Immediate Effects of Medially Posted Insoles on Lower Limb Joint Contact Forces in Adult Acquired Flatfoot: A Pilot Study


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
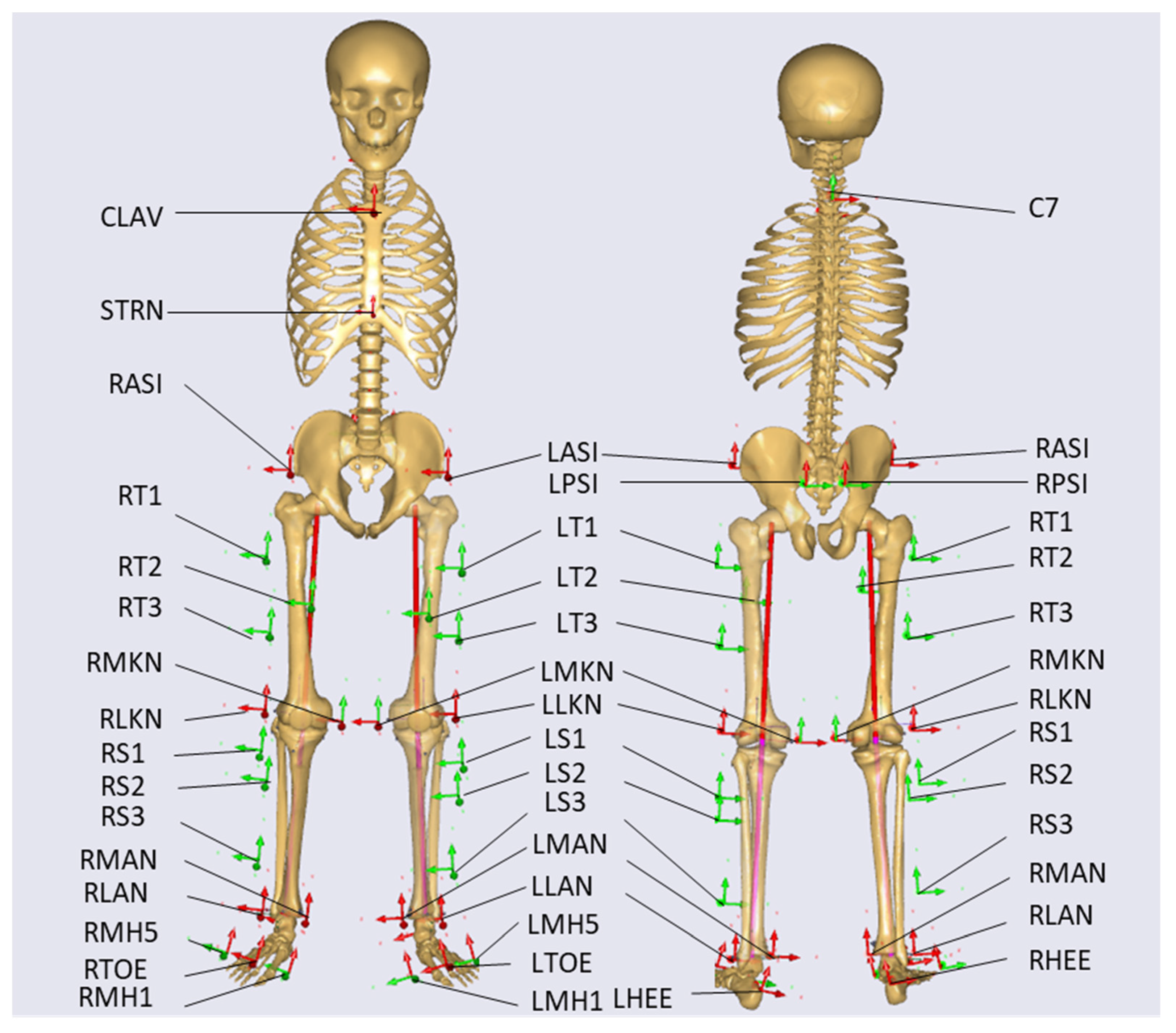
2.2. Equipment and Procedure
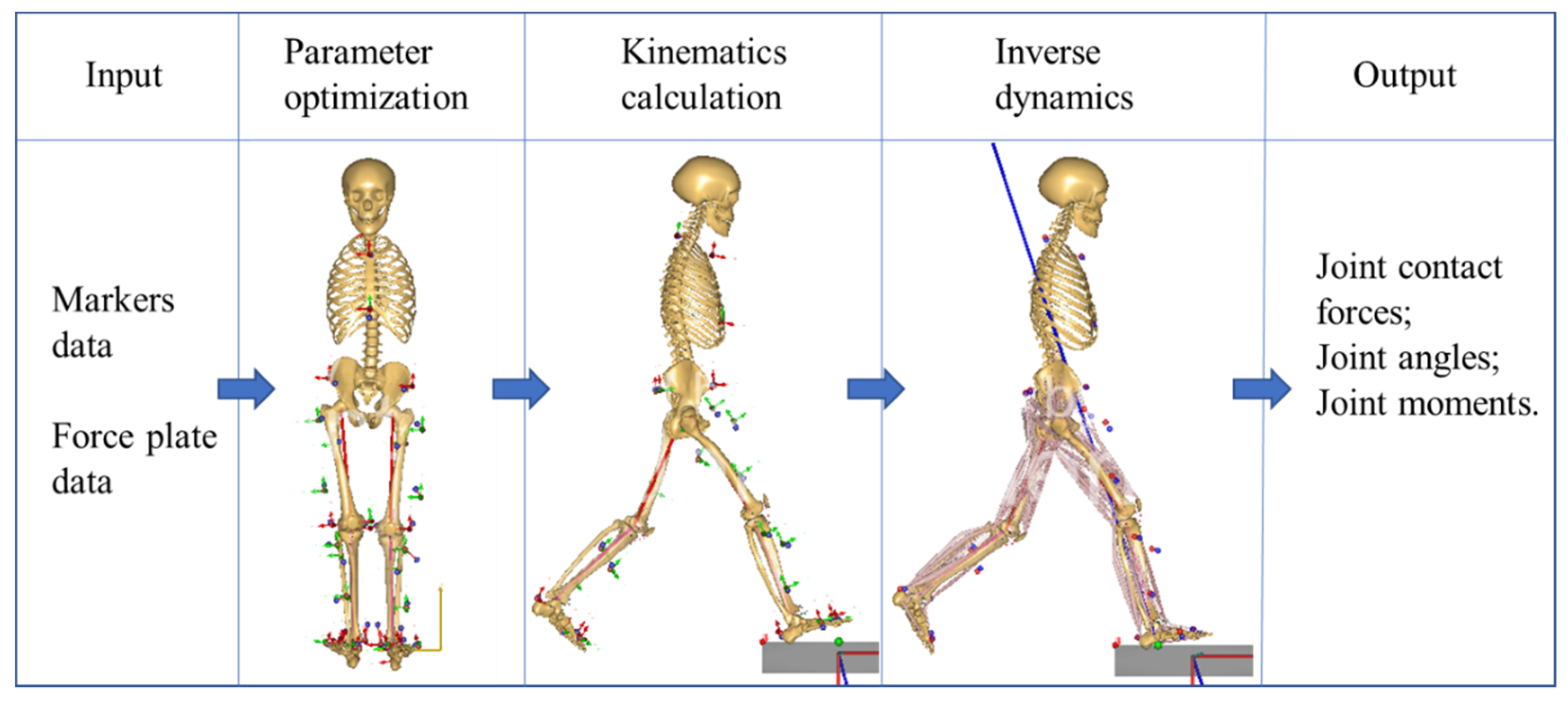
2.3. Musculoskeletal Model
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Shibuya, N.; Jupiter, D.C.; Ciliberti, L.J.; VanBuren, V.; La Fontaine, J. Characteristics of adult flatfoot in the United States. J. Foot Ankle Surg. 2010, 49, 363–368. [Google Scholar] [CrossRef]
- Golightly, Y.M.; Hannan, M.T.; Dufour, A.B.; Jordan, J.M. Racial differences in foot disorders and foot type. Arthritis Care Res. (Hoboken) 2012, 64, 1756–1759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- López-López, D.; Vilar-Fernández, J.M.; Barros-García, G.; Losa-Iglesias, M.E.; Palomo-López, P.; Becerro-de-Bengoa-Vallejo, R.; Calvo-Lobo, C. Foot arch height and quality of life in adults: A strobe observational study. Int. J. Environ. Res. Public Health 2018, 15, 1555. [Google Scholar] [CrossRef] [Green Version]
- Banwell, H.A.; Mackintosh, S.; Thewlis, D. Foot orthoses for adults with flexible pes planus: A systematic review. J. Foot Ankle Res. 2014, 7, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Angin, S.; Crofts, G.; Mickle, K.J.; Nester, C.J. Ultrasound evaluation of foot muscles and plantar fascia in pes planus. Gait Posture 2014, 40, 48–52. [Google Scholar] [CrossRef] [Green Version]
- Kirby, K.A. Longitudinal arch load-sharing system of the foot. Revista Española de Podología 2017, 28, e18–e26. [Google Scholar] [CrossRef]
- Murley, G.S.; Tan, J.M.; Edwards, R.M.; De Luca, J.; Munteanu, S.E.; Cook, J.L. Foot posture is associated with morphometry of the peroneus longus muscle, tibialis anterior tendon, and Achilles tendon. Scand J. Med. Sci. Sports 2014, 24, 535–541. [Google Scholar] [CrossRef]
- Riskowski, J.L.; Dufour, A.B.; Hagedorn, T.J.; Hillstrom, H.J.; Casey, V.A.; Hannan, M.T. Associations of foot posture and function to lower extremity pain: Results from a population-based foot study. Arthritis Care Res. (Hoboken) 2013, 65, 1804–1812. [Google Scholar] [CrossRef] [Green Version]
- Squires, N.A.; Jeng, C.L. Posterior Tibial Tendon Dysfunction. Oper. Tech. Orthop. 2006, 16, 44–52. [Google Scholar] [CrossRef]
- Levinger, P.; Gilleard, W. Tibia and rearfoot motion and ground reaction forces in subjects with patellofemoral pain syndrome during walking. Gait Posture 2007, 25, 2–8. [Google Scholar] [CrossRef]
- Razeghi, M.; Ebrahimi, S.; Yazdani, F. The comparison of patellofemoral joint forces between flat footed and normal subjects during stance phase of gait. Gait Posture 2012, S38. [Google Scholar] [CrossRef]
- Ramappa, A.J.; Apreleva, M.; Harrold, F.R.; Fitzgibbons, P.G.; Wilson, D.R.; Gill, T.J. The effects of medialization and anteromedialization of the tibial tubercle on patellofemoral mechanics and kinematics. Am. J. Sports Med. 2006, 34, 749–756. [Google Scholar] [CrossRef] [PubMed]
- Wahmkow, G.; Cassel, M.; Mayer, F.; Baur, H. Effects of different medial arch support heights on rearfoot kinematics. PLoS ONE 2017, 12, e0172334. [Google Scholar] [CrossRef] [PubMed]
- Kosonen, J.; Kulmala, J.-P.; Müller, E.; Avela, J. Effects of medially posted insoles on foot and lower limb mechanics across walking and running in overpronating men. J. Biomech. 2017, 54, 58–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jafarnezhadgero, A.A.; Shad, M.M.; Majlesi, M. Effect of foot orthoses on the medial longitudinal arch in children with flexible flatfoot deformity: A three-dimensional moment analysis. Gait Posture 2017, 55, 75–80. [Google Scholar] [CrossRef]
- Telfer, S.; Abbott, M.; Steultjens, M.P.; Woodburn, J. Dose-response effects of customised foot orthoses on lower limb kinematics and kinetics in pronated foot type. J. Biomech. 2013, 46, 1489–1495. [Google Scholar] [CrossRef]
- Liu, A.; Nester, C.J.; Jones, R.K.; Lundgren, P.; Lundberg, A.; Arndt, A.; Wolf, P. Effect of an antipronation foot orthosis on ankle and subtalar kinematics. Med. Sci. Sports Exerc. 2012, 44, 2384–2391. [Google Scholar] [CrossRef]
- Desmyttere, G.; Hajizadeh, M.; Bleau, J.; Begon, M. Effect of foot orthosis design on lower limb joint kinematics and kinetics during walking in flexible pes planovalgus: A systematic review and meta-analysis. Clin. Biomech. 2018, 59, 117–129. [Google Scholar] [CrossRef]
- Hsu, W.-H.; Lewis, C.L.; Monaghan, G.M.; Saltzman, E.; Hamill, J.; Holt, K.G. Orthoses posted in both the forefoot and rearfoot reduce moments and angular impulses on lower extremity joints during walking. J. Biomech. 2014, 47, 2618–2625. [Google Scholar] [CrossRef]
- Miyazaki, T.; Wada, M.; Kawahara, H.; Sato, M.; Baba, H.; Shimada, S. Dynamic load at baseline can predict radiographic disease progression in medial compartment knee osteoarthritis. Ann. Rheum. Dis. 2002, 61, 617–622. [Google Scholar] [CrossRef]
- Damsgaard, M.; Rasmussen, J.; Christensen, S.T.; Surma, E.; De Zee, M. Analysis of musculoskeletal systems in the AnyBody Modeling System. Simul. Model. Pract. Theory 2006, 14, 1100–1111. [Google Scholar] [CrossRef]
- Modenese, L.; Montefiori, E.; Wang, A.; Wesarg, S.; Viceconti, M.; Mazza, C. Investigation of the dependence of joint contact forces on musculotendon parameters using a codified workflow for image-based modelling. J. Biomech. 2018, 73, 108–118. [Google Scholar] [CrossRef]
- Hoang, H.X.; Diamond, L.E.; Lloyd, D.G.; Pizzolato, C. A calibrated EMG-informed neuromusculoskeletal model can appropriately account for muscle co-contraction in the estimation of hip joint contact forces in people with hip osteoarthritis. J. Biomech. 2019, 83, 134–142. [Google Scholar] [CrossRef] [Green Version]
- Kim, N.; Browning, R.C.; Lerner, Z.F. The effects of pediatric obesity on patellofemoral joint contact force during walking. Gait & Posture 2019, 73, 209–214. [Google Scholar] [CrossRef]
- Lin, Y.C.; Walter, J.P.; Pandy, M.G. Predictive Simulations of Neuromuscular Coordination and Joint-Contact Loading in Human Gait. Ann. Biomed. Eng. 2018, 46, 1216–1227. [Google Scholar] [CrossRef]
- Marra, M.A.; Vanheule, V.; Fluit, R.; Koopman, B.H.; Rasmussen, J.; Verdonschot, N.; Andersen, M.S. A subject-specific musculoskeletal modeling framework to predict in vivo mechanics of total knee arthroplasty. J. Biomech. Eng. 2015, 137, 020904. [Google Scholar] [CrossRef]
- Chen, Z.; Zhang, X.; Ardestani, M.M.; Wang, L.; Liu, Y.; Lian, Q.; He, J.; Li, D.; Jin, Z. Prediction of in vivo joint mechanics of an artificial knee implant using rigid multi-body dynamics with elastic contacts. Proc. Inst. Mech. Eng. H 2014, 228, 564–575. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Xiong, S.; Goonetilleke, R.S.; Witana, C.P.; Weerasinghe, T.W.; Au, E.Y.L. Foot Arch Characterization. J. Am. Podiat. Med. Assoc. 2010, 100, 14–24. [Google Scholar] [CrossRef] [Green Version]
- Roy, H.; Bhattacharya, K.; Deb, S.; Ray, K. Arch index: An easier approach for arch height (a regression analysis). Al Ameen J. Med. Sci. 2012, 5, 137–146. [Google Scholar]
- Jahss, M.H.; Kummer, F.; Michelson, J.D. Investigations into the fat pads of the sole of the foot: Heel pressure studies. Foot & Ankle 1992, 13, 227–232. [Google Scholar] [CrossRef]
- Lower body modeling with Plug-in Gait. 2002. Available online: https://docs.vicon.com/display/Nexus25/Lower+body+modeling+with+Plug-in+Gait (accessed on 25 March 2020).
- Horsman, M.K.; Koopman, H.F.; van der Helm, F.C.; Prosé, L.P.; Veeger, H. Morphological muscle and joint parameters for musculoskeletal modelling of the lower extremity. Clin. Biomech. 2007, 22, 239–247. [Google Scholar] [CrossRef]
- Peng, Y.; Zhang, Z.; Gao, Y.; Chen, Z.; Xin, H.; Zhang, Q.; Fan, X.; Jin, Z. Concurrent prediction of ground reaction forces and moments and tibiofemoral contact forces during walking using musculoskeletal modelling. Med. Eng. Phys. 2018, 52, 31–40. [Google Scholar] [CrossRef]
- Richards, R.E.; Andersen, M.S.; Harlaar, J.; van den Noort, J.C. Relationship between knee joint contact forces and external knee joint moments in patients with medial knee osteoarthritis: Effects of gait modifications. Osteoarthr. Cartil. 2018, 26, 1203–1214. [Google Scholar] [CrossRef]
- Mannisi, M.; Dell’Isola, A.; Andersen, M.S.; Woodburn, J. Effect of lateral wedged insoles on the knee internal contact forces in medial knee osteoarthritis. Gait Posture 2019, 68, 443–448. [Google Scholar] [CrossRef]
- McGough, J.J.; Faraone, S.V. Estimating the size of treatment effects: Moving beyond p values. Psychiatry (Edgmont (Pa. Township)) 2009, 6, 21–29. [Google Scholar]
- Wong, D.W.-C.; Zhang, M.; Yu, J.; Leung, A.K.-L. Biomechanics of first ray hypermobility: An investigation on joint force during walking using finite element analysis. Med. Eng. Phys. 2014, 36, 1388–1393. [Google Scholar] [CrossRef]
- Brognara, L.; Navarro-Flores, E.; Iachemet, L.; Serra-Catalá, N.; Cauli, O. Beneficial Effect of Foot Plantar Stimulation in Gait Parameters in Individuals with Parkinson’s Disease. Brain Sci. 2020, 10, 69. [Google Scholar] [CrossRef] [Green Version]
- Alvarez, R.G.; Marini, A.; Schmitt, C.; Saltzman, C.L. Stage I and II Posterior Tibial Tendon Dysfunction Treated by a Structured Nonoperative Management Protocol: An Orthosis and Exercise Program. Foot Ankle Int. 2006, 27, 2–8. [Google Scholar] [CrossRef]
- Kohls-Gatzoulis, J.; Angel, J.C.; Singh, D.; Haddad, F.; Livingstone, J.; Berry, G. Tibialis posterior dysfunction: A common and treatable cause of adult acquired flatfoot. Brit. Med. J. 2004, 329, 1328. [Google Scholar] [CrossRef] [Green Version]
- Wong, D.W.-C.; Wang, Y.; Chen, T.L.-W.; Leung, A.K.-L.; Zhang, M. Biomechanical consequences of subtalar joint arthroereisis in treating posterior tibial tendon dysfunction: A theoretical analysis using finite element analysis. Comput. Methods Biomech. Biomed. Eng. 2017, 20, 1525–1532. [Google Scholar] [CrossRef]
- Wong, D.W.-C.; Wang, Y.; Leung, A.K.-L.; Yang, M.; Zhang, M. Finite element simulation on posterior tibial tendinopathy: Load transfer alteration and implications to the onset of pes planus. Clin. Biomech. 2018, 51, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Rabbito, M.; Pohl, M.B.; Humble, N.; Ferber, R. Biomechanical and clinical factors related to stage I posterior tibial tendon dysfunction. J. Orthop. Sports Phys. Ther. 2011, 41, 776–784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murley, G.S.; Buldt, A.K.; Trump, P.J.; Wickham, J.B. Tibialis posterior EMG activity during barefoot walking in people with neutral foot posture. J. Electromyogr. Kinesiol. 2009, 19, e69–e77. [Google Scholar] [CrossRef]
- Kutzner, I.; Trepczynski, A.; Heller, M.O.; Bergmann, G. Knee adduction moment and medial contact force--facts about their correlation during gait. PLoS ONE 2013, 8, e81036. [Google Scholar] [CrossRef] [PubMed]
- Saxby, D.J.; Modenese, L.; Bryant, A.L.; Gerus, P.; Killen, B.; Fortin, K.; Wrigley, T.V.; Bennell, K.L.; Cicuttini, F.M.; Lloyd, D.G. Tibiofemoral contact forces during walking, running and sidestepping. Gait Posture 2016, 49, 78–85. [Google Scholar] [CrossRef] [Green Version]
- Banwell, H.A.; Thewlis, D.; Mackintosh, S. Adults with flexible pes planus and the approach to the prescription of customised foot orthoses in clinical practice: A clinical records audit. The Foot 2015, 25, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Tang, S.F.; Chen, C.H.; Wu, C.K.; Hong, W.H.; Chen, K.J.; Chen, C.K. The effects of total contact insole with forefoot medial posting on rearfoot movement and foot pressure distributions in patients with flexible flatfoot. Clin. Neurol. Neurosurg. 2015, 129, S8–S11. [Google Scholar] [CrossRef]
- Brown, G.P.; Donatelli, R.; Catlin, P.A.; Wooden, M.J. The effect of two types of foot orthoses on rearfoot mechanics. J. Orthop. Sports Phys. Ther. 1995, 21, 258–267. [Google Scholar] [CrossRef] [Green Version]
- Leung, A.K.; Mak, A.F.; Evans, J.H. Biomedical gait evaluation of the immediate effect of orthotic treatment for flexible flat foot. Prosthet. Orthot. Int. 1998, 22, 25–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stacoff, A.; Quervain, I.K.-d.; Dettwyler, M.; Wolf, P.; List, R.; Ukelo, T.; Stüssi, E. Biomechanical effects of foot orthoses during walking. The Foot 2007, 17, 143–153. [Google Scholar] [CrossRef]
- Wang, Y.; Wong, D.W.-C.; Zhang, M. Computational Models of the Foot and Ankle for Pathomechanics and Clinical Applications: A Review. Ann. Biomed. Eng. 2016, 44, 213. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Wong, D.W.-C.; Zhang, H.; Luo, Z.-P.; Zhang, M. The influence of high-heeled shoes on strain and tension force of the anterior talofibular ligament and plantar fascia during balanced standing and walking. Med. Eng. Phys. 2016, 38, 1152–1156. [Google Scholar] [CrossRef]
- Cheung, J.T.-M.; Yu, J.; Wong, D.W.-C.; Zhang, M. Current methods in computer-aided engineering for footwear design. Footwear Sci. 2009, 1, 31–46. [Google Scholar] [CrossRef]
- Rodríguez-Sanz, D.; Tovaruela-Carrión, N.; López-López, D.; Palomo-López, P.; Romero-Morales, C.; Navarro-Flores, E.; Calvo-Lobo, C. Foot disorders in the elderly: A mini-review. Disease-a-Month 2018, 64, 64–91. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | WSFO Mean (SD) | WS Mean (SD) | p−Value | ES (95% CI) |
|---|---|---|---|---|
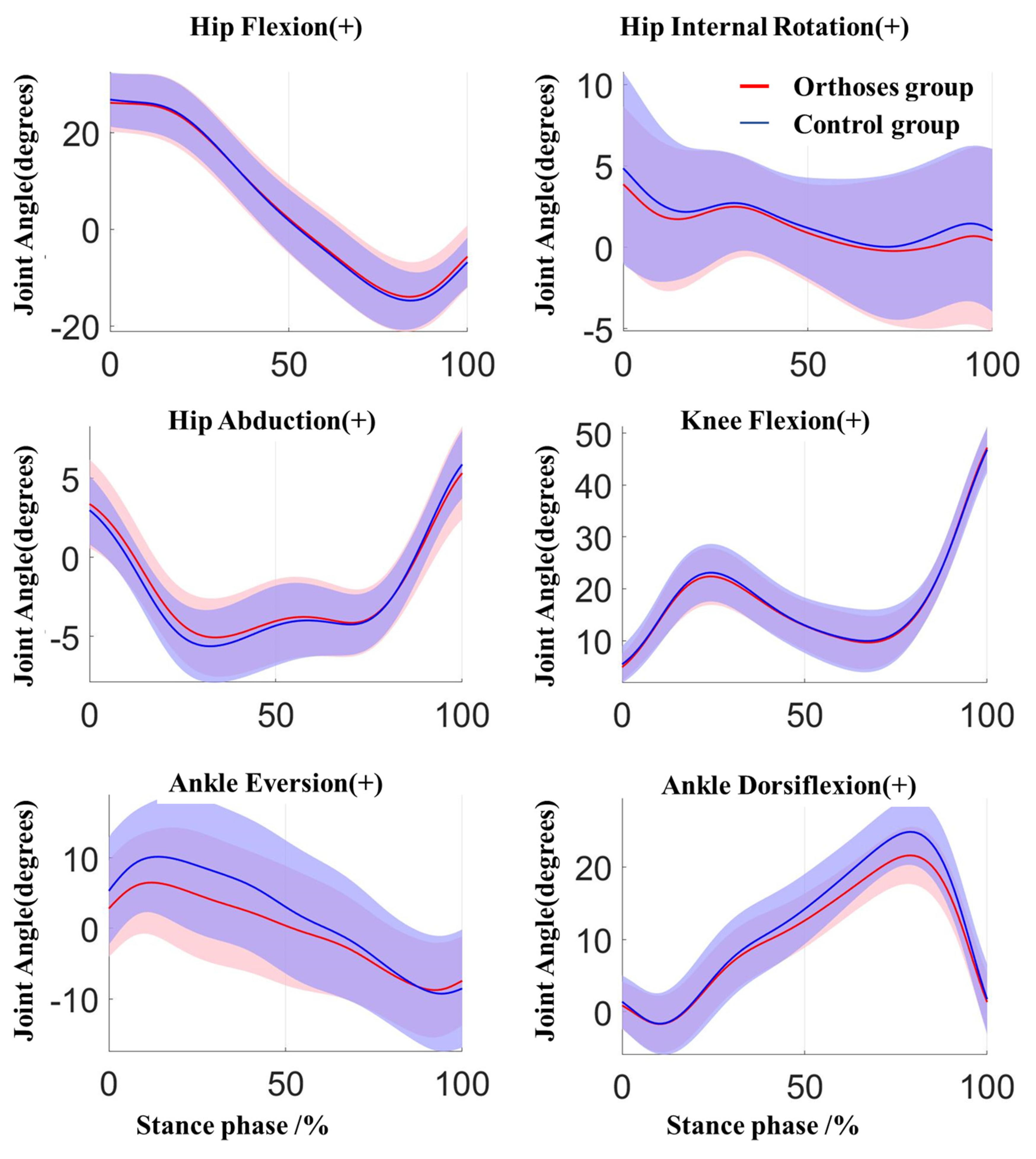
| Hip flexion | 26.827 (6.373) | 27.256 (5.948) | 0.443 | 0.204 (−0.736,1.593) |
| Hip extension | −14.222 (7.347) | −15.025 (5.884) | 0.257 | 0.305 (−2.263,0.656) |
| Hip abduction | 5.868 (2.796) | 6.095 (2.318) | 0.421 | 0.214 (−0.361,0.815) |
| Hip adduction | −5.563 (2.449) | −5.957 (2.355) | 0.072 | 0.502 (−0.828,0.041) |
| Hip external rotation | 5.181 (4.157) | 6.225 (4.622) | 0.145 | 0.398 (−0.407,2.494) |
| Hip internal rotation | −2.212 (4.909) | −2.309 (4.547) | 0.871 | 0.043 (−1.361,1.167) |
| Knee flexion | 47.687 (4.112) | 46.82 (4.539) | 0.223 | 0.329 (−2.326,0.592) |
| Ankle dorsiflexion | 22.848 (4.163) | 24.734 (4.576) | 0.002 1 | 1.015 (0.857,2.915) |
| Ankle plantarflexion | −2.514 (3.917) | −2.663 (4.612) | 0.81 | 0.063 (−1.454,1.155) |
| Ankle eversion | 7.06 (6.675) | 10.886 (6.764) | 0.001 1 | 1.468 (2.382,5.27) |
| Ankle inversion | −9.521 (6.931) | −9.734 (8.737) | 0.85 | 0.05 (−2.588,2.161) |
| Parameter | WSFO Mean (SD) | WS Mean (SD) | p−Value | ES (95% CI) | |
|---|---|---|---|---|---|
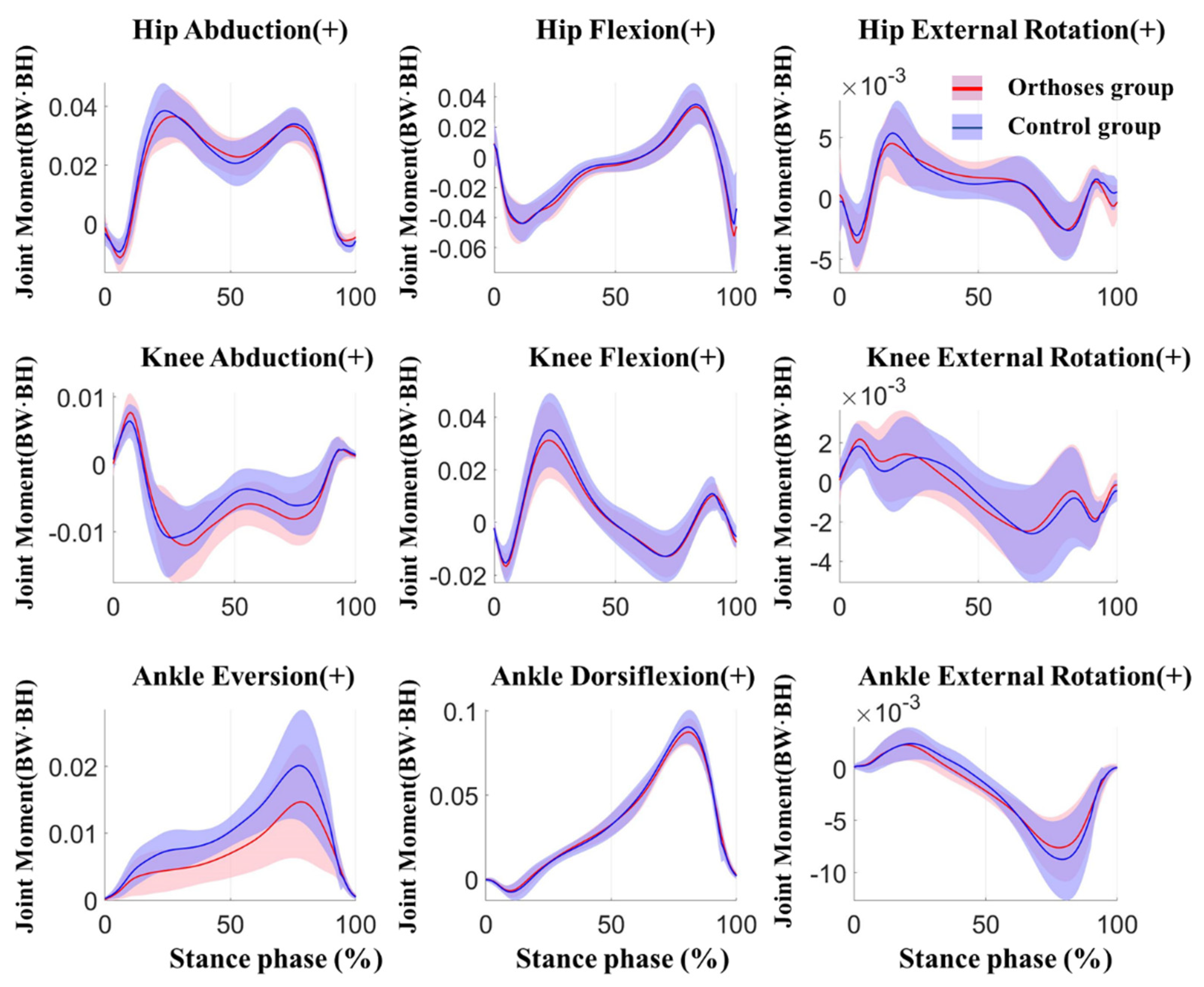
| Hip | First Abduction | −0.039 (0.01) | −0.041 (0.009) | 0.106 | 0.446 (−0.003,0) |
| Second Abduction | −0.034 (0.006) | −0.034 (0.006) | 0.193 | 0.353 (−0.001,0) | |
| External Rotation | 0.006 (0.003) | 0.005 (0.002) | 0.362 | 0.243 (−0.002,0.001) | |
| Internal Rotation | −0.006 (0.002) | −0.006 (0.002) | 0.357 | 0.246 (−0.001,0) | |
| Flexion Rotation | 0.061 (0.016) | 0.058 (0.017) | 0.443 | 0.204 (−0.013,0.006) | |
| Extension Rotation | −0.037 (0.007) | −0.039 (0.01) | 0.191 | 0.355 (−0.005,0.001) | |
| Knee | First Adduction | −0.015 (0.004) | −0.013 (0.004) | 0.007 1 | 0.822 (0,0.003) |
| Second Adduction | −0.009 (0.004) | −0.008 (0.003) | 0.016 1 | 0.707 (0,0.002) | |
| External Rotation | 0.003 (0.002) | 0.003 (0.001) | 0.592 | 0.142 (0,0) | |
| Internal Rotation | −0.003 (0.002) | −0.003 (0.002) | 0.224 | 0.329 (0,0) | |
| Flexion | 0.019 (0.006) | 0.019 (0.007) | 0.932 | 0.022 (−0.002,0.002) | |
| Extension | −0.032 (0.015) | −0.036 (0.015) | 0.18 | 0.364 (−0.009,0.002) | |
| Ankle | Eversion | 0.015 (0.008) | 0.021 (0.008) | 0.002 1 | 1.627 (0.003,0.007) |
| Inversion | 0.001 (0.001) | 0.002 (0.001) | 0.101 | 0.453 (0,0.001) | |
| External | 0.002 (0.001) | 0.003 (0.001) | 0.083 | 0.482 (0,0) | |
| Internal | −0.008 (0.003) | −0.009 (0.004) | 0.014 1 | 0.728 (−0.002,0) | |
| Dorsiflexion | 0.089 (0.008) | 0.091 (0.01) | 0.08 | 0.487 (0,0.005) | |
| Plantarflexion | −0.008 (0.004) | −0.009 (0.005) | 0.182 | 0.363 (−0.002,0.001) | |
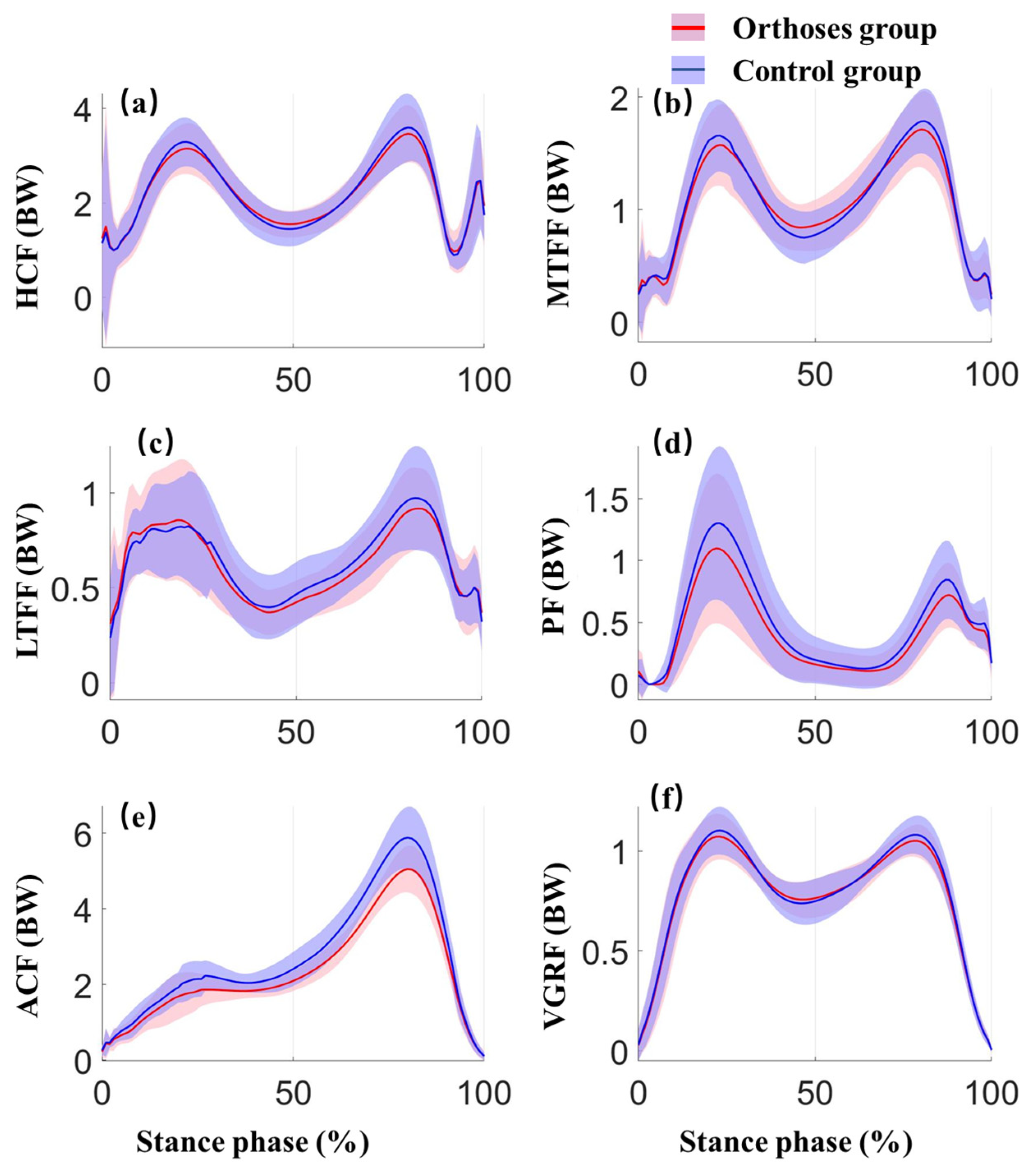
| Parameter | WSFO Mean (SD) | WS Mean (SD) | p−Value | ES (95% CI) | |
|---|---|---|---|---|---|
| Hip | First peak | 3.286 (0.502) | 3.355 (0.523) | 0.42 | 0.215 (−0.109,0.248) |
| Second peak | 3.562 (0.527) | 3.666 (0.675) | 0.201 | 0.347 (−0.062,0.269) | |
| Tibiofemoral joint | First medial peak | 1.617 (0.324) | 1.684 (0.356) | 0.249 | 0.31 (−0.052,0.185) |
| Second medial peak | 1.737 (0.318) | 1.81 (0.313) | 0.262 | 0.302 (−0.061,0.208) | |
| First lateral peak | 0.894 (0.292) | 0.927 (0.264) | 0.503 | 0.177 (−0.07,0.136) | |
| Second lateral peak | 0.904 (0.224) | 0.994 (0.291) | 0.095 | 0.462 (−0.018,0.199) | |
| Patellofemoral joint | First peak | 1.179 (0.63) | 1.324 (0.686) | 0.153 | 0.391 (−0.061,0.352) |
| Second peak | 0.78 (0.259) | 0.869 (0.334) | 0.022 1 | 0.663 (0.015,0.164) | |
| Ankle | Peak | 5.521 (0.627) | 5.925 (0.882) | 0.004 1 | 1.03 (0.187,0.621) |
| Ground force | First peak | 1.099 (0.127) | 1.113 (0.128) | 0.458 | 0.197 (−0.025,0.053) |
| Second peak | 1.066 (0.081) | 1.074 (0.08) | 0.238 | 0.318 (−0.006,0.023) | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peng, Y.; Wong, D.W.-C.; Wang, Y.; Chen, T.L.-W.; Tan, Q.; Chen, Z.; Jin, Z.; Zhang, M. Immediate Effects of Medially Posted Insoles on Lower Limb Joint Contact Forces in Adult Acquired Flatfoot: A Pilot Study. Int. J. Environ. Res. Public Health 2020, 17, 2226. https://doi.org/10.3390/ijerph17072226
Peng Y, Wong DW-C, Wang Y, Chen TL-W, Tan Q, Chen Z, Jin Z, Zhang M. Immediate Effects of Medially Posted Insoles on Lower Limb Joint Contact Forces in Adult Acquired Flatfoot: A Pilot Study. International Journal of Environmental Research and Public Health. 2020; 17(7):2226. https://doi.org/10.3390/ijerph17072226
Chicago/Turabian StylePeng, Yinghu, Duo Wai-Chi Wong, Yan Wang, Tony Lin-Wei Chen, Qitao Tan, Zhenxian Chen, Zhongmin Jin, and Ming Zhang. 2020. "Immediate Effects of Medially Posted Insoles on Lower Limb Joint Contact Forces in Adult Acquired Flatfoot: A Pilot Study" International Journal of Environmental Research and Public Health 17, no. 7: 2226. https://doi.org/10.3390/ijerph17072226