Living Arrangements and Health-Related Quality of Life in Chinese Adolescents Who Migrate from Rural to Urban Schools: Mediating Effect of Social Support

Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Social-Demographical Characteristics
2.3. Socioeconomic Status (SES)
2.4. Social Support
2.5. Quality of Life
2.6. Data Analysis
3. Results
3.1. Characteristics of Adolescent School Children by Living Arrangement
3.2. Living with Family Children Had Higher MCS Scores and Total Social Support
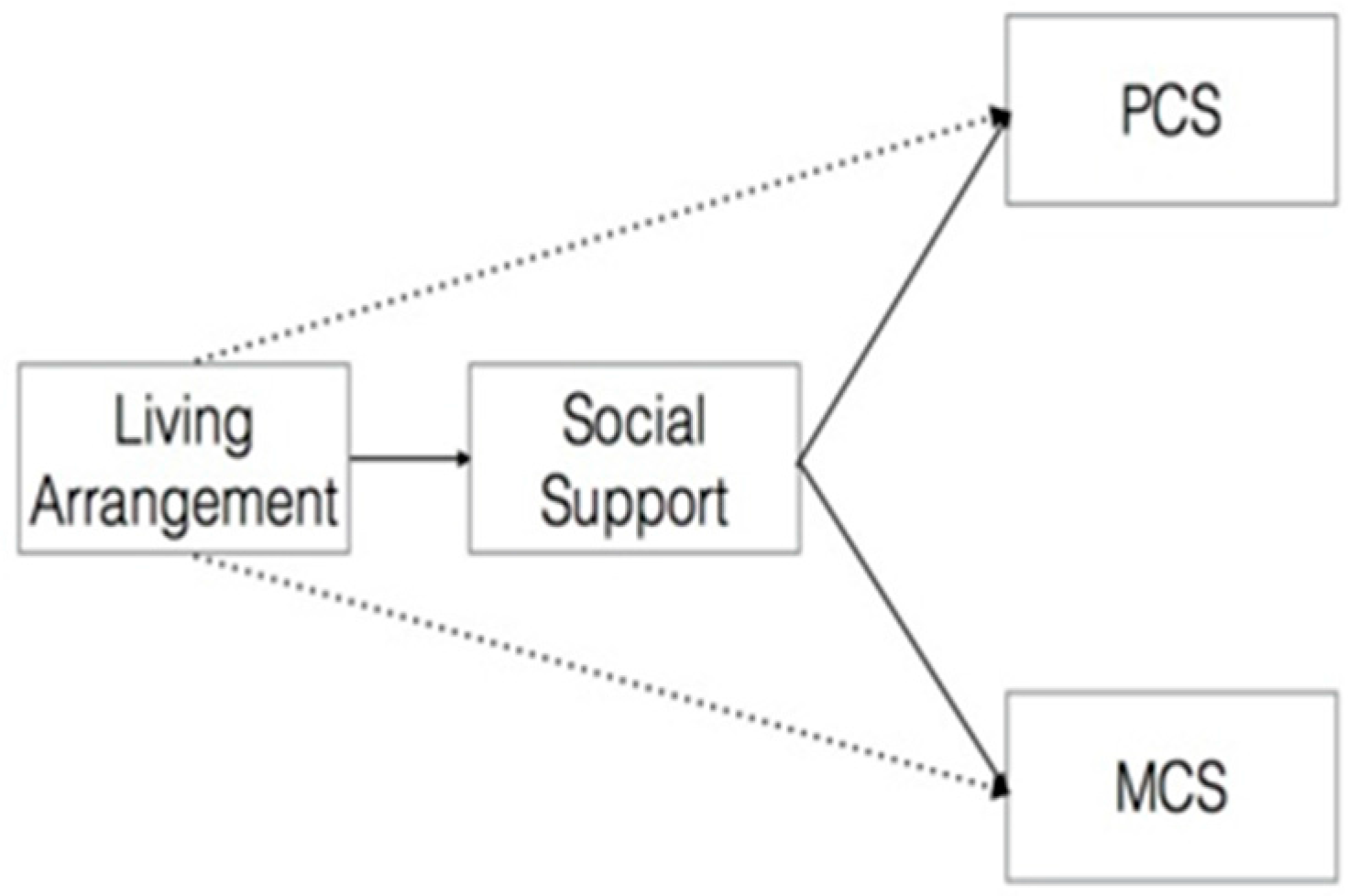
3.3. Social Support Mediation on Mental Health
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Liang, Z. China’s great migration and the prospects of a more integrated society. Annu. Rev. Sociol. 2016, 42, 451–471. [Google Scholar] [CrossRef]
- Xu, H.; Xie, Y. The causal effects of rural-to-urban migration on children’s wellbeing in China. Eur. Sociol. Rev. 2015, 31, 502–519. [Google Scholar] [CrossRef] [PubMed]
- Li, X.Y. Implementation of the layout adjustment and the two exempt and one subsidy in rural schools. Res. Educ. Dev. 2008, 57–61. [Google Scholar]
- Liang, X.Y. China: Challenges Secondary Education; The World Bank: Washington, DC, USA, 2001. [Google Scholar]
- Jia, Y.H.; Zhou, F.F. An exploration of the mapping modes of Chinese rural primary and secondary. J. Hebei Norm. Univ. 2008, 1, 13–18. [Google Scholar]
- Liu, Y.Z. A study on the dilemma of the “boarding system” in the process of rural “school closure and merger”. Leg. Syst. Soc. 2008, 7, 204. [Google Scholar]
- Villalonga-Olives, E.; Forero, C.G.; Erhart, M.; Palacio-Vieira, J.A.; Valderas, J.M.; Herdman, M.; Ferrer, M.; Rajmil, L.; Ravens-Sieberer, U.; Alonso, J. Relationship between life events and psychosomatic complaints during adolescence/youth: A structural equation model approach. J. Adolesc. Health 2011, 49, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Jonkmann, K.; Thoemmes, F.; Ludtke, O.; Trautwein, U. Personality traits and living arrangements in young adulthood: Selection and socialization. Dev. Psychol. 2014, 50, 683–698. [Google Scholar] [CrossRef] [PubMed]
- Crowder, K.; Teachman, J. Do residential conditions explain the relationship between living arrangements and adolescent behavior? J. Marriage Fam. 2004, 66, 721–738. [Google Scholar] [CrossRef]
- Finlay, J.E.; Fink, G.; McCoy, D.C.; Tavarez, L.C.; Chai, J.; Danaei, G.; Ezzati, M.; Fawzi, W.; Fawzi, M.C. Stunting risk of orphans by caregiver and living arrangement in low-income and middle-income countries. J. Epidemiol. Community Health 2016, 70, 784–790. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Li, X.; Lou, C.; Sonenstein, F.L.; Kalamar, A.; Jejeebhoy, S.; Delany-Moretlwe, S.; Brahmbhatt, H.; Olumide, A.O.; Ojengbede, O. The association between social support and mental health among vulnerable adolescents in five cities: Findings from the study of the well-being of adolescents in vulnerable environments. J. Adolesc. Health 2014, 55, S31–S38. [Google Scholar] [CrossRef] [PubMed]
- Romney, S.C.; Litrownik, A.J.; Newton, R.R.; Lau, A. The relationship between child disability and living arrangement in child welfare. Child Welf. 2006, 85, 965–984. [Google Scholar]
- Lo, C.C.; Cheng, T.C.; Bohm, M.; Zhong, H. Rural-to-urban migration, strain, and juvenile delinquency: A study of eighth-grade students in Guangzhou, China. Int. J. Offender Ther. Comp. Criminol. 2016. [Google Scholar] [CrossRef] [PubMed]
- King, V.; Stamps Mitchell, K.; Hawkins, D.N. Adolescents with two nonresident biological parents: Living arrangements, parental involvement, and well-being. J. Fam. Issues 2009, 31, 3–30. [Google Scholar] [CrossRef] [PubMed]
- Yamano, T.; Shimamura, Y.; Sserunkuuma, D. Living arrangements and schooling of orphaned children and adolescents in Uganda. Econ. Dev. Cult. Chang. 2006, 54, 833–856. [Google Scholar] [CrossRef]
- Lu, J.K.; Yin, X.J.; Xiong, J.P.; Liu, J.J.; Watanabe, T.; Tanaka, T. Comparison of the status of overweight/obesity among the youth of local Shanghai, young rural-to-urban migrants and immigrant origin areas. Int. J. Clin. Exp. Med. 2015, 8, 2804–2814. [Google Scholar] [PubMed]
- Zhuang, X.Y.; Wong, D.F. Differential impacts of social support on mental health: A comparison study of chinese rural-to-urban migrant adolescents and their urban counterparts in Beijing, China. Int. J. Soc. Psychiatry 2017, 63, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Kong, S.T.; Meng, X. The educational and health outcomes of the children of migrants the great migration rural-urban migration in China and Indonesia. In Monograph Book; Edward Elgar Publishing: Cheltenham, UK, 2008; Available online: https://www.elgaronline.com/view/9781848446441.00013.xml (accessed on 10 July 2017).
- Kooshiar, H.; Yahaya, N.; Hamid, T.A.; Abu Samah, A.; Sedaghat Jou, V. Living arrangement and life satisfaction in older malaysians: The mediating role of social support function. PLoS ONE 2012, 7, e43125. [Google Scholar] [CrossRef] [PubMed]
- Gill, M.; Chan-Golston, A.M.; Rice, L.N.; Roth, S.E.; Crespi, C.M.; Cole, B.L.; Koniak-Griffin, D.; Prelip, M.L. Correlates of social support and its association with physical activity among young adolescents. Health Educ. Behav. 2017. [Google Scholar] [CrossRef] [PubMed]
- Possel, P.; Burton, S.M.; Cauley, B.; Sawyer, M.G.; Spence, S.H.; Sheffield, J. Associations between social support from family, friends, and teachers and depressive symptoms in adolescents. J. Youth Adolesc. 2017, 10, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Wills, T.A. Stress, social support, and the buffering hypothesis. Psychol. Bull. 1985, 98, 310–357. [Google Scholar] [CrossRef] [PubMed]
- Thoits, P.A. Mechanisms linking social ties and support to physical and mental health. J. Health Soc. Behav. 2011, 52, 145–161. [Google Scholar] [CrossRef] [PubMed]
- Feeney, B.C.; Collins, N.L. A new look at social support: A theoretical perspective on thriving through relationships. Pers. Soc. Psychol. Rev. 2015, 19, 113–147. [Google Scholar] [CrossRef] [PubMed]
- Statistical Bureau of Ningxia Hui Autonomous Region: Statistical Communique of National Economic and Social Development in Yuanzhou District in 2011. National Economic Accounting Office, 2012. Available online: http://www.nxtj.gov.cn/nxtjjxbww/tjgb/2011tjgb/201310/t20131011_31913.html (accessed on 10 July 2017).
- Xiao, S.Y. Social support rating scale: The theoretical basis and research applications. J. Clin. Psychiatry 1994, 4, 98–100. [Google Scholar]
- Ma, X.; Liu, X.; Hu, X.; Qiu, C.; Wang, Y.; Huang, Y.; Wang, Q.; Zhang, W.; Li, T. Risk indicators for post-traumatic stress disorder in adolescents exposed to the 5.12 Wenchuan earthquake in China. Psychiatry Res. 2011, 189, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Wu, R.; Liu, Q.; Wang, H. Relationship of sub-health status to social support and coping styles of left-behind middle school students in a reservoir area of Chongqing. J. Hyg. Res. 2014, 43, 759–763. [Google Scholar]
- Dai, W.; Chen, L.; Tan, H.; Wang, J.; Lai, Z.; Kaminga, A.C.; Li, Y.; Liu, A. Association between social support and recovery from post-traumatic stress disorder after flood: A 13–14 year follow-up study in Hunan, China. BMC Public Health 2016, 16, 194. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.; Kosinski, M.; Keller, S. A 12-item short-form health survey: Construction of scales and preliminary tests of reliability and validity. Med. Care 1996, 34, 220–233. [Google Scholar] [CrossRef] [PubMed]
- Li, N.X.; Liu, D.P.; Liu, C.J.; Ren, X.H.; Gao, B. Assessing quality of life in an urban population in Chengdu using the sf-12. J. Sichuan Univ. 2010, 41, 1044–1046. [Google Scholar]
- Deng, C.H.; Liu, Y.; Zhang, Y.; Ji, Y.Y.; Yin, F.; Yang, S.J.; Liu, Q.L. Reliability and validity of sf-12 among adolescents in western rural areas of China. Chin. J. Public Health 2016, 1513–1516. [Google Scholar]
- Mak, K.K.; Ho, S.Y.; Fong, D.Y.; Lo, W.S.; Lai, Y.K.; Lam, T.H. Norms and demographic differences of the short form-12 health survey version 2 in Chinese adolescents. J. Paediatr. Child Health 2011, 47, 173–182. [Google Scholar] [CrossRef] [PubMed]
- Fong, D.Y.; Lam, C.L.; Mak, K.K.; Lo, W.S.; Lai, Y.K.; Ho, S.Y.; Lam, T.H. The short form-12 health survey was a valid instrument in Chinese adolescents. J. Clin. Epidemiol. 2010, 63, 1020–1029. [Google Scholar] [CrossRef] [PubMed]
- McDonald, J.H. Handbook of Biological Statistics, 3rd ed.; Sparky House Publishing: Baltimore, MD, USA, 2014; Volume 2, pp. 86–89. [Google Scholar]
- Hayes, A.F. Process: A Versatile Computational Tool for Observed Variable Mediation, Moderation, and Conditional Process Modeling [White Paper]. 2012. Available online: http://www.afhayes.com/public/process2012.pdf (accessed on 10 July 2017).
- Preacher, K.J.; Hayes, A.F. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav. Res. Methods 2008, 40, 879–891. [Google Scholar] [CrossRef] [PubMed]
- Jia, X.; Liu, X. Perceived discrimination and antisocial behaviour among chinese rural-to-urban migrant adolescents: Mediating effects of social support. Int. J. Psychol. 2017, 52, 327–335. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, B.N.; Keys, H.M.; Foster, J.; Kohrt, B.A. Social stressors, social support, and mental health among haitian migrants in the Dominican Republic. Rev. Panam. Salud Publica 2015, 38, 157–162. [Google Scholar] [PubMed]
- Oppedal, B.; Roysamb, E. Mental health, life stress and social support among young norwegian adolescents with immigrant and host national background. Scand. J. Psychol. 2004, 45, 131–144. [Google Scholar] [CrossRef] [PubMed]
- Thoits, P.A. Stress and health: Major findings and policy implications. J. Health Soc. Behav. 2010, 51, S41–S53. [Google Scholar] [CrossRef] [PubMed]
- Kasamaki, J. Study on health support strategies by analyzing the diet, alcohol intake, and smoking behavior of university students: Examination of non-communicable disease risk factors according to their sex, age and living arrangement. Nihon Ketsueki Gakkai Zasshi 2015, 70, 81–94. [Google Scholar] [CrossRef] [PubMed]
- Gfroerer, J.C.; Greenblatt, J.C.; Wright, D.A. Substance use in the us college-age population: Differences according to educational status and living arrangement. Am. J. Public Health 1997, 87, 62–65. [Google Scholar] [CrossRef] [PubMed]
- Nelson, R.G. Residential context, institutional alloparental care, and child growth in Jamaica. Am. J. Hum. Biol. 2016, 28, 493–502. [Google Scholar] [CrossRef] [PubMed]
- Lupi, S.; Bagordo, F.; Stefanati, A.; Grassi, T.; Piccinni, L.; Bergamini, M.; De Donno, A. Assessment of lifestyle and eating habits among undergraduate students in Northern Italy. Ann. Ist. Super. Sanita 2015, 51, 154–161. [Google Scholar] [PubMed]
- Meade, T.; Dowswell, E. Adolescents’ health-related quality of life (hrqol) changes over time: A three year longitudinal study. Health Quality Life Outcomes 2016, 14, 14. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Name | Characteristics | Number and Proportion of Graduates in 2017 |
|---|---|---|
| Wuyuan middle school | Private school, key school, since 1941 | 890 (17.3%) |
| Hongwen middle school | Private school, key school, since 1973 | 814 (15.80%) |
| The Third middle school | Public school, since 1979 | 1043 (20.20%) |
| Muslim Secondary school | Public school, more than half of the students are Hui ethnic group, since 1984 | 325 (6.30%) |
| The Fourth middle school | Public school, since 1985 | 463 (9.00%) |
| The Fifth middle school | public school, rebuilt and relocated under the policy of closures and consolidations in 2002 1 | 281 (5.5%) |
| The Sixth middle school | Public school, the newest school for Urbanization with increased number of students, since 2003 | 1017 (19.7%) |
| The Seventh middle school | Public school, rebuilt and relocated under the policy of closures and consolidations in 2006 2 | 322 (6.25%) |
| Variables | Total (n = 459) | Living with Family (n = 283) | Not Living with Family (n = 176) | X2 | p | |||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |||
| Control variables | ||||||||
| Ethnic groups | 0.111 | 0.815 | ||||||
| Han | 361 | 78.6 | 224 | 79.2 | 137 | 77.8 | ||
| Hui | 98 | 21.4 | 59 | 20.8 | 39 | 22.2 | ||
| Sex | 0.877 | 0.388 | ||||||
| male | 237 | 51.6 | 151 | 53.4 | 86 | 48.9 | ||
| female | 222 | 48.4 | 132 | 46.6 | 90 | 51.1 | ||
| Have you felt uncomfortable at any time during the last 14 days | 1.409 | 0.262 | ||||||
| yes | 62 | 13.5 | 34 | 12.0 | 28 | 15.9 | ||
| No | 397 | 86.5 | 249 | 88.0 | 148 | 84.1 | ||
| Do you have a chronic health problem | 6.253 | 0.017 | ||||||
| Yes | 22 | 4.8 | 7 | 2.5 | 13 | 7.4 | ||
| No | 437 | 95.2 | 272 | 97.5 | 161 | 91.5 | ||
| SES | ||||||||
| Father’s educational level | 1.546 | 0.672 | ||||||
| Illiterate | 41 | 8.9 | 24 | 8.8 | 17 | 10.0 | ||
| Primary school | 152 | 33.1 | 94 | 34.3 | 58 | 34.1 | ||
| Junior middle school | 149 | 33.6 | 97 | 35.4 | 52 | 30.6 | ||
| High school or higher | 102 | 22.2 | 59 | 21.5 | 43 | 25.3 | ||
| Mother’s educational level | 2.856 | 0.416 | ||||||
| Illiterate | 117 | 25.5 | 76 | 27.6 | 41 | 24.3 | ||
| Primary school | 153 | 33.3 | 87 | 31.6 | 66 | 39.1 | ||
| Junior middle school | 125 | 27.2 | 82 | 29.8 | 43 | 25.4 | ||
| High school or higher | 49 | 10.7 | 30 | 10.9 | 19 | 11.2 | ||
| Annual per capita income | 3.239 | 0.198 | ||||||
| <2500 | 161 | 37.4 | 108 | 40.6 | 53 | 32.1 | ||
| 2500–5500 | 143 | 33.2 | 85 | 32 | 58 | 35.2 | ||
| >5500 | 127 | 29.5 | 73 | 27.4 | 54 | 32.7 | ||
| Health-related behavior | ||||||||
| Drinking alcohol | 7.9 | 0.005 | ||||||
| No | 350 | 92.1 | 230 | 95.0 | 120 | 87.0 | ||
| Yes | 30 | 7.9 | 12 | 5.0 | 18 | 13.0 | ||
| Regular exercise | 0.01 | 0.991 | ||||||
| Yes | 349 | 91.8 | 217 | 91.9 | 132 | 91.7 | ||
| No | 31 | 8.2 | 19 | 8.1 | 12 | 8.3 | ||
| Variables | Total | Living with Family (n = 283) | Not Living with Family (n = 176) | t | p | Cohen‘s d | |||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | ||||
| PCS | 51.61 | 7.13 | 51.81 | 6.59 | 51.29 | 7.93 | −0.727 | 0.47 | 0.07 |
| MCS | 47.35 | 9.75 | 48.74 | 8.97 | 45.10 | 10.53 | −3.807 | 0.00 | 0.37 |
| Objective Support | 8.21 | 1.89 | 8.62 | 1.80 | 7.56 | 1.84 | −6.112 | 0.00 | 0.59 |
| Subjective Support | 21.00 | 2.78 | 20.92 | 2.75 | 21.14 | 2.83 | 0.829 | 0.41 | 0.08 |
| Availability Support | 8.01 | 1.86 | 8.04 | 1.88 | 7.96 | 1.83 | −0.460 | 0.65 | 0.04 |
| Global Support | 37.22 | 4.63 | 37.58 | 4.52 | 36.65 | 4.77 | −2.091 | 0.04 | 0.20 |
| Unadjusted | Effect | SE | t | p | LLCI | ULCI |
| Total effect | 3.5753 | 0.9225 | 3.8758 | 0.0001 | 1.7625 | 5.3881 |
| Direct Effect | 3.3096 | 0.9184 | 3.6039 | 0.0003 | 1.5049 | 5.1144 |
| Indirect effect | Effect | bootSE | bootLLCI | bootULCI | ||
| Global support | 0.2657 | 0.1598 | 0.028 | 0.6902 | ||
| Adjusted (by sex and ethnicity) | Effect | SE | t | p | LLCI | ULCI |
| Total effect | 3.4931 | 0.9225 | 3.8758 | 0.0001 | 1.7625 | 5.3881 |
| Direct Effect | 3.2175 | 0.9174 | 3.5071 | 0.0005 | 1.4145 | 5.0205 |
| Indirect effect | Effect | bootSE | bootLLCI | bootULCI | ||
| Global support | 0.2756 | 0.1624 | 0.0365 | 0.6968 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, H.; Wu, S.; Wu, H.; Xia, Q.; Li, N. Living Arrangements and Health-Related Quality of Life in Chinese Adolescents Who Migrate from Rural to Urban Schools: Mediating Effect of Social Support. Int. J. Environ. Res. Public Health 2017, 14, 1249. https://doi.org/10.3390/ijerph14101249
Wu H, Wu S, Wu H, Xia Q, Li N. Living Arrangements and Health-Related Quality of Life in Chinese Adolescents Who Migrate from Rural to Urban Schools: Mediating Effect of Social Support. International Journal of Environmental Research and Public Health. 2017; 14(10):1249. https://doi.org/10.3390/ijerph14101249
Chicago/Turabian StyleWu, Haiyan, Shan Wu, Haibo Wu, Qiming Xia, and Ningxiu Li. 2017. "Living Arrangements and Health-Related Quality of Life in Chinese Adolescents Who Migrate from Rural to Urban Schools: Mediating Effect of Social Support" International Journal of Environmental Research and Public Health 14, no. 10: 1249. https://doi.org/10.3390/ijerph14101249