1. Introduction
China has the largest elderly population in the world, with a projection of over 345 million people aged 60 years or above by the end of 2030, and this number is projected to increase rapidly over the next couple of decades [
1,
2]. Health is a critical determinant of healthy aging. Unfortunately, much is of concern in regard to the health of China’s elderly. On October 31, 2016, Wang Peian, the former deputy director of The Nation Health Commission of the People’s Republic of China, issued that among those aged 60 or above, 150 million had at least one chronic disease; approximately 7 million were diagnosed with dementia; 10 million, with permanent disability; and 40 million, with partial disability, and over 30% suffered from a variety of mental diseases. Identifying the factors that affect elderly health is a crucial first step in providing help.
Among the social determinants of health, social capital emerges as an important concept [
3,
4]. From a theoretical perspective, the association between social capital and health is well documented, and the positive relationship among social capital and better health outcomes has been examined in a number of countries and areas, including China [
5,
6,
7], the United States [
8], Japan [
9,
10], Europe [
11,
12], and Sub-Saharan Africa [
13]. In addition, there is increasing evidence of the importance of social capital for promoting health among the aged [
14].
Further, in old age, a large proportion of people live alone and have small social networks and low participation in social activities [
15], making them more susceptible to feelings of loneliness. Loneliness is a common, painful, emotional experience, and it is a significant public health issue, especially among the elderly [
16]. Increasing evidence has documented that loneliness in old age appears to be an important risk factor of being inactive [
17] and worse health, including morbidity and mortality [
18,
19,
20], depression [
21,
22], lower levels of self-rated physical health [
15], and hypertension [
23] as well as cardiovascular disease, diabetes, and migraine [
24]. Using the Chinese Longitudinal Health Longevity Survey’s (CLHLS) last four waves of data from 2002 to 2011, another study found that loneliness has an adverse impact on cognitive functioning and vice versa [
25].
There is an ongoing debate about how to measure social capital, and it is often unclear which activities form various aspects of it [
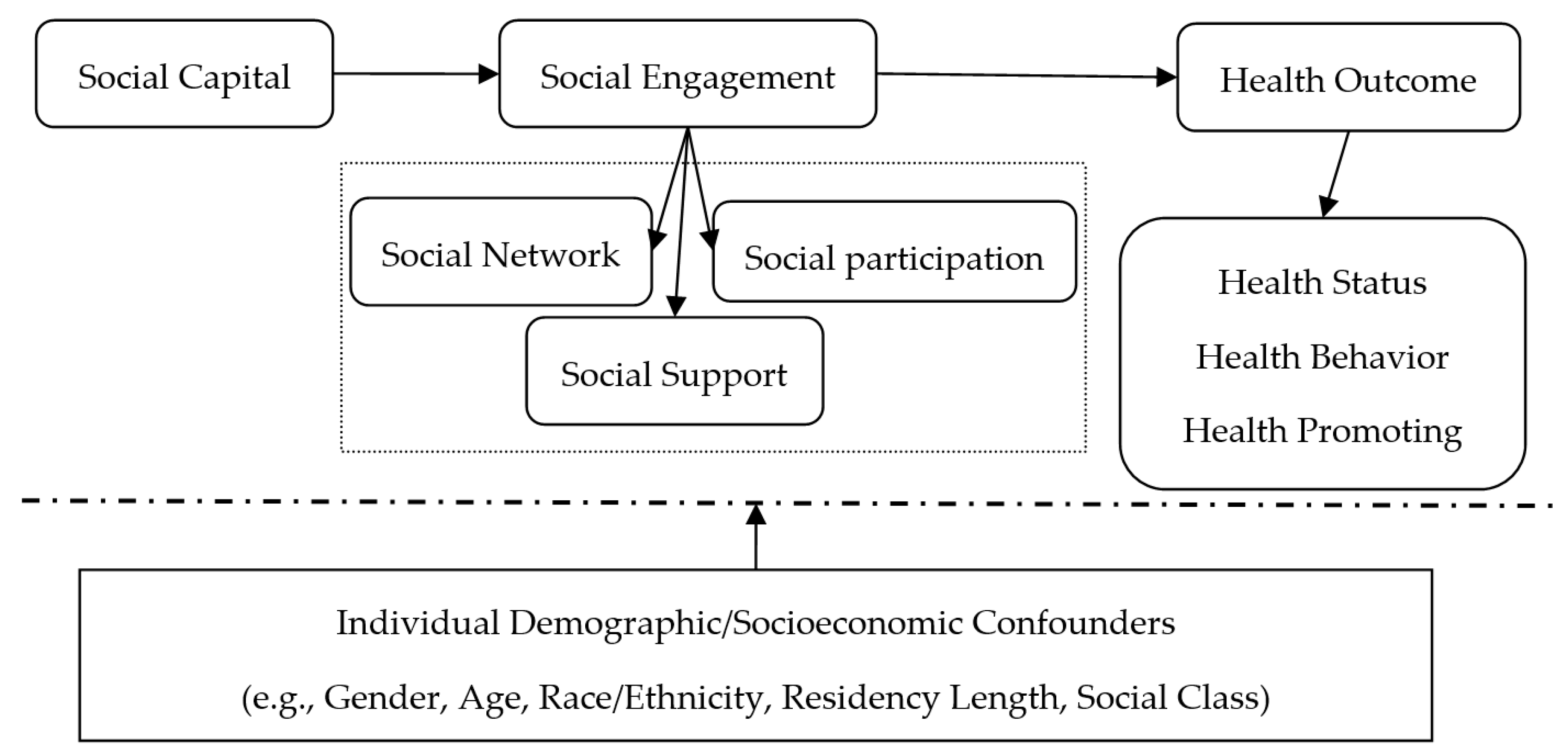
26]. Moreover, there is disagreement about how to define social capital, whose definitions include such concepts as trust, norms, networks, relationship, civic participation, and social support, with social engagement as not included in these definitions. According to previous studies [
27,
28,
29,
30], three components of social capital have been assessed in the literature in relation to health outcomes: social participation, social networks, and social support. Social engagement, a real-life activity that results from association with one’s social ties, plays an important role in reinforcing social relationships, social support or social integration, resulting in maintaining better health and health outcomes [
31,
32] and is regarded as an important component of successful aging [
33].
In later life, most adults no longer work or work fewer hours and have more time for social engagement [
25,
34]. Social engagement has become an important tool for older adults to obtain social resources. At present, there is global consensus on the importance of social engagement to active, healthy aging [
35]. Social engagement not only helps to maintain older adults’ social activities and relations but also has a positive impact on their physical and mental health through communication and social support [
36]. Therefore, it is imperative to investigate the influence of social engagement on elderly health.
Previous research has established an association between social engagement and health promotion effect among old people. Some studies have suggested that social engagement can significantly improve an individual’s health. Using the data from the China Health and Retirement Longitudinal Study (CHARLS) conducted in the Zhejiang and Gansu Provinces in 2008, a previous study found that social engagement can significantly improve the self-rated health of residents 45 years and older [
6]. Another studies replicated this result, using the data from the CHARLS conducted in 2011 [
37]. Additionally, social capital could significantly reduce older adults’ emotional stress in rural areas [
38].
Using the CLHLS, some studies aimed to gain more insight into the relationship between the elderly’s social engagement and self-rated health. Hu et al. noted that social engagement not only had a positive impact on elderly health but also played a positive role in disability prevention [
39]. Lu et al. [
35] found a causal, beneficial impact of social engagement on self-rated health among old people and that the impact of self-rated health on social engagement may be greater than that of social engagement on self-rated health. In addition, according to the Wisconsin study, the relationships between social participation and health vary by the type of trust and activity [
8]. Other studies, however, have suggested that social activities do not affect health. For example, a study on rural residents of the Shandong province found that the impact of structural social capital, such as activity participation and social network, was not significant [
40]. Meng and Chen [
41] investigated the impact of social capital on self-rated health status, using the Chinese General Social Survey (CGSS) conducted in 2005, and found that social participation did not significantly affect residents’ self-rated health status. Similar conclusions were drawn by Snelgrove et al. [
42] and d’Hombres et al. [
43].
Across a range of studies, researchers have consistently shown the effect of social engagement on elderly health. Nonetheless, there are three major reasons why our investigation makes important contributions to the literature.
First, this study builds upon the broader literature that links elderly health to social capital and focuses on the impact of social engagement on health. Most research on social engagement and promoting health focuses on only one indicator of social capital, which is an umbrella concept; thus, it is difficult to identify its aggregate impact. On the based of Putnam’s (2000) social capital theory [
4], social capital consists largely of social networks, trust, and norms through social engagement. People who have more social engagement may create more social links or relationship, have more trust in others, and, thus, can be helpful in terms of sharing health information and knowledge, reinforcing access to quality health care and promoting individual health [
13,
44]. In addition, social engagement is useful for becoming integrated into their neighborhood network and forming a neighborhood-level understanding of the availability of and access to resources. This could be helpful for the elderly to obtain material and emotional support of their neighbors and, thus, support their health [
28,
45]. Further, participating in social activities is a valuable approach to improving quality of life and reducing the burden associated with declining health and functioning as older adults age [
46].
Second, this study recognizes that there is no “typical” elderly, as the health and functional status of the elderly are diverse. Thus, it is often difficult to measure and compare their health status. Despite growing evidence that suggests a relationship between social engagement and elderly self-report health, more objective measures are needed. The elderly often suffers from a variety of serious health-related consequences, such as decreased economic resources and increased medical burden to themselves and their families. These could further affect the elderly’s psychological well-being and health behavior [
47]. A pioneering study found that these serious health-related consequences may even raise the rate of suicide in elderly people, especially the rate for the elderly in rural areas [
48]. What’s important, based on the “China’s Medium-to-Long Term Plan for the Prevention and Treatment of Chronic Diseases (2017–2025)”, which was issued by the General Office of the State Council of the People’s Republic of China on January 22, 2017, there are more than 260 million people who suffer from chronic diseases in China and the rate of death that results from chronic diseases is 86.6%, when disease burden accounts more than 70% for all disease burdens. In the reference literature, it has been provided that neurodegenerative and neuropsychiatric conditions that can affect older people, such as dementia and Parkinson’s disease, are often characterized by significant psychological deficits that reduce their overall quality of life [
49].
To measure the influence of social engagement on the health and well-being of the elderly, we use objective and subjective approaches to measure health, including self-rated health, degree of psychological distress and the numbers of chronic diseases.
Third, a lack of sufficient sample sizes/data in the past may have caused statistically biased estimates [
37]. The current study analyzed the data derived from the 2011 and 2013 waves of the CHARLS and estimates how social engagement affects elderly health in a more comprehensive way, providing evidence on healthy aging in China.
This paper proceeds as follows.
Section 2 presents the hypotheses, model specification, data source, and variable selection.
Section 3 provides the results.
Section 4 presents potential mechanisms for the findings, and
Section 5 concludes the paper.
4. How Social Engagement Influences the Health of the Elderly
Although active social engagement has been shown to be associated with better health outcomes across our study and other literature to date, there is unclear or insufficient evidence that how social engagement leads to better health. New research concerning the relationship would be offered, while an increasing literature has considered the issue. In our opinions, it assumed that social engagement would be associated with elderly health through social engagement’s effect on health behaviors and access to medical and health resources. To verify these two mechanisms, we estimate the following equation:
The dependent variables are healthy behavior and access to medical and health resources. Healthy behavior is determined from whether they exercise regularly. On the CHARLS, respondents are asked, “Do you normally do intense, moderately intense, or leisure activities for at least 10 minutes a week?” (on the CHARLS, respondents were asked to think only about those physical activities that they did for at least 10 minutes at a time) the response to which is a binary variable. For access to medical and health resources, we used the question, “Did you use outpatient services in the past month?” the response to which also was a binary variable.
Based on Equation (4), the results are shown in
Table 6. The results indicate that, in all samples, the effect of participation in social engagement is significant and positive, the probability of physical exercise and of choosing a healthy way of life, which is helpful to maintaining or improving health status. The results also show that, for those who participated in social engagement, the probability of seeing a doctor is significantly increased in the past month, compared with those who do not participate in social activities. As we expected, the results confirm social engagement could help to make older adults obtain medical and health information, which would be useful to promote elderly health.
Finally, we use the method of transforming variables for verification. The results are shown in
Table 7. The results show that the effect of the explanatory variables is consistent with previous results.
5. Discussion
Population aging poses a significant challenge to individual and social health, how to facilitate healthy aging by promoting health and well-being among the elderly is a topic of the utmost importance. Employing detailed longitudinal data from the CHARLS conducted in 2011 and 2013, we applied a 2SRI approach to gain more insight into the association between social engagement and elderly health. We found that social engagement could improve the elderly’s self-rated health and mental health through changing their health behaviors and access to health care and resources and that the urban elderly’s health status in urban was better than that of their rural counterparts.
Our findings suggest policy interventions to maintain and improve health and well-being among the elderly. In addition to comprehensive public health actions, the government should help to create an elderly-friendly environment. It should build activity centers and increase public service fiscal expenditures. In addition, social resources should be mobilized for investment in the elderly-care industry. Finally, the government needs to increase the construction of rural pension service facilities to narrow the gap between urban and rural areas.
This study enriches and expands on previous research and contributes to the literature in three ways. First, we used an innovative research perspective. We focused a community-supporting environment that meets the needs of the elderly and helps them to be actively engaged in their health. We also focused on the impact of interpersonal communication (i.e., social engagement) on the health of the elderly. Further, we measured both subjective and objective indicators of elderly health, providing a more accurate and comprehensive understanding. Second, we adopted new instrumental variables for causal 2SRI estimations: whether the village/community has a chess and card room or activity center for the elderly and how many bus lines be accessible this village/community. Third, our conclusions and policy recommendations are widely applicable to China and other countries with a similar elderly culture.
Though this work provides evidence for increasing social engagement on elderly health, we consider several potential limitations.
First, if the elderly in rural area would migrate to the cities or towns, it would be necessary to gain more insight into the relationship of social engagement and health, and differentiate between the resources only accessible through individual connections and resources provided through social engagement.
Second, in social capital literature, neighborhood social capital or community-level social capital is important for elderly health and health behavior. But as most of the elderly in China, especially those in rural China, have permanent address, available scales could be lacking and fail to capture multiple dimensions of community-level social capital, suggesting the potential generalizability of our study to alternative models, such as hierarchical liner model and the nested level model (we thank an anonymous reviewer for this observation).




{kind=link}