Associations between Family Weight-Based Teasing, Eating Pathology, and Psychosocial Functioning among Adolescent Military Dependents

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.2.1. Body Mass Index (BMI, kg/m2)
2.2.2. Disordered Eating Attitudes and Behaviors
2.2.3. Psychological Functioning
2.3. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Prevalence of Family Weight-Based Teasing
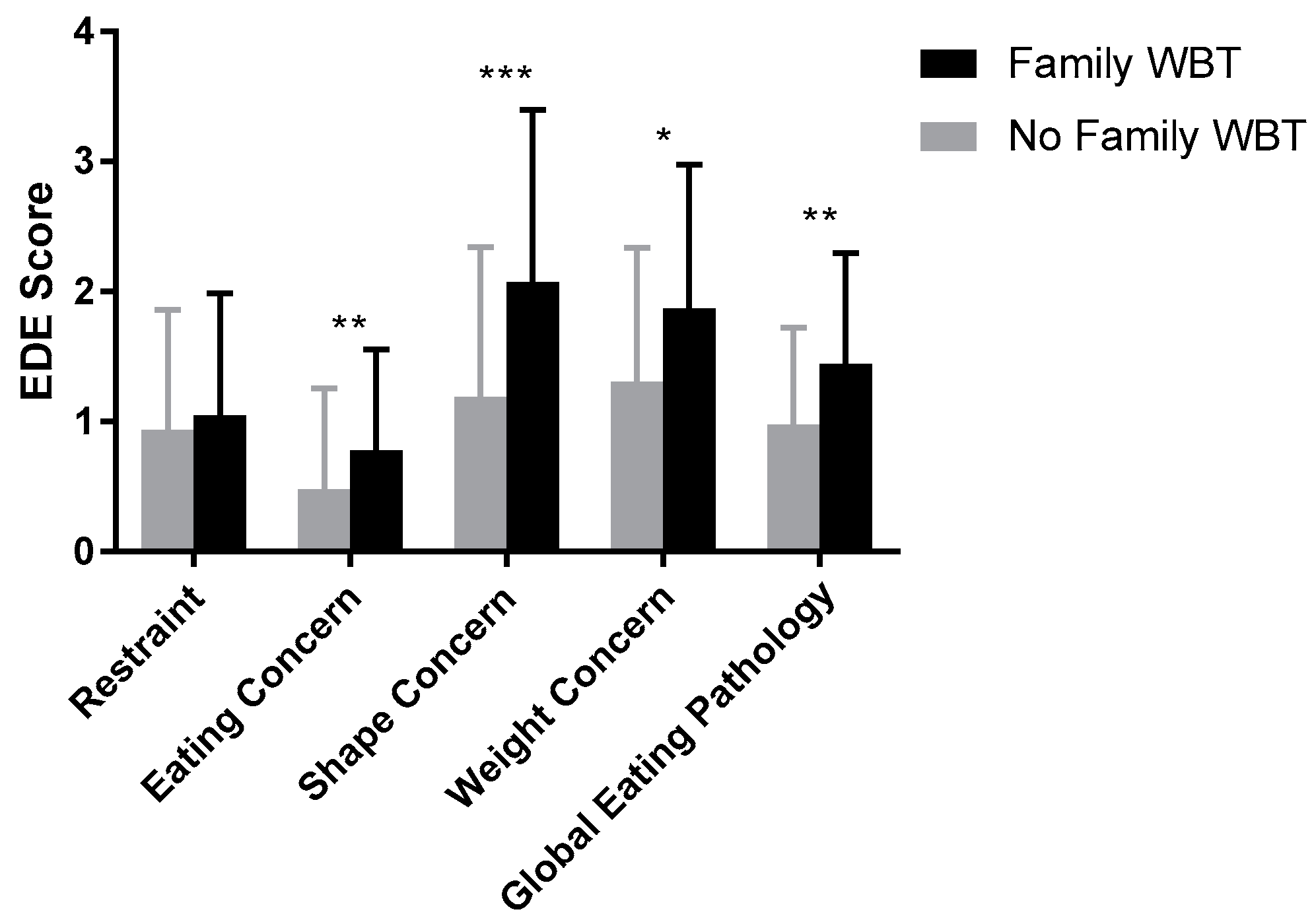
3.3. Associations of Family Weight-Based Teasing with Eating-Related Psychopathology
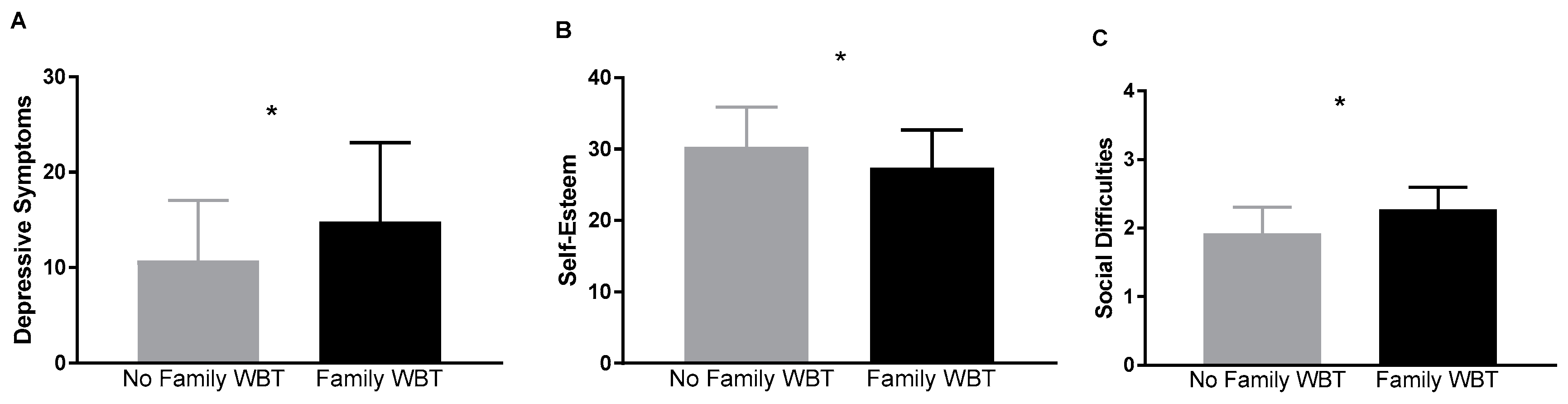
3.4. Associations of Family Weight-Based Teasing with Mood and Psychosocial Functioning
3.5. Exploratory Analyses of Parent- and Sibling-Specific Weight Based Teasing
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Disclaimer
References
- Spera, C. A Review of the Relationship among Parenting Practices, Parenting Styles, and Adolescent School Achievement. Educ. Psychol. Rev. 2005, 17, 125–146. [Google Scholar] [CrossRef] [Green Version]
- Steinberg, L.; Lamborn, S.D.; Dornbusch, S.M.; Darling, N. Impact of Parenting Practices on Adolescent Achievement: Authoritative Parenting, School Involvement, and Encouragement to Succeed. Child Dev. 1992, 63, 1266–1281. [Google Scholar] [CrossRef] [PubMed]
- Martínez, I.; Murgui, S.; García, O.F.; García, F. Parenting in the Digital Era: Protective and Risk Parenting Styles for Traditional Bullying and Cyberbullying Victimization. Comput. Hum. Behav. 2019, 90, 84–92. [Google Scholar] [CrossRef]
- Sears, R.R.; Maccoby, E.E.; Levin, H. Patterns of Child Rearing; Row, Peterson and Co.: New York, NY, USA, 1957. [Google Scholar]
- Garcia, F.; Serra, E.; Garcia, O.F.; Martinez, I.; Cruise, E. A Third Emerging Stage for the Current Digital Society? Optimal Parenting Styles in Spain, the United States, Germany, and Brazil. Int. J. Environ. Res. Public Health 2019, 16, 2333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calafat, A.; García, F.; Juan, M.; Becoña, E.; Fernández-Hermida, J.R. Which Parenting Style Is More Protective against Adolescent Substance Use? Evidence within the European Context. Drug. Alcohol. Depen. 2014, 138, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Schvey, N.A.; Marwitz, S.E.; Mi, S.J.; Galescu, O.A.; Broadney, M.M.; Young-Hyman, D.; Brady, S.M.; Reynolds, J.C.; Tanofsky-Kraff, M.; Yanovski, S.Z.; et al. Weight-Based Teasing is Associated with Gain in BMI and Fat Mass among Children and Adolescents At-Risk for Obesity: A Longitudinal Study. Pediatr. Obes. 2019, e12538. [Google Scholar] [CrossRef]
- Puhl, R.M.; Peterson, J.L.; Luedicke, J. Weight-Based Victimization: Bullying Experiences of Weight Loss Treatment-Seeking Youth. Pediatrics 2013, 131, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Puhl, R.M.; Latner, J.D. Stigma, Obesity, and the Health of the Nation’s Children. Psychol. Bull. 2007, 133, 557–580. [Google Scholar] [CrossRef] [Green Version]
- Puhl, R.M.; Luedicke, J.; Heuer, C. Weight-Based Victimization toward Overweight Adolescents: Observations and Reactions of Peers. J. Sch. Health 2011, 81, 696–703. [Google Scholar] [CrossRef]
- Puhl, R.M.; King, K.M. Weight Discrimination and Bullying. Best Pract. Res. Clin. Endocrinol. Metab. 2013, 27, 117–127. [Google Scholar] [CrossRef]
- Pearce, M.J.; Boergers, J.; Prinstein, M.J. Adolescent Obesity, Overt and Relational Peer Victimization, and Romantic Relationships. Obes. Res. 2002, 10, 386–393. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, L.J.; Wolke, D.; Page, A.S.; Horwood, J. Obesity and Bullying: Different Effects for Boys and Girls. Arch. Dis. Child. 2006, 91, 121–125. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, K.S.; Latner, J.D.; Puhl, R.M.; Vartanian, L.R.; Giles, C.; Griva, K.; Carter, A. The Relationship between Weight Stigma and Eating Behavior is Explained by Weight Bias Internalization and Psychological Distress. Appetite 2016, 102, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Haines, J.; Neumark-Sztainer, D.; Eisenberg, M.E.; Hannan, P.J. Weight Teasing and Disordered Eating Behaviors in Adolescents: Longitudinal Findings from Project Eat (Eating among Teens). Pediatrics 2006, 117, 209–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haines, J.; Neumark-Sztainer, D.; Wall, M.; Story, M. Personal, Behavioral, and Environmental Risk and Protective Factors for Adolescent Overweight. Obesity 2007, 15, 2748–2760. [Google Scholar] [CrossRef] [Green Version]
- Libbey, H.P.; Story, M.T.; Neumark-Sztainer, D.R.; Boutelle, K.N. Teasing, Disordered Eating Behaviors, and Psychological Morbidities among Overweight Adolescents. Obesity 2008, 16 (Suppl. 2), 24–29. [Google Scholar] [CrossRef]
- Puhl, R.; Suh, Y. Health Consequences of Weight Stigma: Implications for Obesity Prevention and Treatment. Curr. Obes. Rep. 2015, 4, 182–190. [Google Scholar] [CrossRef]
- Puhl, R.M.; Wall, M.M.; Chen, C.; Bryn Austin, S.; Eisenberg, M.E.; Neumark-Sztainer, D. Experiences of Weight Teasing in Adolescence and Weight-Related Outcomes in Adulthood: A 15-Year Longitudinal Study. Prev. Med. 2017, 100, 173–179. [Google Scholar] [CrossRef]
- Faith, M.S.; Leone, M.A.; Ayers, T.S.; Heo, M.; Pietrobelli, A. Weight Criticism During Physical Activity, Coping Skills, and Reported Physical Activity in Children. Pediatrics 2002, 110, e23. [Google Scholar] [CrossRef] [Green Version]
- Hayden-Wade, H.A.; Stein, R.I.; Ghaderi, A.; Saelens, B.E.; Zabinski, M.F.; Wilfley, D.E. Prevalence, Characteristics, and Correlates of Teasing Experiences among Overweight Children vs. Non-Overweight Peers. Obes. Res. 2005, 13, 1381–1392. [Google Scholar] [CrossRef] [Green Version]
- Storch, E.A.; Milsom, V.A.; Debraganza, N.; Lewin, A.B.; Geffken, G.R.; Silverstein, J.H. Peer Victimization, Psychosocial Adjustment, and Physical Activity in Overweight and At-Risk-for-Overweight Youth. J. Pediatric Psychol. 2007, 32, 80–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eisenberg, M.E.; Neumark-Sztainer, D.; Story, M. Associations of Weight-Based Teasing and Emotional Well-Being among Adolescents. Arch. Pediatric Adolesc. Med. 2003, 157, 733–738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puhl, R.M.; Luedicke, J. Weight-Based Victimization among Adolescents in the School Setting: Emotional Reactions and Coping Behaviors. J. Youth Adolesc. 2012, 41, 27–40. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, L.J.; Page, A.S. The Impact of Weight-Related Victimization on Peer Relationships: The Female Adolescent Perspective. Obesity 2008, 16 (Suppl. 2), 39–45. [Google Scholar] [CrossRef]
- Neumark-Sztainer, D.; Falkner, N.; Story, M.; Perry, C.; Hannan, P.J.; Mulert, S. Weight-Teasing among Adolescents: Correlations with Weight Status and Disordered Eating Behaviors. Int. J. Obes. Relat. Metab. Disord. 2002, 26, 123–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strauss, R.S.; Pollack, H.A. Social Marginalization of Overweight Children. Arch. Pediatric Adolesc. Med. 2003, 157, 746–752. [Google Scholar] [CrossRef]
- Krukowski, R.A.; West, D.S.; Philyaw Perez, A.; Bursac, Z.; Phillips, M.M.; Raczynski, J.M. Overweight Children, Weight-Based Teasing and Academic Performance. Int. J. Pediatric Obes. 2009, 4, 274–280. [Google Scholar] [CrossRef]
- Suelter, C.S.; Schvey, N.; Kelly, N.R.; Shanks, M.; Thompson, K.A.; Mehari, R.; Brady, S.; Yanovski, S.Z.; Melby, C.L.; Tanofsky-Kraff, M.; et al. Relationship of Pressure to Be Thin with Gains in Body Weight and Fat Mass in Adolescents. Pediatric Obes. 2018, 13, 14–22. [Google Scholar] [CrossRef] [Green Version]
- Gillison, F.B.; Lorenc, A.B.; Sleddens, E.F.; Williams, S.L.; Atkinson, L. Can It Be Harmful for Parents to Talk to Their Child About Their Weight? A Meta-Analysis. Prev. Med. 2016, 93, 135–146. [Google Scholar] [CrossRef] [Green Version]
- Berge, J.M.; Hanson-Bradley, C.; Tate, A.; Neumark-Sztainer, D. Do Parents or Siblings Engage in More Negative Weight-Based Talk with Children and What Does It Sound Like? A Mixed-Methods Study. Body Image 2016, 18, 27–33. [Google Scholar] [CrossRef] [Green Version]
- Schvey, N.A.; Shomaker, L.B.; Kelly, N.R.; Pickworth, C.K.; Cassidy, O.; Galescu, O.; Demidowich, A.P.; Brady, S.M.; Tanofsky-Kraff, M.; Yanovski, J.A. Pressure to Be Thin and Insulin Sensitivity among Adolescents. J. Adolesc. Health 2016, 58, 104–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davison, K.K.; Birch, L.L. Weight Status, Parent Reaction, and Self-Concept in Five-Year-Old Girls. Pediatrics 2001, 107, 46–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davison, K.K.; Birch, L.L. Predictors of Fat Stereotypes among 9-Year-Old Girls and Their Parents. Obes. Res. 2004, 12, 86–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puhl, R. Weight Stigmatization toward Youth: A Significant Problem in Need of Societal Solutions. Child Obes 2011, 7, 359–363. [Google Scholar] [CrossRef] [Green Version]
- Crandall, C.S. Do Heavy-Weight Students Have More Difficulty Paying for College? Pers. Soc. Psychol. B 1991, 17, 606–611. [Google Scholar] [CrossRef]
- Crandall, C.S. Do Parents Discriminate against Their Heavyweight Daughters? Pers. Soc. Psychol. B 1995, 21, 724–735. [Google Scholar] [CrossRef]
- Puhl, R.M.; Brownell, K.D. Confronting and Coping with Weight Stigma: An Investigation of Overweight and Obese Adults. Obesity 2006, 14, 1802–1815. [Google Scholar] [CrossRef]
- Schvey, N.; Barmine, M.; Bates, D.; Oldham, K.; Bakalar, J.; Spieker, E.; Maurer, D.; Stice, E.; Stephens, M.; Tanofsky-Kraff, M.; et al. Weight Stigma among Active Duty U.S. Military Personnel with Overweight and Obesity. Stigma Health 2017, 2, 281–291. [Google Scholar] [CrossRef]
- Armed Forces Health Surveillance. Diagnoses of Overweight/Obesity, Active Component, U.S. Armed Forces, 1998–2010. MSMR 2011, 18, 7–11. [Google Scholar]
- Bray, R.M.; Pemberton, M.R.; Hourani, L.L.; Witt, M.; Olmsted, K.L.; Brown, J.M.; Weimer, B.; Lance, M.E.; Marsden, M.E.; Scheffler, S. Department of Defense Survey of Health Related Behaviors among Active Duty Military Personnel; Research Triangle Inst (RTI): Research Triange Park, NC, USA, 2009. [Google Scholar]
- Agras, W.S.; Hammer, L.D.; McNicholas, F.; Kraemer, H.C. Risk Factors for Childhood Overweight: A Prospective Study from Birth to 9.5 Years. J. Pediatric 2004, 145, 20–25. [Google Scholar] [CrossRef]
- Department of Defense Education Activity. All About DODEA Educational Partnership. Available online: https://www.dodea.edu/Partnership/about.cfm (accessed on 20 June 2019).
- Schvey, N.A.; Sbrocco, T.; Stephens, M.; Bryant, E.J.; Ress, R.; Spieker, E.A.; Conforte, A.; Bakalar, J.L.; Pickworth, C.K.; Barmine, M.; et al. Comparison of Overweight and Obese Military-Dependent and Civilian Adolescent Girls with Loss-of-Control Eating. Int. J. Eat. Disord. 2015, 48, 790–794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chandra, A.; Lara-Cinisomo, S.; Jaycox, L.H.; Tanielian, T.; Burns, R.M.; Ruder, T.; Han, B. Children on the Homefront: The Experience of Children from Military Families. Pediatrics 2010, 125, 16–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gorman, G.H.; Eide, M.; Hisle-Gorman, E. Wartime Military Deployment and Increased Pediatric Mental and Behavioral Health Complaints. Pediatrics 2010, 126, 1058–1066. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hisle-Gorman, E.; Susi, A.; Gorman, G.H. Mental Health Trends in Military Pediatrics. Psychiatr. Serv. 2019. [Google Scholar] [CrossRef] [PubMed]
- Chartrand, M.M.; Frank, D.A.; White, L.F.; Shope, T.R. Effect of Parents’ Wartime Deployment on the Behavior of Young Children in Military Families. Arch. Pediatric Adol. Med. 2008, 162, 1009–1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neyland, M.H.; Shank, L.M.; Burke, N.L.; Schvey, N.A.; Pine, A.; Quattlebaum, M.; Tanofsky-Kraff, M. Parental deployment and distress, and adolescent disordered eating in prevention-seeking military dependents. Int. J. Eat Disord 2019. [Google Scholar] [CrossRef]
- Field, A.E.; Cook, N.R.; Gillman, M.W. Weight Status in Childhood as a Predictor of Becoming Overweight or Hypertensive in Early Adulthood. Obes. Res. 2005, 13, 163–169. [Google Scholar] [CrossRef] [Green Version]
- Tanofsky-Kraff, M.; Yanovski, S.Z.; Schvey, N.A.; Olsen, C.H.; Gustafson, J.; Yanovski, J.A. A Prospective Study of Loss of Control Eating for Body Weight Gain in Children at High Risk for Adult Obesity. Int. J. Eat. Disord. 2009, 42, 26–30. [Google Scholar] [CrossRef] [Green Version]
- Spielberger, C.; Gorsuch, R.; Lushene, R.; Vagg, P.; Jacobs, G. Manual for the State-Trait Anxiety Inventory; Consulting Psychologists Press: Palo Alto, CA, USA, 1983. [Google Scholar]
- Kuczmarski, R.J.; Ogden, C.L.; Guo, S.S.; Grummer-Strawn, L.M.; Flegal, K.M.; Mei, Z.; Wei, R.; Curtin, L.R.; Roche, A.F.; Johnson, C.L. 2000 CDC Growth Charts for the United States: Methods and Development. In Vital Health Statistics; DHHS Publication: Rockville, MD, USA, 2002; pp. 1–190. [Google Scholar]
- Fairburn, C.Z. The Eating Disorder Examination. In Binge Eating: Nature, Assessment and Treatment, 12th ed.; Fairburn, C.G., Wilson, G., Eds.; Guilford Press: New York, NY, USA, 1993. [Google Scholar]
- Tanofsky-Kraff, M.; Shomaker, L.B.; Wilfley, D.E.; Young, J.F.; Sbrocco, T.; Stephens, M.; Ranzenhofer, L.M.; Elliott, C.; Brady, S.; Radin, R.M.; et al. Targeted Prevention of Excess Weight Gain and Eating Disorders in High-Risk Adolescent Girls: A Randomized Controlled Trial. Am. J. Clin. Nutr. 2014, 100, 1010–1018. [Google Scholar] [CrossRef] [Green Version]
- Glasofer, D.R.; Tanofsky-Kraff, M.; Eddy, K.T.; Yanovski, S.Z.; Theim, K.R.; Mirch, M.C.; Ghorbani, S.; Ranzenhofer, L.M.; Haaga, D.; Yanovski, J.A. Binge Eating in Overweight Treatment-Seeking Adolescents. J. Pediatric Psychol. 2007, 32, 95–105. [Google Scholar] [CrossRef] [Green Version]
- Eisenberg, M.E.; Puhl, R.; Watson, R.J. Family Weight Teasing, LGBTQ Attitudes, and Well-Being among LGBTQ Adolescents. Fam. Community Health 2020, 43, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Muris, P.; Merckelbach, H.; Ollendick, T.; King, N.; Bogie, N. Three Traditional and Three New Childhood Anxiety Questionnaires: Their Reliability and Validity in a Normal Adolescent Sample. Behav. Res. Ther. 2002, 40, 753–772. [Google Scholar] [CrossRef] [Green Version]
- Beck, A.; Steer, R.; Brown, G. Manual for the Beck Depression Inventory-II; Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Reynolds, W.M.; Gould, J.W. A Psychometric Investigation of the Standard and Short Form Beck Depression Inventory. J. Consult. Clin. Psychol. 1981, 49, 306–307. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, M. Society and the Adolescent Self-Image; Princeton University Press: Princeton, MA, USA, 2015. [Google Scholar]
- Blascovich, J.; Tomaka, J. Measures of Personality and Social Psychological Attitudes. In Measures of Social Psychological Attitudes; Academic Press: San Diego, CA, USA, 1991; pp. 115–160. [Google Scholar]
- Weissman, M.M.; Bothwell, S. Assessment of Social Adjustment by Patient Self-Report. Arch. Gen. Psychiatry 1976, 33, 1111–1115. [Google Scholar] [CrossRef]
- Gameroff, M.J.; Wickramaratne, P.; Weissman, M.M. Testing the Short and Screener Versions of the Social Adjustment Scale-Self-Report (SAS-SR). Int. J. Methods Psychiatr. Res. 2012, 21, 52–65. [Google Scholar] [CrossRef] [PubMed]
- Osborne, J.W.; Overbay, A. The Power of Outliers (and Why Researchers Should Always Check for Them). Pract. Assess. Res. Eval. 2004, 9, 1–12. [Google Scholar]
- Moretti, M.M.; Peled, M. Adolescent-Parent Attachment: Bonds That Support Healthy Development. Paediatr. Child Health 2004, 9, 551–555. [Google Scholar] [CrossRef]
- Goldfield, G.; Moore, C.; Henderson, K.; Buchholz, A.; Obeid, N.; Flament, M. The Relation Between Weight-Based Teasing and Psychological Adjustment in Adolescents. Paediatr. Child Health 2010, 15, 283–288. [Google Scholar] [CrossRef] [Green Version]
- Fulkerson, J.A.; Strauss, J.; Neumark-Sztainer, D.; Story, M.; Boutelle, K. Correlates of Psychosocial Well-Being among Overweight Adolescents: The Role of the Family. J. Consult. Clin. Psychol. 2007, 75, 181–186. [Google Scholar] [CrossRef]
- McCormack, L.A.; Laska, M.N.; Gray, C.; Veblen-Mortenson, S.; Barr-Anderson, D.; Story, M. Weight-Related Teasing in a Racially Diverse Sample of Sixth-Grade Children. J. Am. Diet. Assoc. 2011, 111, 431–436. [Google Scholar] [CrossRef]
- Neumark-Sztainer, D.; Bauer, K.W.; Friend, S.; Hannan, P.J.; Story, M.; Berge, J.M. Family Weight Talk and Dieting: How Much Do They Matter for Body Dissatisfaction and Disordered Eating Behaviors in Adolescent Girls? J. Adolesc. Health 2010, 47, 270–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quick, V.; Wall, M.; Larson, N.; Haines, J.; Neumark-Sztainer, D. Personal, Behavioral and Socio-Environmental Predictors of Overweight Incidence in Young Adults: 10-Yr Longitudinal Findings. Int. J. Behav. Nutr. Phys. 2013, 10, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hunger, J.M.; Tomiyama, A.J. Weight Labeling and Obesity: A Longitudinal Study of Girls Aged 10 to 19 Years. JAMA Pediatric 2014, 168, 579–580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenleaf, C.; Petrie, T.A.; Martin, S.B. Relationship of Weight-Based Teasing and Adolescents’ Psychological Well-Being and Physical Health. J. Sch. Health 2014, 84, 49–55. [Google Scholar] [CrossRef]
- Cerniglia, L.; Cimino, S.; Tafà, M.; Marzilli, E.; Ballarotto, G.; Bracaglia, F. Family Profiles in Eating Disorders: Family Functioning and Psychopathology. Psychol. Res. Behav. Manag. 2017, 10, 305. [Google Scholar] [CrossRef] [Green Version]
- Tafà, M.; Cimino, S.; Ballarotto, G.; Bracaglia, F.; Bottone, C.; Cerniglia, L. Female Adolescents with Eating Disorders, Parental Psychopathological Risk and Family Functioning. J. Child Fam. Stud. 2017, 26, 28–39. [Google Scholar] [CrossRef]
- Callahan, D. Obesity: Chasing an Elusive Epidemic. Hastings Cent. Rep. 2013, 43, 34–40. [Google Scholar] [CrossRef]
- Bohrer, B.K.; Forbush, K.T.; Hunt, T.K. Are Common Measures of Dietary Restraint and Disinhibited Eating Reliable and Valid in Obese Persons? Appetite 2015, 87, 344–351. [Google Scholar] [CrossRef]
- Hunger, J.M.; Major, B.; Blodorn, A.; Miller, C.T. Weighed Down by Stigma: How Weight-Based Social Identity Threat Contributes to Weight Gain and Poor Health. Soc. Personal. Psychol. Compass 2015, 9, 255–268. [Google Scholar] [CrossRef] [Green Version]
- Bennett, D.A.; Cooper, C.L. Eating Disturbance as a Manifestation of the Stress Process: A Review of the Literature. Stress Med. 1999, 15, 167–182. [Google Scholar] [CrossRef]
- Gluck, M.E. Stress Response and Binge Eating Disorder. Appetite 2006, 46, 26–30. [Google Scholar] [CrossRef]
- Trautwein, U.; Lüdtke, O.; Köller, O.; Baumert, J. Self-Esteem, Academic Self-Concept, and Achievement: How the Learning Environment Moderates the Dynamics of Self-Concept. J. Pers. Soc. Psychol. 2006, 90, 334. [Google Scholar] [CrossRef]
- Berge, J.M.; Trofholz, A.; Fong, S.; Blue, L.; Neumark-Sztainer, D. A Qualitative Analysis of Parents’ Perceptions of Weight Talk and Weight Teasing in the Home Environments of Diverse Low-Income Children. Body Image 2015, 15, 8–15. [Google Scholar] [CrossRef] [Green Version]
- Bauer, K.W.; Bucchianeri, M.M.; Neumark-Sztainer, D. Mother-Reported Parental Weight Talk and Adolescent Girls’ Emotional Health, Weight Control Attempts, and Disordered Eating Behaviors. J. Eat. Disord. 2013, 1, 45. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Family WBT: Presence (n = 61) | Family WBT: Absence (n = 67) | Total Sample (n = 128) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| % | N | % | N | ᵡ2 | % | N | ||||
| Sex | 1.2 | |||||||||
| Female | 59 | 36 | 49.3 | 33 | 53.9 | 69 | ||||
| Male | 41 | 25 | 50.7 | 34 | 46.1 | 59 | ||||
| Race | 6.7 | |||||||||
| Black | 19.7 | 12 | 26.9 | 18 | 23.4 | 30 | ||||
| White | 45.9 | 28 | 56.7 | 38 | 51.6 | 66 | ||||
| Asian | 4.9 | 3 | 1.5 | 1 | 3.1 | 4 | ||||
| Multiple | 14.8 | 9 | 10.4 | 7 | 12.5 | 16 | ||||
| Other | 14.8 | 9 | 4.5 | 3 | 9.4 | 12 | ||||
| Ethnicity | 0.86 | |||||||||
| Hispanic | 23 | 14 | 17.9 | 12 | 20.3 | 26 | ||||
| Weight Status + | 3.1 | |||||||||
| With Overweight | 29.5 | 18 | 16.4 | 11 | 22.7 | 29 | ||||
| With Obesity | 70.5 | 43 | 83.6 | 56 | 77.3 | 99 | ||||
| Reported Loss of Control in Past Month | 54.1 | 33 | 41.8 | 28 | 1.9 | 47.7 | 61 | |||
| Presence of Elevated Anxiety | 93.4 | 57 | 92.5 | 62 | 0.04 | 93.0 | 119 | |||
| M | SD | N | M | SD | N | F | M | SD | N | |
| Age (y) | 14.5 | 1.6 | 61 | 14.2 | 1.5 | 67 | 0.98 | 14.4 | 1.5 | 128 |
| BMIz | 1.9 | 0.41 | 61 | 1.9 | 0.37 | 67 | 1.6 | 1.9 | 0.39 | 128 |
| EDE Restraint Subscale | 1.1 | 0.97 | 61 | 0.94 | 0.92 | 67 | 1.1 | 1.0 | 0.95 | 128 |
| EDE Eating Concern Subscale | 0.77 | 0.71 | 61 | 0.46 | 0.69 | 67 | 5.0 * | 0.61 | 0.72 | 128 |
| EDE Shape Concern Subscale | 2.0 | 1.3 | 61 | 1.2 | 1.2 | 67 | 13.8 *** | 1.6 | 1.3 | 128 |
| EDE Weight Concern Subscale | 1.9 | 1.1 | 61 | 1.3 | 1.0 | 67 | 8.8 ** | 1.6 | 1.1 | 128 |
| EDE Global Score | 1.4 | 8.2 | 61 | 0.98 | 0.74 | 67 | 10.9 ** | 1.2 | 0.81 | 128 |
| Depressive Symptoms | 14.6 | 8.0 | 61 | 10.7 | 6.3 | 67 | 9.4 ** | 12.6 | 7.4 | 128 |
| Self-Esteem | 27.6 | 5.4 | 60 | 30.3 | 5.6 | 67 | 7.6 ** | 29.0 | 5.6 | 127 |
| Social Difficulties | 2.1 | 0.39 | 59 | 1.9 | 0.39 | 66 | 9.9 ** | 2.0 | 0.40 | 125 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pearlman, A.T.; Schvey, N.A.; Higgins Neyland, M.K.; Solomon, S.; Hennigan, K.; Schindler, R.; Leu, W.; Gillmore, D.; Shank, L.M.; Lavender, J.M.; et al. Associations between Family Weight-Based Teasing, Eating Pathology, and Psychosocial Functioning among Adolescent Military Dependents. Int. J. Environ. Res. Public Health 2020, 17, 24. https://doi.org/10.3390/ijerph17010024
Pearlman AT, Schvey NA, Higgins Neyland MK, Solomon S, Hennigan K, Schindler R, Leu W, Gillmore D, Shank LM, Lavender JM, et al. Associations between Family Weight-Based Teasing, Eating Pathology, and Psychosocial Functioning among Adolescent Military Dependents. International Journal of Environmental Research and Public Health. 2020; 17(1):24. https://doi.org/10.3390/ijerph17010024
Chicago/Turabian StylePearlman, Arielle T., Natasha A. Schvey, M. K. Higgins Neyland, Senait Solomon, Kathrin Hennigan, Rachel Schindler, William Leu, Dakota Gillmore, Lisa M. Shank, Jason M. Lavender, and et al. 2020. "Associations between Family Weight-Based Teasing, Eating Pathology, and Psychosocial Functioning among Adolescent Military Dependents" International Journal of Environmental Research and Public Health 17, no. 1: 24. https://doi.org/10.3390/ijerph17010024