Sleep Difficulties in Preschoolers with Psychiatric Diagnoses

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Psychiatric Diagnosis
2.3. Sleep
2.4. Data Analyses
3. Results
3.1. Descriptive Data
3.2. The Proportion of Sleep Problems in Preschoolers with Psychiatric Disorders and the Association between Parental-Reported Sleep Problems and Diagnostic Categories
3.3. Association between Specific Sleep Problems and Diagnostic Categories
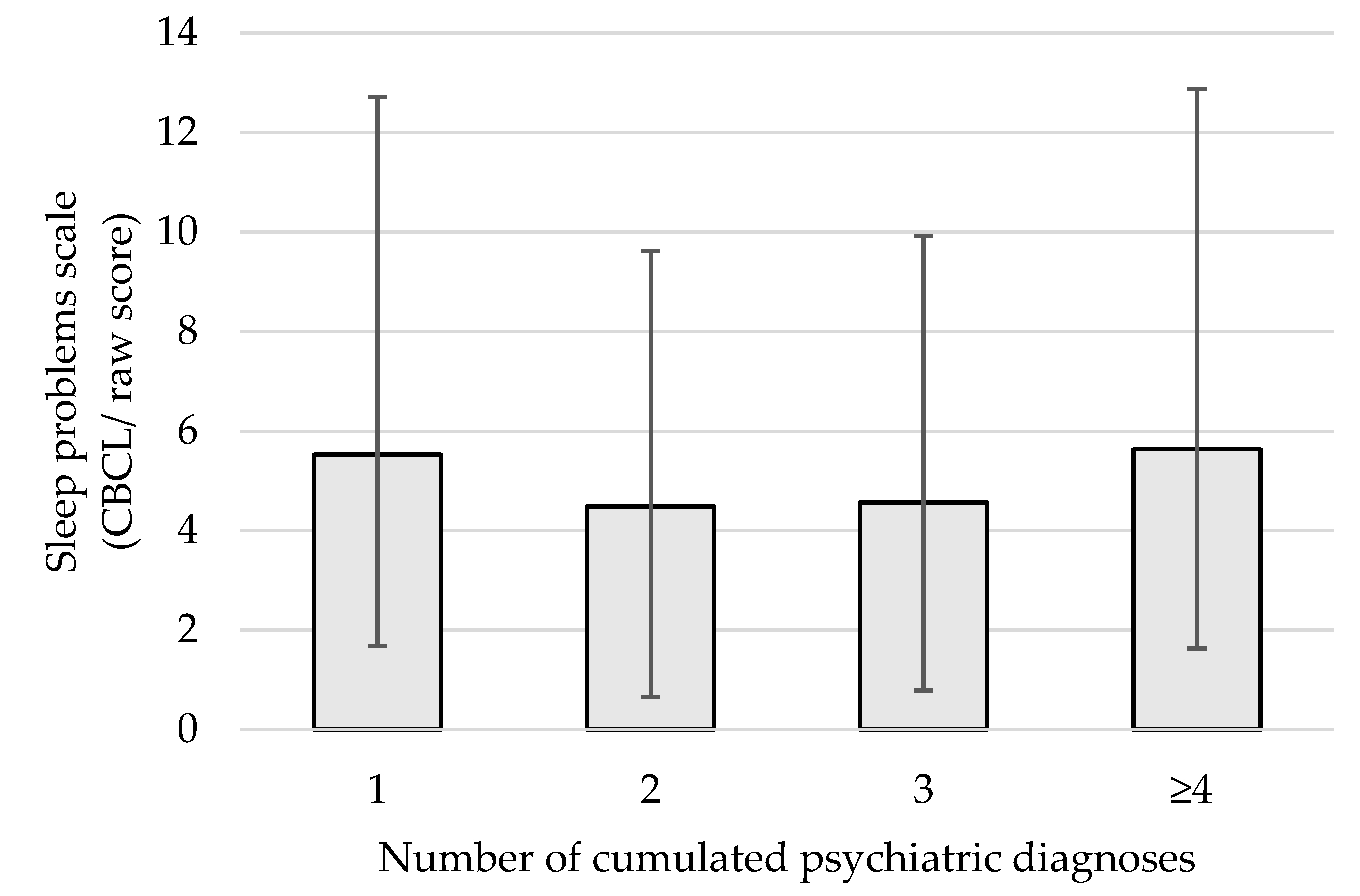
3.4. Effect of Cumulating Positive Diagnostic Categories on Sleep Difficulties
4. Discussion
4.1. The Proportion of Sleep Problems in Preschoolers with Psychiatric Disorders
4.2. Sleep Problems and Behavioral Disorders
4.3. Sleep Problems and Relational Disorders and Psychosocial Problems
4.4. Sleep Problems and Developmental Coordination Disorder
4.5. Sleep Problems and Communication Disorders
4.6. Effect of Cumulating Positive Diagnostic Categories on Sleep Difficulties
4.7. Limitations and Future Research
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hiscock, H.; Canterford, L.; Ukoumunne, O.C.; Wake, M. Adverse associations of sleep problems in Australian preschoolers: national population study. Pediatrics 2007, 119, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Aronen, E.T.; Paavonen, E.J.; Fjällberg, M.; Soininen, M.; Törrönen, J. Sleep and psychiatric symptoms in school-age children. J. Am. Acad. Child Adolesc. Psychiatry 2000, 39, 502–508. [Google Scholar] [CrossRef]
- Gregory, A.M.; Sadeh, A. Sleep, emotional and behavioral difficulties in children and adolescents. Sleep Med. Rev. 2012, 16, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Fallone, G.; Owens, J.A.; Deane, J. Sleepiness in children and adolescents: Clinical implications. Sleep Med. Rev. 2002, 6, 287–306. [Google Scholar] [CrossRef] [PubMed]
- Alfano, C.A.; Zakem, A.H.; Costa, N.M.; Taylor, L.K.; Weems, C.F. Sleep problems and their relation to cognitive factors, anxiety, and depressive symptoms in children and adolescents. Depress. Anxiety 2008. [Google Scholar] [CrossRef]
- Wilhelm, I.; Metzkow-Mészàros, M.; Knapp, S.; Born, J. Sleep-dependent consolidation of procedural motor memories in children and adults: The pre-sleep level of performance matters. Dev. Sci. 2012, 15, 506–515. [Google Scholar] [CrossRef]
- Randazzo, A.C.; Muehlbach, M.J.; Schweitzer, P.K.; Waish, J.K. Cognitive function following acute sleep restriction in children ages 10–14. Sleep 1998, 21, 861–868. [Google Scholar]
- Sivertsen, B.; Harvey, A.G.; Reichborn-Kjennerud, T.; Torgersen, L.; Ystrom, E.; Hysing, M. Later Emotional and Behavioral Problems Associated with Sleep Problems in Toddlers. JAMA Pediatr. 2015, 169, 575. [Google Scholar] [CrossRef]
- Owens, J. Classification and Epidemiology of Childhood Sleep Disorders. Prim. Care Clin. Off. Pract. 2008, 35, 533–546. [Google Scholar] [CrossRef]
- Byars, K.C.; Yolton, K.; Rausch, J.; Lanphear, B.; Beebe, D.W. Prevalence, patterns, and persistence of sleep problems in the first 3 years of life. Pediatrics 2012, 129, e276–e284. [Google Scholar] [CrossRef]
- Steinsbekk, S.; Berg-Nielsen, T.S.; Wichstrøm, L. Sleep disorders in preschoolers: Prevalence and comorbidity with psychiatric symptoms. J. Dev. Behav. Pediatr. 2013, 34, 633–641. [Google Scholar] [CrossRef] [PubMed]
- Lozoff, B.; Wolf, A.W.; Davis, N.S. Sleep problems seen in pediatric practice. Pediatrics 1985, 75, 477–483. [Google Scholar] [PubMed]
- Mindell, J.A.; Kuhn, B.; Lewin, D.S.; Meltzer, L.J.; Sadeh, A. Behavioral Treatment of Bedtime Problems and Night Wakings in Infants and Young Children. Sleep 2006, 29, 1263–1276. [Google Scholar] [CrossRef] [PubMed]
- Amintehran, E.; Ghalehbaghi, B.; Asghari, A.; Jalilolghadr, S.; Ahmadvand, A.; Foroughi, F. High prevalence of sleep problems in school-and preschool-aged children in Tehran: a population based study. Iran. J. Pediatr. 2013, 23, 45. [Google Scholar]
- Bufferd, S.J.; Dougherty, L.R.; Carlson, G.A.; Klein, D.N. Parent-reported mental health in preschoolers: Findings using a diagnostic interview. Compr. Psychiatry 2011, 52, 359–369. [Google Scholar] [CrossRef] [PubMed]
- Wichstrøm, L.; Berg-Nielsen, T.S.; Angold, A.; Egger, H.L.; Solheim, E.; Sveen, T.H. Prevalence of psychiatric disorders in preschoolers. J. Child Psychol. Psychiatry 2012, 53, 695–705. [Google Scholar] [CrossRef] [PubMed]
- Egger, H.L.; Angold, A. Common emotional and behavioral disorders in preschool children: Presentation, nosology, and epidemiology. J. Child Psychol. Psychiatry 2006, 47, 313–337. [Google Scholar] [CrossRef]
- Bufferd, S.J.; Dougherty, L.R.; Carlson, G.A.; Rose, S.; Klein, D.N. Psychiatric disorders in preschoolers: Continuity from ages 3 to 6. Am. J. Psychiatry 2012, 169, 1157–1164. [Google Scholar] [CrossRef]
- Boekamp, J.R.; Williamson, L.R.; Martin, S.E.; Hunter, H.L.; Anders, T.F. Sleep onset and night waking insomnias in preschoolers with psychiatric disorders. Child Psychiatry Hum. Dev. 2015, 46, 622–631. [Google Scholar] [CrossRef]
- Goodlin-Jones, B.L.; Tang, K.; Liu, J.; Anders, T.F. Sleep patterns in preschool-age children with autism, developmental delay, and typical development. J. Am. Acad. Child Adolesc. Psychiatry 2008, 47, 930–938. [Google Scholar] [CrossRef]
- O’Hare, A. Communication disorders in preschool children. Paediatr. Child Health 2017, 27, 447–453. [Google Scholar] [CrossRef]
- Harris, S.R.; Mickelson, E.C.; Zwicker, J.G. Diagnosis and management of developmental coordination disorder. CMAJ 2015, 187, 659–665. [Google Scholar] [CrossRef] [PubMed]
- Werner, H.; Hunkeler, P.; Benz, C.; Molinari, L.; Huber, R.; Jenni, O.G. Valid methods for estimating children’s sleep problems in clinical practice. Acta Paediatr. 2014, 103, e555–e557. [Google Scholar] [CrossRef] [PubMed]
- Gregory, A.M.; Cousins, J.C.; Forbes, E.E.; Trubnick, L.; Ryan, N.D.; Axelson, D.A.; Birmaher, B.; Sadeh, A.; Dahl, R.E. Sleep Items in the Child Behavior Checklist: A Comparison with Sleep Diaries, Actigraphy, and Polysomnography. J. Am. Acad. Child Adolesc. Psychiatry 2011, 50, 499–507. [Google Scholar] [CrossRef]
- Hudziak, J.J.; Achenbach, T.M.; Althoff, R.R.; Pine, D.S. A dimensional approach to developmental psychopathology. Int. J. Methods Psychiatr. Res. 2007, 16, S16–S23. [Google Scholar] [CrossRef]
- El-Sheikh, M.; Bagley, E.J.; Keiley, M.; Elmore-Staton, L.; Chen, E.; Buckhalt, J.A. Economic adversity and children’s sleep problems: Multiple indicators and moderation of effects. Health Psychol. 2013, 32, 849. [Google Scholar] [CrossRef]
- Bøe, T.; Øverland, S.; Lundervold, A.J.; Hysing, M. Socioeconomic status and children’s mental health: Results from the Bergen Child Study. Soc. Psychiatry Psychiatr. Epidemiol. 2012, 47, 1557–1566. [Google Scholar] [CrossRef]
- Bagley, E.J.; Kelly, R.J.; Buckhalt, J.A.; El-Sheikh, M. What keeps low-SES children from sleeping well: The role of presleep worries and sleep environment. Sleep Med. 2015, 16, 496–502. [Google Scholar] [CrossRef]
- Achenbach, T.M.; Rescorla, L.A. Manual for the ASEBA Preschool Forms & Profiles: An Integrated System of Multi-Informant Assessment; Child Behavior Checklist for Ages 1 1/2-5; Language Development Survey; Caregiver-Teacher Report form Rescorla; University of Vermont: Burlington, VT, USA, 2000. [Google Scholar]
- Achenbach, T.M.; Rescorla, L.A. Manual for the ASEBA Preschool Forms and Profiles; Burlington: Burlington, NJ, USA, 2010. [Google Scholar]
- Achenbach, T.M.; Edelbrock, C.; Howell, C.T. Empirically based assessment of the behavioral/emotional problems of 2-and 3-year-old children. J. Abnorm. Child Psychol. 1987, 15, 629–650. [Google Scholar] [CrossRef]
- Shanahan, L.; Copeland, W.E.; Angold, A.; Bondy, C.L.; Costello, E.J. Sleep Problems Predict and Are Predicted by Generalized Anxiety/Depression and Oppositional Defiant Disorder. J. Am. Acad. Child Adolesc. Psychiatry 2014, 53, 550–558. [Google Scholar] [CrossRef]
- Bates, J.E.; Viken, R.J.; Alexander, D.B.; Beyers, J.; Stockton, L. Sleep and Adjustment in Preschool Children: Sleep Diary Reports by Mothers Relate to Behavior Reports by Teachers. Child Dev. 2002, 73, 62–75. [Google Scholar] [CrossRef] [PubMed]
- Aronen, E.T.; Lampenius, T.; Fontell, T.; Simola, P. Sleep in Children with Disruptive Behavioral Disorders. Behav. Sleep Med. 2014, 12, 373–388. [Google Scholar] [CrossRef] [PubMed]
- Kay, J.; Tasman, A. Relational Problems. In Essentials of Psychiatry; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2006; pp. 838–842. [Google Scholar]
- Reid, M.J.; Walter, A.L.; O’Leary, S.G. Treatment of Young Children’s Bedtime Refusal and Nighttime Wakings: A Comparison of “Standard” and Graduated Ignoring Procedures. J. Abnorm. Child Psychol. 1999, 27, 5–16. [Google Scholar] [CrossRef] [PubMed]
- Pennestri, M.-H.; Moss, E.; O’Donnell, K.; Lecompte, V.; Bouvette-Turcot, A.-A.; Atkinson, L.; Minde, K.; Gruber, R.; Fleming, A.S.; Meaney, M.J.; et al. Establishment and consolidation of the sleep-wake cycle as a function of attachment pattern. Attach. Hum. Dev. 2015, 17, 23–42. [Google Scholar] [CrossRef]
- Wiggs, L.; Sparrowhawk, M.; Barnett, A.L. Parent Report and Actigraphically Defined Sleep in Children with and without Developmental Coordination Disorder; Links with Fatigue and Sleepiness. Front. Pediatr. 2016, 4, 81. [Google Scholar] [CrossRef] [Green Version]
- Carson, D.K.; Klee, T.; Perry, C.K.; Muskina, G.; Donaghy, T. Comparisons of children with delayed and normal language at 24 months of age on measures of behavioral difficulties, social and cognitive development. Infant Ment. Health J. 1998, 19, 59–75. [Google Scholar] [CrossRef]
- Quach, J.; Hiscock, H.; Canterford, L.; Wake, M. Outcomes of child sleep problems over the school-transition period: Australian population longitudinal study. Pediatrics 2009, 123, 1287–1292. [Google Scholar] [CrossRef]
- Parry-Fielder, B.; Collins, K.; Fisher, J.; Keir, E.; Anderson, V.; Jacobs, R.; Scheffer, I.E.; Nolan, T. Electroencephalographic abnormalities during sleep in children with developmental speech-language disorders: A case–control study. Dev. Med. Child Neurol. 2009, 51, 228–234. [Google Scholar] [CrossRef]
- Botting, N.; Baraka, N. Sleep behaviour relates to language skills in children with and without communication disorders. Int. J. Dev. Disabil. 2017, 1–6. [Google Scholar] [CrossRef]
- Becker, S.P.; Ramsey, R.R.; Byars, K.C. Convergent validity of the Child Behavior Checklist sleep items with validated sleep measures and sleep disorder diagnoses in children and adolescents referred to a sleep disorders center. Sleep Med. 2015, 16, 79–86. [Google Scholar] [CrossRef]
- Coskun, M.; Ilyas, K. Prevalence and Patterns of Psychiatric Disorders in Preschool Children Referred to an Outpatient Psychiatry Clinic/Psikiyatri Kliniğine Başvuran Okulöncesi Çocuklarda Psikiyatrik Bozuklukların Yaygınlığı ve Örüntüleri. Anadolu Klin. Tıp Bilimleri Derg. 2016, 21, 42–47. [Google Scholar]
- Basgül, S.S.; Etiler, N.; Çakin-Memik, N.; Coskun, A.; Agaoglu, B. Frequency and correlates of psychiatric disorders in early childhood: A study of population and clinical samples in Turkey. Turk. J. Pediatr. 2011, 53, 666. [Google Scholar] [PubMed]
- Kirby, A.; Sugden, D.A. Children with developmental coordination disorders. J. R. Soc. Med. 2007, 100, 182–186. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Age (months) N % | N | % |
|---|---|---|
| <18 months | 4 | 1.8 |
| 18 to <24 | 5 | 2.2 |
| 24 to <36 | 32 | 14.0 |
| 36 to <48 | 70 | 30.7 |
| 48 to <60 | 65 | 28.5 |
| 60 to <72 | 52 | 22.8 |
| Sex | ||
| Boys | 169 | 74.1 |
| Girls | 59 | 25.9 |
| Number of Categories with Positive Diagnoses | ||
| 1 | 23 | 10.1 |
| 2 | 119 | 52.2 |
| 3 | 62 | 27.2 |
| 4 | 24 | 10.5 |
| Post-Secondary Education | ||
| Mothers | 127 | 55.7 |
| Family Composition | ||
| Biological family | 155 | 68.6 |
| Diagnostic Categories | B | 95% CI | Beta | p-Value |
|---|---|---|---|---|
| Behavioral disorders | 1.08 | (0.13, 2.04) | 0.15 | 0.04 |
| Relational disorders | 0.62 | (−0.48, 1.71) | 0.09 | 0.27 |
| Developmental coordination disorder (DCD) | −2.35 | (−4.01, −0.69) | −0.29 | 0.01 |
| Communication disorders | 1.74 | (0.02, 3.46) | 0.21 | 0.05 |
| Diagnostic Categories | Has Trouble Falling Asleep | Wakes Often at Night | Talks or Cries in Sleep | |||
|---|---|---|---|---|---|---|
| X2(2) | p | X2(2) | p | X2(2) | p | |
| Behavioral disorders | 6.48 | 0.04 | 1.46 | 0.48 | 5.13 | 0.08 |
| Relational disorders | 1.16 | 0.56 | 0.20 | 0.90 | 3.39 | 0.18 |
| Developmental coordination disorder (DCD) | 8.76 | 0.01 | 7.65 | 0.02 | 3.92 | 0.14 |
| Communication disorders | 2.33 | 0.31 | 6.36 | 0.04 | 2.80 | 0.25 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chénier-Leduc, G.; Béliveau, M.-J.; Dubois-Comtois, K.; Butler, B.; Berthiaume, C.; Pennestri, M.-H. Sleep Difficulties in Preschoolers with Psychiatric Diagnoses. Int. J. Environ. Res. Public Health 2019, 16, 4485. https://doi.org/10.3390/ijerph16224485
Chénier-Leduc G, Béliveau M-J, Dubois-Comtois K, Butler B, Berthiaume C, Pennestri M-H. Sleep Difficulties in Preschoolers with Psychiatric Diagnoses. International Journal of Environmental Research and Public Health. 2019; 16(22):4485. https://doi.org/10.3390/ijerph16224485
Chicago/Turabian StyleChénier-Leduc, Gabrielle, Marie-Julie Béliveau, Karine Dubois-Comtois, Bryan Butler, Claude Berthiaume, and Marie-Hélène Pennestri. 2019. "Sleep Difficulties in Preschoolers with Psychiatric Diagnoses" International Journal of Environmental Research and Public Health 16, no. 22: 4485. https://doi.org/10.3390/ijerph16224485