The Effectiveness of Parent Training Programs for Child Maltreatment and Their Components: A Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
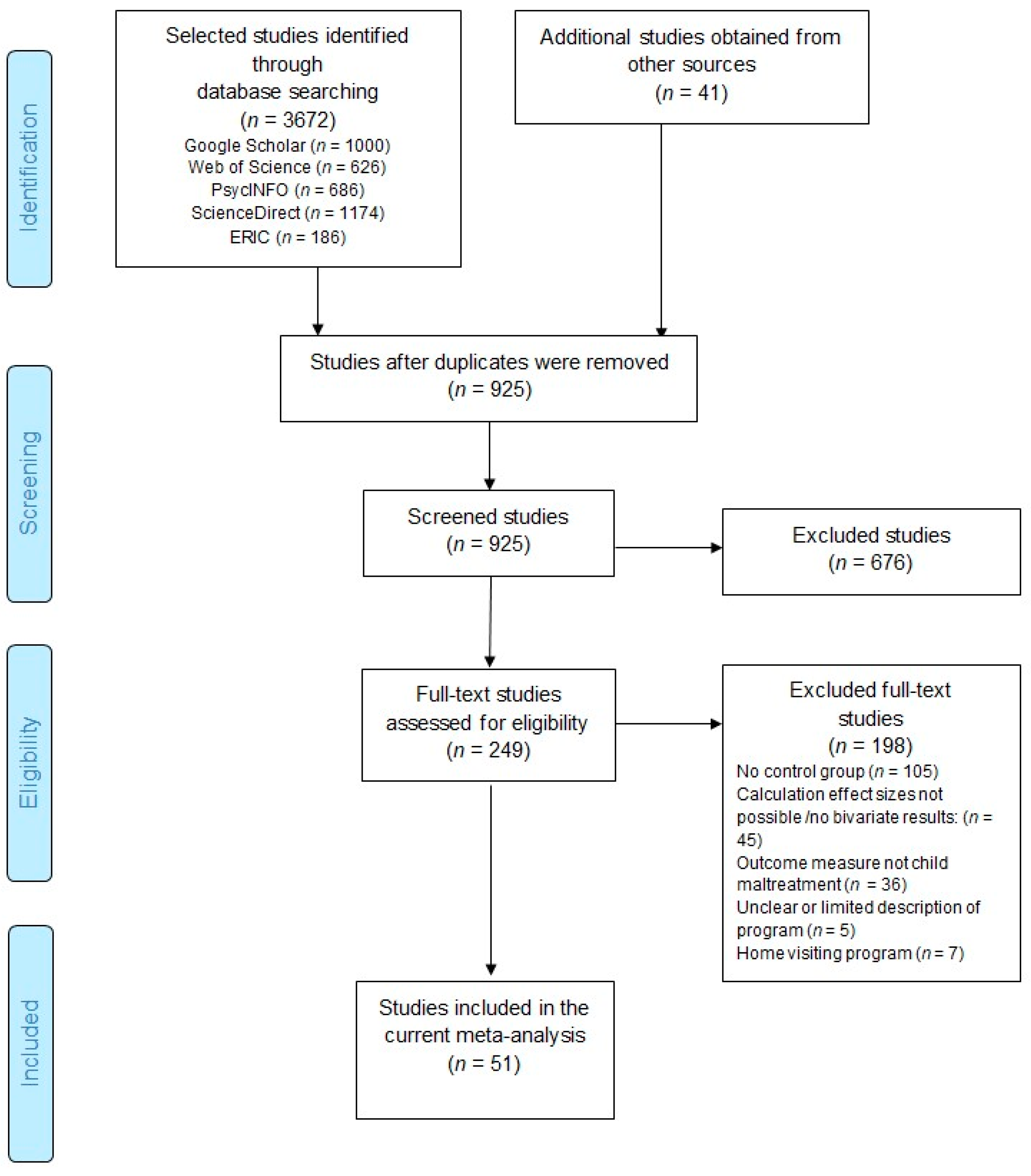
2.2. Selection of Studies
2.3. Coding the Studies
2.4. Calculation of Effect Sizes
2.5. Statistical Analyses
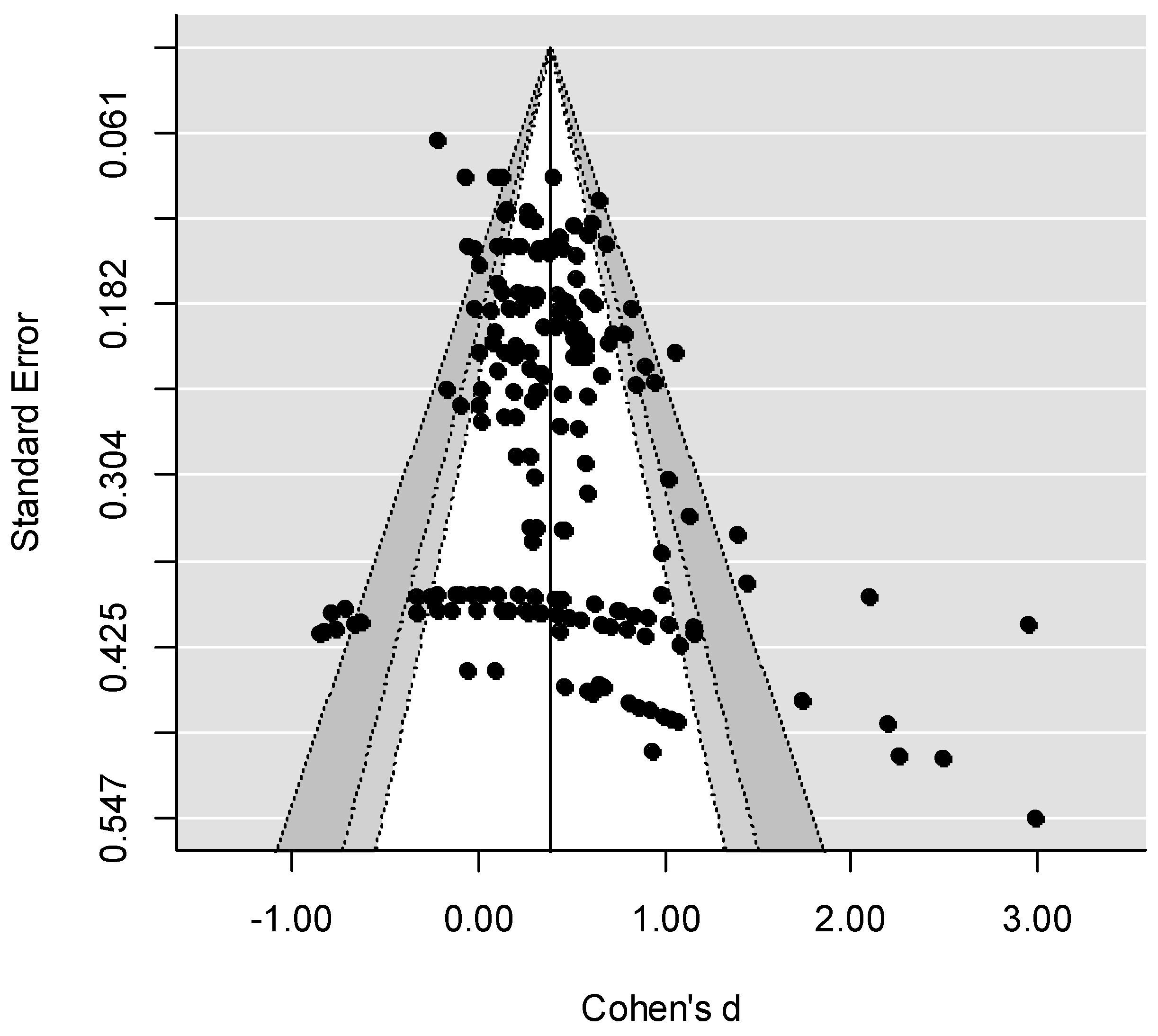
2.6. Bias Assessment
3. Results
3.1. Overall Effect
3.2. Moderator Analyses
3.2.1. Study Design Characteristics
3.2.2. Contextual Factors
3.2.3. Structural Elements
3.2.4. Program Components
3.2.5. Delivery Techniques
4. Discussion
4.1. Study Characteristics
4.2. Contextual Factors, Structural Elements, Program Components, and Techniques
4.3. Limitations
4.4. Implications for Clinical Practice and Future Research
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Author(s) a | Pub. Year | Nb | # ES | Name Program c | Design d | Sample e |
|---|---|---|---|---|---|---|
| Akin et al. [81] | 2017 | 918 | 1 | Parent Management Training Oregon | RCT | R |
| Baker et al. [82] | 2017 | 200 | 6 | Triple P Online Brief | RCT | R |
| Britner & Reppucci [83] | 1997 | 221–438 | 2 | Parent education program for teen mothers | QE | R |
| Calheiros et al. [84] | 2018 | 35 | 2 | Family Support Program | RCT | R |
| Chaffin et al. [24] | 2004 | 68–77 | 4 | PCIT/ Enhanced PCIT | RCT | M |
| Chaffin et al. [85] | 2011 | 76 | 1 | PCIT | RCT | M |
| Chavis et al. [86] | 2016 | 258 | 1 | Play Nicely program | RCT | G |
| Conn et al. [87] | 2018 | 33 | 1 | Incredible Years—trauma-informed version | RCT | R |
| Dawe & Harnett [88] | 2007 | 41–42 | 2 | Brief parenting skills training/PUP | RCT | R |
| Day & Sanders [89] | 2018 | 117–126 | 8 | Triple P Online | RCT | R |
| Feinberg et al. [90] | 2016 | 314 | 2 | Family Foundations | RCT | G |
| Fennell & Fishel [91] | 1998 | 18 | 1 | Systematic Training for Effective Parenting (STEP) | RCT | M |
| Foley et al. [92] | 2016 | 44 | 1 | PCIT | RCT | M |
| Fujiwara et al. [93] | 2011 | 115 | 1 | Group Triple P | QE | R |
| Hurlburt et al. [94] | 2013 | 75–303 | 4 | Incredible Years | RCT | R/M |
| Javier et al. [95] | 2016 | 24 | 1 | Incredible Years | RCT | R |
| Jouriles et al. [96] | 2010 | 35 | 4 | Project Support | RCT | M |
| Kagitcibasi et al. [97] | 2001 | 217–225 | 2 | Turkish Early Enrichment Project (TEEP) | RCT | R |
| Kan & Feinberg [98] | 2014 | 169 | 1 | Family Foundations program | RCT | R |
| Keown et al. [99] | 2018 | 70 | 2 | Te Whānau Pou Toru (culturally adapted version Triple P) | RCT | R |
| Khowaja et al. [100] | 2015 | 50 | 1 | SOS Help for Parents | QE | G |
| Knox et al. [101] | 2011 | 92 | 3 | ACT-Parents Raising Safe Kids | QE | R |
| Knox et al. [21] | 2013 | 84 | 1 | ACT-Parents Raising Safe Kids | RCT | R |
| Kolko [53] | 1996 | 27–30 | 56 | Cognitive Behavioral Therapy/Family Therapy | RCT | M |
| Lachman et al. [102] | 2017 | 68 | 1 | Sinuvuyo Caring Families Program for Young Children | RCT | R |
| Lam et al. [103] | 2009 | 20 | 9 | Parent Skills with Behavioral Couples Therapy (PSBCT) | RCT | R |
| Leijten et al. [104] | 2012 | 78 | 2 | Parents and Children Talking Together | RCT | R |
| Lessard et al. [105] | 2016 | 77 | 6 | Incredible Years plus medication | RCT | R |
| Letarte et al. [106] | 2010 | 35 | 2 | Incredible Years | QE | M |
| Linares et al. [107] | 2006 | 99–108 | 2 | Incredible Years | RCT | M |
| Oveisi et al. [108] | 2010 | 224 | 1 | SOS Helps for Parents | RCT | G |
| Peterson et al. [109] | 2003 | 99 | 4 | 7-level parenting model | QE | R |
| Portwood et al. [20] | 2011 | 156–207 | 2 | ACT-Parents Raising Safe Kids | RCT | R |
| Posthumus et al. [110] | 2012 | 132 | 6 | Incredible Years | QE/M | R |
| Puffer et al. [111] | 2015 | 270 | 1 | Parents Make the Difference | RCT | R |
| Puffer et al. [112] | 2017 | 479 | 4 | Strengthening Families Program | RCT | R |
| Reedtz & Klest [113] | 2016 | 189 | 3 | Incredible Years (shortened version) | RCT | G |
| Rodrigo et al. [114] | 2006 | 290 | 1 | Apoyo Personal y Familiar | QE/M | R |
| Sanders et al. [115] | 2012 | 104 | 6 | Triple P Online | RCT | R |
| Sawasdipanich et al. [116] | 2010 | 116 | 2 | Cognitive adjustment program | RCT | R |
| Schaeffer et al. [117] | 2013 | 43 | 2 | Multisystemic Therapy-Building Stronger Families | QE/M | M |
| Schilling et al. [118] | 2017 | 120 | 1 | PriCARE | RCT | R |
| Scholer et al. [119] | 2010 | 64 | 1 | Play Nicely program | RCT | G |
| Scudder et al. [120] | 2018 | 69 | 2 | PCIT | RCT | R |
| Swenson et al. [121] | 2010 | 86 | 8 | Multisystemic Therapy-Child Abuse and Neglect | RCT | M |
| Szykula & Fleischman [122] | 1985 | 48 | 1 | Social learning treatment | RCT | M |
| Thomas & Zimmer-Gembeck [123] (2) Thomas & Zimmer-Gembeck (2012) [124] | 2011 | 76–198 | 3 | PCIT | RCT | M |
| Van Holen et al. [125] | 2016 | 62 | 2 | NVR treatment program (foster families adaption) | RCT | R |
| Villodas et al. [126] | 2017 | 21 | 4 | Combined PCIT with Motivational Interviewing | RCT | R |
| Wolfe et al. [127] | 1988 | 30 | 1 | Parenting training | QE | R |
References
- Stoltenborgh, M.; Bakermans-Kranenburg, M.J.; Alink, L.R.A.; van Ijzendoorn, M.H. The prevalence of child maltreatment across the globe: Review of a series of meta-analyses. Child Abuse Rev. 2014, 24, 37–50. [Google Scholar] [CrossRef]
- Alink, L.R.A.; Cicchetti, D.; Kim, J.; Rogosch, F.A. Longitudinal associations among child maltreatment, social functioning, and cortisol regulation. Dev. Psychol. 2012, 48, 224–236. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, R.; Spatz Widom, C.; Browne, K.; Fergusson, D.; Webb, E.; Janson, S. Child Maltreatment 1: Burden and consequences of child maltreatment in high-income countries. Lancet 2009, 373, 68–81. [Google Scholar] [CrossRef]
- Jonson-Reid, M.; Kohl, P.L.; Drake, B. Child and adult outcomes of chronic child maltreatment. Pediatrics 2012, 129, 839–845. [Google Scholar] [CrossRef] [PubMed]
- Euser, S.; Alink, L.R.A.; Stoltenborgh, M.; Bakermans-Kranenburg, M.J.; van Ijzendoorn, M.H. A gloomy picture: A meta-analysis of randomized controlled trials reveals disappointing effectiveness of programs aiming at preventing child maltreatment. BMC Public Health 2015, 15, 1–14. [Google Scholar] [CrossRef]
- Geeraerts, L.; van den Noortgate, W.; Grietens, H.; Ongehena, P. The effects of early prevention programs for families with young children at risk for physical child abuse and neglect: A meta-analysis. Child. Maltreat. 2004, 9, 277–291. [Google Scholar] [CrossRef]
- MacLeod, J.; Nelson, G. Programs for the promotion of family wellness and the prevention of child maltreatment: A meta-analytic review. Child. Abuse Negl. 2000, 24, 1127–1149. [Google Scholar] [CrossRef]
- Sweet, M.A.; Appelbaum, M.I. Is home visiting an effective strategy? A meta-analytic review of home visiting programs for families with young children. Child. Dev. 2004, 75, 1435–1456. [Google Scholar] [CrossRef]
- van der Put, C.E.; Assink, M.; Gubbels, J.; Boekhout van Solinge, N.F. Identifying effective components of child Maltreatment interventions: A meta-analysis. Clin. Child Fam. Psychol. Rev. 2018, 21, 171–202. [Google Scholar] [CrossRef]
- Belsky, J. Child maltreatment: An ecological integration. Am. Psychol. 1980, 35, 320–335. [Google Scholar] [CrossRef]
- Belsky, J. Etiology of child maltreatment: A developmental ecological analysis. Psychol. Bull. 1993, 114, 413–434. [Google Scholar] [CrossRef] [PubMed]
- Bronfenbrenner, U. The Ecology of Human Development: Experiments by Nature and Design; Harvard University Press: Cambridge, MA, USA, 1986; ISBN 9780674224575. [Google Scholar]
- Bronfenbrenner, U. Ecology of the family as a context for human development. Am. Psychol. 1986, 32, 513–531. [Google Scholar] [CrossRef]
- Belsky, J. The determinants of parenting: A process model. Child Dev. 1984, 55, 83–96. [Google Scholar] [CrossRef] [PubMed]
- Assink, M.; van der Put, C.E.; Meeuwsen, W.C.M.; de Jong, N.M.; Oort, F.J.; Stams, G.J.J.M.; Hoeve, M. Risk factors for child sexual abuse victimization: A meta-analytic review. Psychol. Bull. 2019, 145, 459–489. [Google Scholar] [CrossRef] [PubMed]
- Mulder, T.M.; Kuiper, K.C.; van der Put, C.E.; Stams, G.J.J.M.; Assink, M. Risk factors for child neglect: A meta-analytic review. Child Abuse Negl. 2018, 77, 198–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stith, S.M.; Liu, T.; Davies, L.C.; Boykin, E.L.; Alder, M.C.; Harris, J.M.; Som, A.; McPherson, M.; Dees, J.E.M.E.G. Risk factors in child maltreatment: A meta-analytic review of the literature. Aggress. Violent Behav. 2009, 14, 13–29. [Google Scholar] [CrossRef] [Green Version]
- Lundahl, B.W.; Nimer, J.; Parsons, B. Preventing child abuse: A meta-analysis of parent training programs. Res. Soc. Work Pract. 2006, 16, 251–262. [Google Scholar] [CrossRef]
- Silva, J. Parents Raising Safe Kids: ACT 8-Week Program for Parents; American Psychological Association: Washington, DC, USA, 2007. [Google Scholar]
- Portwood, S.G.; Lambert, R.; Abrams, L.P.; Nelson, E. An evaluation of the Adults and Children Together (ACT) Against Violence Parents Raising Safe Kids program. J. Prev. 2011, 32, 147–160. [Google Scholar] [CrossRef]
- Knox, M.; Burkhart, K.; Cromley, A. Supporting positive parenting in community health centers: The ACT Raising Safe Kids Program. J. Community Psychol. 2013, 41, 395–407. [Google Scholar] [CrossRef]
- McNeil, C.; Hembree-Kigin, T.L. Parent-Child Interaction Therapy; Springer: New York, NY, USA, 2010; ISBN 978-0-387-88639-8. [Google Scholar]
- Thomas, R.; Abell, B.; Webb, H.J.; Avdagic, E.; Zimmer-Gembeck, M.J. Parent-Child Interaction Therapy: A Meta-analysis. Pediatrics 2017, 140, 1–17. [Google Scholar] [CrossRef]
- Chaffin, M.; Silovsky, J.F.; Funderburk, B.; Valle, L.A.; Brestan, L.V.; Balachova, T.; Jackson, S.; Lensgraf, J.; Bonner, B.L. Parent-Child Interaction Therapy with physically abusive parents: Efficacy for reducing future abuse reports. J. Consult. Clin. Psychol. 2004, 72, 500–510. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Chan, K.L. Effects of parent training programs on child maltreatment prevention: A meta-analysis. Trauma Violence Abuse 2016, 17, 88–104. [Google Scholar] [CrossRef] [PubMed]
- Pinquart, M.; Teubert, D. Effects of parenting education with expectant and new parents: A meta-analysis. J. Fam. Psychol. 2010, 24, 316–327. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum: Hillsdale, MG, USA, 1988; ISBN 9781483276489. [Google Scholar]
- Lundahl, B.W.; Risser, R.M.; Lovejoy, C. A meta-analysis of parent training: Moderators and follow-up effects. Clin. Psychol. Rev. 2006, 26, 86–104. [Google Scholar] [CrossRef] [PubMed]
- Chorpita, B.F.; Daleiden, E.L.; Weisz, J.R. Identifying and selecting the common elements of evidence based interventions: A distillation and matching model. Ment. Health Serv. Res. 2005, 7, 5–20. [Google Scholar] [CrossRef]
- Barth, R.P.; Liggett-Creel, K. Common components of parenting programs for children birth to eight years of age involved with child welfare services. Child. Youth Serv. Rev. 2014, 40, 6–12. [Google Scholar] [CrossRef]
- Blase, K.; Fixsen, D. Core Intervention Components. Identifying and Operationalizing what Makes Programs Work; Office of Human Services Policy, US Department of Health and Human Service: Washington, DC, USA, 2013.
- Temcheffa, C.E.; Letarte, M.-J.; Boutina, S.; Marcil, K. Common components of evidence-based parenting programs for preventing maltreatment of school-age children. Child Abuse Negl. 2018, 80, 226–237. [Google Scholar] [CrossRef]
- Kaminski, J.W.; Valle, L.A.; Filene, J.H.; Boyle, C.L. A meta-analytic review of components associated with parent training program effectiveness. J. Abnorm. Child Psychol. 2008, 36, 567–589. [Google Scholar] [CrossRef]
- Filene, J.H.; Kaminski, J.W.; Valle, L.A.; Cachat, P. Components associated with home visiting program outcomes: A meta-analysis. Pediatrics 2013, 132, 100–109. [Google Scholar] [CrossRef]
- Leeb, R.T.; Paulozzzi, L.; Melanson, C.; Simon, T.; Arias, I. Child Maltreatment Surveillance. Uniform Definitions for Public Health and Recommended Data Elements; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2008. [Google Scholar]
- Batzer, S.; Berg, T.; Godinet, M.T.; Stotzer, R.L. Efficacy or chaos? Parent–Child Interaction Therapy in maltreating populations: A review of research. Trauma Violence Abuse 2018, 19, 3–19. [Google Scholar] [CrossRef]
- Landers, A.L.; McLuckie, A.; Cann, R.; Shapiro, V.; Visintini, S.; MacLaurin, B.; Trocmé, N.; Saini, M.; Carrey, N.J. A scoping review of evidence-based interventions available to parents of maltreated children ages 0-5 involved with child welfare services. Child Abuse Negl. 2018, 76, 546–560. [Google Scholar] [CrossRef] [PubMed]
- Vlahovicova, K.; Melendez-Torres, G.J.; Leijten, P.; Knerr, W.; Gardner, F. Parenting programs for the prevention of child physical abuse recurrence: A systematic review and meta-analysis. Clin. Child Fam. Psychol. Rev. 2018, 20, 351–365. [Google Scholar] [CrossRef] [PubMed]
- Wekerle, C.; Wolfe, D.A. Prevention of child physical abuse and neglect: Promising new directions. Clin. Psychol. Rev. 1993, 13, 501–540. [Google Scholar] [CrossRef]
- Lipsey, M.W.; Wilson, D.B. Practical Meta-Analysis; Sage: Thousand Oaks, CA, USA, 2001; ISBN 9780761921684. [Google Scholar]
- Ferguson, G.A. Statistical Analysis in Psychology & Education; McGraw-Hill: New York, NY, USA, 1966; p. 244. ISBN 9780070204850. [Google Scholar]
- Rosenthal, R. Parametric measures of effect size. In The Handbook of Research Synthesis; Cooper, H., Hedges, L.V., Eds.; Sage: New York, NY, USA, 1994; ISBN 9780871542267. [Google Scholar]
- Durlak, J.A.; Lipsey, M.W. A practitioner’s guide to meta-analysis. Am. J. Community Psychol. 1991, 19, 291–332. [Google Scholar] [CrossRef] [PubMed]
- Van den Noortgate, W.; López-López, J.A.; Marin-Martinez, F.; Sánchez-Meca, J. Three-level meta-analysis of dependent effect sizes. Behav. Res. Methods 2013, 45, 576–594. [Google Scholar] [CrossRef] [PubMed]
- Assink, M.; Wibbelink, C.J.M. Fitting three-level meta-analytic models in R: A step-by-step tutorial. Quant. Method Psychol. 2016, 12, 154–174. [Google Scholar] [CrossRef] [Green Version]
- Cheung, M.W.L. Modeling dependent effect sizes with three-level meta-analyses: A structural equation modeling approach. Psychol. Methods 2014, 19, 211–229. [Google Scholar] [CrossRef] [PubMed]
- Hox, J. Multilevel Analysis: Techniques and Applications; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 2002; ISBN 978-1848728462. [Google Scholar]
- van den Noortgate, W.; López-López, J.A.; Marin-Martinez, F.; Sánchez-Meca, J. Meta-analysis of multiple outcomes: A multilevel approach. Behav. Res. Methods 2015, 47, 1274–1294. [Google Scholar] [CrossRef] [PubMed]
- Viechtbauer, W. Conducting meta-analyses in R with the metaphor package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef]
- Rosenthal, R. Writing meta-analytic reviews. Psychol. Bull. 1995, 118, 183–192. [Google Scholar] [CrossRef]
- Duval, S.; Tweedie, R. A nonparametric ‘trim and fill’ method of accounting for publication bias in meta-analysis. J. Am. Stat. Assoc. 2000, 95, 89–99. [Google Scholar] [CrossRef]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–460. [Google Scholar] [CrossRef] [PubMed]
- Kolko, D.J. Individual cognitive behavioral treatment and family therapy for physically abused children and their offending parents: A comparison of clinical outcomes. Child Maltreat. 1996, 1, 322–342. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Gavaghan, D.; Egger, M. Publication and related bias in meta-analysis: power of statistical tests and prevalence in the literature. J. Clin. Epidemiol. 2000, 53, 1119–1129. [Google Scholar] [CrossRef]
- Kjaergard, L.L.; Villumsen, J.; Gluud, C. Reported methodologic quality and discrepancies between large and small randomized trials in meta-analyses. Ann. Intern. Med. 2001, 135, 982–989. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, S.; Santos, E.S.A. Methodological issues and advances in biological meta-analysis. Evol. Ecol. 2012, 26, 1253–1274. [Google Scholar] [CrossRef]
- Peters, J.L.; Sutton, A.J.; Jones, D.R.; Abrams, K.R.; Rushton, L. Performance of the trim and fill method in the presence of publication bias and between-study heterogeneity. Stat. Med. 2007, 26, 4544–4562. [Google Scholar] [CrossRef]
- Terrin, N.; Schmid, C.H.; Lau, J.; Olkin, I. Adjusting for publication bias in the presence of heterogeneity. Stat. Med. 2003, 22, 2113–2126. [Google Scholar] [CrossRef] [PubMed]
- Brass, C.T.; Nunez-Neto, B.; Williams, E.D. Congress and Program Evaluation: An Overview of Randomized Controlled Trials (RCTs) and Related Issues; Congressional Research Service, Library of Congress: Washington, DC, USA, 2006.
- Shavelson, R.J.; Towne, L. Scientific Research in Education; National Academy Press: Washington, DC, USA, 2002; ISBN 0-309-50953-X. [Google Scholar]
- Jaffee, S.R.; Caspi, A.; Moffitt, T.E.; Taylor, A. Physical maltreatment victim to antisocial child: Evidence of an environmentally mediated process. J. Abnorm. Psychol. 2004, 113, 44–55. [Google Scholar] [CrossRef] [PubMed]
- Teisl, M.; Cicchetti, D. Physical abuse, cognitive and emotional processes, and aggressive/disruptive behavior problems. Soc. Dev. 2008, 17, 1–23. [Google Scholar] [CrossRef]
- Thibodeau, E.L.; Cicchetti, D.; Rogosch, F.A. Child Maltreatment, Impulsivity, and Antisocial Behavior in African-American Children: Moderation Effects from a Cumulative Dopaminergic Gene Index. Dev. Psychopathol. 2015, 27, 1621–1636. [Google Scholar] [CrossRef] [PubMed]
- Busschers, I.; Van Vugt, E.S.; Stams, G.J.J.M. Case management for child protection services: A multi-level evaluation study. Child. Youth Serv. Rev. 2016, 68, 169–177. [Google Scholar] [CrossRef]
- Van Yperen, T.; Van der Steege, M.; Addink, A.; Boendermaker, L. Algemeen en Specifiek Werkzame Factoren in de Jeugdzorg: Stand van de Discussie [Common and Specific Therapeutic Factors in Youth Care: The Current Discussion]; Netherlands Youth Institute: Utrecht, The Netherlands, 2010. [Google Scholar]
- Fryling, M.J.; Wallace, M.D.; Yassine, J.N. Impact of treatment integrity on intervention effectiveness. J. Appl. Behav. Anal. 2012, 45, 449–453. [Google Scholar] [CrossRef] [PubMed]
- Goense, P.G.; Assink, M.; Stams, G.J.J.M.; Boendermaker, L.; Hoeve, M. Making ‘what works’ work: A meta-analytic study of the effect of treatment integrity on outcomes of evidence-based interventions for juveniles with antisocial behavior. Aggress. Violent Behav. 2016, 31, 106–115. [Google Scholar] [CrossRef]
- Karver, M.S.; Handelsman, J.B.; Fields, S.; Bickman, L. Meta-analysis of therapeutic relationship variables in youth and family therapy: the evidence for different relationship variables in the child and adolescent treatment outcome literature. Clin. Psychol. Rev. 2006, 26, 50–65. [Google Scholar] [CrossRef] [PubMed]
- Kazdin, A.E.; Whitley, M.K. Pretreatment social relations, therapeutic alliance, and improvements in parenting practices in parent management training. J. Consult. Clin. Psychol. 2006, 74, 346–355. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, F.; Chomycz, S.; Houlding, C.; Kruse, A.; Franks, J. The association between therapeutic alliance and treatment outcomes in a Group Triple P intervention. J. Child Fam. Stud. 2013, 23, 1337–1350. [Google Scholar] [CrossRef]
- Cyr, K.; Chamberland, C.; Clément, M.; Lessard, G.; Wemmers, J.A.; Collin-Vézina, D.; Gagné, M.-H.; Damant, D. Polyvictimization and victimization of children and youth: Results from a populational survey. Child Abuse Negl. 2013, 37, 814–820. [Google Scholar] [CrossRef]
- Finkelhor, D.; Ormrod, R.K.; Turner, H.A. The victimization of children and youth: A comprehensive, national survey. Child Maltreat. 2005, 10, 5–25. [Google Scholar] [CrossRef]
- Finkelhor, D.; Ormrod, R.K.; Turner, H.A. Lifetime assessment of poly-victimization in a national sample of children and youth. Child Abuse Negl. 2009, 33, 403–411. [Google Scholar] [CrossRef]
- Gill, D.G. Violence Against Children: Physical Abuse in the Unites States; Harvard University Press: Cambridge, MA, USA, 1973; ISBN 9780674187917. [Google Scholar]
- Kadushin, A.; Martin, J.A. Child Abuse: An Interventional Event; Columbia University Press: New York, NY, USA, 1981. [Google Scholar]
- Knox, M. On hitting children: A review of corporal punishment in the United States. J. Pediatr. Health Care 2010, 24, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Straus, M.A. Corporal punishment and primary prevention of physical abuse. Child Abuse Negl. 2000, 24, 1109–1114. [Google Scholar] [CrossRef]
- Lundahl, B.W.; Tollefson, D.; Risser, H.; Lovejoy, M.C.A. Meta-analysis of father involvement in parent training research on social work practice. Res. Soc. Work. Pract. 2008, 18, 97–106. [Google Scholar] [CrossRef]
- Tiano, J.D.; McNeil, C.B. The inclusion of fathers in behavioral parent training: A critical evaluation. Child Fam. Behav. Ther. 2005, 27, 1–28. [Google Scholar] [CrossRef]
- Panter-Brick, C.; Burgess, A.; Eggerman, M.; McAllister, F.; Pruett, K.; Leckman, J.F. Practitioner review: Engaging fathers—Recommendations for a game change in parenting interventions based on a systematic review of the global evidence. J. Child Psychol. Psychiatry 2014, 55, 1187–1212. [Google Scholar] [CrossRef] [PubMed]
- Akin, B.A.; Lang, K.; McDonald, T.P.; Yan, Y.; Little, T. Randomized study of PMTO in foster care: Six-month parent outcomes. Res. Soc. Work. Pract. 2018, 28, 810–826. [Google Scholar] [CrossRef]
- Baker, S.; Sanders, M.R.; Turner, K.M.; Morawska, A. A randomized controlled trial evaluating a low-intensity interactive online parenting intervention, Triple P Online Brief, with parents of children with early onset conduct problems. Behav. Res. Ther. 2017, 91, 78–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Britner, P.A.; Reppucci, N.D. Prevention of child maltreatment: Evaluation of a parent education program for teen mothers. J. Child. Fam. Stud. 1997, 6, 165–175. [Google Scholar] [CrossRef]
- Calheiros, M.M.; Patrício, J.N.; Graça, J.; Magalhães, E. Evaluation of an intervention program for families with children at risk for maltreatment and developmental impairment: A preliminary study. J. Child Fam. Stud. 2018, 27, 1605–1613. [Google Scholar] [CrossRef]
- Chaffin, M.; Funderburk, B.; Bard, D.; Valle, L.A.; Gurwitch, R. A combined motivation and parent–child interaction therapy package reduces child welfare recidivism in a randomized dismantling field trial. J. Consult Clin. Psychol. 2011, 79, 84–95. [Google Scholar] [CrossRef]
- Chavis, A.; Hudnut-Beumler, J.; Webb, M.W.; Neely, J.A.; Bickman, L.; Dietrich, M.S.; Scholer, S.J. A brief intervention affects parents’ attitudes toward using less physical punishment. Child Abuse Negl. 2013, 37, 1192–1201. [Google Scholar] [CrossRef] [PubMed]
- Conn, A.-M.; Szilagyi, M.A.; Alpert-Gillis, L.; Webster-Stratton, C.; Manly, J.T.; Goldstein, N.; Jee, S.H. Pilot randomized controlled trial of foster parent training: A mixed-methods evaluation of parent and child outcomes. Child. Youth Serv. Rev. 2018, 89, 188–197. [Google Scholar] [CrossRef]
- Dawe, S.; Harnett, P. Reducing potential for child abuse among methadone-maintained parents: Results from a randomized controlled trial. J. Subst. Abuse Treat. 2017, 32, 381–390. [Google Scholar] [CrossRef] [PubMed]
- Day, J.J.; Sanders, M.R. Do parents benefit from help when completing a self-guided parenting program online? A randomized controlled trial comparing Triple P Online with and without telephone support. Behav. Ther. 2018, 49, 1020–1038. [Google Scholar] [CrossRef] [PubMed]
- Feinberg, M.E.; Jones, D.E.; Hostetler, M.L.; Roettger, M.E.; Paul, I.M.; Ehrenthal, D.B. Couple-focused prevention at the transition to parenthood, a randomized trial: Effects on coparenting, parenting, family violence, and parent and child adjustment. Prev. Sci. 2016, 17, 751–764. [Google Scholar] [CrossRef]
- Fennell, D.C.; Fishel, A.H. Parent education: an evaluation of STEP on abusive parents’ perceptions and abuse potential. J. Child Adolesc. Psychiatr. Nurs. 1998, 11, 107–120. [Google Scholar] [CrossRef] [PubMed]
- Foley, K.; McNeil, C.B.; Norman, M.; Wallace, N.M. Effectiveness of group format Parent-Child Interaction Therapy compared to treatment as ssual in a community outreach organization. Child Fam. Behav. Ther. 2016, 38, 279–298. [Google Scholar] [CrossRef]
- Fujiwara, T.; Kato, N.; Sanders, M.R. Effectiveness of Group Positive Parenting Program (Triple P) in changing child behavior, parenting style, and parental adjustment: An intervention study in Japan. J. Child Fam. Stud. 2011, 20, 804–813. [Google Scholar] [CrossRef]
- Hurlburt, M.S.; Nguyen, K.; Reid, J.; Webster-Stratton, C.; Zhang, J. Efficacy of the Incredible Years group parent program with families in Head Start who self-reported a history of child maltreatment. Child Abuse Negl. 2013, 37, 531–543. [Google Scholar] [CrossRef]
- Javier, J.R.; Coffey, D.M.; Schrager, S.M.; Palinkas, L.A.; Miranda, J. Parenting Intervention for Prevention of Behavioral Problems in Elementary School-Age Filipino-American Children: A Pilot Study in Churches. J. Dev. Behav. Pediatr. 2016, 37, 737–745. [Google Scholar] [CrossRef]
- Jouriles, E.N.; McDonald, R.; Rosenfield, D.; Spiller, L.; Corbitt-Shindler, D.; Norwood, W.D.; Stephens, N.; Ehrensaft, M. Improving parenting in families peferred for child maltreatment: A randomized controlled trial examining effects of project support. J. Fam. Psychol. 2010, 24, 328–338. [Google Scholar] [CrossRef] [PubMed]
- Kagitcibasi, C.; Sunar, D.; Bekman, S. Long-term effects of early intervention: Turkish low-income mothers and children. J. Appl. Dev. Psychol. 2001, 22, 333–361. [Google Scholar] [CrossRef]
- Kan, M.L.; Feinberg, M.E. Can a Family-Focused, Transition-to-Parenthood Program Prevent Parent and Partner Aggression Among Couples with Young Children? Violence Vict. 2014, 29, 967–980. [Google Scholar] [CrossRef] [PubMed]
- Keown, L.J.; Sanders, M.R.; Franke, N.; Shepherd, M. Te whānau pou toru: A Randomized Controlled Trial (RCT) of a culturally adapted low-intensity variant of the Triple P-Positive Parenting Program for indigenous Māori families in New Zealand. Prev. Sci. 2018, 19, 954–965. [Google Scholar] [CrossRef] [PubMed]
- Khowaja, Y.; Karmaliani, R.; Hirani, S.; Khowaja, A.R.; Rafique, G.; McFarlane, J. A pilot study of a 6-week parenting program for mothers of pre-school children attending family health centers in Karachi, Pakistan. Int. J. Health Policy Manag. 2016, 5, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Knox, M.S.; Burkhart, K.; Hunter, K.E. ACT against Violence Parents Raising Safe Kids Program: Effects on Maltreatment-Related Parenting Behaviors and Beliefs. J. Fam. Issues 2011, 32, 55–74. [Google Scholar] [CrossRef]
- Lachman, J.M.; Cluver, L.; Ward, C.L.; Hutchings, J.; Mlotshwa, S.; Wessels, I.; Gardner, F. Randomized controlled trial of a parenting program to reduce the risk of child maltreatment in South Africa. Child Abuse Negl. 2017, 72, 338–351. [Google Scholar] [CrossRef] [Green Version]
- Lam, W.K.; Fals-Stewart, W.; Kelley, M.L. Parent training with behavioral couples therapy for fathers’ alcohol abuse: Effects on substance use, parental relationships, parenting, and CPS involvement. Child Maltreat 2009, 14, 243–254. [Google Scholar] [CrossRef]
- Leijten, P.; Overbeek, G.; Janssens, J.M.A.M. Effectiveness of a parent training program in (pre)adolescence: Evidence from a randomized controlled trial. J. Adolesc. 2012, 35, 833–842. [Google Scholar] [CrossRef]
- Lessard, J.; Normandeau, S.; Robaey, P. Effects of the Incredible Years program in families of children with ADHD. J. Child Fam. Stud. 2016, 25, 3716–3727. [Google Scholar] [CrossRef]
- Letarte, M.-J.; Normandeau, S.; Allard, J. Effectiveness of a parent training program “Incredible Years” in a child protection service. Child Abuse Negl. 2010, 34, 253–261. [Google Scholar] [CrossRef] [PubMed]
- Linares, O.L.; Montalto, D.; Li, M.; Oza, V.S. A promising parenting intervention in foster care. J. Consult Clin. Psychol. 2006, 74, 32–41. [Google Scholar] [CrossRef] [PubMed]
- Oveisi, S.; Ardabili, H.E.; Dadds, M.R.; Majdzadeh, R.; Mohammadkhani, P.; Rad, J.A.; Shahrivar, Z. Primary prevention of parent-child conflict and abuse in Iranian mothers: A randomized-controlled trial. Child Abuse Negl. 2010, 34, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Peterson, L.; Tremblay, G.; Ewigman, B.; Saldana, L. Multilevel selected primary prevention of child maltreatment. J. Consult. Clin. Psychol. 2003, 71, 601–612. [Google Scholar] [CrossRef] [PubMed]
- Posthumus, J.A.; Raaijmakers, M.A.; Maassen, G.H.; Van Engeland, H.; Matthys, W. Sustained effects of Incredible Years as a preventive intervention in preschool children with conduct problems. J. Abnorm. Child Psychol. 2012, 40, 487–500. [Google Scholar] [CrossRef]
- Puffer, E.S.; Green, E.P.; Chase, R.M.; Sim, A.L.; Zayzay, J.; Friis, E.; Garcia-Rolland, E.; Boone, L. Parents make the difference: A randomized-controlled trial of a parenting intervention in Liberia. Glob. Ment. Health 2015, 2, e15. [Google Scholar] [CrossRef]
- Puffer, E.S.; Annan, J.; Sim, A.L.; Salhi, C.; Betancourt, T.S. The impact of a family skills training intervention among Burmese migrant families in Thailand: A randomized controlled trial. PLoS ONE 2017, 12, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Reedtz, C.; Klest, S. Improved parenting maintained four years following a brief parent training intervention in a non-clinical sample. BMC Psychol. 2016, 4, 1–16. [Google Scholar] [CrossRef]
- Rodrigo, M.J.; Maiquez, M.L.; Correa, A.D.; Martin, J.C.; Rodriguez, G. Outcome Evaluation of a Community Center-Based Program for Mothers at High Psychosocial Risk. Child Abuse Negl. 2006, 30, 1049–1064. [Google Scholar] [CrossRef]
- Sanders, M.R.; Baker, S.; Turner, K.M.T. A randomized controlled trial evaluating the efficacy of Triple P Online with parents of children with early-onset conduct problems. Behav. Res. Ther. 2012, 50, 675–684. [Google Scholar] [CrossRef]
- Sawasdipanich, N.; Srisuphan, W.; Yenbut, J.; Tiansawad, S.; Humphreys, J. Effects of a cognitive adjustment program for Thai parents. Nurs. Health Sci. 2010, 12, 306–313. [Google Scholar] [CrossRef] [PubMed]
- Schaeffer, C.M.; Swenson, C.C.; Tuerk, E.H.; Henggeler, S.W. Comprehensive treatment for co-occurring child maltreatment and parental substance abuse: Outcomes from a 24-month pilot study of the MST-Building Stronger Families program. Child Abuse Negl. 2013, 37, 596–607. [Google Scholar] [CrossRef] [PubMed]
- Schilling, S.; French, B.; Berkowitz, S.J.; Dougherthy, S.L.; Scribano, P.; Wood, J.N. Child–Adult Relationship Enhancement in Primary Care (PriCARE): A Randomized Trial of a Parent Training for Child Behavior Problems. Acad. Pediatr. 2017, 17, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Scholer, S.J.; Hamilton, E.C.; Johnson, M.C.; Scott, T.A. A brief intervention may affect parents’ attitudes toward using less physical punishment. Fam. Community Health 2010, 33, 106–116. [Google Scholar] [CrossRef] [PubMed]
- Scudder, A.T.; McNeil, C.B.; Chengappa, K.; Costello, A.H. Evaluation of an existing parenting class within a women’s state correctional facility and a parenting class modeled from Parent–Child Interaction Therapy. Child. Youth Serv. Rev. 2014, 46, 238–247. [Google Scholar] [CrossRef]
- Swenson, C.C.; Schaeffer, C.M.; Henggler, S.W.; Faldowski, R. Multisystemic therapy for child abuse and neglect: A randomized effectiveness trial. J. Fam. Psychol. 2010, 24, 497–507. [Google Scholar] [CrossRef] [PubMed]
- Szykula, S.A.; Fleischman, M.J. Reducing out-of-home placements of abused children: Two controlled field studies. Child Abuse Negl. 1985, 9, 277–283. [Google Scholar] [CrossRef]
- Thomas, R.; Zimmer-Gembeck, M.J. Accumulating Evidence for Parent–Child Interaction Therapy in the Prevention of Child Maltreatment. Child Dev. 2011, 82, 177–192. [Google Scholar] [CrossRef]
- Thomas, R.; Zimmer-Gembeck, M.J. Parent–Child Interaction Therapy: An Evidence-Based Treatment for Child Maltreatment. Child Maltreat. 2012, 17, 253–266. [Google Scholar] [CrossRef]
- Van Holen, F.; Vanderfaeillie, J.; Omer, H.; Vanschoonlandt, F. Training in Nonviolent Resistance for Foster Parents: A Randomized Controlled Trial. Res. Soc. Work Pract. 2016, 1–12. [Google Scholar] [CrossRef]
- Villodas, M.T.; Bagner, D.M.; Villodas, F.M.; Huang, H. An Evidence-Based Parent-Child Relational Intervention for Young Children At-Risk for Abuse and Neglect; Florida Institute for Child Welfare: Miami, FL, USA, 2017. [Google Scholar]
- Wolfe, D.A.; Edwards, B.; Manion, I.; Koverola, C. Early intervention for parents at risk of child abuse and neglect: A preliminary investigation. J. Consult Clin. Psychol. 1988, 56, 40–47. [Google Scholar] [CrossRef] [PubMed]


| Program Components | % | Description |
|---|---|---|
| (1) Parent-child relationship in general | 83.8 | Improving parental skills regarding the parent-child relationship (including program components 2–5). |
| (2) Parent-child communication | 64.9 | Improving the communicative skills of parents in interaction with their child, and learning parents to interact in a positive way with their child. |
| (3) Affection, sensitivity, and/or responsivity | 24.9 | Improving affective behavior of parents towards their child, such as holding and cuddling their child, and responding sensitively to the child’s emotional and psychological needs. |
| (4) Quality time | 14.1 | Encouraging parents to spend quality time with the child, i.e., playing with the child, and doing fun activities together. |
| (5) Parent-child attachment | 13.5 | Stimulating a safe parent-child attachment. |
| (6) Disciplining skills in general | 97.8 | Improving parental skills regarding disciplining the child (including program components 7–12). |
| (7) Clear rules/consequences | 50.3 | Improving parental disciplinary communication skills, such as giving clear directions, setting limits and rules, and stating behavioral expectations and consequences. |
| (8) Time-out | 58.9 | Encouraging parents to use time-out as a disciplinary technique. |
| (9) Planned ignoring | 62.7 | Encouraging parents to ignore certain ‘bad’ or attention-seeking behaviors of their child as a disciplinary technique. |
| (10) Positive reinforcement | 70.3 | Encouraging parents to use positive reinforcement, such as praise and rewards, and to reinforce ‘good’ or prosocial behaviors of the child. |
| (11) Negative punishment | 48.6 | Encouraging parents to use negative consequences for ‘bad’ behavior of the child, such as taking away privileges, as a disciplinary technique. |
| (12) Alternatives for negative/physical discipline | 70.3 | Encouraging parents to use alternative parenting techniques for their negative parenting or physical discipline. |
| (13) Parental personal skills in general | 95.1 | All parental personal skills (including program components 14–20). |
| (14) Problem solving | 64.9 | Improving parental problem-solving skills. |
| (15) Stress management | 23.2 | Applying stress management strategies, such as meditation and other relaxation exercises, in order to reduce parental stress. |
| (16) Anger management | 47.6 | Applying anger/emotion management strategies, such as calming down, in order to reduce parental anger towards the child. |
| (17) Goal setting | 20.0 | Encouraging parents to select goals that are based on their own values, beliefs, and traditions. |
| (18) Cognitive skills | 31.4 | Improving cognitive (behavioral) skills of parents, including effective coping strategies. |
| (19) Listening skills | 15.7 | Stimulating parental attentive and active listening to their child. |
| (20) Being a role model | 26.5 | Encouraging parents to be a good role model for their child. |
| (21) Components regarding the stimulation of children’s skills | 88.8 | Encouraging parents to stimulate all skills of children (including program component 22–24). |
| (22) Pro-social/less anti-social behavior | 64.9 | Encouraging parents to stimulate pro-social behavior of children or to discourage anti-social behavior. |
| (23) Social skills | 46.5 | Stimulating the development of social skills of children, such as playing with others and cooperating. |
| (24) Cognitive/academic skills | 23.2 | Stimulating the development of cognitive/academic skills of children, such as language development and school success. |
| Other components | ||
| (25) Supervision | 13.5 | Improving monitoring and supervising practices of parents. |
| (26) Consistency | 22.7 | Encouraging parents to react on certain child behaviors in a consistent manner. |
| (27) Calm, clear language, positive tone | 14.1 | Encouraging parents to stay calm, use clear language, and/or a positive tone when giving instructions to their child. |
| (28) Anticipating ‘high-risk’ situations | 14.6 | Encouraging parents to identify and anticipate on high-risk situations (i.e., situations in which there is a high risk of parenting problems or child abuse, such as during shopping), for example by setting up a prevention plan. |
| (29) Knowledge of child/development | 42.7 | Improving parental knowledge of their child’s developmental stages, and their child’s behavior and needs so that parents are able to provide developmentally appropriate physical care and to foster their child’s positive social-emotional development. |
| (30) Attitudes | 15.7 | Decreasing parental negative attitudes/attribution towards parenting, their child, or their child’s behavior, for example by using attributional retraining. |
| (31) Expectations | 43.8 | Improving realistic expectations/beliefs of parents regarding their child and/or parenting. |
| (32) Relation/collaboration parents | 40.5 | Improving the relationship and cooperation between parents, for example by stimulating that parents support each other if their child behaves problematic, and by giving and receiving constructive feedback. Also addressing marital problems or partner issues can be addressed. |
| (33) Parental competence/empowerment | 37.8 | Empowering parents and increasing their sense of self-esteem and competence regarding parenting. |
| (34) Social network | 20.5 | Helping parents to create a strong social network and to increase their involvement with the community, such as the school their child is attending. |
| Delivery techniques | ||
| (1) Modelling | 47.0 | Giving live demonstrations of proper parenting behaviors or other forms of proper behavior. |
| (2) Role-playing | 40.0 | Practicing skills in program sessions by role-playing, either with the trainer or a peer (in a parenting group). |
| (3) Practice and rehearsal | 69.7 | Practicing skills (with a child) in the program sessions by rehearsal and direct feedback of the trainer. |
| (4) Video-feedback | 0.5 | Video-recording of parenting skills or parent-child interactions, so that the trainer has the opportunity to give feedback on video-recorded behavior and that parents can critique their own behavior. |
| (5) Homework assignments | 70.8 | Written, verbal, or behavioral assignments that are to be complete between sessions, including keeping a diary or practicing skills at home. |
| (6) (Group) discussion | 67.0 | Discussing parenting skills, either with an individual parent or in a group. |
| (7) CBT techniques for parents | 11.9 | Using cognitive behavioral therapy techniques (i.e., cognitive restructuring) or mindfulness techniques. |
| (8) Services for children | 13.0 | Having a child participate in a behavioral, social, cognitive, or social skills training separately from the parent. |
| (9) Additional services for parents | 17.8 | Providing additional services for parents which are not specifically aimed at improving parenting skills, such as offering social support and/or practical support, or referring parents for mental health or addiction problems. |
| Overall Effect | # Studies | # ES | Mean d (SE) | 95% CI | Sig. Mean d (p) | % Var. at Level 1 | Level 2 Variance | % Var. at Level 2 | Level 3 Variance | % Var. at Level 3 |
|---|---|---|---|---|---|---|---|---|---|---|
| Overall effect | 50 | 185 | 0.416 (0.042) *** | (0.334, 0.498) | <0.0010 *** | 33.3 | 0.053 *** | 39.3 | 0.037 * | 27.4 |
| Overall effect without Kolko [53] | 49 | 129 | 0.425 (0.047) *** | (0.331, 0.518) | <0.0010 *** | 28.6 | 0.012 * | 9.9 | 0.074 *** | 61.5 |
| Moderator Variables | # Studies | # ES | Intercept/Mean d (95% CI) | β1(95% CI) | F (df1, df2) ᵃ | p ᵇ | Level 2 Variance | Level 3 Variance |
|---|---|---|---|---|---|---|---|---|
| Overall Effect | 50 | 185 | 0.416 (0.334, 0.498) *** | 0.232 *** | 0.193 * | |||
| A: Study characteristics | ||||||||
| Publication year | 50 | 185 | 0.449 (0.355, 0.544) *** | −0.009 (−0.021, 0.003) | 1.968 (1, 183) | 0.162 | 0.051 *** | 0.037 ** |
| Sample characteristics | ||||||||
| Type of sample | 0.623 (2, 182) | 0.537 | 0.051 *** | 0.044 * | ||||
| Risk group (RC) | 32 | 89 | 0.419 (0.314, 0.525) *** | |||||
| General sample | 6 | 9 | 0.543 (0.278, 0.808) *** | 0.124 (−0.162, 0.409) | ||||
| Maltreating sample | 13 | 87 | 0.365 (0.196, 0.534) *** | −0.054 (−0.250, 0.142) | ||||
| Sample size | 50 | 185 | 0.448 (0.370, 0.525) *** | −0.001 (−0.001, −0.000) ** | 69.058 (1, 183) | 0.003 ** | 0.052 *** | 0.022 * |
| Age category child | ||||||||
| Unborn child/baby (≤2) | 0.026 (1, 182) | 0.872 | 0.052 *** | 0.043 * | ||||
| No (RC) | 35 | 153 | 0.428 (0.326, 0.529) *** | |||||
| Yes | 14 | 31 | 0.412 (0.249, 0.575) *** | −0.016 (−0.207, 0.176) | ||||
| Infant/toddler (2-5) | 0.248 (1, 182) | 0.619 | 0.051 *** | 0.044 * | ||||
| No (RC) | 13 | 96 | 0.391 (0.235, 0.556) *** | |||||
| Yes | 36 | 88 | 0.438 (0.334, 0.542) *** | 0.047 (−0.140, 0.234) | ||||
| Primary school (6-12) | 1.809 (1, 182) | 0.180 | 0.051 *** | 0.042 * | ||||
| No (RC) | 11 | 26 | 0.530 (0.351, 0.709) *** | |||||
| Yes | 38 | 158 | 0.391 (0.294, 0.488) *** | −0.139 (−0.342, 0.065) | ||||
| High school (≥12) | 2.616 (1, 182) | 0.108 | 0.052 *** | 0.035 * | ||||
| No (RC) | 41 | 108 | 0.452 (0.361, 0.542) *** | |||||
| Yes | 8 | 76 | 0.282 (0.095, 0.469) *** | −0.170 (−0.378, 0.037) | ||||
| Age of child (average) | 39 | 164 | 0.419 (0.303, 0.534) *** | −0.017 (−0.049, 0.015) | 1.109 (1, 162) | 0.294 | 0.056 *** | 0.067 * |
| Age of the parent(s) (average) | 46 | 126 | 0.420 (0.324, 0.516) *** | −0.016 (−0.033, 0.001) + | 3.621 (1, 124) | 0.059 + | 0.012 * | 0.072 *** |
| Percentage cultural minorities | 29 | 136 | 0.401 (0.318, 0.484) *** | 0.042 (−0.254, 0.337) | 0.077 (1, 134) | 0.781 | 0.087 *** | 0.005 |
| Design characteristics | ||||||||
| Research design | 6.770 (2, 182) | 0.001 ** | 0.047 *** | 0.029 | ||||
| RCT (RC) | 40 | 162 | 0.358 (0.274, 0.441) *** | |||||
| Quasi-experimental, matched | 3 | 9 | 0.388 (0.094, 0.683) * | 0.031 (−0.276, 0.337) | ||||
| Quasi-experimental, not matched | 7 | 14 | 0.805 (0.580, 1.031) *** | 0.448 (0.207, 0.688) *** | ||||
| Intent-to-treat design | 2.320 (1, 183) | 0.129 | 0.050 *** | 0.040 ** | ||||
| No (RC) | 23 | 99 | 0.495 (0.364, 0.626) *** | |||||
| Yes | 27 | 86 | 0.364 (0.257, 0.472) *** | −0.131 (−0.300, 0.039) | ||||
| Min. 12 month follow-up | 0.542 (1, 183) | 0.463 | 0.053 *** | 0.038 * | ||||
| No (RC) | 38 | 91 | 0.396 (0.297, 0.495) *** | |||||
| Yes | 12 | 94 | 0.463 (0.313, 0.614) *** | 0.067 (−0.113, 0.247) | ||||
| Study quality index (numerical score combining previous three variables) | 50 | 185 | 0.396 (0.313, 0.478) *** | −0.112 (−0.195, −0.030) ** | 7.264 (1, 183) | 0.008 ** | 0.047 *** | 0.037 * |
| Control group | 0.683 (3, 176) | 0.564 | 0.054 *** | 0.046 * | ||||
| Treatment as usual (TAU; RC) | 28 | 120 | 0.424 (0.299, 0.549) *** | |||||
| No treatment | 4 | 11 | 0.493 (0.219, 0.768) *** | 0.070 (−0.232, 0.371) | ||||
| Waiting list | 12 | 35 | 0.318 (0.144, 0.492) *** | −0.106 (−0.321, 0.108) | ||||
| Other | 7 | 11 | 0.507 (0.262, 0.752) *** | 0.083 (−0.192, 0.358) | ||||
| Outcome characteristics | ||||||||
| Assessment type | 2.062 (3, 181) | 0.107 | 0.049 *** | 0.036 + | ||||
| Self-report parents (RC) | 44 | 137 | 0.391 (0.305, 0.477) *** | |||||
| Official reports | 9 | 15 | 0.646 (0.428, 0.865) *** | 0.255 (0.030, 0.481) * | ||||
| Observations | 3 | 8 | 0.462 (0.143, 0.782) ** | 0.071 (−0.256, 0.398) | ||||
| Child-report | 4 | 25 | 0.316 (0.124, 0.508) ** | −0.075 (−0.261, 0.110) | ||||
| Follow-up duration (in months) | 27 | 96 | 0.446 (0.345, 0.547) *** | 0.002 (−0.006, 0.009) | 0.195 (1, 94) | 0.660 | 0.062 ** | 0.016 |
| B: Contextual factors | ||||||||
| General aim of the program | 0.558 (1, 183) | 0.456 | 0.053 *** | 0.038 * | ||||
| Prevention (RC) | 38 | 98 | 0.434 (0.339, 0.529) *** | |||||
| Reduction | 13 | 87 | 0.364 (0.200, 0.527) *** | −0.071 (−0.257, 0.116) | ||||
| Delivery location | ||||||||
| Home/ambulant | 0.267 (1, 183) | 0.606 | 0.052 *** | 0.041 * | ||||
| No (RC) | 30 | 73 | 0.436 (0.325, 0.547) *** | |||||
| Yes | 21 | 112 | 0.393 (0.267, 0.519) *** | −0.043 (−0.209, 0.122) | ||||
| Treatment center | 0.478 (1, 183) | 0.490 | 0.052 *** | 0.041 * | ||||
| No (RC) | 13 | 44 | 0.468 (0.302, 0.633) *** | |||||
| Yes | 37 | 141 | 0.400 (0.302, 0.499) *** | −0.067 (−0.260, 0.125) | ||||
| By telephone | 0.711 (1, 183) | 0.400 | 0.048 *** | 0.045 * | ||||
| No (RC) | 47 | 177 | 0.411 (0.324, 0.498) *** | |||||
| Yes | 4 | 8 | 0.531 (0.254, 0.808) *** | 0.120 (−0.160, 0.400) | ||||
| Online | 0.214 (1, 183) | 0.644 | 0.051 *** | 0.043 * | ||||
| No (RC) | 47 | 165 | 0.425 (0.335, 0.515) *** | |||||
| Yes | 3 | 20 | 0.359 (0.090, 0.627) ** | −0.066 (−0.349, 0.217) | ||||
| Other | 1.203 (1, 183) | 0.274 | 0.029 *** | 0.042 * | ||||
| No (RC) | 46 | 170 | 0.403 (0.315, 0.491) *** | |||||
| Yes | 6 | 15 | 0.550 (0.297, 0.7803) *** | 0.147 (−0.117, 0.411) | ||||
| Delivery setting | ||||||||
| Only parent(s) | 0.484 (1, 181) | 0.487 | 0.054 *** | 0.042 * | ||||
| No (RC) | 36 | 134 | 0.403 (0.302, 0.505) *** | |||||
| Yes | 12 | 49 | 0.471 (0.309, 0.632) *** | 0.067 (−0.124, 0.258) | ||||
| Both parent(s) and child | 1.263 (1, 181) | 0.263 | 0.053 *** | 0.041 * | ||||
| No (RC) | 32 | 112 | 0.451 (0.351, 0.552) *** | |||||
| Yes | 17 | 71 | 0.368 (0.240, 0.495) *** | −0.084 (−0.231, 0.063) | ||||
| Parent group (without children) | 0.227 (1, 181) | 0.634 | 0.052 *** | 0.045 * | ||||
| No (RC) | 20 | 94 | 0.404 (0.284, 0.523) *** | |||||
| Yes | 29 | 89 | 0.439 (0.331, 0.547) *** | 0.035 (−0.110, 0.180) | ||||
| C: Structural elements | ||||||||
| Duration | 0.235 (2, 182) | 0.790 | 0.050 *** | 0.046 * | ||||
| 13–24 weeks (RC) | 10 | 85 | 0.364 (0.182, 0.546) *** | |||||
| 0–12 weeks | 30 | 70 | 0.432 (0.318, 0.546) *** | 0.068 (−0.147, 0.283) | ||||
| >24 weeks | 11 | 30 | 0.444 (0.259, 0.629) *** | 0.080 (−0.180, 0.339) | ||||
| Minimum duration (in weeks) | 22 | 65 | 0.450 (0.319, 0.582) *** | 0.004 (−0.011, 0.018) | 0.247 (1, 63) | 0.621 | 0.006 | 0.056 ** |
| Maximum duration (in weeks) | 47 | 181 | 0.409 (0.330, 0.488) *** | 0.000 (−0.004, 0.005) | 0.035 (1, 179) | 0.851 | 0.065 *** | 0.024 + |
| Average number of sessions | 33 | 88 | 0.346 (0.260, 0.432) *** | 0.003 (−0.004, 0.010) | 0.671 (1, 86) | 0.415 | 0.015 ** | 0.030 * |
| Interval sessions | 1.059 (3, 154) | 0.368 | 0.110 *** | 0.000 | ||||
| Weekly (RC) | 28 | 116 | 0.363 (0.282, 0.445) *** | |||||
| Multiple sessions a week | 8 | 31 | 0.511 (0.358, 0.664) *** | 0.148 (−0.025, 0.322) + | ||||
| Every other week/monthly | 3 | 6 | 0.489 (0.163, 0.816) ** | 0.126 (−0.210, 0.463) | ||||
| Ascending/descending intensity | 2 | 5 | 0.371 (−0.004, 0.746) + | 0.008 (−0.376, 0.392) | ||||
| D: Program components | ||||||||
| Parent-child relationship in general | 2.371 (1, 183) | 0.125 | 0.052 *** | 0.037 ** | ||||
| No (RC) | 3 | 30 | 0.583 (0.354, 0.813) *** | |||||
| Yes | 49 | 155 | 0.410 (0.327, 0.482) *** | −0.173 (−0.395, 0.049) | ||||
| Parent-child communication | 0.002 (1, 183) | 0.969 | 0.053 *** | 0.040 * | ||||
| No (RC) | 19 | 65 | 0.419 (0.294, 0.544) *** | |||||
| Yes | 32 | 120 | 0.416 (0.318, 0.514) *** | −0.003 (−0.148, 0.142) | ||||
| Affection, sensitivity, and/or responsivity | 1.417 (1, 183) | 0.235 | 0.053 *** | 0.037 * | ||||
| No (RC) | 33 | 136 | 0.453 (0.351, 0.556) *** | |||||
| Yes | 18 | 46 | 0.350 (0.213, 0.487) *** | −0.103 (−0.274, 0.068) | ||||
| Quality time | 3.168 (1, 183) | 0.077 + | 0.052 *** | 0.034 * | ||||
| No (RC) | 41 | 159 | 0.382 (0.294, 0.470) *** | |||||
| Yes | 10 | 26 | 0.574 (0.380, 0.769) *** | 0.193 (−0.021, 0.406) + | ||||
| Parent-child attachment | 1.016 (1, 183) | 0.315 | 0.053 *** | 0.038 * | ||||
| No (RC) | 38 | 126 | 0.439 (0.345, 0.533) *** | |||||
| Yes | 13 | 25 | 0.338 (0.164, 0.513) *** | −0.101 (−0.299, 0.097) | ||||
| Disciplining skills | 0.005 (1, 183) | 0.946 | 0.053 *** | 0.041 * | ||||
| No (RC) | 2 | 4 | 0.432 (0.004, 0.861) * | |||||
| Yes | 48 | 181 | 0.417 (0.331, 0.503) *** | −0.015 (−0.452, 0.422) | ||||
| Clear rules/consequences | 0.006 (1, 183) | 0.940 | 0.052 *** | 0.041 * | ||||
| No (RC) | 17 | 92 | 0.422 (0.279, 0.564) *** | |||||
| Yes | 34 | 93 | 0.415 (0.311, 0.520) *** | −0.007 (−0.183, 0.170) | ||||
| Time-out | 1.054 (1, 183) | 0.306 | 0.051 *** | 0.043 * | ||||
| No (RC) | 22 | 76 | 0.377 (0.260, 0.493) *** | |||||
| Yes | 30 | 109 | 0.450 (0.345, 0.556) *** | 0.074 (−0.068, 0.216) | ||||
| Planned ignoring | 0.148 (1, 183) | 0.701 | 0.051 *** | 0.042 * | ||||
| No (RC) | 21 | 69 | 0.401 (0.280, 0.522) *** | |||||
| Yes | 30 | 116 | 0.429 (0.327, 0.530) *** | 0.028 (−0.116, 0.171) | ||||
| Positive reinforcement | 0.556 (1, 183) | 0.457 | 0.051 *** | 0.043 * | ||||
| No (RC) | 13 | 55 | 0.374 (0.231, 0.518) *** | |||||
| Yes | 39 | 130 | 0.433 (0.339, 0.527) *** | 0.059 (−0.096, 0.214) | ||||
| Negative punishment | 0.025 (1, 183) | 0.875 | 0.054 *** | 0.038 * | ||||
| No (RC) | 29 | 95 | 0.422 (0.318, 0.526) *** | |||||
| Yes | 22 | 90 | 0.410 (0.297, 0.524) *** | −0.011 (−0.151, 0.129) | ||||
| Alternatives for negative/physical discipline | 1.588 (1, 183) | 0.209 | 0.052 *** | 0.040 * | ||||
| No (RC) | 20 | 55 | 0.485 (0.350, 0.620) *** | |||||
| Yes | 31 | 130 | 0.375 (0.268, 0.482) *** | −0.110 (−0.281, 0.062) | ||||
| Personal skills of parents | 10.520 (1, 183) | 0.001 ** | 0.056 *** | 0.022 + | ||||
| No (RC) | 6 | 9 | 0.816 (0.558, 1.075) *** | |||||
| Yes | 45 | 176 | 0.373 (0.297, 0.450) *** | −0.443 (−0.713, 0.174) ** | ||||
| Problem solving | 4.195 (1, 183) | 0.042 * | 0.047 *** | 0.042 ** | ||||
| No (RC) | 22 | 65 | 0.512 (0.388, 0.637) *** | |||||
| Yes | 29 | 120 | 0.363 (0.265, 0.462) *** | −0.149 (−0.293, −0.005) * | ||||
| Stress management | 1.431 (1, 183) | 0.233 | 0.053 *** | 0.037 * | ||||
| No (RC) | 34 | 142 | 0.451 (0.351, 0.551) *** | |||||
| Yes | 17 | 43 | 0.345 (0.203, 0.488) *** | −0.106 (−0.280, 0.069) | ||||
| Anger management | 2.631 (1, 183) | 0.107 | 0.056 *** | 0.027 * | ||||
| No (RC) | 27 | 97 | 0.464 (0.364, 0.564) *** | |||||
| Yes | 25 | 88 | 0.355 (0.273, 0.500) *** | −0.109 (−0.241, 0.024) | ||||
| Goal setting | 0.353 (1, 183) | 0.553 | 0.052 *** | 0.040 * | ||||
| No (RC) | 40 | 148 | 0.432 (0.335, 0.528) *** | |||||
| Yes | 11 | 37 | 0.374 (0.206, 0.541) *** | −0.058 (−0.251, 0.125) | ||||
| Cognitive skills | 0.423 (1, 183) | 0.516 | 0.052 *** | 0.042 * | ||||
| No (RC) | 39 | 127 | 0.405 (0.312, 0.498) *** | |||||
| Yes | 14 | 58 | 0.456 (0.313, 0.598) *** | 0.051 (−0.103, 0.205) | ||||
| Listening skills | 0.791 (1, 183) | 0.375 | 0.053 *** | 0.039 * | ||||
| No (RC) | 39 | 156 | 0.437 (0.343, 0.530) *** | |||||
| Yes | 11 | 29 | 0.344 (0.162, 0.526) *** | −0.092 (−0.297, 0.113) | ||||
| Being a role model | 0.667 (1, 183) | 0.415 | 0.054 *** | 0.040 * | ||||
| No (RC) | 33 | 136 | 0.444 (0.338, 0.550) *** | |||||
| Yes | 17 | 49 | 0.372 (0.234, 0.510) *** | −0.072 (−0.246, 0.102) | ||||
| Skills of children | 2.232 (1, 183) | 0.137 | 0.051 *** | 0.041 * | ||||
| No (RC) | 40 | 21 | 0.547 (0.356, 0.738) *** | |||||
| Yes | 11 | 164 | 0.386 (0.292, 0.480) *** | −0.161 (−0.374, 0.052) | ||||
| Pro-social/less anti-social behavior | 5.134 (1, 183) | 0.025 * | 0.049 *** | 0.039 ** | ||||
| No (RC) | 18 | 65 | 0.527 (0.400, 0.655) *** | |||||
| Yes | 33 | 120 | 0.361 (0.266, 0.457) *** | −0.166 (−0.311, 0.021) * | ||||
| Social skills | 0.015 (1, 183) | 0.903 | 0.053 *** | 0.040 * | ||||
| No (RC) | 30 | 99 | 0.413 (0.309, 0.518) *** | |||||
| Yes | 21 | 86 | 0.422 (0.307, 0.537) *** | 0.009 (−0.142, 0.150) | ||||
| Cognitive/academic skills | 0.759 (1, 183) | 0.759 | 0.051 *** | 0.041 * | ||||
| No (RC) | 34 | 142 | 0.443 (0.341, 0.545) *** | |||||
| Yes | 16 | 43 | 0.364 (0.216, 0.511) *** | −0.079 (−0.258, 0.100) | ||||
| Other components | ||||||||
| Supervision | 1.107 (1, 183) | 0.294 | 0.048 *** | 0.046 * | ||||
| No (RC) | 39 | 160 | 0.442 (0.346, 0.539) *** | |||||
| Yes | 11 | 25 | 0.329 (0.141, 0.518) *** | −0.113 (−0.324, 0.099) | ||||
| Consistency | 2.424 (1, 183) | 0.121 | 0.051 *** | 0.036 * | ||||
| No (RC) | 39 | 143 | 0.459 (0.361, 0.557) *** | |||||
| Yes | 11 | 42 | 0.321 (0.176, 0.465) *** | −0.138 (−0.312, 0.037) | ||||
| Calm, clear language, positive tone | 1.197 (1, 183) | 0.275 | 0.052 *** | 0.040 * | ||||
| No (RC) | 42 | 159 | 0.439 (0.336, 0.531) *** | |||||
| Yes | 8 | 26 | 0.317 (−0.098, 0.340) ** | −0.121 (−0.340, 0.098) | ||||
| Anticipating ‘high-risk’ situation | 0.008 (1, 183) | 0.927 | 0.052 *** | 0.042 * | ||||
| No (RC) | 43 | 158 | 0.420 (0.327, 0.513) *** | |||||
| Yes | 7 | 27 | 0.409 (0.206, 0.613) *** | −0.010 (−0.234, 0.213) | ||||
| Knowledge of child/development | 0.431 (1, 183) | 0.512 | 0.052 *** | 0.042 * | ||||
| No (RC) | 16 | 106 | 0.458 (0.312, 0.603) *** | |||||
| Yes | 35 | 79 | 0.398 (0.294, 0.502) *** | −0.060 (−0.238, 0.119) | ||||
| Attitudes | 0.966 (1, 183) | 0.327 | 0.052 *** | 0.041 * | ||||
| No (RC) | 38 | 156 | 0.441 (0.345, 0.538) *** | |||||
| Yes | 12 | 29 | 0.343 (0.171, 0.512) *** | −0.098 (−0.296, 0.099) | ||||
| Expectations | 0.652 (1, 183) | 0.420 | 0.051 *** | 0.041 * | ||||
| No (RC) | 33 | 104 | 0.394 (0.292, 0.496) *** | |||||
| Yes | 19 | 81 | 0.452 (0.333, 0.572) *** | 0.058 (−0.084, 0.200) | ||||
| Relation/collaboration parents | 1.071 (1, 183) | 0.302 | 0.047 *** | 0.046 * | ||||
| No (RC) | 38 | 110 | 0.443 (0.345, 0.540) *** | |||||
| Yes | 15 | 75 | 0.366 (0.233, 0.498) *** | −0.077 (−0.224, 0.070) | ||||
| Parental competence/empowerment | 1.313 (1, 183) | 0.253 | 0.051 *** | 0.040 * | ||||
| No (RC) | 28 | 115 | 0.462 (0.348, 0.577) *** | |||||
| Yes | 23 | 70 | 0.366 (0.245, 0.487) *** | −0.097 (−0.263, 0.070) | ||||
| Social network | 0.089 (1, 183) | 0.766 | 0.053 *** | 0.039 * | ||||
| No (RC) | 36 | 147 | 0.409 (0.310, 0.508) *** | |||||
| Yes | 15 | 38 | 0.437 (0.283, 0.590) *** | 0.028 (−0.155, 0.210) | ||||
| E: Delivery techniques | ||||||||
| Modelling | 3.545 (1, 183) | 0.061 + | 0.050 *** | 0.036 * | ||||
| No (RC) | 18 | 98 | 0.313 (0.179, 0.477) *** | |||||
| Yes | 33 | 87 | 0.474 (0.372, 0.575) *** | 0.160 (−0.008, 0.328) + | ||||
| Role-playing | 0.185 (1, 183) | 0.667 | 0.052 *** | 0.041 * | ||||
| No (RC) | 22 | 111 | 0.438 (0.313, 0.563) *** | |||||
| Yes | 28 | 74 | 0.401 (0.287, 0.551) *** | −0.037 (−0.206, 0.132) | ||||
| Practice and rehearsal | 5.485 (1, 183) | 0.020* | 0.054 *** | 0.028 + | ||||
| No (RC) | 23 | 56 | 0.512 (0.398, 0.627) *** | |||||
| Yes | 27 | 128 | 0.329 (0.225, 0.433) *** | −0.184 (−0.338, −0.029) * | ||||
| Video-feedback | 1.358 (1, 183) | 0.245 | 0.053 *** | 0.035 * | ||||
| No (RC) | 49 | 184 | 0.412 (0.330, 0.494) *** | |||||
| Yes | 1 | 1 | 0.984 (0.019, 1.949) * | 0.572 (−0.397, 1.541) | ||||
| Homework assignments | 0.000 (1, 183) | 0.988 | 0.053 *** | 0.039 * | ||||
| No (RC) | 17 | 54 | 0.418 (0.281, 0.554) *** | |||||
| Yes | 34 | 131 | 0.417 (0.323, 0.510) *** | −0.001 (−0.152, 0.149) | ||||
| (Group)discussion | 0.968 (1, 183) | 0.327 | 0.048 *** | 0.045 * | ||||
| No (RC) | 18 | 61 | 0.366 (0.230, 0.502) *** | |||||
| Yes | 34 | 124 | 0.448 (0.344, 0.553) *** | 0.082 (−0.083, 0.247) | ||||
| CBT techniques for parents | 0.043 (1, 183) | 0.836 | 0.053 *** | 0.039 * | ||||
| No (RC) | 46 | 163 | 0.414 (0.327, 0.502) *** | |||||
| Yes | 5 | 22 | 0.442 (0.191, 0.693) *** | 0.028 (−0.236, 0.291) | ||||
| Services for children | 0.206 (1, 183) | 0.651 | 0.053 *** | 0.040 * | ||||
| No (RC) | 44 | 161 | 0.425 (0.335, 0.516) *** | |||||
| Yes | 6 | 24 | 0.372 (0.158, 0.586) *** | −0.053 (−0.286. 0.179) | ||||
| Additional services for parents | 0.176 (1, 183) | 0.675 | 0.051 *** | 0.044 * | ||||
| No (RC) | 40 | 152 | 0.428 (0.332, 0.524) *** | |||||
| Yes | 11 | 33 | 0.386 (0.209, 0.562) *** | −0.042 (−0.242, 0.157) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gubbels, J.; van der Put, C.E.; Assink, M. The Effectiveness of Parent Training Programs for Child Maltreatment and Their Components: A Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 16, 2404. https://doi.org/10.3390/ijerph16132404
Gubbels J, van der Put CE, Assink M. The Effectiveness of Parent Training Programs for Child Maltreatment and Their Components: A Meta-Analysis. International Journal of Environmental Research and Public Health. 2019; 16(13):2404. https://doi.org/10.3390/ijerph16132404
Chicago/Turabian StyleGubbels, Jeanne, Claudia E. van der Put, and Mark Assink. 2019. "The Effectiveness of Parent Training Programs for Child Maltreatment and Their Components: A Meta-Analysis" International Journal of Environmental Research and Public Health 16, no. 13: 2404. https://doi.org/10.3390/ijerph16132404