The Moderating Role of the School Context on the Effects of the Healthy Primary School of the Future

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
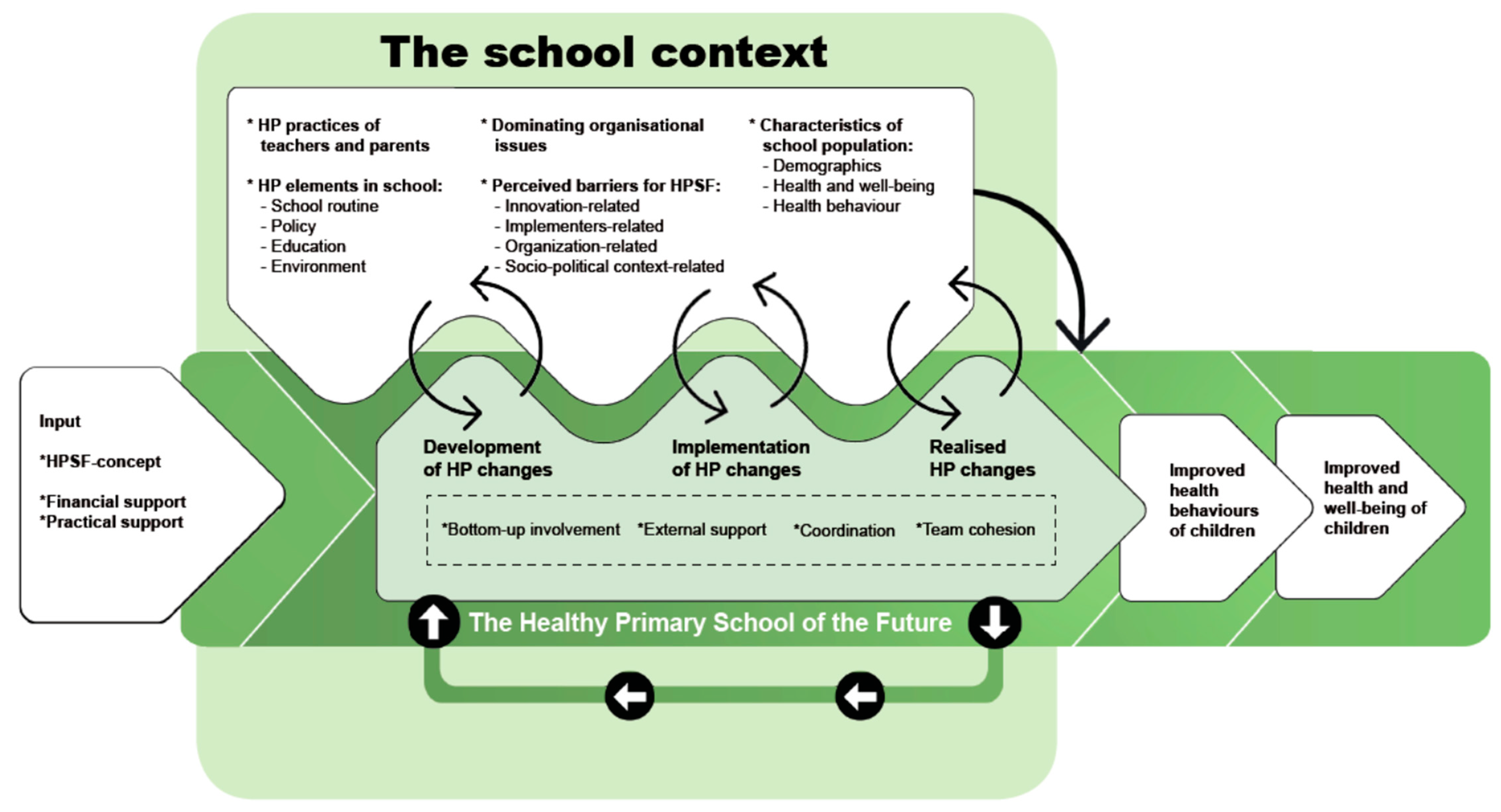
2.1. The Healthy Primary School of the Future
2.2. Study Design
2.3. Measures
2.3.1. Effect Measures
2.3.2. Context Measures
Characteristics of the School Population
HP Practices of the Teachers
Perceived Barriers to the Implementation of HP Changes
HP Elements in the School
Dominating Organizational Issues
2.4. Analyses
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Suhrcke, M.; de Paz Nieves, C. The Impact of Health and Health Behaviours on Educational Outcomes in High-Income Countries: A Review of The Evidence; World Health Organization, Regional Office for Europe: Copenhagen, Denmark, 2011. [Google Scholar]
- Fiscella, K.; Kitzman, H. Disparities in academic achievement and health: The intersection of child education and health policy. J. Pediatr. 2009, 123, 1073–1080. [Google Scholar] [CrossRef] [PubMed]
- Dooris, M.; Poland, B.; Kolbe, L.; De Leeuw, E.; McCall, D.S.; Wharf-Higgins, J. Healthy settings. In Global Perspectives on Health Promotion Effectiveness; Springer: Berlin, Germany, 2007; pp. 327–352. [Google Scholar]
- Langford, R.; Campbell, R.; Magnus, D.; Bonell, C.P.; Murphy, S.M.; Waters, E.; Komro, K.A.; Gibbs, L.F.; Magnus, D.; Campbell, R. The WHO Health Promoting School framework for improving the health and well-being of students and staff. Cochrane Database Syst. Rev. 2011, 1. [Google Scholar] [CrossRef]
- Bonell, C.; Parry, W.; Wells, H.; Jamal, F.; Fletcher, A.; Harden, A.; Thomas, J.; Campbell, R.; Petticrew, M.; Murphy, S.; et al. The effects of the school environment on student health: A systematic review of multi-level studies. Health Place 2013, 21, 180–191. [Google Scholar] [CrossRef] [PubMed]
- Leurs, M.T.; Schaalma, H.P.; Jansen, M.W.; Mur-Veeman, I.M.; St Leger, L.H.; De Vries, N. Development of a collaborative model to improve school health promotion in the Netherlands. Health Promot. Int. 2005, 20, 296–305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Promoting Health through Schools: Report of a Who Expert Committee on Comprehensive School Health Education and Promotion; WHO: Geneva, Switzerland, 1997. [Google Scholar]
- WHO. Health Promoting Schools: A Framework for Action; World Health Organization Western Pacific Region: Manila, Philippines, 2009. [Google Scholar]
- Deschesnes, M.; Martin, C.; Hill, A.J. Comprehensive approaches to school health promotion: How to achieve broader implementation? Health Promot. Int. 2003, 18, 387–396. [Google Scholar] [CrossRef] [PubMed]
- Lee, A. Health-promoting schools. Appl. Health Econ. Health Policy 2009, 7, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Langford, R.; Bonell, C.P.; Jones, H.E.; Pouliou, T.; Murphy, S.M.; Waters, E.; Komro, K.A.; Gibbs, L.F.; Magnus, D.; Campbell, R. The WHO Health Promoting School framework for improving the health and well-being of students and their academic achievement. Cochrane Database Syst. Rev. 2014, 4, CD008958. [Google Scholar] [CrossRef] [PubMed]
- Darlington, E.J.; Violon, N.; Jourdan, D. Implementation of health promotion programmes in schools: An approach to understand the influence of contextual factors on the process? BMC Public Health 2018, 18, 163. [Google Scholar] [CrossRef] [PubMed]
- Schaap, R.; Bessems, K.; Otten, R.; Kremers, S.; van Nassau, F. Measuring implementation fidelity of school-based obesity prevention programmes: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 75. [Google Scholar] [CrossRef] [PubMed]
- Keshavarz, N.; Nutbeam, D.; Rowling, L.; Khavarpour, F. Schools as social complex adaptive systems: A new way to understand the challenges of introducing the health promoting schools concept. Soc. Sci. Med. 2010, 70, 1467–1474. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi, N.K. Complexity Science, Schools and Health: Applications for Management of Change in Schools TO Promote Health and Education; Lambert Academic Publishing: Saarbrucken, Germany, 2010. [Google Scholar]
- Snyder, S. The Simple, the Complicated, and the Complex: Educational Reform through the Lens of Complexity Theory; OECD Publishing: Paris, France, 2013. [Google Scholar]
- Paina, L.; Peters, D.H. Understanding pathways for scaling up health services through the lens of complex adaptive systems. Health Policy Plan. 2011, 27, 365–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, G.F.; Evans, R.E.; Hawkins, J.; Littlecott, H.; Melendez-Torres, G.; Bonell, C.; Murphy, S. From complex social interventions to interventions in complex social systems: Future directions and unresolved questions for intervention development and evaluation. Evaluation 2019, 25, 23–45. [Google Scholar] [CrossRef] [PubMed]
- Hovmand, P.S. Introduction to Community-Based System Dynamics. In Community Based System Dynamics; Springer: New York, NY, USA, 2014; pp. 1–15. [Google Scholar]
- Turunen, H.; Sormunen, M.; Jourdan, D.; Von Seelen, J.; Buijs, G. Health Promoting Schools—A complex approach and a major means to health improvement. Health Promot. Int. 2017, 32, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Moore, G.F.; Audrey, S.; Barker, M.; Bond, L.; Bonell, C.; Hardeman, W.; Moore, L.; O’Cathain, A.; Tinati, T.; Wight, D.; et al. Process evaluation of complex interventions: Medical Research Council guidance. BMJ 2015, 350, h1258. [Google Scholar] [CrossRef] [PubMed]
- Patton, M.Q. Developmental Evaluation: Applying Complexity Concepts to Enhance Innovation and Use; Guilford Press: New York, NY, USA, 2011. [Google Scholar]
- Pawson, R.; Tilley, N. Realistic Evaluation; Sage: London, UK, 1997. [Google Scholar]
- Rosas, S.R. Systems thinking and complexity: Considerations for health promoting schools. Health Promot. Int. 2015, 32, 301–311. [Google Scholar] [CrossRef] [PubMed]
- Bisset, S.; Daniel, M.; Potvin, L. Exploring the intervention—Context interface: A case from a school-based nutrition intervention. Am. J. Eval. 2009, 30, 554–571. [Google Scholar] [CrossRef]
- Poland, B.; Krupa, G.; McCall, D. Settings for health promotion: An analytic framework to guide intervention design and implementation. Health Promot. Pract. 2009, 10, 505–516. [Google Scholar] [CrossRef]
- Damschroder, L.J.; Aron, D.C.; Keith, R.E.; Kirsh, S.R.; Alexander, J.A.; Lowery, J.C. Fostering implementation of health services research findings into practice: A consolidated framework for advancing implementation science. Implement. Sci. 2009, 4, 1. [Google Scholar] [CrossRef]
- Bartelink, N.; van Assema, P.; Jansen, M.; Savelberg, H.; Moore, G.; Hawkings, J.; Kremers, S.P.J. Process evaluation of the Healthy primary School of the Future: The key learning points. BMC Public Health 2019, 19, 698. [Google Scholar] [CrossRef]
- Fleuren, M.A.; Paulussen, T.G.; Van Dommelen, P.; Van Buuren, S. Towards a measurement instrument for determinants of innovations. Int. J. Qual. Health Care 2014, 26, 501–510. [Google Scholar] [CrossRef] [Green Version]
- Willeboordse, M.; Jansen, M.; van den Heijkant, S.; Simons, A.; Winkens, B.; de Groot, R.; Bartelink, N.; Kremers, S.P.; Van Assema, P.; Savelberg, H.H.; et al. The Healthy Primary School of the Future: Study protocol of a quasi-experimental study. BMC Public Health 2016, 16, 639. [Google Scholar] [CrossRef] [PubMed]
- Bartelink, N.; van Assema, P.; Jansen, M.; Savelberg, H.; Willeboordse, M.; Kremers, S. The Healthy Primary School of the Future: A Contextual Action-Oriented Research Approach. Int. J. Environ. Res. Public. Health 2018, 15, 2243. [Google Scholar] [CrossRef] [PubMed]
- Bartelink, N.H.; van Assema, P.; Kremers, S.P.; Savelberg, H.H.; Oosterhoff, M.; Willeboordse, M.; van Schayck, O.C.; Winkens, B.; Jansen, M.W. One-and Two-Year Effects of the Healthy Primary School of the Future on Children’s Dietary and Physical Activity Behaviours: A Quasi-Experimental Study. Nutrients 2019, 11, 689. [Google Scholar] [CrossRef] [PubMed]
- Bartelink, N.H.; van Assema, P.; Kremers, S.P.; Savelberg, H.H.; Oosterhoff, M.; Willeboordse, M. Can the Healthy Primary School of the Future offer perspective in the on-going obesity epidemic in young children?—A quasi-experimental study. Submitted.
- Schils, T. Pupils in Secondary Education: Who Are They? What Is Their Sense of Self-Worth? How Smart Are They? Kaans Reports k04201102-k04201104; Kaans/Maastricht University School of Business and Economics: Maastricht, The Netherlands, 2011. (In Dutch) [Google Scholar]
- Vermeer, A.J.M.; Boot, N.M.W.M.; Hesdahl, M.H.; Janssen-Goffin, M.J.H.; Linssen, E.C.A.J.; Rutten, N. Local Reports on Public Health Development: A New Perspective on Health in Heerlen, Kerkrade, Landgraaf and Brunssum; GGD Zuid Limburg: Geleen, The Netherlands, 2014. (In Dutch) [Google Scholar]
- Schönbeck, Y.; Talma, H.; van Dommelen, P.; Bakker, B.; Buitendijk, S.E.; HiraSing, R.A.; van Buuren, S. Increase in prevalence of overweight in Dutch children and adolescents: A comparison of nationwide growth studies in 1980, 1997 and 2009. PLoS ONE 2011, 6, e27608. [Google Scholar] [CrossRef] [PubMed]
- Evenson, K.R.; Catellier, D.J.; Gill, K.; Ondrak, K.S.; McMurray, R.G. Calibration of two objective measures of physical activity for children. J. Sports Sci. 2008, 26, 1557–1565. [Google Scholar] [CrossRef] [PubMed]
- Keij, I. How Does Statistics Netherlands Do This? Standard Definition of Emigrants; CBS: Heerlen, The Netherlands, 2000. (In Dutch) [Google Scholar]
- Shavers, V.L. Measurement of socioeconomic status in health disparities research. J. Natl. Med. Assoc. 2007, 99, 1013. [Google Scholar]
- Gevers, D.W.; Kremers, S.P.; de Vries, N.K.; van Assema, P. Patterns of food parenting practices and children’s intake of energy-dense snack foods. Nutrients 2015, 7, 4093–4106. [Google Scholar] [CrossRef]
- Gevers, D.; Kremers, S.; de Vries, N.; van Assema, P. The Comprehensive Snack Parenting Questionnaire (CSPQ): Development and Test-Retest Reliability. Int. J. Environ. Res. Public Health 2018, 15, 862. [Google Scholar] [CrossRef]
- O’Connor, T.M.; Cerin, E.; Hughes, S.O.; Robles, J.; Thompson, D.I.; Mendoza, J.A.; Baranowski, T.; Lee, R.E. Psychometrics of the preschooler physical activity parenting practices instrument among a Latino sample. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 3. [Google Scholar] [CrossRef]
- Fleuren, M.; Paulussen, T.; Van Dommelen, P.; Van Buuren, S. Measurement Instrument for Determinants of Innovations (MIDI); TNO: Leiden, The Netherlands, 2014. [Google Scholar]
- Kane, H.; Lewis, M.A.; Williams, P.A.; Kahwati, L.C. Using qualitative comparative analysis to understand and quantify translation and implementation. Transl. Behav. Med. 2014, 4, 201–208. [Google Scholar] [CrossRef] [Green Version]
- Schneider, C.Q.; Wagemann, C. Set-Theoretic Methods for the Social Sciences: A Guide to Qualitative Comparative Analysis; Cambridge University Press: New York, NY, USA, 2012. [Google Scholar]
- Burton, C. Heavy tailed distributions of effect sizes in systematic reviews of complex interventions. PLoS ONE 2012, 7, e34222. [Google Scholar] [CrossRef] [PubMed]
- Lorenc, T.; Petticrew, M.; Welch, V.; Tugwell, P. What types of interventions generate inequalities? Evidence from systematic reviews. J. Epidemiol. Community Health 2013, 67, 190–193. [Google Scholar] [CrossRef] [PubMed]
- Gubbels, J.S.; Van Kann, D.H.; de Vries, N.K.; Thijs, C.; Kremers, S.P. The next step in health behavior research: The need for ecological moderation analyses-an application to diet and physical activity at childcare. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 52. [Google Scholar] [CrossRef] [PubMed]
- Lohrmann, D.K. A complementary ecological model of the coordinated school health program. Public Health Rep. 2008, 123, 695–703. [Google Scholar] [CrossRef] [PubMed]
- Vermeiren, A.P.; Willeboordse, M.; Oosterhoff, M.; Bartelink, N.; Muris, P.; Bosma, H. Socioeconomic multi-domain health inequalities in Dutch primary school children. Eur. J. Public Health 2018, 28, 610–616. [Google Scholar] [CrossRef] [PubMed]
- Ball, K. Traversing myths and mountains: Addressing socioeconomic inequities in the promotion of nutrition and physical activity behaviours. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 142. [Google Scholar] [CrossRef] [PubMed]
- Gubbels, J.S.; Gerards, S.M.; Kremers, S.P. Use of food practices by childcare staff and the association with dietary intake of children at childcare. Nutrients 2015, 7, 2161–2175. [Google Scholar] [CrossRef]
- Hawe, P.; Shiell, A.; Riley, T. Theorising interventions as events in systems. Am. J. Commun. Psychol. 2009, 43, 267–276. [Google Scholar] [CrossRef]
- Kremers, S.P.; Visscher, T.L.; Schuit, A.J. Effect in its context. Tijdschr Gezondh. 2018, 96, 128–131. (In Dutch) [Google Scholar] [CrossRef]


{kind=link}
| Effects of HPSF in Each School (Effect Sizes) * | ||||||||
| Full HPSF | Outcome measures | Partial HPSF | ||||||
| School 1 | School 2 | School 3 | School 4 | |||||
| T0–T2 | T0–T2 | T0–T2 | T0–T2 | |||||
| −0.11 | −0.05 | BMI z−score | −0.04 | −0.08 | ||||
| −0.27 | −0.08 | Sedentary time | −0.03 | −0.08 | ||||
| 0.26 | 0.09 | Light PA | 0.01 | 0.02 | ||||
| 0.15 | 0.05 | MVPA | 0.04 | 0.15 | ||||
| 0.25 | 0.03 | Healthy dietary behaviors | 0.08 | −0.08 | ||||
| −0.13 | −0.07 | Unhealthy dietary behaviors | 0.06 | −0.02 | ||||
| 1.16 | 1.17 | Water consumption in school | −0.20 | 0.14 | ||||
| 2.52 | 3.96 | Minimum of two food types during lunch (OR) | 0.20 | 0.94 | ||||
| The Four School Contexts | ||||||||
| Characteristics of the school population—Children | ||||||||
| Full HPSF | Contextual aspects | Partial HPSF | ||||||
| School 1 | School 2 | School 3 | School 4 | |||||
| T0 | T0 | T0 | T0 | |||||
| 324 | 234 | Number of children (N) | 233 | 389 | ||||
| 48.6 | 51.0 | Gender (% boys) | 45.7 | 49.5 | ||||
| 8.04 (2.21) | 8.55 (2.22) | Age in years (mean (SD)) | 8.45 (2.34) | 7.82 (2.43) | ||||
| 24.0 | 32.3 | SES (% lowest tertile) | 38.4 | 28.1 | ||||
| 94.8 | 94.3 | Ethnicity (% western) | 98.4 | 94.9 | ||||
| Characteristics of the school population—Teachers | ||||||||
| Full HPSF | Contextual aspects | Partial HPSF | ||||||
| School 1 | School 2 | School 3 | School 4 | |||||
| T0 | T0 | T0 | T0 | |||||
| 26 | 15 | Number of teachers (N) | 16 | 21 | ||||
| 19.2 | 33.3 | Gender (% men) | 0 | 22.7 | ||||
| 45.35 (13.71) | 44.60 (11.81) | Age in years (mean (SD)) | 41.80 (13.46) | 41.27 (10.74) | ||||
| 12.31 (12.72) | 11.47 (7.28) | Working in the school in years (mean (SD)) | 0.92 (1.24) | 12.64 (8.56) | ||||
| Starting situation of the school population—Children | ||||||||
| Full HPSF | Contextual aspects | Partial HPSF | ||||||
| School 1 | School 2 | School 3 | School 4 | |||||
| T0 | T0 | T0 | T0 | |||||
| 0.028 (1.00) | 0.092 (1.02) | BMI z-score (mean (SD)) | 0.082 (1.01) | 0.099 (0.91) | ||||
| 58.5 (6.76) | 61.9 (7.45) | Sedentary time (% per day) | 61.6 (6.54) | 60.3 (7.29) | ||||
| 32.8 (5.48) | 30.6 (5.98) | Light PA (% per day) | 31.1 (5.35) | 32.4 (5.80) | ||||
| 8.7 (2.63) | 7.5 (2.72) | MVPA (% per day) | 7.3 (2.58) | 7.3 (2.51) | ||||
| 5.06 (1.16) | 5.33 (1.05) | Healthy dietary behavior in days/week (mean (SD)) | 5.24 (0.81) | 5.07 (1.12) | ||||
| 1.12 (0.64) | 1.08 (0.66) | Unhealthy dietary behavior in days/week (mean (SD)) | 1.02 (0.53) | 1.11 (0.63) | ||||
| 2.16 (1.11) | 2.20 (1.07) | School water consumption: range 0-3 (mean (SD)) | 2.94 (1.22) | 1.93 (1.06) | ||||
| 78.7 | 84.6 | Minimum of two food types during lunch (% yes) | 94.7 | 79.3 | ||||
| Starting situation of the school population—Teachers | ||||||||
| Full HPSF | Contextual aspects | Partial HPSF | ||||||
| School 1 | School 2 | School 3 | School 4 | |||||
| T0 | T0 | T0 | T0 | |||||
| 23.79 (3.16) | 27.50 (4.61) | Self-reported BMI in kg/m2 (mean (SD)) | 23.23 (2.67) | 24.23 (3.00) | ||||
| Nutrition-related teacher practices (range 1-5; presented as mean (SD)) ** | ||||||||
| Full HPSF | Contextual aspects | Partial HPSF | ||||||
| School 1 | School 2 | School 3 | School 4 | |||||
| T0 | T2 | T0 | T2 | T0 | T2 | T0 | T2 | |
| 4.4 (±0.80) | 4.5 (±0.74) | 4.3 (±1.10) | 4.7 (±0.56) Δ | Healthy modelling | 4.2 (±0.97) | 4.1 (±0.99) Δ | 4.1 (±1.05) | 4.0 (±0.89) Δ |
| 4.0 (±1.20) | 4.6 (±0.69) | 4.2 (±0.94) | 4.9 (±0.62) Δ | Prevent unhealthy modelling | 4.1 (±1.10) | 3.5 (±1.20) | 3.5 (±1.18) | 3.7 (±1.17) Δ |
| 4.5 (±0.51) | 4.6 (±0.56) | 4.3 (±0.88) | 4.9 (±0.46) Δ | Encouragement | 4.7 (±0.48) | 4.5 (±0.54) Δ | 4.5 (±0.60) | 4.3 (±0.75) Δ |
| 4.4 (±0.63) | 4.5 (±0.63) | 4.1 (±1.16) | 4.5 (±0.51) Δ | Involving | 4.3 (±0.95) | 4.4 (±0.52) Δ | 4.3 (±1.03) | 4.1 (±0.95) |
| 4.4 (±0.75) | 4.4 (±0.57) | 4.3 (±0.72) | 4.7 (±0.45) Δ | Discussing | 4.5 (±0.53) | 4.3 (±0.71) | 4.2 (±0.61) | 4.1 (±0.68) Δ |
| 4.2 (±0.77) | 4.5 (±0.69) Δ | 4.2 (±0.68) | 4.5 (±0.61) Δ | Educating | 4.6 (±0.70) | 4.1 (±0.64) | 4.1 (±0.68) | 4.3 (±0.74) Δ |
| 4.0 (±0.66) | 4.2 (±0.69) | 3.9 (±0.80) | 4.3 (±0.56) Δ | Providing feedback | 3.7 (±1.06) | 4.1 (±0.35) Δ | 4.1 (±0.99) | 3.8 (±1.02) |
| 3.7 (±1.23) | 3.7 (±1.31) | 3.6 (±1.24) | 4.1 (±0.71) Δ | Visibility | 4.0 (±0.82) | 3.0 (±1.07) | 3.7 (±1.56) | 3.7 (±0.96 Δ |
| 4.4 (±0.85) | 4.5 (±0.51) | 4.3 (±0.98) | 4.7 (±0.48) Δ | Routines | 4.2 (±0.83) | 4.4 (±0.52) Δ | 4.2 (±0.81) | 4.2 (±0.82) |
| 3.5 (±1.07) | 4.5 (±1.30) Δ | 3.5 (±1.13) | 3.8 (±1.03) | Monitoring | 3.5 (±1.43) | 3.8 (±0.46) | 2.9 (±1.41) | 3.4 (±1.59) Δ |
| 4.5 (±0.91) | 4.9 (±0.65) Δ | 4.5 (±0.52) | 4.7 (±0.58) | Rules | 4.4 (±0.70) | 4.3 (±0.89) | 4.2 (±0.96) | 4.4 (±0.89) Δ |
| 3.3 (±1.09) | 3.6 (±1.15) Δ | 3.6 (±0.91) | 3.9 (±1.73) Δ | Pressure to eat *** | 3.5 (±1.35) | 3.0 (±0.76) Δ | 3.6 (±1.37) | 3.2 (±1.47) |
| 2.5 (±1.75) | 2.4 (±1.78) | 2.8 (±1.52) | 1.5 (±1.17) Δ | Instrumental feeding *** | 2.8 (±1.48) | 2.1 (±1.25) Δ | 2.9 (±1.39) | 2.8 (±1.63) |
| PA-related teacher practices (range 1–5; presented as mean (SD)) ** | ||||||||
| Full HPSF | Contextual aspects | Partial HPSF | ||||||
| School 1 | School 2 | School 3 | School 4 | |||||
| T0 | T2 | T0 | T2 | T0 | T2 | T0 | T2 | |
| 4.2 (±0.71) | 4.6 (±0.57) Δ | 4.5 (±0.64) | 4.4 (±0.61) | Encouragement | 4.5 (±0.71) | 4.6 (±0.52) | 4.2 (±0.81) | 4.5 (±0.78) Δ |
| 4.1 (±0.89) | 4.6 (±0.83) Δ | 4.1 (±0.83) | 4.1 (±0.71) | Rewarding | 4.1 (±0.99) | 4.3 (±0.89) Δ | 4.1 (±1.11) | 4.0 (±1.00) |
| 3.8 (±0.91) | 4.1 (±0.95) Δ | 4.2 (±0.68) | 3.9 (±0.71) | Involving | 4.5 (±0.53) | 4.5 (±0.54) | 3.5 (±1.03) | 4.2 (±0.78) Δ |
| 3.7 (±1.01) | 4.0 (±0.98) Δ | 3.9 (±0.92) | 3.9 (±0.71) | Healthy modelling | 3.9 (±0.88) | 4.1 (±0.84) | 3.4 (±1.37) | 3.9 (±1.15) Δ |
| 4.1 (±0.74) | 4.2 (±0.77) | 4.0 (±0.85) | 4.2 (±0.50) Δ | Discussing | 4.5 (±0.53) | 4.3 (±0.71) | 4.3 (±0.80) | 4.3 (±0.76) Δ |
| 4.2 (±0.63) | 4.5 (±0.74) Δ | 4.2 (±0.56) | 4.2 (±0.69) | Educating | 4.7 (±0.68) | 4.6 (±0.74) Δ | 4.5 (±0.80) | 4.3 (±0.74) |
| 3.9 (±0.94) | 3.7 (±1.11) Δ | 3.4 (±1.30) | 3.8 (±0.83) | Discouragement *** | 3.9 (±1.10) | 3.0 (±0.93) Δ | 4.4 (±0.85) | 3.9 (±1.06) |
| 3.6 (±0.90) | 4.2 (±0.97) Δ | 3.7 (±1.10) | 3.7 (±0.89) | Providing feedback | 3.7 (±1.16) | 4.0 (±0.76) Δ | 3.5 (±1.37) | 3.7 (±1.08) |
| 4.4 (±1.03) | 4.3 (±1.00) | 4.1 (±0.64) | 4.3 (±0.45) Δ | Availability | 4.3 (±0.48) | 4.3 (±0.89) Δ | 4.1 (±1.07) | 4.0 (±1.00) |
| 3.6 (±1.50) | 4.0 (±1.59) Δ | 3.1 (±1.30) | 3.5 (±0.90) Δ | Visibility | 3.3 (±1.34) | 4.0 (±1.69) Δ | 3.6 (±1.71) | 3.1 (±1.32) |
| 4.2 (±0.71) | 4.4 (±0.62) Δ | 4.6 (±0.63) | 4.6 (±0.51) | Accessibility | 4.6 (±0.52) | 4.6 (±0.52) Δ | 4.5 (±0.67) | 4.5 (±0.59) Δ |
| 3.9 (±0.77) | 4.5 (±1.18) Δ | 4.1 (±0.80) | 4.1 (±0.78) | Routines | 4.3 (±0.82) | 4.3 (±0.71) | 3.8 (±1.15) | 4.4 (±0.71) Δ |
| 2.8 (±1.20) | 3.2 (±1.54) | 2.8 (±0.94) | 2.7 (±1.45) Δ | Warning PA *** | 2.6 (±1.35) | 2.4 (±1.30) Δ | 3.1 (±1.68) | 3.1 (±1.64) |
| 3.5 (±1.11) | 3.9 (±1.45) Δ | 3.1 (±1.03) | 3.2 (±1.17) | Monitoring | 3.1 (±1.29) | 3.0 (±0.93) Δ | 3.3 (±1.67) | 3.0 (±1.57) |
| 4.2 (±0.98) | 4.3 (±0.67) Δ | 4.4 (±0.63) | 4.4 (±0.61) | Rules | 4.5 (±0.53) | 4.6 (±0.74) Δ | 4.5 (±1.14) | 4.5 (±0.66) |
| 4.3 (±0.62) | 4.1 (±0.64) Δ | 4.5 (±0.83) | 4.4 (±0.50) | Pressure to be physically active *** | 4.5 (±0.53) | 4.6 (±0.52) Δ | 4.2 (±1.01) | 4.5 (±0.78) |
| 3.6 (±1.44) | 4.0 (±1.24) | 3.5 (±1.25) | 3.4 (±1.30) Δ | Instrumental feeding *** | 4.4 (±1.08) | 3.8 (±1.58) Δ | 4.0 (±1.25) | 4.0 (±1.37) |
| Teacher—perceived barriers for HPSF, related to (range 1–10; presented as mean (SD)) | ||||||||
| Full HPSF | Contextual aspects | Partial HPSF | ||||||
| School 1 | School 2 | School 3 | School 4 | |||||
| T0 | T2 | T0 | T2 | T0 | T2 | T0 | T2 | |
| 7.9 (±0.51) | 7.6 (±0.75) | 8.5 (±0.53) | 8.4 (±0.72) Δ | User | 8.1 (±0.96) | 8.6 (±0.73) Δ | 7.9 (±0.57) | 8.2 (±0.76) |
| 6.3 (±1.20) | 6.8 (±1.28) Δ | 7.3 (±0.64) | 7.3 (±0.90) | Innovation | 7.5 (±1.21) | 8.3 (±0.97) Δ | 7.4 (±0.83) | 8.0 (±0.82) |
| 6.8 (±0.93) | 7.8 (±1.17) Δ | 7.8 (±0.59) | 7.7 (±0.76) | Support | 7.1 (±1.80) | 8.6 (±0.65) Δ | 7.5 (±0.87) | 8.0 (±0.94) |
| 7.3 (±1.43) | 7.3 (±0.97) | 7.5 (±1.02) | 7.7 (±0.82) Δ | Organization | 7.7 (±1.56) | 8.5 (±0.80) Δ | 8.2 (±2.10) | 8.1 (±0.87) |
| 8.0 (±0.87) | 7.6 (±0.75) | 8.1 (±0.96) | 8.3 (±0.83) Δ | Socio-political context | 7.7 (±2.08) | 8.8 (±0.95) Δ | 7.8 (±1.02) | 8.3 (±0.93) |
| External pedagogical employee—perceived barriers for HPSF, related to (range 1–10; presented as mean (SD)) | ||||||||
| Full HPSF | Contextual aspects | Partial HPSF | ||||||
| School 1 | School 2 | School 3 | School 4 | |||||
| T0 | T2 | T0 | T2 | T0 | T2 | T0 | T2 | |
| 8.2 (±0.94) | 8.1 (±0.82) | 8.0 (±0.71) | 8.0 (±0.62) Δ | User | 7.5 (±0.68) | 7.2 (±0.55) | 7.6 (±0.65) | 7.9 (±0.38) Δ |
| 7.6 (±1.42) | 7.6 (±0.87) | 6.9 (±0.20) | 7.3 (±1.04) Δ | Innovation | 6.8 (±0.67) | 6.9 (±0.37) | 6.9 (±0.73) | 7.3 (±0.82) Δ |
| 7.4 (±1.33) | 8.1 (±0.60) | 5.6 (±1.53) | 7.8 (±0.62) Δ | Support | 5.6 (±1.62) | 6.6 (±1.30) Δ | 7.0 (±1.10) | 7.9 (±0.28) |
| 8.0 (±1.01) | 7.7 (±0.89) | 6.3 (±1.68) | 8.0 (±0.48) Δ | Organization | 5.9 (±0.88) | 6.9 (±0.53) Δ | 7.4 (±0.40) | 7.8 (±0.49) |
| 8.5 (±1.01) | 8.0 (±1.14) | 8.3 (±0.35) | 7.9 (±0.76) Δ | Socio-political context | 6.1 (±0.72) | 6.6 (±0.56) Δ | 8.0 (±0.91) | 7.3 (±0.90) |
| Health-promoting elements in school (absent (-), minimally present (X), moderately present (XX), largely present (XXX)) | ||||||||
| Full HPSF | Contextual aspects | Partial HPSF | ||||||
| School 1 | School 2 | School 3 | School 4 | |||||
| T0 | T2 | T0 | T2 | T0 | T2 | T0 | T2 | |
| X | XXX | X | XXX | Policy | X | XX | - | X |
| - | XX | - | XX | Education | XX | XXX | X | XX |
| X | XX | X | XX | Environment | XX | XX | X | XX |
| X | XXX | X | XXX | School routine | XX | XX | XX | XX |
| Dominating organizational issues (absent (-) or present (X)) | ||||||||
| Full HPSF | Contextual aspects | Partial HPSF | ||||||
| School 1 | School 2 | School 3 | School 4 | |||||
| T0–T2 | T0–T2 | T0–T2 | T0–T2 | |||||
| X (Nov 2015) | X (Sep 2016) | Merge | - | - | ||||
| - | - | Staff turn-over | X (Sep 2015) | - | ||||
| - | X (school year 2015/2016) | Temporary location | - | - | ||||
| X (Nov 2015) | - | New school building | - | - | ||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bartelink, N.; van Assema, P.; Jansen, M.; Savelberg, H.; Kremers, S. The Moderating Role of the School Context on the Effects of the Healthy Primary School of the Future. Int. J. Environ. Res. Public Health 2019, 16, 2432. https://doi.org/10.3390/ijerph16132432
Bartelink N, van Assema P, Jansen M, Savelberg H, Kremers S. The Moderating Role of the School Context on the Effects of the Healthy Primary School of the Future. International Journal of Environmental Research and Public Health. 2019; 16(13):2432. https://doi.org/10.3390/ijerph16132432
Chicago/Turabian StyleBartelink, Nina, Patricia van Assema, Maria Jansen, Hans Savelberg, and Stef Kremers. 2019. "The Moderating Role of the School Context on the Effects of the Healthy Primary School of the Future" International Journal of Environmental Research and Public Health 16, no. 13: 2432. https://doi.org/10.3390/ijerph16132432