Adverse Childhood Experiences of Children Adopted from Care: The Importance of Adoptive Parental Warmth for Future Child Adjustment


Abstract
:1. Introduction
1.1. Adoption
1.2. Parental Warmth as a Moderator of the Impact of ACEs
1.3. The Present Study
2. Materials and Methods
2.1. Study Design
2.2. Ethical Considerations
2.3. Data Collection
2.4. Participants
2.5. Measures
2.5.1. Adversity
2.5.2. Age Placed for Adoption
2.5.3. Child Internalising Symptoms and Externalising Problems
2.5.4. Parent-to-Child Warmth
2.5.5. Missing Data
2.5.6. Analysis
3. Results
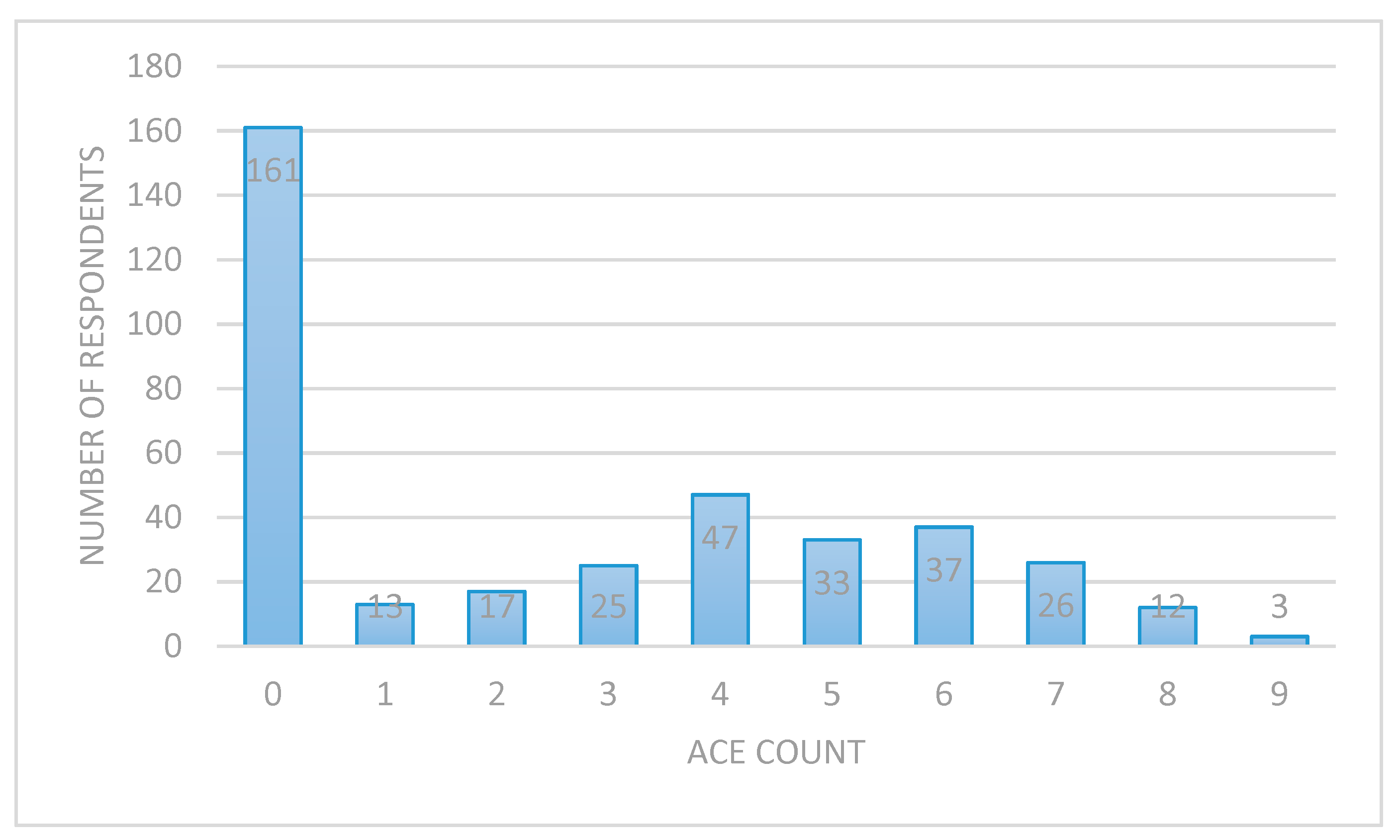
3.1. Description of Pre-Placement Experiences
3.2. Child Internalising Symptoms and Externalising Problems
3.3. The impact of ACEs on Child Internalising Symptoms and Externalising Problems: The Moderating Effect of Parental Warmth
3.3.1. Externalising Problems
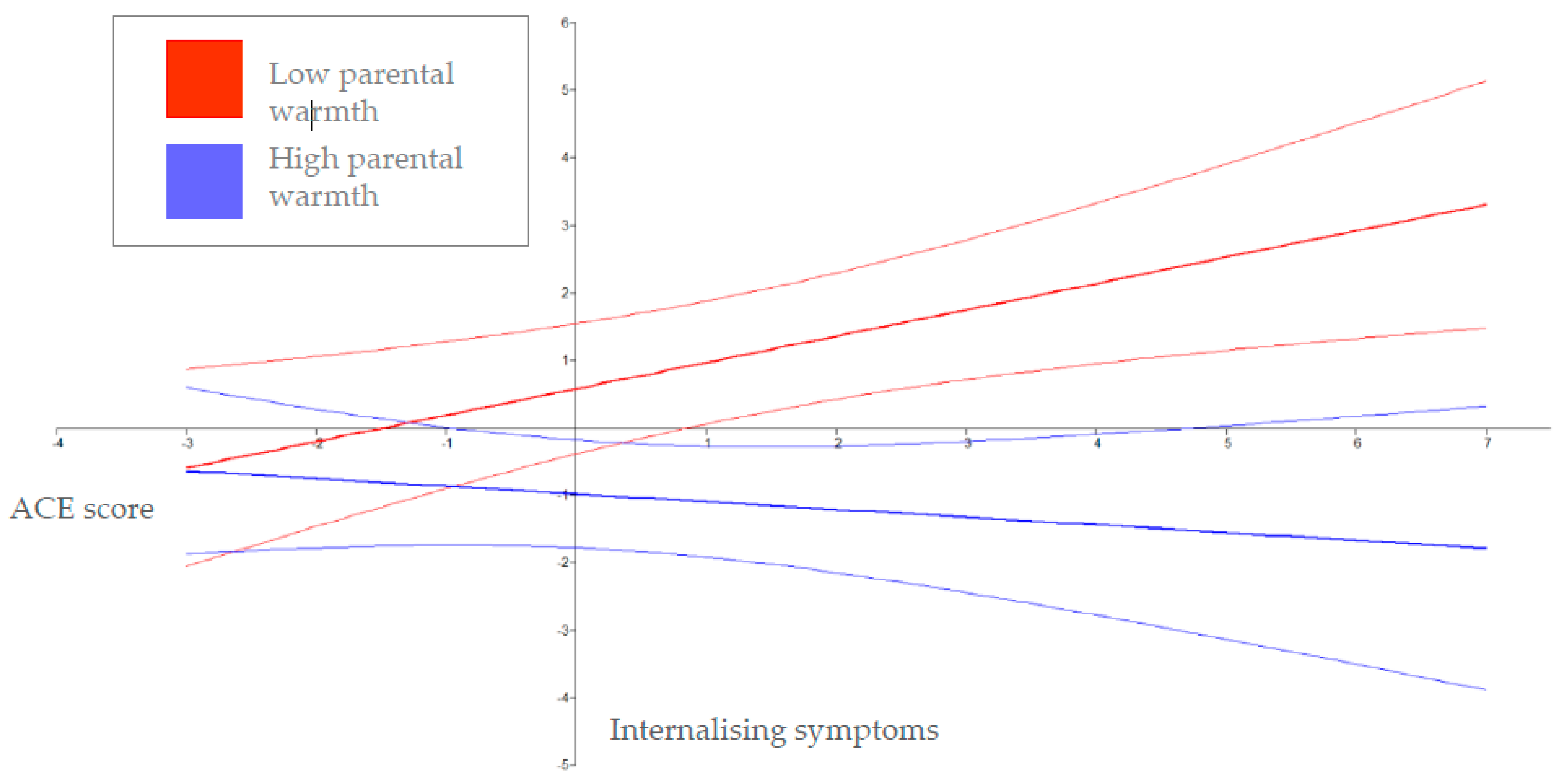
3.3.2. Internalising Symptoms
4. Discussion
4.1. Strengths
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Felitti, V.J.; Anda, R.F.; Nordenberg, D.; Williamson, D.F.; Spitz, A.M.; Edwards, V.; Koss, M.P.; Marks, J.S. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults—The adverse childhood experiences (ace) study. Am. J. Prev. Med. 1998, 14, 245–258. [Google Scholar] [CrossRef]
- Hughes, K.; Bellis, M.A.; Hardcastle, K.A.; Sethi, D.; Butchart, A.; Mikton, C.; Jones, L.; Dunne, M.P. The effect of multiple adverse childhood experiences on health: A systematic review and meta-analysis. Lancet Public Health 2017, 2, E356–E366. [Google Scholar] [CrossRef]
- Oh, D.L.; Jerman, P.; Silverio Marques, S.; Koita, K.; Purewal Boparai, S.K.; Burke Harris, N.; Bucci, M. Systematic review of pediatric health outcomes associated with childhood adversity. BMC Pediatr. 2018, 18, 83. [Google Scholar] [CrossRef]
- Liming, K.W.; Grube, W.A. Wellbeing outcomes for children exposed to multiple adverse experiences in early childhood: A systematic review. Child Adolesc. Soc. Work J. 2018, 35, 317–335. [Google Scholar] [CrossRef]
- Simkiss, D. The needs of looked after children from an adverse childhood experience perspective. Paediatr. Child Health 2019, 29, 25–33. [Google Scholar] [CrossRef]
- Baker, A.J.L.; Schneiderman, M.; Licandro, V. Mental health referrals and treatment in a sample of youth in foster care. Child Youth Serv. Rev. 2017, 78, 18–22. [Google Scholar] [CrossRef]
- Bruskas, D.; Tessin, D.H. Adverse childhood experiences and psychosocial well-being of women who were in foster care as children. Perm. J. 2013, 17, e131–e141. [Google Scholar] [CrossRef] [PubMed]
- Kerker, B.D.; Zhang, J.; Nadeem, E.; Stein, R.E.; Hurlburt, M.S.; Heneghan, A.; Landsverk, J.; McCue Horwitz, S. Adverse childhood experiences and mental health, chronic medical conditions, and development in young children. Acad. Pediatr. 2015, 15, 510–517. [Google Scholar] [CrossRef]
- McCrae, J.S.; Bender, K.; Brown, S.M.; Phillips, J.D.; Rienks, S. Adverse childhood experiences and complex health concerns among child welfare-involved children. Child. Health Care 2019, 48, 38–58. [Google Scholar] [CrossRef]
- Department for Education. Adoption: A Vision for Change; DfE: London, UK, 2016.
- Berlin, M.; Vinnerljung, B.; Hjern, A. School performance in primary school and psychosocial problems in young adulthood among care leavers from long term foster care. Child Youth Serv. Rev. 2011, 33, 2489–2497. [Google Scholar] [CrossRef]
- Neil, E.; Beek, M.; Ward, E. Contact after Adoption: A Follow up in Late Adolescence; University of East Anglia: Norfolk, UK, 2013. [Google Scholar]
- Triseliotis, J. Long-term foster care or adoption? The evidence examined. Child Fam. Soc. Work 2002, 7, 23–33. [Google Scholar] [CrossRef]
- Selwyn, J.; Quinton, D. Stability, permanence, outcomes and support: Foster care and adoption compared. Adopt. Foster. 2004, 28, 6–15. [Google Scholar] [CrossRef]
- McGhee, J.; Bunting, L.; McCartan, C.; Elliott, M.; Bywaters, P.; Featherstone, B. Looking after children in the uk—convergence or divergence? Br. J. Soc. Work 2017, 48, 1176–1198. [Google Scholar] [CrossRef]
- Tregeagle, S.; Moggach, L.; Trivedi, H.; Ward, H. Previous life experiences and the vulnerability of children adopted from out-of-home care: The impact of adverse childhood experiences and child welfare decision making. Child Youth Serv. Rev. 2019, 96, 55–63. [Google Scholar] [CrossRef]
- Juffer, F.; Van Ijzendoorn, M.H. Behavior problems and mental health referrals of international adoptees: A meta-analysis. Jama 2005, 293, 2501–2515. [Google Scholar] [CrossRef] [PubMed]
- Keyes, M.A.; Sharma, A.; Elkins, I.J.; Iacono, W.G.; McGue, M. The mental health of us adolescents adopted in infancy. Arch. Pediatr. Adolesc. Med. 2008, 162, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Brown, A.; Waters, C.S.; Shelton, K.H. A systematic review of the school performance and behavioural and emotional adjustments of children adopted from care. Adopt. Foster. 2017, 41, 346–368. [Google Scholar] [CrossRef]
- Simmel, C.; Brooks, D.; Barth, R.P.; Hinshaw, S.P. Externalizing symptomatology among adoptive youth: Prevalence and preadoption risk factors. J. Abnorm. Child Psychol. 2001, 29, 57–69. [Google Scholar] [CrossRef] [PubMed]
- Grotevant, H.D.; Van Dulmen, M.H.; Dunbar, N.; Nelson-Christinedaughter, J.; Christensen, M.; Fan, X.; Miller, B.C. Antisocial behavior of adoptees and nonadoptees: Prediction from early history and adolescent relationships. J. Res. Adolesc. 2006, 16, 105–131. [Google Scholar] [CrossRef]
- Dong, M.; Giles, W.H.; Felitti, V.J.; Dube, S.R.; Williams, J.E.; Chapman, D.P.; Anda, R.F. Insights into causal pathways for ischemic heart disease: Adverse childhood experiences study. Circulation 2004, 110, 1761–1766. [Google Scholar] [CrossRef]
- Kriebel, D.K.; Wentzel, K. Parenting as a moderator of cumulative risk for behavioral competence in adopted children. Adopt. Q. 2011, 14, 37–60. [Google Scholar] [CrossRef]
- Tilbury, C.; Thoburn, J. Children in out-of-home care in australia: International comparisons. Child. Aust. 2008, 33, 5–12. [Google Scholar] [CrossRef]
- Mignot, J.-F. Full adoption in england and wales and france: A comparative history of law and practice (1926–2015). Adopt. Foster. 2017, 41, 142–158. [Google Scholar] [CrossRef]
- Waid, J.; Alewine, E. An exploration of family challenges and service needs during the post-adoption period. Child Youth Serv. Rev. 2018, 91, 213–220. [Google Scholar] [CrossRef]
- Tan, T.X.; Marfo, K. Parental ratings of behavioral adjustment in two samples of adopted chinese girls: Age-related versus socio-emotional correlates and predictors. J. Appl. Dev. Psychol. 2006, 27, 14–30. [Google Scholar] [CrossRef]
- Selwyn, J.; Meakings, S.; Wijedesa, D. Beyond the Adoption Order. Challenges, Interventions and Adoption Disruption; BAAF: London, UK, 2015. [Google Scholar]
- Balenzano, C.; Coppola, G.; Cassibba, R.; Moro, G. Pre-adoption adversities and adoptees’ outcomes: The protective role of post-adoption variables in an italian experience of domestic open adoption. Child Youth Serv. Rev. 2018, 85, 307–318. [Google Scholar] [CrossRef]
- Tan, T.X.; Marfo, K. Pre-adoption adversity and behavior problems in adopted chinese children: A longitudinal study. J. Appl. Dev. Psychol. 2016, 42, 49–57. [Google Scholar] [CrossRef]
- Grotevant, H.D.; McDermott, J.M. Adoption: Biological and social processes linked to adaptation. Annu. Rev. Psychol. 2014, 65, 235–265. [Google Scholar] [CrossRef]
- Simmel, C.; Barth, R.P.; Brooks, D. Adopted foster youths’ psychosocial functioning: A longitudinal perspective. Child Fam. Soc. Work 2007, 12, 336–348. [Google Scholar] [CrossRef]
- Palacios, J.; Román, M.; Moreno, C.; León, E.; Peñarrubia, M.-G. Differential plasticity in the recovery of adopted children after early adversity. Child Dev. Perspect. 2014, 8, 169–174. [Google Scholar] [CrossRef]
- Van der Voort, A.; Linting, M.; Juffer, F.; Bakermans-Kranenburg, M.J.; Schoenmaker, C.; van Ijzendoorn, M.H. The development of adolescents’ internalizing behavior: Longitudinal effects of maternal sensitivity and child inhibition. J. Youth Adolesc. 2014, 43, 528–540. [Google Scholar] [CrossRef]
- Woolgar, M. The practical implications of the emerging findings in the neurobiology of maltreatment for looked after and adopted children: Recognising the diversity of outcomes. Adopt. Foster. 2013, 37, 237–252. [Google Scholar] [CrossRef]
- Burt, S.A. Rethinking environmental contributions to child and adolescent psychopathology: A meta-analysis of shared environmental influences. Psychol. Bull. 2009, 135, 608–637. [Google Scholar] [CrossRef]
- Harris, P.; Selwyn, J.; Quinton, D.; Wijedesa, D.; Nawaz, S.; Wood, M. Pathways to Permanence for Black, Asian & Mixed Ethnicity Children; British Association for Adoption & Fostering: London, UK, 2010. [Google Scholar]
- Pinquart, M. Associations of parenting dimensions and styles with externalizing problems of children and adolescents: An updated meta-analysis. Dev. Psychol. 2017, 53, 873–932. [Google Scholar] [CrossRef]
- Pinquart, M. Associations of parenting dimensions and styles with internalizing symptoms in children and adolescents: A meta-analysis. Marriage Fam. Rev. 2017, 53, 613–640. [Google Scholar] [CrossRef]
- Bayer, J.K.; Sanson, A.V.; Hemphill, S.A. Parent influences on early childhood internalizing difficulties. J. Appl. Dev. Psychol. 2006, 27, 542–559. [Google Scholar] [CrossRef]
- Boeldt, D.L.; Rhee, S.H.; Dilalla, L.F.; Mullineaux, P.Y.; Schulz-Heik, R.J.; Corley, R.P.; Young, S.E.; Hewitt, J.K. The association between positive parenting and externalizing behavior. Infant Child Dev. 2012, 21, 85–106. [Google Scholar] [CrossRef] [PubMed]
- Masten, A.S. Global perspectives on resilience in children and youth. Child Dev. 2014, 85, 6–20. [Google Scholar] [CrossRef]
- Stormshak, E.A.; Bierman, K.L.; McMahon, R.J.; Lengua, L.J. Parenting practices and child disruptive behavior problems in early elementary school. Conduct problems prevention research group. J. Clin. Child Psychol. 2000, 29, 17–29. [Google Scholar] [CrossRef]
- Calafat, A.; García, F.; Juan, M.; Becoña, E.; Fernández-Hermida, J.R. Which parenting style is more protective against adolescent substance use? Evidence within the european context. Drug Alcohol Depend. 2014, 138, 185–192. [Google Scholar] [CrossRef]
- Reuben, J.D.; Shaw, D.S.; Neiderhiser, J.M.; Natsuaki, M.N.; Reiss, D.; Leve, L.D. Warm parenting and effortful control in toddlerhood: Independent and interactive predictors of school-age externalizing behavior. J. Abnorm. Child Psychol. 2016, 44, 1083–1096. [Google Scholar] [CrossRef] [PubMed]
- Martínez, I.; Murgui, S.; Garcia, O.F.; Garcia, F. Parenting in the digital era: Protective and risk parenting styles for traditional bullying and cyberbullying victimization. Comput. Hum. Behav. 2019, 90, 84–92. [Google Scholar] [CrossRef]
- Beijersbergen, M.D.; Juffer, F.; Bakermans-Kranenburg, M.J.; van Ijzendoorn, M.H. Remaining or becoming secure: Parental sensitive support predicts attachment continuity from infancy to adolescence in a longitudinal adoption study. Dev. Psychol. 2012, 48, 1277–1282. [Google Scholar] [CrossRef] [PubMed]
- Van IJzendoorn, M.H.; Juffer, F. The emanuel miller memorial lecture 2006: Adoption as intervention. Meta-analytic evidence for massive catch-up and plasticity in physical, socio-emotional, and cognitive development. J. Child Psychol. Psychiatry 2006, 47, 1228–1245. [Google Scholar] [CrossRef] [PubMed]
- Zvara, B.J.; Sheppard, K.W.; Cox, M. Bidirectional effects between parenting sensitivity and child behavior: A cross-lagged analysis across middle childhood and adolescence. J. Fam. Psychol. 2018, 32, 484–495. [Google Scholar] [CrossRef] [PubMed]
- Eisenberg, N.; Valiente, C.; Spinrad, T.L.; Cumberland, A.; Liew, J.; Reiser, M.; Zhou, Q.; Losoya, S.H. Longitudinal relations of children’s effortful control, impulsivity, and negative emotionality to their externalizing, internalizing, and co-occurring behavior problems. Dev. Psychol. 2009, 45, 988–1008. [Google Scholar] [CrossRef]
- Garvin, M.C.; Tarullo, A.R.; Ryzin, M.V.; Gunnar, M.R. Postadoption parenting and socioemotional development in postinstitutionalized children. Dev. Psychopathol. 2012, 24, 35–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meakings, S.; Ottaway, H.; Coffey, A.; Palmer, C.; Doughty, J.; Shelton, K. The support needs and experiences of newly formed adoptive families: Findings from the wales adoption study. Adopt. Foster. 2018, 42, 58–75. [Google Scholar] [CrossRef]
- Anthony, R.; Meakings, S.; Doughty, J.; Ottaway, H.; Holland, S.; Shelton, K.H. Factors affecting adoption in wales: Predictors of variation in time between entry to care and adoptive placement. Child. Youth Serv. Rev. 2016, 67, 184–190. [Google Scholar] [CrossRef]
- Meakings, S.; Coffey, A.; Shelton, K.H. The influence of adoption on sibling relationships: Experiences and support needs of newly formed adoptive families. Br. J. Soc. Work 2017, 47, 1781–1799. [Google Scholar] [CrossRef]
- Office for National Statistics. Gross Household Income, UK, Financial Year Ending. 2018. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/personalandhouseholdfinances/incomeandwealth/adhocs/009772grosshouseholdincomeukfinancialyearending2018 (accessed on 21 February 2019).
- Villodas, M.T.; Litrownik, A.J.; Newton, R.R.; Davis, I.P. Long-term placement trajectories of children who were maltreated and entered the child welfare system at an early age: Consequences for physical and behavioral well-being. J. Pediatr. Psychol. 2016, 41, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Goodman, R. The strengths and difficulties questionnaire: A research note. J. Child Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Achenbach, T.M.; Becker, A.; Döpfner, M.; Heiervang, E.; Roessner, V.; Steinhausen, H.-C.; Rothenberger, A. Multicultural assessment of child and adolescent psychopathology with aseba and sdq instruments: Research findings, applications, and future directions. J. Child Psychol. Psychiatry 2008, 49, 251–275. [Google Scholar] [CrossRef] [PubMed]
- Goodman, A.; Goodman, R. “Strengths and difficulties questionnaire as a dimensional measure of child mental health”: Erratum. J. Am. Acad. Child Adolesc. Psychiatry 2009, 48, 580. [Google Scholar] [CrossRef] [PubMed]
- Goodman, R. Psychometric properties of the strengths and difficulties questionnaire. J. Am. Acad. Child Adolesc. Psychiatry 2001, 40, 1337–1345. [Google Scholar] [CrossRef] [PubMed]
- Goodman, R.; Ford, T.; Corbin, T.; Meltzer, H. Using the strengths and difficulties questionnaire (sdq) multi-informant algorithm to screen looked-after children for psychiatric disorders. Eur. Child Adolesc. Psychiatry 2004, 13, ii25–ii31. [Google Scholar] [CrossRef]
- Melby, J.N.; Conger, R.D.; Book, R.; Reuter, M.; Lucy, L.; Repinski, D. The Iowa Family Interaction Rating Scales, 5th ed.; Iowa State University, Institute for Social and Behavioral Research: Ames, IA, USA, 1998. [Google Scholar]
- Schafer, J.L.; Graham, J.W. Missing data: Our view of the state of the art. Psychol. Methods 2002, 7, 147–177. [Google Scholar] [CrossRef]
- Muthén, L.K. Mplus User’s Guide, 7th ed.; Muthén and Muthén: Los Angeles, CA, USA, 1998. [Google Scholar]
- Frigon, J.-Y.; Laurencelle, L. Analysis of covariance: A proposed algorithm. Educ. Psychol. Meas. 1993, 53, 1–18. [Google Scholar] [CrossRef]
- Bowerman, B.L.; O’Connell, R.T. Linear Statistical Models; Thomson Wadsworth: Stamford, CT, USA, 1990. [Google Scholar]
- Wilson, H.W.; Samuelson, S.L.; Staudenmeyer, A.H.; Widom, C.S. Trajectories of psychopathology and risky behaviors associated with childhood abuse and neglect in low-income urban african american girls. Child Abuse Negl. 2015, 45, 108–121. [Google Scholar] [CrossRef]
- Meltzer, H.; Gatward, R.; Goodman, R.; Ford, T. Mental health of children and adolescents in great britain (reprinted from 2000). Int. Rev. Psychiatr. 2003, 15, 185–187. [Google Scholar] [CrossRef]
- Goodman, A.; Goodman, R. Strengths and difficulties questionnaire scores and mental health in looked after children. Br. J. Psychiatry 2012, 200, 426–427. [Google Scholar] [CrossRef] [PubMed]
- Ashton, K.; Bellis, M.; Hughes, K. Adverse childhood experiences and their association with health-harming behaviours and mental wellbeing in the welsh adult population: A national cross-sectional survey. Lancet 2016, 388, 21. [Google Scholar] [CrossRef]
- Ford, T.; Vostanis, P.; Meltzer, H.; Goodman, R. Psychiatric disorder among british children looked after by local authorities: Comparison with children living in private households. Br. J. Psychiatry 2007, 190, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Wretham, A.E.; Woolgar, M. Do children adopted from british foster care show difficulties in executive functioning and social communication? Adopt. Foster. 2017, 41, 331–345. [Google Scholar] [CrossRef]
- Grotevant, H.D.; Lo, A.Y.H.; Fiorenzo, L.; Dunbar, N.D. Adoptive identity and adjustment from adolescence to emerging adulthood: A person-centered approach. Dev. Psychol. 2017, 53, 2195–2204. [Google Scholar] [CrossRef] [PubMed]
- Biglan, A.; Van Ryzin, M.J.; Hawkins, J.D. Evolving a more nurturing society to prevent adverse childhood experiences. Acad. Pediatr. 2017, 17, S150–S157. [Google Scholar] [CrossRef]
- Toth, S.L.; Cicchetti, D. A developmental psychopathology perspective on child maltreatment. Child Maltreatment 2013, 18, 135–139. [Google Scholar] [CrossRef]
- Grotevant, H.D.; Ross, N.M.; Marchel, M.A.; McRoy, R.G. Adaptive behavior in adopted children: Predictors from early risk, collaboration in relationships within the adoptive kinship network, and openness arrangements. J. Adolesc. Res. 1999, 14, 231–247. [Google Scholar] [CrossRef]
- Thompson, R.; Flaherty, E.G.; English, D.J.; Litrownik, A.J.; Dubowitz, H.; Kotch, J.B.; Runyan, D.K. Trajectories of adverse childhood experiences and self-reported health at age 18. Acad. Pediatr. 2015, 15, 503–509. [Google Scholar] [CrossRef]
- Trickett, P.K.; Putnam, F.W. Developmental consequences of child sexual abuse. In Violence Against Children in the Family and the Community; American Psychological Association: Washington, DC, USA, 1998; pp. 39–56. [Google Scholar]
- Cohen, J.A. Practice parameter for the assessment and treatment of children and adolescents with posttraumatic stress disorder. J. Am. Acad. Child Adolesc. Psychiatry 2010, 49, 414–430. [Google Scholar]
- Dube, S.R.; Williamson, D.F.; Thompson, T.; Felitti, V.J.; Anda, R.F. Assessing the reliability of retrospective reports of adverse childhood experiences among adult hmo members attending a primary care clinic. Child Abus. Negl. 2004, 28, 729–737. [Google Scholar] [CrossRef] [PubMed]
- Widom, C.S.; Raphael, K.G.; DuMont, K.A. The case for prospective longitudinal studies in child maltreatment research: Commentary on dube, williamson, thompson, felitti, and anda (2004). Child Abus. Negl. 2004, 28, 715–722. [Google Scholar] [CrossRef] [PubMed]
- Hardt, J.; Rutter, M. Validity of adult retrospective reports of adverse childhood experiences: Review of the evidence. J. Child Psychol. Psychiatry 2004, 45, 260–273. [Google Scholar] [CrossRef] [PubMed]
- Della Femina, D.; Yeager, C.A.; Lewis, D.O. Child abuse: Adolescent records vs. Adult recall. Child Abus. Negl. 1990, 14, 227–231. [Google Scholar] [CrossRef]
- Brown, G.W.; Harris, T. Social origins of depression: A reply. Psychol. Med. 1978, 8, 577–588. [Google Scholar] [CrossRef] [PubMed]
- Greenfield, E.A. Child abuse as a life-course social determinant of adult health. Maturitas 2010, 66, 51–55. [Google Scholar] [CrossRef] [PubMed]
- Fritz, M.S.; Cox, M.G.; MacKinnon, D.P. Increasing statistical power in mediation models without increasing sample size. Eval. Health Prof. 2015, 38, 343–366. [Google Scholar] [CrossRef]
- Roskam, I.; van der Voort, A.; Juffer, F.; Stievenart, M.; Bader, M.; Muntean, A.; Escobar, M.J.; Santelices, M.P.; Molina, P.; Casonato, M.; et al. Cross-informant ratings of internalizing and externalizing behavior in adolescent–parent pairs in six countries. Does being adopted make a difference? Int. Perspect. Psychol. Res. Pract. Consult. 2017, 6, 32–46. [Google Scholar] [CrossRef]
- London, K.; Bruck, M.; Wright, D.B. Review of the contemporary literature on how children report sexual abuse to others: Findings, methodological issues, and implications for forensic interviewers. Memory 2008, 16, 29–47. [Google Scholar] [CrossRef]
- Farmer, E.; Dance, C. Family finding and matching in adoption: What helps to make a good match? Br. J. Soc. Work 2016, 46, 974–992. [Google Scholar] [CrossRef]
- Sara, G.; Lappin, J. Childhood trauma: Psychiatry’s greatest public health challenge? Lancet Public Health 2017, 2, e300–e301. [Google Scholar] [CrossRef]
- Stoto, M.A.; Almario, D.A.; McCormick, M.C. (Eds.) Reducing the Odds: Preventing Perinatal Transmission of HIV in the United States; National Academy Press: Washington, DC, USA, 1999; p. 397. [Google Scholar]



{kind=link}
{kind=link}
| Adverse Childhood Experiences (ACEs) | CAR Sample (n = 374) | Longitudinal Subsample (n = 84) |
|---|---|---|
| Emotional abuse | 85 (23) | 20 (24) |
| Physical abuse | 70 (19) | 19 (23) |
| Sexual abuse | 14 (4) | 5 (6) |
| Neglect | 203 (54) | 45 (54) |
| Parental separation | 113 (30) | 24 (29) |
| Domestic violence | 138 (37) | 34 (31) |
| Parent mental illness | 118 (32) | 31 (37) |
| Parent alcohol abuse | 96 (26) | 20 (24) |
| Parent drug abuse | 126 (34) | 27 (32) |
| Parent incarceration | 74 (20) | 19 (23) |
| ACE “score” (M, SD) | 2.68 (2.75) | 2.65 (2.82) |
| Samples and Subpopulations | n | SDQ Total Difficulty Score, Mean (95% CI) |
|---|---|---|
| UK general population | 10,298 | 8.4 |
| Looked after children | ||
| Foster care | 781 | 15.3 (14.7–15.8) |
| At risk children living with natural parents | 190 | 16.2 (15.0–17.3) |
| Kinship care | 165 | 12.2 (11.0–13.4) |
| Residential care | 255 | 20.0 (19.1–20.8) |
| Wales Adoption Cohort Study | ||
| Time 1 | 58 | 13.6 (11.87–15.43) |
| Time 2 | 76 | 10.6 (9.31–11.81) |
| Time 3 | 70 | 10.8 (9.40–12.17) |
| Average | Slightly Raised | High | Very High | Average | Slightly Raised | High | Very High | Average | Slightly Raised | High | Very High | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Normative sample | 80% | 10% | 5% | 5% | 80% | 10% | 5% | 5% | 80% | 10% | 5% | 5% |
| Time 1 n (%) | Time 2 n (%) | Time 3 n (%) | ||||||||||
| Total difficulties | 34 (59) | 7 (12) | 5 (9) | 12 (21) | 50 (66) | 15 (20) | 6 (8) | 5 (7) | 48 (72) | 6 (9) | 7 (10) | 6 (9) |
| Emotional problems | 39 (67) | 5 (9) | 7 (12) | 7 (12) | 55 (72) | 11 (15) | 5 (7) | 5 (7) | 51 (76) | 3 (5) | 7 (10) | 6 (9) |
| Conduct problems | 36 (62) | 6 (10) | 7 (12) | 9 (16) | 60 (79) | 5 (7) | 5 (7) | 6 (8) | 43 (64) | 10 (15) | 8 (12) | 6 (9) |
| Hyperactivity | 29 (51) | 13 (23) | 3 (5) | 12 (21) | 50 (66) | 13 (17) | 5 (7) | 8 (11) | 47 (70) | 6 (9) | 5 (8) | 9 (13) |
| Peer problems | 38 (67) | 10 (18) | 3 (5) | 6 (11) | 54 (71) | 13 (17) | 4 (5) | 5 (7) | 47 (70) | 5 (8) | 9 (13) | 6 (9) |
| Prosocial | 28 (48) | 8 (14) | 10 (17) | 12 (21) | 46 (60) | 5 (7) | 10 (13) | 16 (21) | 37 (55) | 8 (12) | 11 (16) | 11 (16) |
| Measure | 1 | 2 | 3 | 4 | 5 | 6 | |
|---|---|---|---|---|---|---|---|
| 1 | Child gender | - | |||||
| 2 | Child age at placement | −0.07 (373) | - | ||||
| 3 | ACE count | −0.09 (374) | 0.62 ** (373) | - | |||
| 4 | T3 child externalising | −0.01 (62) | 0.15 (62) | 0.14 (62) | - | ||
| 5 | T3 child internalising | −0.08 (62) | 0.36 ** (62) | 0.26 * (62) | 0.48 ** (70) | - | |
| 6 | T2 parent warmth | −0.12 (72) | −0.45 ** (72) | −0.29 ** (72) | −0.39 ** (69) | −0.43 ** (69) | - |
| Mean | 0.52 | 2.32 | 2.65 | 6.98 | 3.80 | 38.17 | |
| (SD) | (50) | (2.23) | (2.82) | (3.61) | (3.07) | (4.45) | |
| Variables | T3 externalising Problems | T3 internalising Problems | ||||
|---|---|---|---|---|---|---|
| B | SE | β | B | SE | β | |
| Age placed | −0.03 | 0.26 | −0.02 | 0.20 | 0.20 | 0.16 |
| ACE count | 0.11 | 0.20 | 0.09 | 0.03 | 0.15 | 0.03 |
| T2 parental warmth | −0.17 | 0.11 | −0.22 | −0.14 ** | 0.07 | −0.22 |
| ACE × parental warmth | 0.01 | 0.04 | 0.02 | −0.06 ** | 0.02 | −0.24 * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anthony, R.E.; Paine, A.L.; Shelton, K.H. Adverse Childhood Experiences of Children Adopted from Care: The Importance of Adoptive Parental Warmth for Future Child Adjustment. Int. J. Environ. Res. Public Health 2019, 16, 2212. https://doi.org/10.3390/ijerph16122212
Anthony RE, Paine AL, Shelton KH. Adverse Childhood Experiences of Children Adopted from Care: The Importance of Adoptive Parental Warmth for Future Child Adjustment. International Journal of Environmental Research and Public Health. 2019; 16(12):2212. https://doi.org/10.3390/ijerph16122212
Chicago/Turabian StyleAnthony, Rebecca E., Amy L. Paine, and Katherine H. Shelton. 2019. "Adverse Childhood Experiences of Children Adopted from Care: The Importance of Adoptive Parental Warmth for Future Child Adjustment" International Journal of Environmental Research and Public Health 16, no. 12: 2212. https://doi.org/10.3390/ijerph16122212