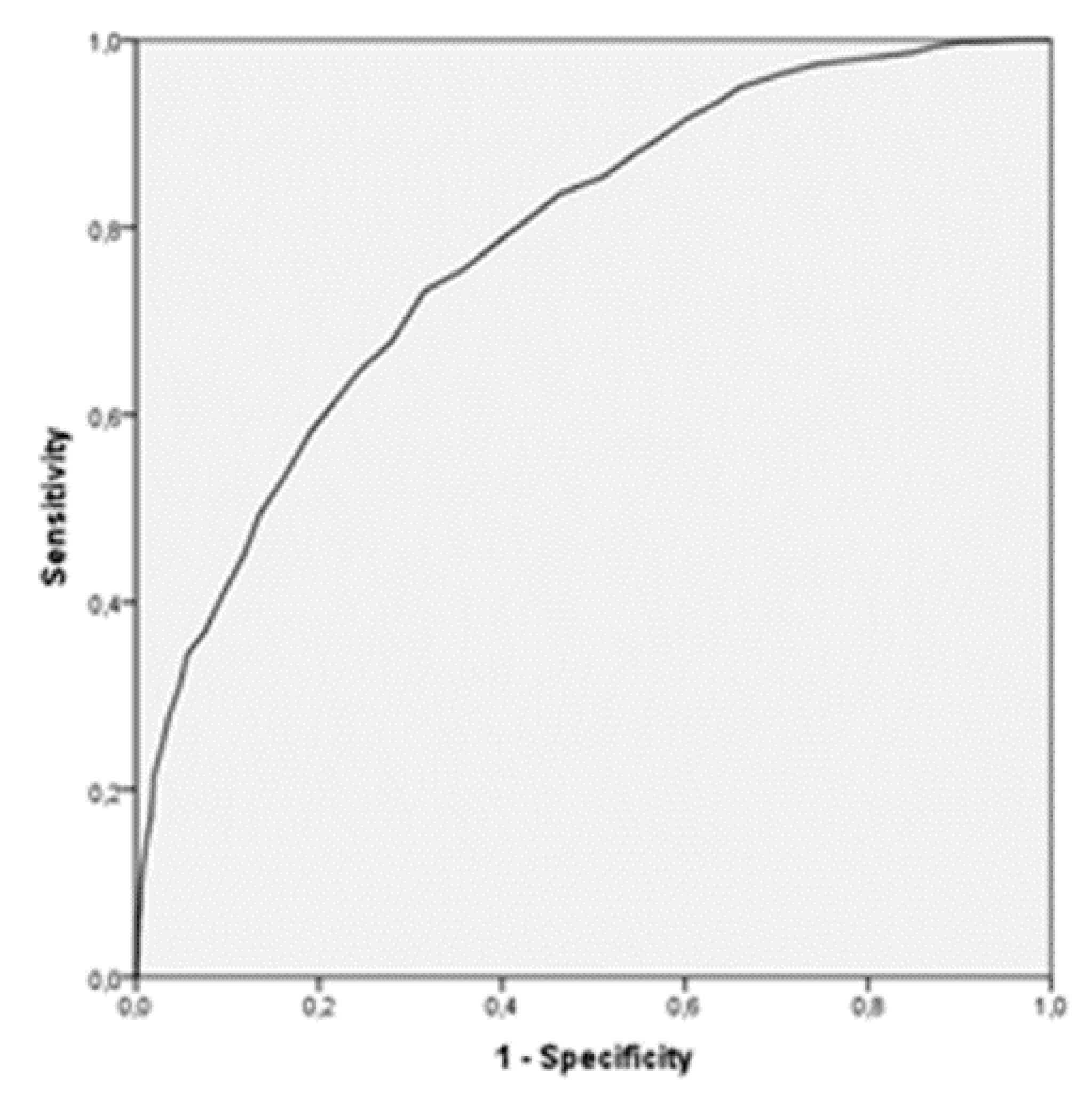
3.2. ROC Analysis Results
3.3. SPAI–Spain Cutoff Score Determination
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Chóliz, M. Historia De Una Adicción: Del Vicio Al Trastorno Del Juego. Cuadernos de medicina psicosomática y psiquiatría de enlace. Rev. Iberoam. Psicosom. 2014, 111, 84–88. [Google Scholar]
- Muñoz-Rivas, M.; Shih, P.C. Abuso de dispositivos móviles. In Abuso De Internet: Antesala Para La Adicción Al Juego De Azar Online; Echeburúa, E., Ed.; Pirámide: Madrid, Spain, 2016. [Google Scholar]
- Harris, B.; Regan, T.; Schueler, J.; Fields, S.A. Problematic Mobile Phone and Smartphone use Scales: A Systematic Review. Front. Psychol. 2020, 11, 672. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, M. Gambling on the Internet: A Brief Note. J. Gambl. Stud. 1996, 12, 471–473. [Google Scholar] [CrossRef] [PubMed]
- Echeburúa, E. Adicciones Sin Drogas? Las Nuevas Adicciones: Juego, Sexo, Comida, Compras, Trabajo, Internet, 2nd ed.; Editorial Desclée de Brouwer: Bilbao, Spain, 2009. [Google Scholar]
- Flores Robaina, N.; Jenaro Río, C.; González Gil, F.; Martín, E.; Poy, R. Adicción Al Móvil En Alumnos De Secundaria: Efectos En La Convivencia. Eur. J. Investig. Health Psychol. Educ. 2013, 3, 215–225. [Google Scholar] [CrossRef]
- Liese, B.S.; Benau, E.M.; Atchley, P.; Reed, D.; Becirevic, A.; Kaplan, B. The Self-Perception of Text-Message Dependency Scale (STDS): Psychometric Update Based on a United States Sample. Am. J. Drug Alcohol Abus. 2018, 45, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Fernandez, O.; Kuss, D.J.; Pontes, H.M.; Griffiths, M.D.; Dawes, C.; Justice, L.V.; Männikkö, N.; Kääriäinen, M.; Rumpf, H.; Bischof, A.; et al. Measurement Invariance of the Short Version of the Problematic Mobile Phone use Questionnaire (PMPUQ-SV) Across Eight Languages. Int. J. Environ. Res. Public Health 2018, 15, 1213. [Google Scholar] [CrossRef] [Green Version]
- Sasmaz, T.; Oner, S.; Kurt, A.Ö.; Yapici, G.; Yazici, A.E.; Bugdayci, R.; Sis, M. Prevalence and Risk Factors of Internet Addiction in High School Students. Eur. J. Public Health 2014, 24, 15–20. [Google Scholar] [CrossRef] [Green Version]
- Sohn, S.; Rees, P.; Wildridge, B.; Kalk, N.J.; Carter, B. Prevalence of Problematic Smartphone Usage and Associated Mental Health Outcomes Amongst Children and Young People: A Systematic Review, Meta-Analysis and GRADE of the Evidence. Bmc Psychiatry 2019, 19, 356. [Google Scholar]
- Cimino, S.; Cerniglia, L. A Longitudinal Study for the Empirical Validation of an Etiopathogenetic Model of Internet Addiction in Adolescence Based on Early Emotion Regulation. Biomed Res. Int. 2018, 2018, 4038541–4038548. [Google Scholar] [CrossRef]
- Nakayama, H.; Ueno, F.; Mihara, S.; Kitayuguchi, T.; Higuchi, S. Relationship between Problematic Internet use and Age at Initial Weekly Internet Use. J. Behave. Addict. 2020, 9, 129–139. [Google Scholar] [CrossRef] [Green Version]
- Chóliz Montañés, M.; Villanueva Silvestre, V. Evaluación De La Adicción Al Móvil En La Adolescencia. Rev. Esp. Drogodep; Departamento de Psicología Básica. Universidad de Valencia: Valencia, Spain, 2011; pp. 165–183. [Google Scholar]
- Lu, X.; Watanabe, J.; Liu, Q.; Uji, M.; Shono, M.; Kitamura, T. Internet and Mobile Phone Text-Messaging Dependency: Factor Structure and Correlation with Dysphoric Mood among Japanese Adults. Comput. Hum. Behav. 2011, 27, 1702–1709. [Google Scholar] [CrossRef]
- Chóliz, M.; Pinto, L.; Phansalkar, S.; Corr, E.; Mujjahid, A.; Flores, C.; Barrientos, P. Development of a Brief Multicultural Version of the Test of Mobile Phone Dependence (TMDbrief) Questionnaire. Front. Psychol. 2016, 7, 650. [Google Scholar]
- Körmendi, A.; Brutöczki, Z.; Petra Végh, B.; Székely, R. Smartphone use can be Addictive? A Case Report. J. Behav. Addict. 2016, 5, 548–552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwon, M.; Lee, J.; Won, W.; Park, J.; Min, J.; Hahn, C.; Gu, X.; Choi, J.; Kim, D. Development and Validation of a Smartphone Addiction Scale (SAS). PLoS ONE 2013, 8, e56936. [Google Scholar] [CrossRef] [PubMed]
- Long, J.; Liu, T.; Liao, Y.; Qi, C.; He, H.; Chen, S.; Billieux, J. Prevalence and Correlates of Problematic Smartphone use in a Large Random Sample of Chinese Undergraduates. BMC Psychiatry 2016, 16, 408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De-Sola Gutiérrez, J.; Rodríguez de Fonseca, F.; Rubio, G. Cell-Phone Addiction: A Review. Front. Psychiatry 2016, 7, 175. [Google Scholar] [CrossRef] [Green Version]
- Lin, J.C. Popularity, Funding for Health-Effect Research and Cell-Phone Addiction. Ap-M 2010, 52, 164–166. [Google Scholar] [CrossRef]
- Ivanova, A.; Gorbaniuk, O.; Błachnio, A.; Przepiórka, A.; Mraka, N.; Polishchuk, V.; Gorbaniuk, J. Mobile Phone Addiction, Phubbing, and Depression among Men and Women: A Moderated Mediation Analysis. Psychiatr. Q. 2020. [Google Scholar] [CrossRef] [Green Version]
- Fischer-Grote, L.; Kothgassner, O.D.; Felnhofer, A. Risk Factors for Problematic Smartphone use in Children and Adolescents: A review of Existing Literature. Neuropsychiatr. Klin. Diagn. Ther. Rehabil. Organ Ges. Osterr. Nervenarzte Psychiater 2019, 33, 179–190. [Google Scholar] [CrossRef] [Green Version]
- Billieux, J. Problematic use of the Mobile Phone: A Literature Review and a Pathways Model. Curr. Psychiatry Rev. 2012, 15, 142. [Google Scholar] [CrossRef] [Green Version]
- Simó Sanz, C.; Martinez Sabater, A.; Ballestar Tarín, M.; Domínguez Romero, A. Instrumentos De Evaluación Del Uso Problemático Del Teléfono Móvil/Smartphone. Health Addict. Salud Y Drog. 2017, 17, 5. [Google Scholar] [CrossRef] [Green Version]
- Billieux, J.; Maurage, P.; Lopez-Fernandez, O.; Kuss, D.; Griffiths, M. Can Disordered Mobile Phone use be Considered a Behavioral Addiction? an Update on Current Evidence and a Comprehensive Model for Future Research. Curr. Addict. Rep. 2015, 2, 156–162. [Google Scholar] [CrossRef] [Green Version]
- Lin, Y.; Chiang, C.; Lin, P.; Chang, L.; Ko, C.; Lee, Y.; Lin, S. Proposed Diagnostic Criteria for Smartphone Addiction. PLoS ONE 2016, 11, e0163010. [Google Scholar] [CrossRef] [Green Version]
- Becerra Álvarez, D.R.; Delgado Martínez, A.C.; Villamizar Acevedo, G.A. Autopercepción De Estudiantes De Psicología Sobre Sus Competencias En Los Campos Laboral, Educativo Y Salud. Rexe Rev. Estud. Exp. Educ. 2014, 13, 151–167. [Google Scholar]
- Escamilla Cruz, S.; Campos Castolo, M.; Córdoba Ávila, M.Á. Autopercepción De Competencias Profesionales De Alumnos De La Licenciatura En Enfermería. Rev. Conamed 2012, 17, 67–75. [Google Scholar]
- Kirkcaldy, B.D.; Shephard, R.J.; Siefen, R.G. The Relationship between Physical Activity and Self-Image and Problem Behaviour among Adolescents. Soc. Psychiatry Psychiatr. Epidemiol. 2002, 37, 544–550. [Google Scholar] [CrossRef]
- Lockertsen, Ø.; Procter, N.; Vatnar, S.K.B.; Færden, A.; Eriksen, B.M.S.; Roaldset, J.O.; Varvin, S. Screening for Risk of Violence using Service Users’ Self-perceptions: A Prospective Study from an Acute Mental Health Unit. Int. J. Ment. Health Nurs. 2018, 27, 1055–1065. [Google Scholar] [CrossRef]
- Domenico, L.H.; Strobbe, S.; Stein, K.F.; Giordani, B.J.; Hagerty, B.M.; Pressler, S.J. Identifying the Structure and Effect of Drinking-Related Self-Schemas. West. J. Nurs. Res. 2017, 39, 942–981. [Google Scholar] [CrossRef] [Green Version]
- Grubbs, J.B.; Wilt, J.A.; Exline, J.J.; Pargament, K.I.; Kraus, S.W. Moral Disapproval and Perceived Addiction to Internet Pornography: A Longitudinal Examination. Addiction 2018, 113, 496–506. [Google Scholar] [CrossRef]
- Suurvali, H.; Hodgins, D.; Toneatto, T.; Cunningham, J. Motivators for Seeking Gambling-Related Treatment among Ontario Problem Gamblers. J. Gambl. Stud. 2012, 28, 273–296. [Google Scholar] [CrossRef]
- Agrawal, A.; Dick, D.M.; Bucholz, K.K.; Madden, P.A.F.; Cooper, M.L.; Sher, K.J.; Heath, A.C. Drinking Expectancies and Motives: A Genetic Study of Young Adult Women. Addiction 2008, 103, 194–204. [Google Scholar] [CrossRef] [PubMed]
- Zins, M.; Carle, F.; Bugel, I.; Leclerc, A.; Orio, F.D.; Goldberg, M. Predictors of Change in Alcohol Consumption among Frenchmen of the GAZEL Study Cohort. Addiction 1999, 94, 385–395. [Google Scholar] [CrossRef] [PubMed]
- Fleury, M.; Ngui, A.N.; Bamvita, J.; Grenier, G.; Caron, J. Predictors of Healthcare Service Utilization for Mental Health Reasons. Int. J. Environ. Res. Public Health 2014, 11, 10559–10586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Acosta, L.D.; Carrizo, E.D.; Pelaez, E. Factores Asociados a La Autopercepción De Salud En Adultos Mayores. Rev. Cuba. Salud Pública 2015, 41, 638–648. [Google Scholar]
- Simó-Sanz, C.; Ballestar-Tarín, M.L.; Martínez-Sabater, A. Smartphone Addiction Inventory (SPAI): Translation, Adaptation and Validation of the Tool in Spanish Adult Population. PLoS ONE 2018, 13, e0205389. [Google Scholar] [CrossRef] [Green Version]
- Arpaci, I.; Esgi, N. Psychometric Properties of the Turkish Version of the Smartphone Addiction Inventory (SPAI). Curr. Psychol. 2018, 1–6. [Google Scholar] [CrossRef]
- Lin, Y.; Chang, L.; Lee, Y.; Tseng, H.; Kuo, T.B.J.; Chen, S. Development and Validation of the Smartphone Addiction Inventory (SPAI). PLoS ONE 2014, 9, e98312. [Google Scholar] [CrossRef] [Green Version]
- Machado Khoury, J.; Corrêa de Freitas, A.A.; Valente Roque, M.A.; Rodrigues Albuquerque, M.; Maila de Castro, L.N.; Duarte Garcia, F. Assessment of the Accuracy of a New Tool for the Screening of Smartphone Addiction. PloS ONE 2017, 12, e0176924. [Google Scholar] [CrossRef]
- Pavia, L.; Cavani, P.; Di Blasi, M.; Giordano, C. Smartphone Addiction Inventory (SPAI): Psychometric Properties and Confirmatory Factor Analysis. Comput. Hum. Behav. 2016, 63, 170–178. [Google Scholar] [CrossRef]
- Streiner, D.L.; Cairney, J. What’s Under the ROC? an Introduction to Receiver Operating Characteristics Curves. Can. J. Psychiatry 2007, 52, 121–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perkins, N.J.; Schisterman, E.F. The Inconsistency of “Optimal” Cutpoints obtained using Two Criteria Based on the Receiver Operating Characteristic Curve. Am. J. Epidemiol. 2006, 163, 670–675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopez-Fernandez, O.; Kuss, D.J.; Romo, L.; Morvan, Y.; Kern, L.; Graziani, P.; Rousseau, A.; Rumpf, H.; Bischof, A.; GÄSSLER, A.; et al. Self-Reported Dependence on Mobile Phones in Young Adults: A European Cross-Cultural Empirical Survey. J. Behav. Addict. 2017, 6, 168–177. [Google Scholar] [CrossRef] [PubMed]
- Cerda, J.; Cifuentes, L. Using ROC Curves in Clinical Investigation: Theoretical and Practical Issues. Rev. Chil. Infectol. Organo Of. Soc. Chil. Infectol. 2012, 29, 138–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nanishi, K.; Green, J.; Taguri, M.; Jimba, M. Determining a Cut-Off Point for Scores of the Breastfeeding Self-Efficacy Scale–Short Form: Secondary Data Analysis of an Intervention Study in Japan. PLoS ONE 2015, 10, e0129698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, Y.; Pan, Y.; Lin, S.; Chen, S. Development of Short-Form and Screening Cutoff Point of the Smartphone Addiction Inventory (SPAI-SF). Int. J. Methods Psychiatr. Res. 2017, 26, e1525. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Martínez, M.; Otero, A. Factors Associated with Cell Phone use in Adolescents in the Community of Madrid (Spain). Cyberpsychol. Behav. 2009, 12, 131–137. [Google Scholar] [CrossRef]
- Lopez-Fernandez, O.; Männikkö, N.; Kääriäinen, M.; Griffiths, M.D.; Kuss, D.J. Mobile Gaming and Problematic Smartphone use: A Comparative Study between Belgium and Finland. J. Behave. Addict. 2018, 7, 88–99. [Google Scholar] [CrossRef]
- Roberts, J.A.; Yaya, L.H.P.; Manolis, C. The Invisible Addiction: Cell-Phone Activities and Addiction among Male and Female College Students. J. Behav. Addict. 2014, 3, 254–265. [Google Scholar] [CrossRef] [Green Version]
- Machado Khoury, J.; Maila de Castro, L.N.; Valente Roque, M.A.; Correa de Freitas, A.A.; Ralil da Costa, M.; Duarte Garcia, F. Smartphone and Facebook Addictions Share Common Risk and Prognostic Factors in a Sample of Undergraduate Students. Trends Psychiatry Psychother. 2019, 41, 358–368. [Google Scholar] [CrossRef] [Green Version]
- Smetaniuk, P. A Preliminary Investigation into the Prevalence and Prediction of Problematic Cell Phone Use. J. Behav. Addict. 2014, 3, 41–53. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Mean | SD | n | % | |
|---|---|---|---|---|
| Age | 27.96 | 12.13 | ||
| 18–25 | 1944 | 65.7 | ||
| 26–35 | 408 | 13.8 | ||
| 36–45 | 253 | 8.6 | ||
| Over 46 | 353 | 11.9 | ||
| Gender | ||||
| Men | 1025 | 34.7 | ||
| Women | 1933 | 65.3 | ||
| Age When Started Using A Smartphone | 17.11 | 9.27 | ||
| Smartphone’s Dedication Hours | ||||
| <4 (Nondependent) | 2062 | 69.7 | ||
| ≥4 (Dependent) | 896 | 30.3 | ||
| Smartphone’s Dependence Perception | ||||
| <8 (Nondependent) | 2005 | 67.8 | ||
| ≥8 (Dependent) | 953 | 32.2 |
| SPAI–Spain: | |||||
| Cut-off point = 44 | |||||
| Nondependent | Dependent | ||||
| n | % | n | % | ||
| Dependence Self-Perception | Nondependent | 1371 | 68.4 | 632 | 31.6 |
| Dependent | 255 | 26.8 | 698 | 73.2 | |
| SPAI–Spain: | |||||
| Cut-off point = 42 | |||||
| Nondependent | Dependent | ||||
| n | % | n | % | ||
| Hours of Dedication | Nondependent | 1154 | 56.0 | 906 | 44.0 |
| Dependent | 254 | 28.2 | 643 | 71.8 | |
| Nondependent | Dependent | ||||
|---|---|---|---|---|---|
| N | % | N | % | ||
| Gender | Female | 1041 | 53.9 | 891 | 46.1 |
| Male | 585 | 57.1 | 439 | 42.9 |
| Nondependent | Dependent | ||||
|---|---|---|---|---|---|
| N | % | N | % | ||
| Age Group | 18–25 | 956 | 49.2 | 988 | 50.8 |
| 26–35 | 240 | 59.0 | 167 | 41.0 | |
| 36–45 | 157 | 62.1 | 96 | 37.9 | |
| Over 46 | 273 | 77.6 | 79 | 22.4 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ballestar-Tarín, M.L.; Simó-Sanz, C.; Chover-Sierra, E.; Saus-Ortega, C.; Casal-Angulo, C.; Martínez-Sabater, A. Self-Perception of Dependence as an Indicator of Smartphone Addiction—Establishment of a Cutoff Point in the SPAI–Spain Inventory. Int. J. Environ. Res. Public Health 2020, 17, 3838. https://doi.org/10.3390/ijerph17113838
Ballestar-Tarín ML, Simó-Sanz C, Chover-Sierra E, Saus-Ortega C, Casal-Angulo C, Martínez-Sabater A. Self-Perception of Dependence as an Indicator of Smartphone Addiction—Establishment of a Cutoff Point in the SPAI–Spain Inventory. International Journal of Environmental Research and Public Health. 2020; 17(11):3838. https://doi.org/10.3390/ijerph17113838
Chicago/Turabian StyleBallestar-Tarín, María Luisa, Conchín Simó-Sanz, Elena Chover-Sierra, Carlos Saus-Ortega, Carmen Casal-Angulo, and Antonio Martínez-Sabater. 2020. "Self-Perception of Dependence as an Indicator of Smartphone Addiction—Establishment of a Cutoff Point in the SPAI–Spain Inventory" International Journal of Environmental Research and Public Health 17, no. 11: 3838. https://doi.org/10.3390/ijerph17113838