Impact of the New Cooperative Medical Scheme on the Rural Residents’ Hospitalization Medical Expenses: A Five-Year Survey Study for the Jiangxi Province in China


Abstract
:1. Introduction
2. Materials and Methods
2.1. Methods
2.2. Questionnaires and Data Collection
2.3. Quality of Data
2.4. Data Analysis
3. Results
3.1. Myers Blended Index
3.2. Family Members’ Social Demographic Characteristics
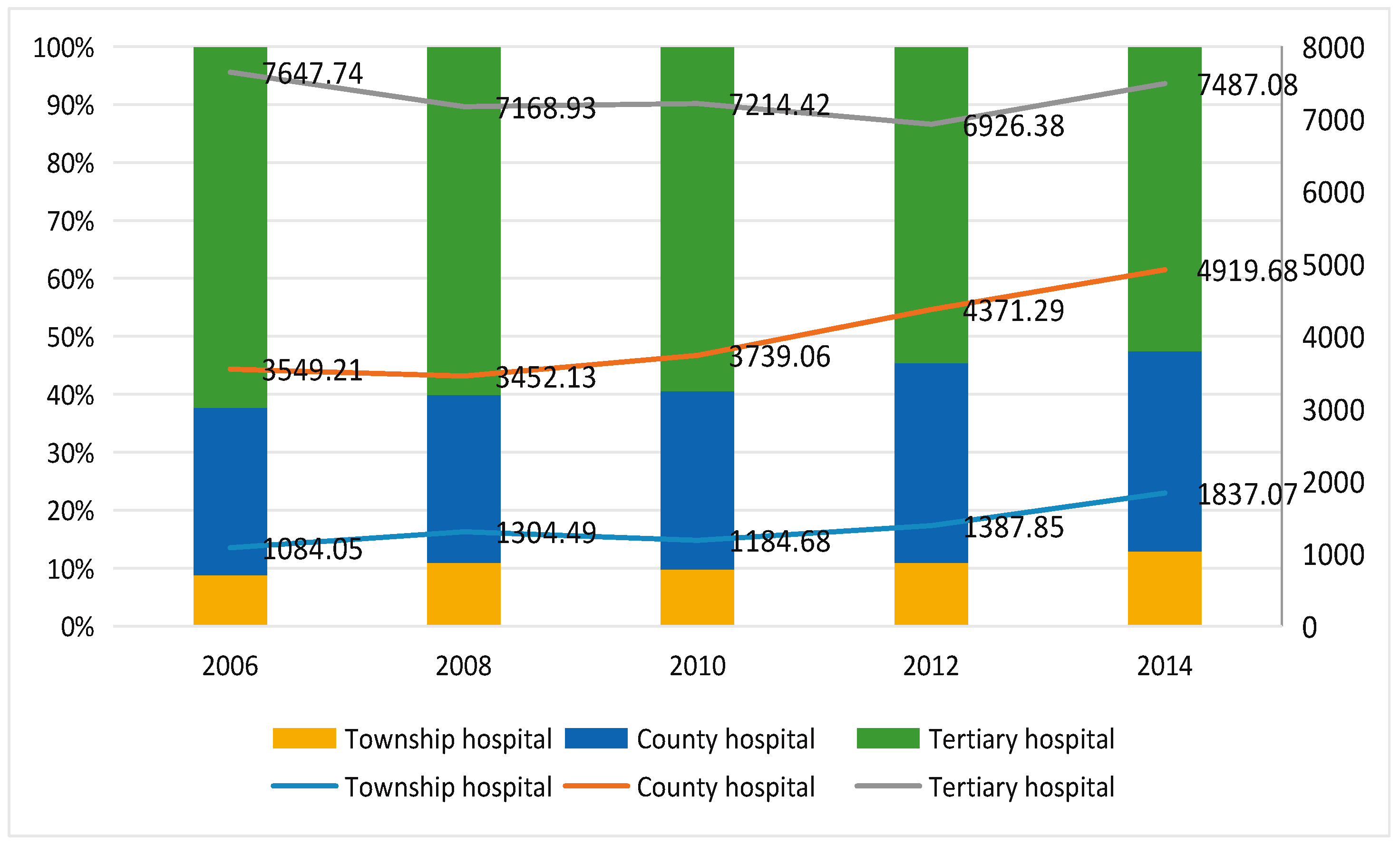
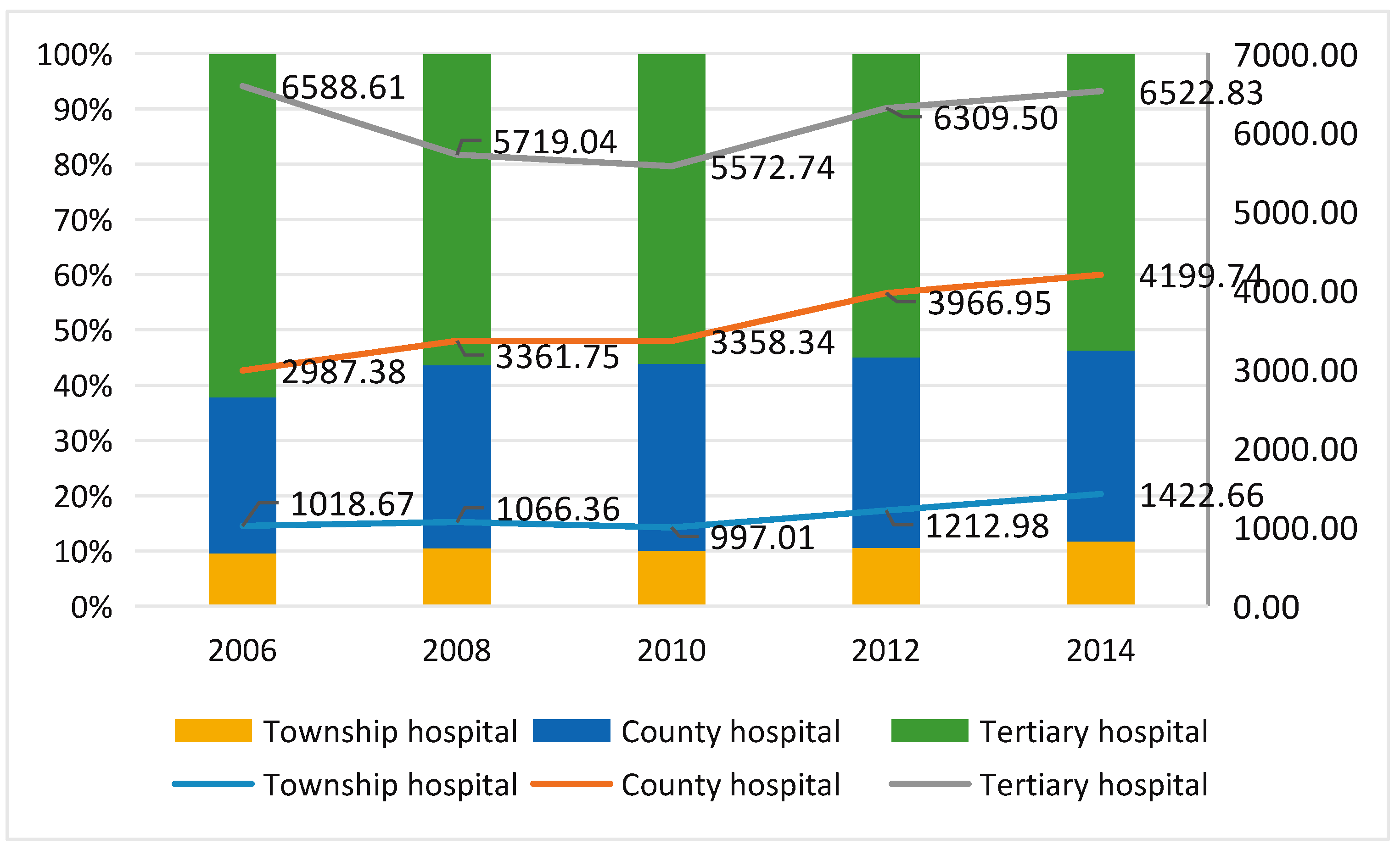
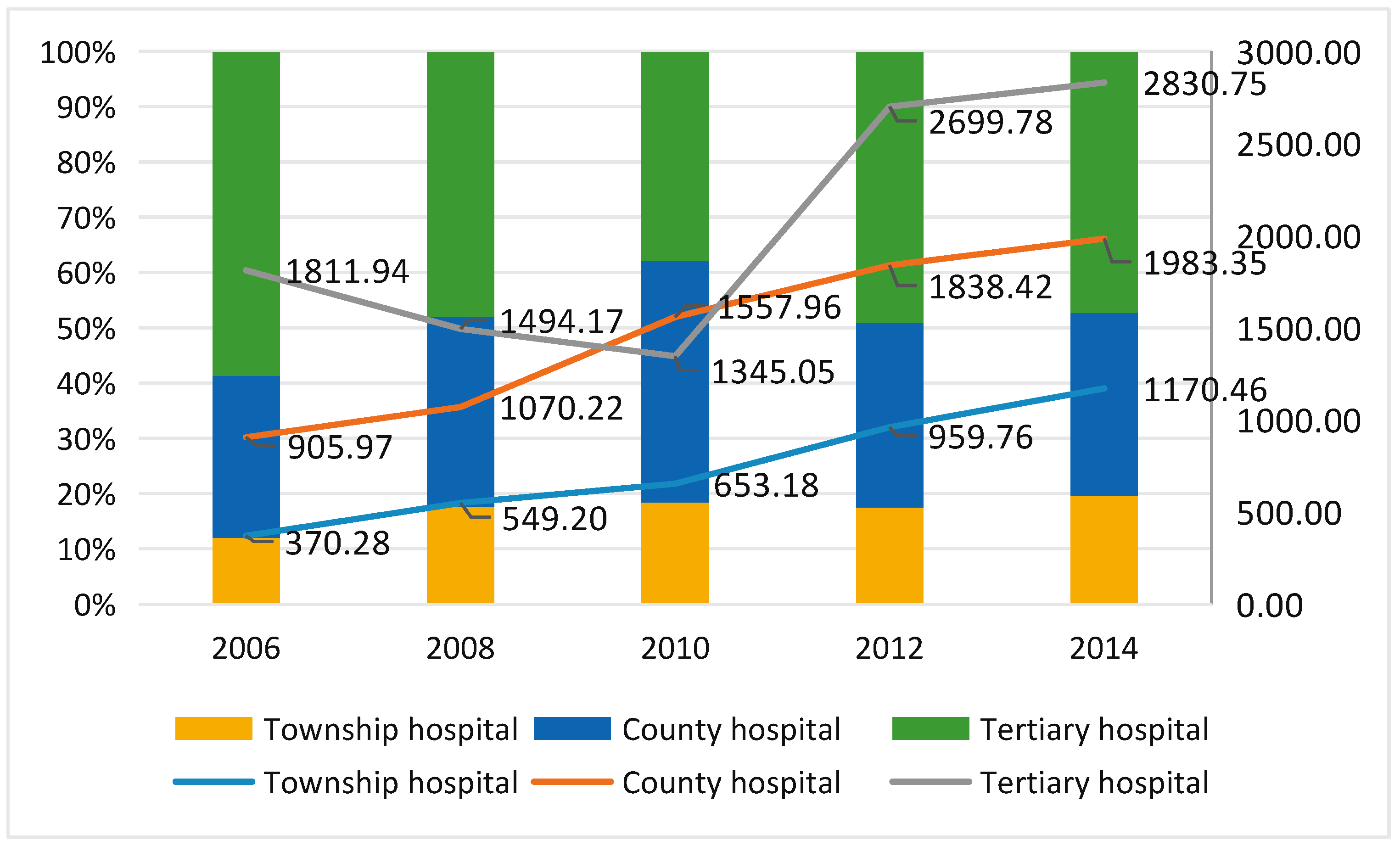
3.3. Analysis of Hospitalization Medical Expenses
4. Discussion
4.1. Per Capita and Secondary Hospitalization Expenses
4.2. Reimbursement Costs
4.3. Reimbursement of Total Medical Expenditure and Rural Residents’ Cash Expenditure on Medical Expenses
5. Limitation
6. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Wang, F.; Liang, Y. China’s Rural Cooperative Medical Scheme: A type of health insurance or a type of health cooperative? Prim. Health Care Res. Dev. 2017, 18, 194–199. [Google Scholar] [CrossRef] [PubMed]
- Pan, B.B.; Towne, S.D.; Chen, Y.X.; Yuan, Z.K. The inequity of inpatient services in rural areas and the New–Type Rural Cooperative Medical System (NRCMS) in China: Repeated cross sectional analysis. Health Policy Plan. 2017, 32, 634–636. [Google Scholar] [CrossRef] [PubMed]
- You, X.; Kobayashi, Y. The new cooperative medical scheme in China. Health Policy 2009, 91, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Dong, H.; Duan, S.; Bogg, L.; Wu, Y.; You, H.; Chen, J.; Ye, X.; Seccombe, K.; Yu, H. The impact of expanded health system reform on governmental contributions and individual copayments in the new Chinese rural cooperative medical system. Int. J. Health Plan. Manag. 2016, 31, 36–48. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.; Tang, K.K.; Zhao, L.F.; Zhang, Y.H. Will China’s Cooperative Medical scheme fail again? Insight from farmer satisfaction survey. Health Promot. Int. 2015, 30, 251–261. [Google Scholar] [CrossRef] [PubMed]
- Pan, X.L.; Zhang, Y.; Xu, L.; Huang, J.; Zhao, Q. An analysis of farmers’ perception of the new cooperative medical scheme in Liaoning Province, China. BMC Health Serv. Res. 2009, 9, 230. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Sun, X.; Zhao, Y.; Meng, Q. Financial protection of rural health insurance for patients with hypertension and diabetes: Repeated cross–sectional surveys in rural China. BMC Health Serv. Res. 2016, 16, 481. [Google Scholar] [CrossRef] [PubMed]
- Cheng, L.; Liu, H.; Zhang, Y.; Shen, K.; Zeng, Y. The Impact of Health Insurance on Health Outcomes and Spending of the Elderly: Evidence from China’s New Cooperative Medical Scheme. Health Econ. 2015, 24, 672–691. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Wang, C.T. The Association between the New Rural Cooperative Medical scheme and Health Care Seeking Behavior among Middle—Aged and Older Chinese. J. Aging Soc. Policy 2017, 29, 168–181. [Google Scholar] [CrossRef] [PubMed]
- Peng, X.B.; Conley, D. The implication of health insurance for child development and maternal nutrition: Evidence from China. Eur. J. Health Econ. 2016, 17, 521–534. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.L.; Shi, L.; Tian, F.; Zhang, L. Care Utilization with China’s New Rural Cooperative Medical Scheme: Updated Evidence from the China Health and Retirement Longitudinal Study 2011–2012. Int. J. Behav. Med. 2016, 23, 655–663. [Google Scholar] [CrossRef] [PubMed]
- Sun, M.; Shen, J.J.; Li, C.Y.; Cochran, C.; Wang, Y.; Chen, F.; Li, P.; Lu, J.; Chang, F.; Li, X.; Hao, M. Effects of China’s New Rural Cooperative Medical Scheme on reducing medical impoverishment in rural Yanbian: An alternative approach. BMC Health Serv. Res. 2016, 16, 422. [Google Scholar] [CrossRef] [PubMed]
- Yan, Z.H.; Wan, D.; Li, L. Patient satisfaction in two Chinese provinces: Rural and urban differences. Int. J. Qual Health Care 2011, 23, 384–389. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.H.; Yu, H.; Dong, H.J. Effect of the new rural cooperative medical scheme on farmers’ medical service needs and utilization in Ningbo, China. BMC Health Serv. Res. 2016, 16, 593–599. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Liu, H.; Lu, Z.X.; Luo, Q.; Liu, J.A. Role of the new rural cooperative medical scheme in alleviating catastrophic medical payments for hypertension, stroke and coronary heart disease in poor rural areas of China. BMC Public Health 2014, 14, 907–917. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.; Tsegai, D.; Litaker, D.; Braun, J. Under regional characteristics of rural China: A clearer view on the performance of the New Rural Cooperative Medical Scheme. Int. J. Health Econ. Manag. 2015, 15, 407–431. [Google Scholar] [CrossRef] [PubMed]
- Qin, X.Z.; Pan, J.; Liu, G.G. Does participating in health insurance benefit the migrant workers in China? An empirical investigation. China Econ. Rev. 2014, 30, 263–278. [Google Scholar] [CrossRef]
- Sagli, G.; Zhang, J.M.; Ingstad, B.; Fjeld, H.E. Poverty and disabled households in the People’s Republic of China: Experiences with a new rural health insurance scheme. Disabil. Soc. 2013, 28, 218–231. [Google Scholar] [CrossRef]
- Shi, W.X.; Chongsuvivatwong, V.; Geater, A.; Zhang, J.H.; Zhang, H.; Brombal, D. The influence of the rural health security schemes on health utilization and household impoverishment in rural China: Data from a household survey of western and central China. Int. J. Equity Health 2010, 9, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lei, X.; Lin, W. The New Cooperative Medical Scheme in rural China: Does more coverage mean more service and better health? Health Econ. 2009, 18, S25–S46. [Google Scholar] [CrossRef] [PubMed]
- Yang, W. Catastrophic Outpatient Health Payments and Health Payment–induced Poverty under China’s New Rural Cooperative Medical Scheme. Appl. Econ. Perspect. Policy 2015, 37, 64–85. [Google Scholar] [CrossRef]
- Bello, Y. Error Detection in Outpatients’ Age Data Using Demographic Techniques. Int. J. Pure. Appl. Sci. Technol. 2012, 10, 27–36. [Google Scholar]
- Pardeshi, G.S. Age Heaping and Accuracy of Age Data Collected During a Community Survey in the Yavatmal District, Maharashtra. Indian J. Community Med. 2010, 35, 391–395. [Google Scholar] [CrossRef] [PubMed]
- ZZhang, L.; Li, S.; Yi, H.; D’Intignano, L.M.; Ding, Y. Correlation between New Cooperative Medical Scheme Policy Design and Catastrophic Medical Payment: Evidence From 25 Counties in Rural China. Asia Pac. J. Public Health 2015, 28, 26–38. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Jackson, S.; Carmichael, G.; Sleigh, A.C. Catastrophic medical payment and financial protection in rural China: Evidence from the New Cooperative Medical Scheme in Shandong Province. Health Econ. 2009, 18, 103–119. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Gao, J.; Zhou, Z.; Yan, J.; Lai, S.; Xu, Y.; Chen, G. Assessing the Effects of the New Cooperative Medical Scheme on Alleviating the Health Payment–Induced Poverty in Shaanxi Province, China. PLoS ONE 2016, 11, e0157918. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Xu, J.; Zhang, Z.; Wang, J. New cooperative medical scheme decreased financial burden but expanded the gap of income–related inequity: Evidence from three provinces in rural China. Int. J. Equity Health 2016, 15, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Cheng, X.; Tolhurst, R.; Tang, S.; Liu, X. How effectively can the New Cooperative Medical Scheme reduce catastrophic health expenditure for the poor and non–poor in rural China? Trop. Med. Int. Health 2010, 15, 468–475. [Google Scholar] [CrossRef] [PubMed]
- Jing, S.; Yin, A.; Shi, L.; Liu, J. Whether New Cooperative Medical Schemes Reduce the Economic Burden of Chronic Disease in Rural China. PLoS ONE 2013, 8, e53062. [Google Scholar] [CrossRef] [PubMed]
- Yu, B.; Meng, Q.; Collins, C.; Tolhurst, R.; Tang, S.; Yan, F.; Bogg, L.; Liu, X. How does the New Cooperative Medical Scheme influence health service utilization? A study in two provinces in rural China. BMC Health Serv. Res. 2010, 10, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, W.A.; Ashigbie, P.G.; Brooks, M.I.; Wirtz, V.J. Comparison of medicines management strategies in insurance schemes in middle–income countries: Four case studies. J. Pharm. Policy Pract. 2016, 10, 17–26. [Google Scholar] [CrossRef] [PubMed]
- Dong, L.; Wang, D.; Gao, J.; Yan, H. Doctor’s injection prescribing and its correlates in village health clinics across 10 provinces of western China. J. Public Health 2011, 33, 565–570. [Google Scholar] [CrossRef] [PubMed]
- Xiaohong, L.; Jay, J.S.; Fang, Y.; Chunxin, J.; Fengshui, C.; Fengfeng, H.; Jun, L. Does exam–targeted training help village doctors pass the certified (assistant) physician exam and improve their practical skills? A cross–sectional analysis of village doctors’ perspectives in Changzhou in Eastern China. BMC Med. Educ. 2018, 18, 107–117. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| The Ending Figure of Age | 10–49 Years Old | 20–59 Years Old | (4) + (7) | Percentile | ǀ(9)−10ǀ c | ||||
|---|---|---|---|---|---|---|---|---|---|
| NO. | Weights | (2) × (3) a | NO. | Weights | (5) × (6) | (8)/45039 b | |||
| (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | (10) |
| 0 | 390 | 1 | 390 | 419 | 9 | 3771 | 4161 | 9.24 | 0.76 |
| 1 | 377 | 2 | 754 | 426 | 8 | 3408 | 4162 | 9.24 | 0.76 |
| 2 | 424 | 3 | 1272 | 456 | 7 | 3192 | 4464 | 9.91 | 0.09 |
| 3 | 376 | 4 | 1504 | 361 | 6 | 2166 | 3670 | 8.15 | 1.85 |
| 4 | 444 | 5 | 2220 | 482 | 5 | 2410 | 4630 | 10.28 | 0.28 |
| 5 | 518 | 6 | 3108 | 530 | 4 | 2120 | 5228 | 11.61 | 1.61 |
| 6 | 461 | 7 | 3227 | 480 | 3 | 1440 | 4667 | 10.36 | 0.36 |
| 7 | 464 | 8 | 3712 | 528 | 2 | 1056 | 4768 | 10.59 | 0.59 |
| 8 | 478 | 9 | 4302 | 517 | 1 | 517 | 4819 | 10.70 | 0.70 |
| 9 | 447 | 10 | 4470 | 477 | 0 | 0 | 4470 | 9.92 | 0.08 |
| Total | 45039 | 100.00 | 7.07 | ||||||
| Variables | 2006 | 2008 | 2010 | 2012 | 2014 |
|---|---|---|---|---|---|
| Number of interviewees | 8082 | 8015 | 7506 | 7857 | 7811 |
| Number of households | 1924 | 1879 | 1885 | 1890 | 1896 |
| Average number of family members per household | 4.20 | 4.27 | 3.98 | 4.16 | 4.12 |
| Gender a | |||||
| Male | 4144 | 4102 | 3974 | 4073 | 4054 |
| Female | 3938 | 3913 | 3532 | 3784 | 3757 |
| Female/Male | 1.05 | 1.05 | 1.13 | 1.07 | 1.08 |
| Age (%) b | |||||
| <5 | 5.88 | 6.38 | 6.59 | 7.32 | 5.94 |
| 5– | 9.63 | 10.23 | 11.02 | 12.13 | 14.15 |
| 15– | 20.18 | 17.40 | 15.07 | 12.98 | 9.85 |
| 25– | 18.30 | 18.35 | 17.03 | 17.13 | 16.68 |
| 35– | 16.56 | 15.93 | 16.39 | 15.46 | 15.47 |
| 45– | 13.02 | 13.14 | 14.65 | 14.70 | 15.76 |
| 55– | 8.64 | 9.86 | 11.06 | 11.79 | 12.34 |
| 65– | 7.81 | 8.71 | 8.19 | 8.49 | 9.82 |
| Average age (year) c | 34.26 | 34.85 | 35.54 | 35.46 | 36.60 |
| Number of hospitalizations | 129 | 304 | 429 | 628 | 747 |
| The average length of stay in hospital (day) | 13.21 | 9.55 | 9.75 | 11.40 | 11.77 |
| Variables | NO. | 2006 | 2008 | 2010 | 2012 | 2014 |
|---|---|---|---|---|---|---|
| Hospitalization expense | 1 | 3492.25 | 3324.33 | 3289.27 | 4202.51 | 4441.76 |
| Reimbursement | 2 | 852.51 | 961.94 | 1247.41 | 1789.29 | 1836.11 |
| Proportion of reimbursement (%) a | 3 | 24.41 | 28.94 | 37.92 | 42.58 | 41.34 |
| Paid by farmers | 4 | 2639.74 | 2362.39 | 2041.85 | 2413.22 | 2605.65 |
| Annual income per capita of farmers b | 5 | 4682.19 | 5559.91 | 6560.55 | 8154.60 | 9704.24 |
| 4/5 (%) c | 6 | 56.38 | 42.49 | 31.12 | 29.59 | 26.85 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xie, F.; Jiang, X.; Yuan, F.; Chen, X.; Yuan, Z.; Lu, Y. Impact of the New Cooperative Medical Scheme on the Rural Residents’ Hospitalization Medical Expenses: A Five-Year Survey Study for the Jiangxi Province in China. Int. J. Environ. Res. Public Health 2018, 15, 1368. https://doi.org/10.3390/ijerph15071368
Xie F, Jiang X, Yuan F, Chen X, Yuan Z, Lu Y. Impact of the New Cooperative Medical Scheme on the Rural Residents’ Hospitalization Medical Expenses: A Five-Year Survey Study for the Jiangxi Province in China. International Journal of Environmental Research and Public Health. 2018; 15(7):1368. https://doi.org/10.3390/ijerph15071368
Chicago/Turabian StyleXie, Fei, Xiaoqing Jiang, Fang Yuan, Xiaoyun Chen, Zhaokang Yuan, and Yuanan Lu. 2018. "Impact of the New Cooperative Medical Scheme on the Rural Residents’ Hospitalization Medical Expenses: A Five-Year Survey Study for the Jiangxi Province in China" International Journal of Environmental Research and Public Health 15, no. 7: 1368. https://doi.org/10.3390/ijerph15071368