Hyperhidrosis, Endoscopic Thoracic Sympathectomy, and Cardiovascular Outcomes: A Cohort Study Based on the Korean Health Insurance Review and Assessment Service Database

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
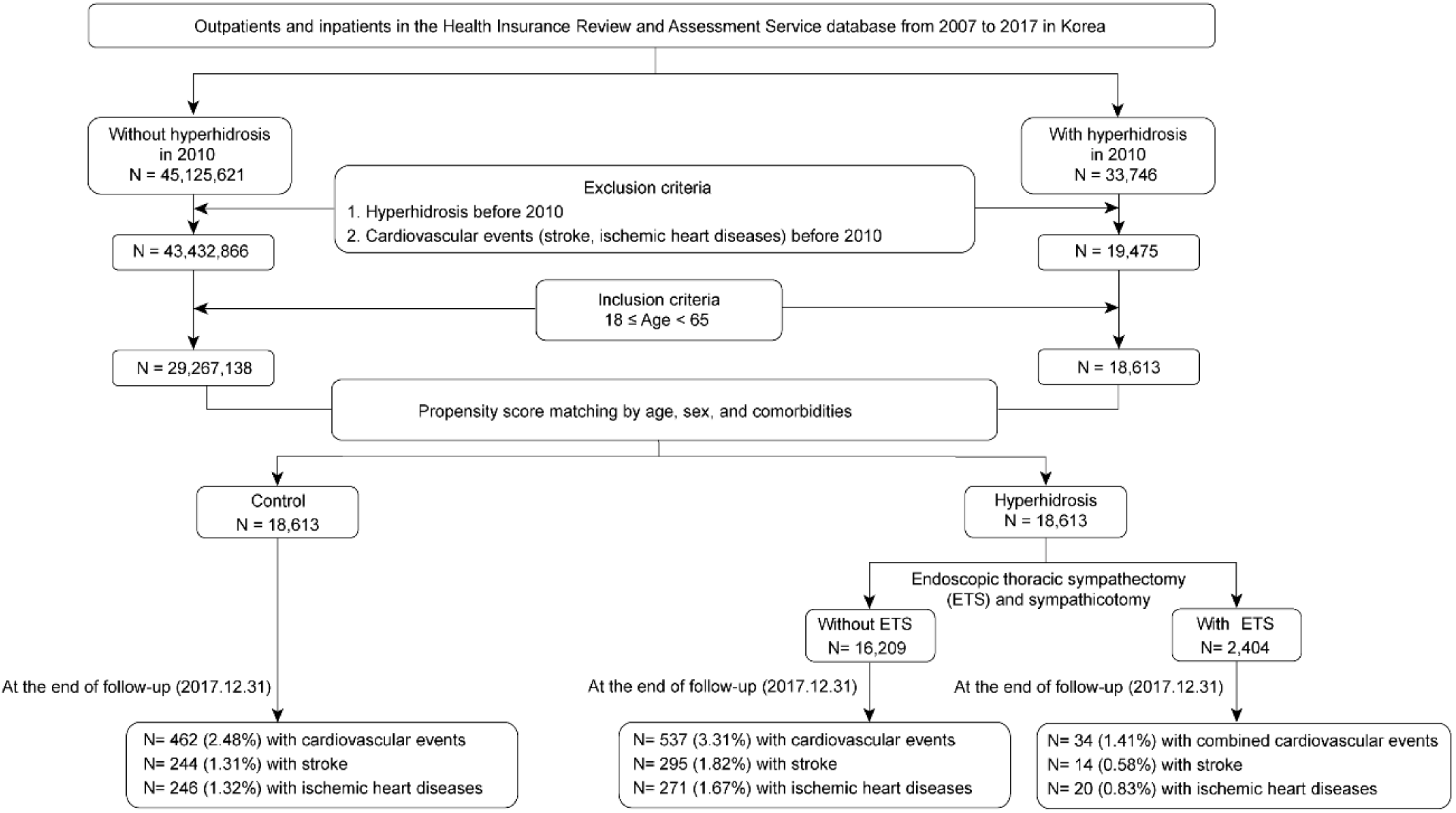
2.2. Study Population and Design
2.3. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Worle, B.; Rapprich, S.; Heckmann, M. Definition and treatment of primary hyperhidrosis. J. Dtsch. Dermatol. Ges. 2007, 5, 625–628. [Google Scholar] [CrossRef] [PubMed]
- Strutton, D.R.; Kowalski, J.W.; Glaser, D.A.; Stang, P.E. US prevalence of hyperhidrosis and impact on individuals with axillary hyperhidrosis: Results from a national survey. J. Am. Acad. Dermatol. 2004, 51, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Dohn, D.F.; Zraik, O. Essential hyperhidrosis—Pathogenesis and treatment. Report of seven cases treated by upper thoracic sympathectomy. Clevel. Clin. Q. 1969, 36, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Solish, N.; Bertucci, V.; Dansereau, A.; Hong, H.C.; Lynde, C.; Lupin, M.; Smith, K.C.; Storwick, G.; Canadian Hyperhidrosis Advisory Committee. A comprehensive approach to the recognition, diagnosis, and severity-based treatment of focal hyperhidrosis: Recommendations of the Canadian Hyperhidrosis Advisory Committee. Dermatol. Surg. 2007, 33, 908–923. [Google Scholar] [CrossRef]
- Solish, N.; Wang, R.; Murray, C.A. Evaluating the patient presenting with hyperhidrosis. Thorac. Surg. Clin. 2008, 18, 133–140. [Google Scholar] [CrossRef]
- Flaa, A.; Mundal, H.H.; Eide, I.; Kjeldsen, S.; Rostrup, M. Sympathetic activity and cardiovascular risk factors in young men in the low, normal, and high blood pressure ranges. Hypertension 2006, 47, 396–402. [Google Scholar] [CrossRef]
- Hering, D.; Lachowska, K.; Schlaich, M. Role of the sympathetic nervous system in stress-mediated cardiovascular disease. Curr. Hypertens. Rep. 2015, 17, 80. [Google Scholar] [CrossRef]
- Malpas, S.C. Sympathetic nervous system overactivity and its role in the development of cardiovascular disease. Physiol. Rev. 2010, 90, 513–557. [Google Scholar] [CrossRef]
- Marina, N.; Teschemacher, A.G.; Kasparov, S.; Gourine, A.V. Glia, sympathetic activity and cardiovascular disease. Exp. Physiol. 2016, 101, 565–576. [Google Scholar] [CrossRef] [Green Version]
- Fisher, J.P.; Fadel, P.J. Therapeutic strategies for targeting excessive central sympathetic activation in human hypertension. Exp. Physiol. 2010, 95, 572–580. [Google Scholar] [CrossRef] [Green Version]
- Manolis, A.J.; Poulimenos, L.E.; Kallistratos, M.S.; Gavras, I.; Gavras, H. Sympathetic overactivity in hypertension and cardiovascular disease. Curr. Vasc. Pharmacol. 2014, 12, 4–15. [Google Scholar] [PubMed]
- Brunner-La Rocca, H.P.; Esler, M.D.; Jennings, G.L.; Kaye, D.M. Effect of cardiac sympathetic nervous activity on mode of death in congestive heart failure. Eur. Heart J. 2001, 22, 1136–1143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaye, D.M.; Lefkovits, J.; Jennings, G.L.; Bergin, P.; Broughton, A.; Esler, M.D. Adverse consequences of high sympathetic nervous activity in the failing human heart. J. Am. Coll. Cardiol. 1995, 26, 1257–1263. [Google Scholar] [CrossRef] [Green Version]
- Askari, A.; Kordzadeh, A.; Lee, G.H.; Harvey, M. Endoscopic thoracic sympathectomy for primary hyperhidrosis: A 16-year follow up in a single UK centre. Surgeon 2013, 11, 130–133. [Google Scholar] [CrossRef]
- Moraites, E.; Vaughn, O.A.; Hill, S. Endoscopic thoracic sympathectomy. Dermatol. Clin. 2014, 32, 541–548. [Google Scholar] [CrossRef]
- Nakamura, Y.; Fujimoto, M.; Nagata, Y.; Shiraishi, K.; Yoshizawa, H.; Kida, H.; Matsumoto, Y. Effects of endoscopic transthoracic sympathicotomy on hemodynamic and neurohumoral responses to exercise in humans. Circ. J. 2002, 66, 357–361. [Google Scholar] [CrossRef]
- Cheng, C.A.; Cheng, C.G.; Chu, H.; Lin, H.C.; Chung, C.H.; Chiu, H.W.; Chien, W.C. Risk reduction of long-term major adverse cardiovascular events after endoscopic thoracic sympathectomy in palmar hyperhidrosis. Clin. Auton. Res. 2017, 27, 393–400. [Google Scholar] [CrossRef]
- National Health Insurance Service. National Health Insurance Statistical Yearbook 2015; National Health Insurance Service: Seoul, Korea, 2016. [Google Scholar]
- Kim, L.; Kim, J.A.; Kim, S. A guide for the utilization of health insurance review and assessment service national patient samples. Epidemiol. Health 2014, 36, e2014008. [Google Scholar] [CrossRef]
- Chu, D.; Chen, R.C.; Lee, C.H.; Yang, N.P.; Chou, P. Incidence and frequency of endoscopic sympathectomy for the treatment of hyperhidrosis palmaris in Taiwan. Kaohsiung J. Med. Sci. 2010, 26, 123–129. [Google Scholar] [CrossRef]
- Nawrocki, S.; Cha, J. The etiology, diagnosis and management of hyperhidrosis: A comprehensive review. Part I. Etiology and clinical work-up. J. Am. Acad. Dermatol. 2019, 81, 657–666. [Google Scholar] [CrossRef]
- Cruz, J.; Sousa, J.; Oliveira, A.G.; Silva-Carvalho, L. Effects of endoscopic thoracic sympathectomy for primary hyperhidrosis on cardiac autonomic nervous activity. J. Thorac. Cardiovasc. Surg. 2009, 137, 664–669. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeng, J.S.; Yip, P.K.; Huang, S.J.; Kao, M.C. Changes in hemodynamics of the carotid and middle cerebral arteries before and after endoscopic sympathectomy in patients with palmar hyperhidrosis: Preliminary results. J. Neurosurg. 1999, 90, 463–467. [Google Scholar] [CrossRef] [PubMed]
- Shibasaki, M.; Crandall, C.G. Mechanisms and controllers of eccrine sweating in humans. Front. Biosci. (Schol. Ed.) 2010, 2, 685–696. [Google Scholar] [PubMed]
- Hornberger, J.; Grimes, K.; Naumann, M.; Glaser, D.A.; Lowe, N.J.; Naver, H.; Ahn, S.; Stolman, L.P.; Multi-Specialty Working Group on the Recognition, Diagnosis, and Treatment of Primary Focal Hyperhidrosis. Recognition, diagnosis, and treatment of primary focal hyperhidrosis. J. Am. Acad. Dermatol. 2004, 51, 274–286. [Google Scholar]
- Harker, M. Psychological sweating: A systematic review focused on aetiology and cutaneous response. Skin Pharmacol. Physiol. 2013, 26, 92–100. [Google Scholar] [CrossRef]
- Hu, Y.; Converse, C.; Lyons, M.C.; Hsu, W.H. Neural control of sweat secretion: A review. Br. J. Dermatol. 2018, 178, 1246–1256. [Google Scholar] [CrossRef]
- Yeung, A.C.; Vekshtein, V.I.; Krantz, D.S.; Vita, J.A.; Ryan, T.J., Jr.; Ganz, P.; Selwyn, A.P. The effect of atherosclerosis on the vasomotor response of coronary arteries to mental stress. N. Engl. J. Med. 1991, 325, 1551–1556. [Google Scholar] [CrossRef]
- Malkoff, S.B.; Muldoon, M.F.; Zeigler, Z.R.; Manuck, S.B. Blood platelet responsivity to acute mental stress. Psychosom. Med. 1993, 55, 477–482. [Google Scholar] [CrossRef]
- Iyngkaran, P.; Anavekar, N.; Majoni, W.; Thomas, M.C. The role and management of sympathetic overactivity in cardiovascular and renal complications of diabetes. Diabetes Metab. 2013, 39, 290–298. [Google Scholar] [CrossRef]
- Manolis, A.J.; Olympios, C.; Sifaki, M.; Handanis, S.; Bresnahan, M.; Gavras, I.; Gavras, H. Suppressing sympathetic activation in congestive heart failure. A new therapeutic strategy. Hypertension 1995, 26, 719–724. [Google Scholar] [CrossRef]
- Rafiq, K.; Noma, T.; Fujisawa, Y.; Ishihara, Y.; Arai, Y.; Nabi, A.H.; Suzuki, F.; Nagai, Y.; Nakano, D.; Hitomi, H.; et al. Renal sympathetic denervation suppresses de novo podocyte injury and albuminuria in rats with aortic regurgitation. Circulation 2012, 125, 1402–1413. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, J.L.; Fode-Thomas, N.C.; Fealey, R.D.; Eisenach, J.H.; Goerss, S.J. Endoscopic transthoracic limited sympathotomy for palmar-plantar hyperhidrosis: Outcomes and complications during a 10-year period. Mayo Clin. Proc. 2011, 86, 721–729. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.Y.; Wang, L.; Xu, J.J. The effects of thoracic sympathotomy on heart rate variability in patients with palmar hyperhidrosis. Yonsei Med. J. 2012, 53, 1081–1084. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.G.; Cheng, C.A.; Chien, W.C.; Chung, C.H.; Lee, J.T. Associated with ischemic stroke risk reduction after endoscopic thoracic sympathectomy for palmar sweating. J. Stroke Cerebrovasc. Dis. 2018, 27, 2235–2242. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Control | Hyperhidrosis | p-Value | Control | Hyperhidrosis | p-Value | Post Hoc | ||
|---|---|---|---|---|---|---|---|---|
| Without ETS | With ETS | |||||||
| N | 18,613 | 18,613 | 18,613 | 16,209 | 2404 | |||
| Age (years) | 32.8 ± 12.2 | 32.8 ± 12.2 | 0.961 | 32.8 ± 12.2 | 33.4 ± 12.4 | 28.8 ± 9.9 | <0.001 | a, b, c |
| Sex | 0.909 | 0.041 | b, c | |||||
| Female | 9123 (49.0%) | 9134 (49.1%) | 9123 (49.0%) | 8012 (49.4%) | 1122 (46.7%) | |||
| Male | 9490 (51.0%) | 9479 (50.9%) | 9490 (51.0%) | 8197 (50.6%) | 1282 (53.3%) | |||
| Comorbidity | ||||||||
| Diabetes mellitus | 640 (3.4%) | 633 (3.4%) | 0.842 | 640 (3.4%) | 609 (3.8%) | 24 (1.0%) | <0.001 | b, c |
| Hypertension | 1301 (7.0%) | 1292 (7.0%) | 0.855 | 1301 (7.0%) | 1204 (7.4%) | 88 (3.7%) | <0.001 | b, c |
| Atrial fibrillation | 47 (0.3%) | 37 (0.2%) | 0.275 | 47 (0.3%) | 34 (0.2%) | 3 (0.1%) | 0.394 | — |
| Dyslipidemia | 1185 (6.4%) | 1202 (6.5%) | 0.719 | 1185 (6.4%) | 1096 (6.8%) | 106 (4.4%) | <0.001 | b, c |
| Congestive heart failure | 22 (0.1%) | 22 (0.1%) | >0.999 | 22 (0.1%) | 21 (0.1%) | 1 (0.1%) | 0.504 | — |
| Mood disorder | 862 (4.6%) | 853 (4.6%) | 0.824 | 862 (4.6%) | 785 (4.8%) | 68 (2.8%) | <0.001 | b, c |
| Anxiety disorder | 809 (4.4%) | 809 (4.4%) | >0.999 | 809 (4.4%) | 733 (4.5%) | 76 (3.2%) | 0.009 | b, c |
| Renal disease | 46 (0.2%) | 31 (0.2%) | 0.087 | 46 (0.2%) | 30 (0.2%) | 1 (0.1%) | 0.081 | — |
| Malignant neoplasm | 243 (1.3%) | 225 (1.2%) | 0.402 | 243 (1.3%) | 210 (1.3%) | 15 (0.6%) | 0.016 | b, c |
| Control | Hyperhidrosis | |
|---|---|---|
| Stroke | ||
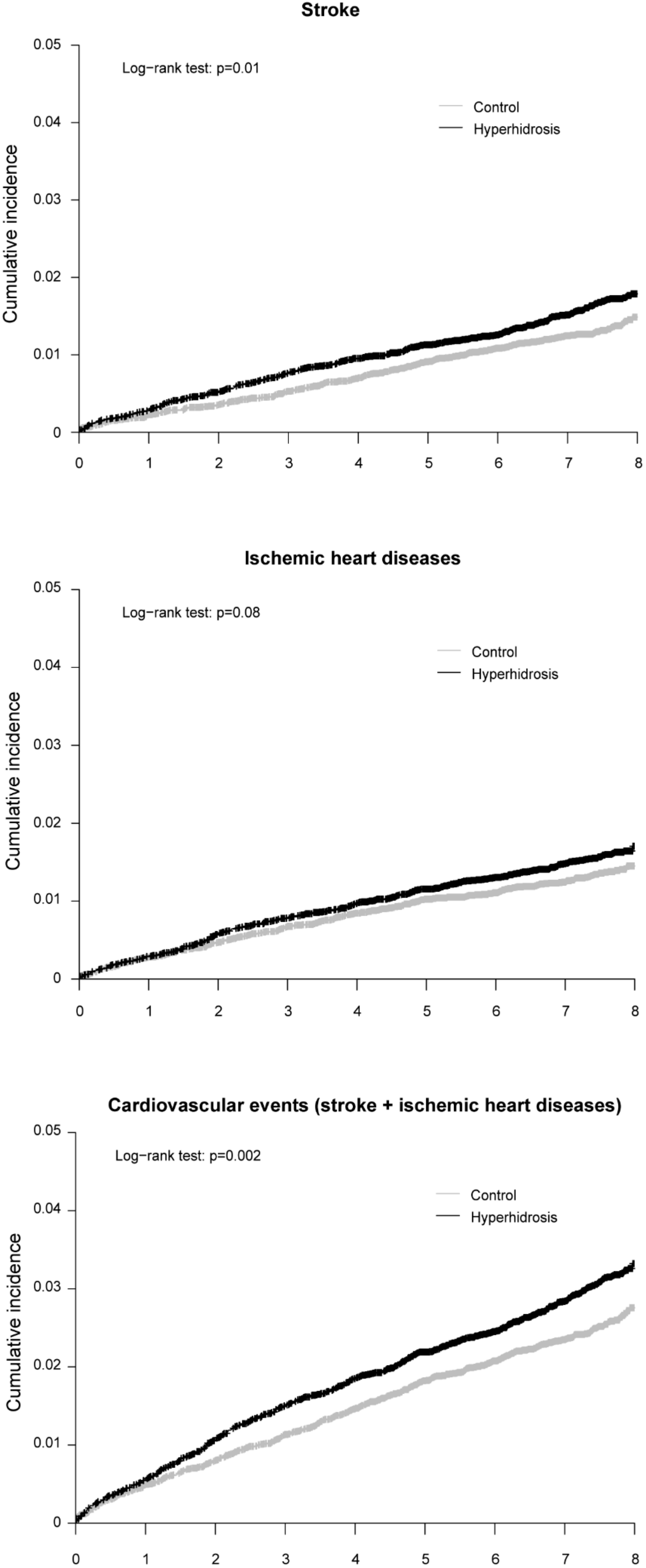
| Crude HR (95% CI) | 1 (reference) | 1.24 (1.05–1.47) |
| Adjusted HR 1 (95% CI) | 1 (reference) | 1.28 (1.08–1.51) |
| Ischemic heart diseases | ||
| Crude HR (95% CI) | 1 (reference) | 1.16 (0.98–1.38) |
| Adjusted HR 1 (95% CI) | 1 (reference) | 1.17 (0.99–1.39) |
| Combined cardiovascular events | ||
| Crude HR (95% CI) | 1 (reference) | 1.22 (1.08–1.37) |
| Adjusted HR 1 (95% CI) | 1 (reference) | 1.24 (1.10–1.41) |
| Control | Hyperhidrosis | ||
|---|---|---|---|
| Without ETS | With ETS | ||
| Stroke | |||
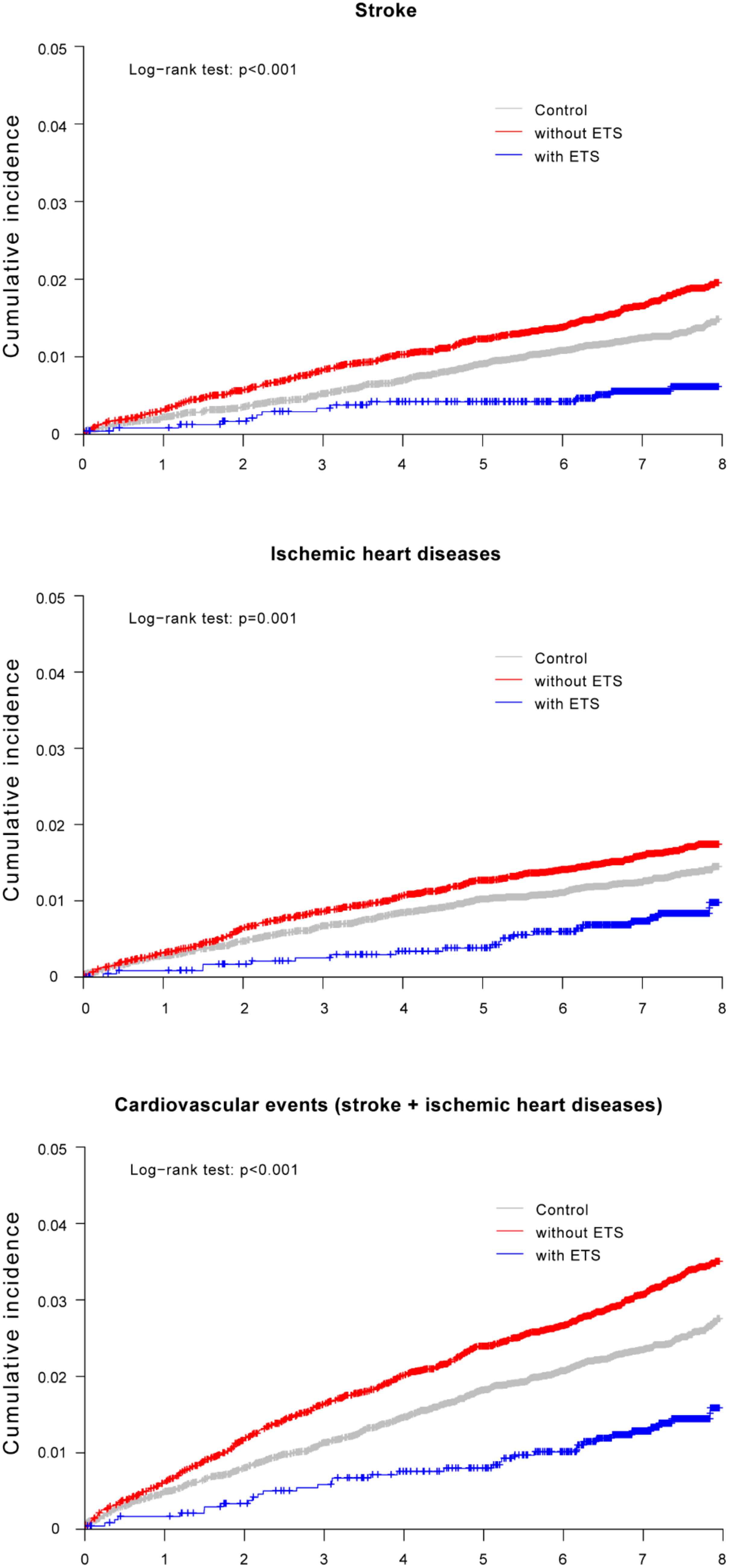
| Crude HR (95% CI) | 1 (reference) | 1.36 (1.15–1.61) | 0.44 (0.26–0.75) |
| Adjusted HR 1 (95% CI) | 1 (reference) | 1.32 (1.12–1.57) | 0.72 (0.42–1.24) |
| Ischemic heart diseases | |||
| Crude HR (95% CI) | 1 (reference) | 1.24 (1.05–1.48) | 0.62 (0.39–0.98) |
| Adjusted HR 1 (95% CI) | 1 (reference) | 1.19 (1.01–1.41) | 0.97 (0.61–1.53) |
| Combined cardiovascular events | |||
| Crude HR (95% CI) | 1 (reference) | 1.31 (1.16–1.49) | 0.56 (0.40–0.79) |
| Adjusted HR 1 (95% CI) | 1 (reference) | 1.28 (1.13–1.45) | 0.89 (0.63–1.26) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, J.-M.; Moon, D.H.; Lee, H.S.; Park, J.-y.; Lee, J.-W.; Lee, S. Hyperhidrosis, Endoscopic Thoracic Sympathectomy, and Cardiovascular Outcomes: A Cohort Study Based on the Korean Health Insurance Review and Assessment Service Database. Int. J. Environ. Res. Public Health 2019, 16, 3925. https://doi.org/10.3390/ijerph16203925
Park J-M, Moon DH, Lee HS, Park J-y, Lee J-W, Lee S. Hyperhidrosis, Endoscopic Thoracic Sympathectomy, and Cardiovascular Outcomes: A Cohort Study Based on the Korean Health Insurance Review and Assessment Service Database. International Journal of Environmental Research and Public Health. 2019; 16(20):3925. https://doi.org/10.3390/ijerph16203925
Chicago/Turabian StylePark, Jae-Min, Duk Hwan Moon, Hye Sun Lee, Ju-young Park, Ji-Won Lee, and Sungsoo Lee. 2019. "Hyperhidrosis, Endoscopic Thoracic Sympathectomy, and Cardiovascular Outcomes: A Cohort Study Based on the Korean Health Insurance Review and Assessment Service Database" International Journal of Environmental Research and Public Health 16, no. 20: 3925. https://doi.org/10.3390/ijerph16203925