New Technologies to Improve Pain, Anxiety and Depression in Children and Adolescents with Cancer: A Systematic Review

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Exclusion and Inclusion Criteria
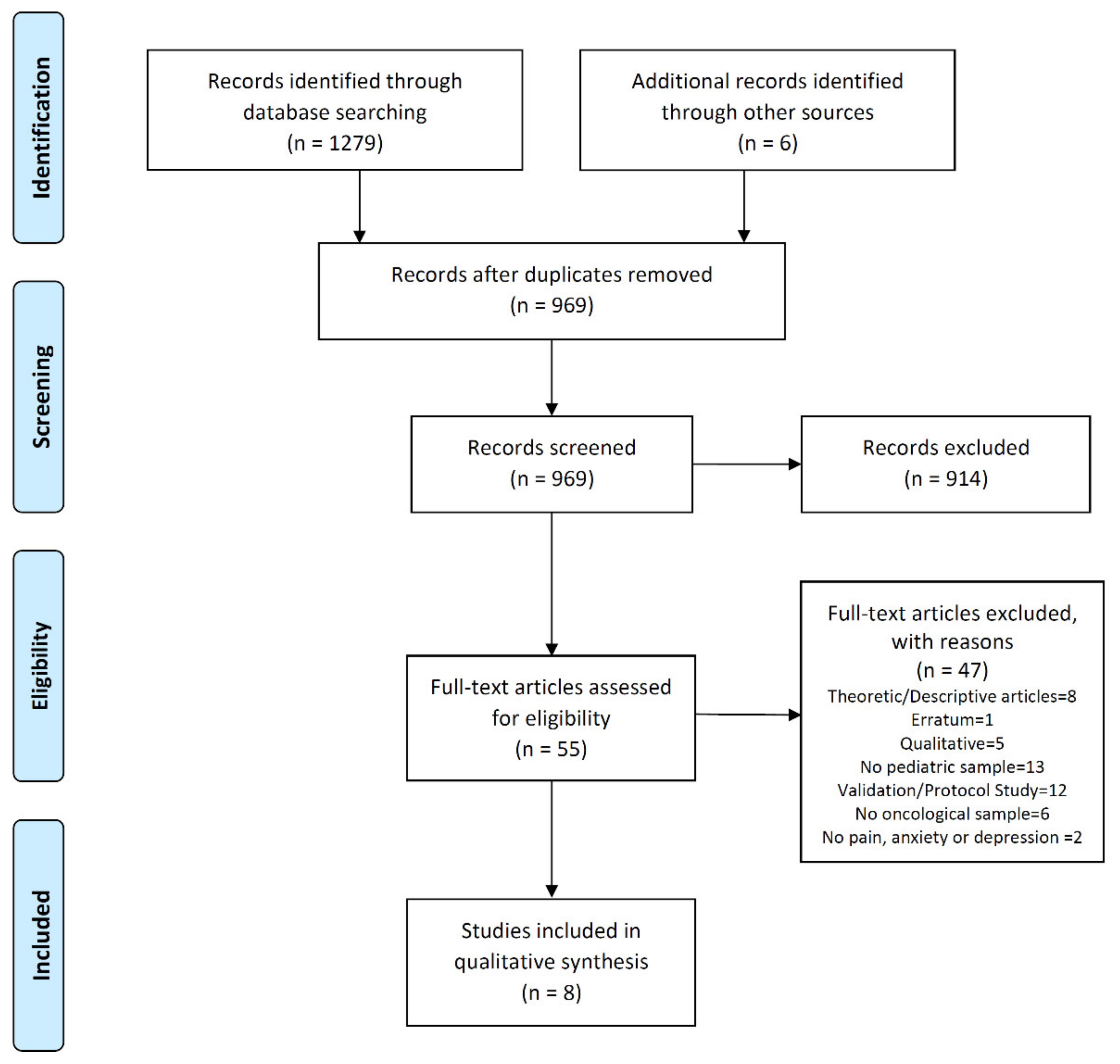
2.3. Screening Process
2.4. Methodological Quality Evaluation
3. Results
3.1. Publication Data
3.2. Participants and Interventions
3.3. Measures and Results
3.4. Intervention Period and Follow up
3.5. Methodological Quality Evaluation
4. Discussion
4.1. Main Findings
4.2. Comparison with Existing Literature
5. Limitations and Strengths
6. Implications and Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Fitzmaurice, C.; Akinyemiju, T.F.; al Lami, F.H.; Alam, T.; Alizadeh-Navaei, R.; Allen, C.; Alsharif, U.; Alvis-Guzman, N.; Amini, E.; Anderson, B.O.; et al. Global, Regional, and National Cancer Incidence, Mortality Years of Life Lost, Tears Lived With Disability, and Disability Adjusted Life-Years for 32 Cancer Groups, 1990 to 205 A systematic Analysis for the Global Burden of Disease Study. JAMA Oncol. 2017, 3, 524–548. [Google Scholar] [CrossRef] [PubMed]
- Ward, E.; DeSantis, C.; Robbins, A.; Kohler, B.; Jemal, A. Childhood and Adolescent Cancer Satistics. CA Cancer J. Clin. 2014, 64, 83–103. [Google Scholar] [CrossRef] [PubMed]
- Steliarova-Foucher, E.; Colombet, M.; Ries, L.A.; Moreno, F.; Dolya, A.; Bray, F.; Hesseling, P.; Shin, H.Y.; Stiller, C.A.; Bouzbid, S.; et al. International incidence of childhood cancer, 2001–2010: A population-based registry study. Lancet Oncol 2017, 18, 719–731. [Google Scholar] [CrossRef]
- Tauty, A.; Noblet, V.; Paillard, C.; Fornecker, L.M.; Namer, I.J.; Bund, C. Evaluation of the effects of chemotherapy on brain glucose metabolism in children with Hodgkin’s lymphoma. Ann. Nucl, Med. 2019, 33, 564–569. [Google Scholar] [CrossRef]
- Nguyen, L.D.; Ehrlich, B.E. Cellular mechanisms and treatments for chemobrain: Insight from aging and neurodegenerative diseases. EMBO Mol. Med. 2020, 29, e12075. [Google Scholar] [CrossRef]
- Schmidt, B.L. The Neurobiology of Cancer Pain. Neuroscientist 2014, 20, 546–562. [Google Scholar] [CrossRef] [Green Version]
- Yamanaka, M. A Concept Analysis of Self-Management of Cancer Pain. Asia Pac. J. Oncol. Nurs. 2018, 5, 254–261. [Google Scholar] [CrossRef]
- Adam, R.; De Bruin, M.; Burton, C.D.; Bond, C.M.; Clausen, M.G.; Murchie, P. What are the current challenges of managing cancer pain and could digital technologies help? BMJ Supportive Palliat. Care 2018, 8, 204–212. [Google Scholar] [CrossRef] [Green Version]
- Compas, B.E.; Desjardins, L.; Vannatta, K.; Young-Saleme, T.; Rodríguez, E.M.; Dunn, M.; Bemis, H.; Snyder, S.; Gerhadt, C.A. Children and Adolescents Coping With Cancer: Self-and Parent Reports of Coping and Anxiety/Depression. Health Psychol. 2014, 33, 853–861. [Google Scholar] [CrossRef] [Green Version]
- Park, E.M.; Rosenstein, D.L. Depression in adolescents and young adults with cancer. Dialogues Clin. Neurosci. 2015, 17, 171–180. [Google Scholar]
- Choo, C.C.; Chew, P.K.H.; Tan, P.; Choo, J.Q.; Choo, A.M.H.; Ho, R.C.; Quah, T.C. Health-Related Quality of Life in Pediatric Patients with Leukemia in Singapore: A Cross-Sectional Pilot Study. Int. J. Environ. Res. Public Health 2019, 16, 2069. [Google Scholar] [CrossRef] [Green Version]
- Arane, K.; Behboudi, A.; Goldman, R.D. Virtual reality for pain and anxiety management in children. Can. Fam. Physician 2017, 63, 932–934. [Google Scholar]
- Lee, J.; Park, S.H.; Ju, J.H.; Cho, J.H. Application of a real-time pain monitoring system in Korean fybromialgia patients: A pilot study. Int. J. Rheum Dis. 2019, 1–6. [Google Scholar] [CrossRef]
- Irvine, A.B.; Russell, H.; Manocchia, M.; Mino, D.E.; Cox Glassen, T.; Morgan, R.; Gau, J.M.; Birney, A.J.; Ary, D.V. Mobile-Web App to Self-Manage Low Back Pain: Randomized Controlled Trial. J. Med. Internet Res. 2015, 17, e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hernández, S.E.; Lawler, S.; Langbecker, D. The effectiveness of mHealth for self-management in improving pain, psychological distress, fatigue and sleep in cancer survivors: A systematic review. J. Cancer Surviv. 2019, 12, 97–107. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Moseley, A.M.; Herbert, R.D.; Sherrington, C.; Maher, C.G. Evidence for physiotherapy practice: A survey of the Physiotherapy Evidence Database (PEDro). Aust. J. Physiother. 2002, 48, 43–49. [Google Scholar] [CrossRef] [Green Version]
- Jibb, L.; Birnie, K.A.; Nathan, P.C.; Beran, T.N.; Hum, V.; Victor, J.C.; Stinson, J.N. Using the MEDiPORT humanoid robot to reduce procedural pain and distress in children with cancer: A pilot randomized controlled trial. Pediatr. Blood Cancer 2018, 65, e27242. [Google Scholar] [CrossRef]
- Alemi, M.; Meghdari, A.; Ghanbarzadeh, A. Impact of a Social Humanoid Robot as a Therapy Assistant in Children Cancer Treatment. In Proceedings of the Social Robotics 6th International Conference, Sydney, Australia, 27–29 October 2014. [Google Scholar]
- Fazelniya, Z.; Najafi, M.; Moafi, A.; Talakoub, S. The Impact of an Interactive Computer Game on the Quality of Life of Children Undergoing Chemotherapy. Iran. J. Nurs. Midwifery Res. 2017, 22, 431–435. [Google Scholar] [CrossRef]
- Atzori, B.; Hoffman, H.G.; Vagnoli, L.; Patterson, D.R.; Alhalabi, W.; Messeri, A.; Lauro Grotto, R. Virtual Reality Analgesia During Venipuncture in Pediatric Patients With Onco-Hematological Diseases. Front. Psychol. 2018, 9, 2508. [Google Scholar] [CrossRef]
- Nilsson, S.; Finnstrom, B.; Kokinsky, E.; Enskar, K. The use of Virtual Reality for needle-related procedural pain and distress in children and adolescents in a paediatric oncologic unit. Eur. J. Oncol. Nurs. 2009, 13, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Chung, J.; Ho, E. The effectiveness of therapeutic play, using virtual reality computer games, in promoting the psychological well-being of children hospitalised with cancer. J. Clin. Nurs. 2011, 20, 2135–2143. [Google Scholar] [CrossRef]
- Li, W.; Chung, J.; Ho, E.; Chiu, S. Effectiveness and feasibility of using the computerized interactive virtual space in reducing depressive symptoms of Hong Kong Chinese children hospitalized with cancer. J. Spec. Pediatr. Nurs. 2011, 16, 190–198. [Google Scholar] [CrossRef] [PubMed]
- Jibb, L.; Stevens, B.J.; Nathan, P.C.; Seto, E.; Cafazzo, J.A.; Johnston, D.L.; Hum, V.; Stinson, J.N. Implementation and preliminary effectiveness of a real-time pain management smartphone app for adolescents with cancer: A multicenter pilot clinical study. Pediatr. Blood Cancer 2017, 64, e26554. [Google Scholar] [CrossRef] [PubMed]
- Fundación Española para la Ciencia y la Tecnología. FECYT web site. Available online: http://jcr.fecyt.es (accessed on 28 February 2019).
- Beran, T.N.; Ramirez-Serrano, A.; Vanderkooi, O.G.; Kuhn, S. Reducing children’s pain and distress towards flu vaccinations: A novel and effective application of humanoid robotics. Vaccine 2013, 31, 2772–2777. [Google Scholar] [CrossRef] [PubMed]
- Govender, M.; Bowen, R.C.; German, M.L.; Bulaj, G.; Bruggers, C.S. Clinical and Neurobiological Perspectives of Empowering Pediatric Cancer Patients Using Videogames. Games Health J. 2015, 4, 362–374. [Google Scholar] [CrossRef] [PubMed]
- Staiano, A.E.; Flynn, R. Therapeutic Uses of Active Videogames: A Systematic Review. Games Health J. 2014, 3, 351–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garret, B.; Taverner, T.; McDade, P. Virtual Reality as an Adjunct Home Therapy in Chronic Pain Management: An Exploratory Study. JMIR Med. Inform. 2017, 5, e11. [Google Scholar] [CrossRef]
- Won, A.S.; Bailey, J.; Bailenson, J.; Tataru, C.; Yoon, I.A.; Golianu, B. Immersive Virtual Reality for Pediatric Pain. Children (Basel) 2017, 4, 52. [Google Scholar] [CrossRef] [Green Version]
- Higgins, K.S.; Tutelman, P.R.; Chambers, C.T.; Witteman, H.O.; Barwick, M.; Corkum, P.; Grant, D.; Stinson, J.N.; Lalloo, C.; Robins, S.; et al. Availability of researcher-led eHealth tolos for pain assessment and management: Barriers, facilitators, costs, and design. Pain Rep. 2018, 3, e686. [Google Scholar] [CrossRef]
- Do, T.; Le, M.D.; Van Nguyen, T.; Tran, B.X.; Le, H.T.; Nguyen, H.D.; Nguyen, L.H.; Nguyen, C.T.; Tran, T.D.; Latkin, C.A.; et al. Receptiveness and preferences of Health-related Smartphone applications among Vietnamese youth and young adults. BCM Public Health 2018, 18, 764. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.W.B.; Ho, R.C.M. Enabling Psychiatrists to Explore the Full Potential of E-Health. Front. Psychiatry 2015, 6, 177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anthes, E. Pocket Psychiatry. Nature 2016, 530, 20–23. [Google Scholar] [CrossRef]
- Zhang, M.W.B.; Ho, R.C.M.; Ng, C.G. 5-Minutes Mindfulness for palliative care: Integrating evidence and good design. Technol. Health Care 2017, 25, 1173–1176. [Google Scholar] [CrossRef] [PubMed]
- Dupuis, L.L.; Lu, X.; Mitchell, H.R.; Sung, L.; Devidas, M.; Mattano, L.A., Jr.; Carroll, W.L.; Winick, N.; Hunger, S.P.; Maloney, K.W.; et al. Anxiety, pain, and nausea during the treatment of standart-risk childhood acute lymphoblastic leukemia: A prospective, longitudinal study fom the Children’s Oncology Group. Cancer 2016, 122, 1116–1125. [Google Scholar] [CrossRef]
- Myers, R.M.; Balsamo, L.; Lu, X.; Devidas, M.; Hunger, S.P.; Carroll, W.L.; Winick, N.J.; Maloney, K.W.; Kadan-Lottick, N.S. A prospective study of anxiety, depression, and behavioral changes in the first year after a diagnosis of childhood acute lymphoblastic leukemia: A report from the Children’s Oncology Group. Cancer 2014, 1, 1417–1425. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Study | Design | Population | Outcomes | Intervention | Timing | Results | Limitations | Selection Criteria |
|---|---|---|---|---|---|---|---|---|
| Alemi M et al. [19] | RCT | 11 participants with any type of cancer. 7–12 years (Mean = 9.45) GC: n = 5 GI: n = 10; 4 dropouts Does not specify gender | Anxiety: MASC. Depression: CDI. Anger: CIA. | Use of the Robot NAO in 8 scenarios (8 sessions during 3 weeks) Different roles in each session. | Pretest: Before 1st session Post-test: after 3 weeks of intervention | GI: Decrease anxiety, depression and anger. GC: No differences | Small sample Difficulty to complete 8 sessions They knew the research team before study | Pediatric sample. Participants in active oncological treatment. |
| Fazelniya Z et al. [20] | RCT with two step test plan of before and after the intervention | 64 participants with cancer in active Chemotherapy treatment 8–12 years (Mean = 10.05) GC: n = 32; (Mean age: 10.2) GI: n = 32; (Mean age: 9.9) 30 girls (46.88%) | Quality of Life: PedsQL with specific dimensions for pediatric cancer (pain and anxiety) | GI: Play a Videogame 3 h peer week 1 month GC: Care routine | Pretest: Before intervention Post-test: Immediately after the intervention Follow-up: 4 weeks in the intervention’s period | GI: Improve quality of life after intervention and 1 month of follow-up GC: No changes | Small sample Short follow-up. Use of other ways to education during the study | Pediatric sample with any type of cancer. Ability to read and use videogames. No physical or mental deficits before the disease. |
| Jibb L et al. [25] | A pilot one-group pre-post study | N = 40 participants with cancer 12–18 years old (Mean: 14.2) 17 girls (43%) | Effectiveness of the mobile App: AES. Pain: BPI. Interference of pain: PROMIS-PPI-SFS Quality of Life: PedsQL. Self-efficacy: GSE-Sherer. | Use an app during 28 days and participants’ valuation after intervention. | Pretest: Before intervention Post-test after Intervention Follow up: 28 days in the intervention’s period. | GI: Improves pain intensity and interference. Good adherence although it was reduced over time | Pilot Study. Small sample. No control group. | Pediatric sample Active oncological treatment at least 2 months Pain registers higher than 3 (VAS) at least once a week prior selection. Not comorbidities. Not final phase of life. |
| Atzori B et al. [21] | RCT | N= 15 participants with cancer (n = 11) and hematological diseases. (n = 4). GC: n = 15 GI: n = 15 (They all go through both conditions) 5 girls (33.3%) Mean age: 10.92 | Pain: VAS Quality of VR: Self-administered questionnaire. Sickness: VAS Fun: VAS | GI: Use of VR during a venous puncture. GC: A conversation as a distraction | A single measurement after the application of the invasive technique. | GI: Improve pain after use VR during invasive technique. Higher level of fun. GC: Higher level of pain. No sickness differences between groups. | Small sample. Use of a care standard as an intervention in the GC instead of a Conventional intervention. | Pediatric sample with oncological and hematological diseases. Participants without physical or mental deficits before disease. Able to wear a helmet and willing to interact with the VR environment. |
| Nilsson et al. [22] | RCT | 42 participants with any type of cancer. 5–18 years (Mean age: 11) GC: n = 21 (Mean age: 11) GI: n = 21 (Mean age: 11) 4 dropouts. 17 girls (40.5%) | Pain: CAS, FAS, FLACC, Heart rate. | VR as a distraction during a puncture. | Test before intervention, during intervention and immediately after the intervention. No follow up. | No significant differences between GC and GI. | Small sample. Difficulty to adapt the VR to the procedure. | Pediatric sample with any type of cancer. No cognitive impairments. |
| Li et al. [23] | Quasi experimental control group pre-post between-subject design. | 122 participants with any type of cancer 8–16 years (No mean age in total group) GC: n = 70 (Mean age: 12.1) GI: n= 52 (Mean age: 11.6) No dropouts. 57 girls (46.7%) | State Anxiety: CSAS-C; Depressive symptom: CES-DC | Game of Virtual reality in groups | Two phases: pre-test (phase 1), a washing period, (1 month), post-test (phase 2). No follow up. | GI: Decrease depressive symptom. No significative differences in anxiety. GC: No changes. | Little generalizable results. Difficulty to participate in intervention after chemotherapy | Pediatric sample with any type of cancer. No cognitive or learning problems. |
| Li et al. [24] | Quasi experimental control group pre-post between-subject design. | 122 participants with any type of cancer. 8–16 years. GC: n = 70 (Mean age: 12.1) GI: n= 52 (Mean age: 11.6). No dropouts. 57 girls (46.7%). | Depressive symptom: CES-DC. | Game of Virtual reality in groups | Two phases: pre-test (phase 1), a washing period, (1 month), post-test (phase 2). No follow up | GI: Decrease depressive symptom. GC: No changes. | Little generalizable results. Difficulty to participate in intervention after chemotherapy | Pediatric sample with any type of cancer. No cognitive or learning problems. |
| Jibb L et al. [18] | Parallel Clinical randomized trial | N= 40 participants with cancer 4–9 years old. Mean of age: 6.2 16 girls (40%) GI: n = 19 GC: n = 21 | Pain: FPS-R Stress: BAADS Fear: CFS | Robot that uses cognitive-behavioral interventions or dances and sings during puncture. | Pretest: Pain level in previous punctures. Post-test: Immediately after the intervention. | There were not differences in pain, fear and stress levels in both groups. | Results difficult to generalize (single site study). Limited robot ability to assess impact on pain | Pediatric sample. In active oncological treatment at least 1 month since diagnosed. No previous physical or mental problems. Previously exposed to venous punctures. |
| Study | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Alemi M et al. [19] | Y | N | N | Y | N | N | N | N | N | Y | Y | 4 (fair) |
| Fazelniya Z et al. [20] | Y | Y | N | Y | N | N | N | Y | Y | Y | Y | 7 (good) |
| Jibb L et al. [25] | Y | N | N | Y | N | N | N | N | N | N | Y | 3 (poor) |
| Atzori B et al. [21] | Y | Y | N | Y | N | N | N | Y | Y | N | Y | 6 (good) |
| Jibb L et al. [18] | Y | Y | N | Y | N | N | Y | Y | Y | Y | Y | 8 (good) |
| Nilsson et al. [22] | Y | N | N | Y | N | N | N | Y | N | Y | Y | 5 (fair) |
| Li et al. [23] | Y | N | N | Y | N | Y | Y | Y | N | Y | Y | 7 (good) |
| Li et al. [24] | Y | N | N | Y | N | Y | Y | Y | N | Y | Y | 7 (good) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lopez-Rodriguez, M.M.; Fernández-Millan, A.; Ruiz-Fernández, M.D.; Dobarrio-Sanz, I.; Fernández-Medina, I.M. New Technologies to Improve Pain, Anxiety and Depression in Children and Adolescents with Cancer: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 3563. https://doi.org/10.3390/ijerph17103563
Lopez-Rodriguez MM, Fernández-Millan A, Ruiz-Fernández MD, Dobarrio-Sanz I, Fernández-Medina IM. New Technologies to Improve Pain, Anxiety and Depression in Children and Adolescents with Cancer: A Systematic Review. International Journal of Environmental Research and Public Health. 2020; 17(10):3563. https://doi.org/10.3390/ijerph17103563
Chicago/Turabian StyleLopez-Rodriguez, María Mar, Alejandro Fernández-Millan, María Dolores Ruiz-Fernández, Iria Dobarrio-Sanz, and Isabel María Fernández-Medina. 2020. "New Technologies to Improve Pain, Anxiety and Depression in Children and Adolescents with Cancer: A Systematic Review" International Journal of Environmental Research and Public Health 17, no. 10: 3563. https://doi.org/10.3390/ijerph17103563