
Domain-Specific Self-Reported and Objectively Measured Physical Activity in Children

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
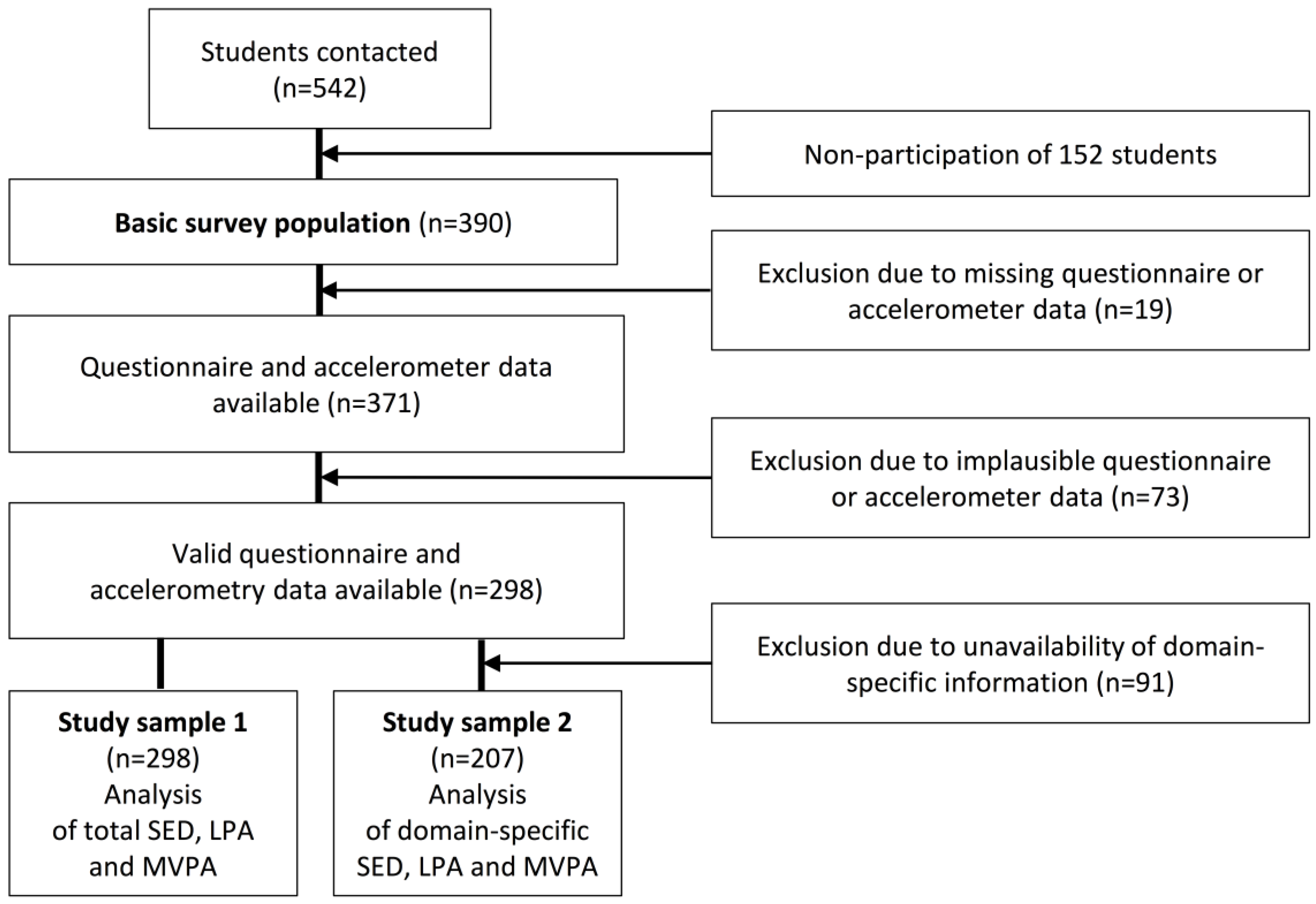
2.1. Study Sample
2.2. Data Collection
2.2.1. Accelerometry
2.2.2. Accelerometer Diary
2.2.3. Seven-Day Recall PA Questionnaire (PAQ)
2.2.4. Time-Stamping of PA Data
2.2.5. Analysis Group
2.3. Statistical Analysis
3. Results
3.1. Descriptive Values
3.2. Duration and Proportion of SED, LPA and MVPA in Different Domains
3.3. Correlation of Self-Reported and Objectively Measured Total SED, LPA and MVPA
3.4. Domain-Specific Correlation for SED, LPA and MVPA
4. Discussion
4.1. Differences of Age- and Sex-Specific PA
4.2. Differences of Domain-Specific PA
4.3. Strengths and Limitations
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Availability of Data
References
- Andersen, L.B.; Riddoch, C.; Kriemler, S.; Hills, A.P. Physical activity and cardiovascular risk factors in children. Br. J. Sports Med. 2011, 45, 871–876. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janssen, I.; Leblanc, A.G. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int. J. Behave. Nutr. Phys. Act. 2010, 7. [Google Scholar] [CrossRef] [PubMed]
- Strong, W.B.; Malina, R.M.; Blimkie, C.J.; Daniels, S.R.; Dishman, R.K.; Gutin, B.; Hergenroeder, A.C.; Must, A.; Nixon, P.A.; Pivarnik, J.M.; et al. Evidence based physical activity for school-age youth. J. Pediatr. 2005, 146, 732–737. [Google Scholar] [CrossRef] [PubMed]
- Hallal, P.C.; Andersen, L.B.; Bull, F.C.; Guthold, R.; Haskell, W.; Ekelund, U. Global physical activity levels: Surveillance progress, pitfalls, and prospects. Lancet 2012, 380, 247–257. [Google Scholar] [CrossRef]
- Konstabel, K.; Veidebaum, T.; Verbestel, V.; Moreno, L.A.; Bammann, K.; Tornaritis, M.; Eiben, G.; Molnar, D.; Siani, A.; Sprengeler, O.; et al. Objectively measured physical activity in European children: The IDEFICS study. Int. J. Obes. 2014, 38, S135–S143. [Google Scholar] [CrossRef] [PubMed]
- Bailey, D.P.; Fairclough, S.J.; Savory, L.A.; Denton, S.J.; Pang, D.; Deane, C.S.; Kerr, C.J. Accelerometry-assessed sedentary behaviour and physical activity levels during the segmented school day in 10–14-year-old children: The HAPPY study. Eur. J. Pediatr. 2012, 171, 1805–1813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chinapaw, M.J.; Proper, K.I.; Brug, J.; van Mechelen, W.; Singh, A.S. Relationship between young peoples’ sedentary behaviour and biomedical health indicators: A systematic review of prospective studies. Obes. Rev. Off. J. Int. Assoc. Stud. Obes. 2011, 12, e621–e632. [Google Scholar] [CrossRef] [PubMed]
- Pratt, M.; Macera, C.A.; Sallis, J.F.; O’Donnell, M.; Frank, L.D. Economic interventions to promote physical activity: Application of the SLOTH model. Am. J. Prev. Med. 2004, 27, 136–145. [Google Scholar] [CrossRef] [PubMed]
- Escalante, Y.; Garcia-Hermoso, A.; Backx, K.; Saavedra, J.M. Playground designs to increase physical activity levels during school recess: A systematic review. Health Educ. Behav. Off. Publ. Soc. Public Health Educ. 2014, 41, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Guinhouya, B.C.; Lemdani, M.; Apété, G.K.; Durocher, A.; Vilhelm, C.; Hubert, H. How school time physical activity is the “Big One” for daily activity among schoolchildren: A semi-experimental approach. J. Phys. Act. Health 2009, 6, 510–519. [Google Scholar] [CrossRef] [PubMed]
- Trost, S.G. State of the art reviews: Measurement of physical activity in children and adolescents. Am. J. Lifestyle Med. 2007, 1, 299–314. [Google Scholar] [CrossRef]
- Nilsson, A.; Andersen, L.B.; Ommundsen, Y.; Froberg, K.; Sardinha, L.B.; Piehl-Aulin, K.; Ekelund, U. Correlates of objectively assessed physical activity and sedentary time in children: A cross-sectional study (The European Youth Heart Study). BMC Public Health 2009, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Sluijs, E.M.; Fearne, V.A.; Mattocks, C.; Riddoch, C.; Griffin, S.J.; Ness, A. The contribution of active travel to children’s physical activity levels: Cross-sectional results from the ALSPAC study. Prev. Med. 2009, 48, 519–524. [Google Scholar] [CrossRef] [PubMed]
- Adamo, K.B.; Prince, S.A.; Tricco, A.C.; Connor-Gorber, S.; Tremblay, M. A comparison of indirect versus direct measures for assessing physical activity in the pediatric population: A systematic review. Int. J. Pediatr. Obes. IJPO Off. J. Int. Assoc. Stud. Obes. 2009, 4, 2–27. [Google Scholar] [CrossRef] [PubMed]
- Helmerhorst, H.; Brage, S.; Warren, J.; Besson, H.; Ekelund, U. A systematic review of reliability and objective criterion-related validity of physical activity questionnaires. Int. J. Behav. Nutr. Phys. Act. 2012, 103, 1–55. [Google Scholar] [CrossRef] [PubMed]
- Ekelund, U.; Tomkinson, G.; Armstrong, N. What proportion of youth are physically active? Measurement issues, levels and recent time trends. Br. J. Sports Med. 2011, 45, 859–865. [Google Scholar] [CrossRef] [PubMed]
- Ridgers, N.D.; Salmon, J.; Ridley, K.; O’Connell, E.; Arundell, L.; Timperio, A. Agreement between activPAL and ActiGraph for assessing children’s sedentary time. Int. J. Behav. Nutr. Phys. Act. 2012, 9. [Google Scholar] [CrossRef] [PubMed]
- Reilly, J.J.; Penpraze, V.; Hislop, J.; Davies, G.; Grant, S.; Paton, J.Y. Objective measurement of physical activity and sedentary behaviour: Review with new data. Arch. Dis. Childhood 2008, 93, 614–619. [Google Scholar] [CrossRef] [PubMed]
- Westerterp, K.R. Assessment of physical activity: A critical appraisal. Eur. J. Appl. Physiol. 2009, 105, 823–828. [Google Scholar] [CrossRef] [PubMed]
- Nettlefold, L.; McKay, H.A.; Warburton, D.E.; McGuire, K.A.; Bredin, S.S.; Naylor, P.J. The challenge of low physical activity during the school day: At recess, lunch and in physical education. Br. J. Sports Med. 2011, 45, 813–819. [Google Scholar] [CrossRef] [PubMed]
- Rainham, D.G.; Bates, C.J.; Blanchard, C.M.; Dummer, T.J.; Kirk, S.F.; Shearer, C.L. Spatial classification of youth physical activity patterns. Am. J. Prev. Med. 2012, 42, e87–e96. [Google Scholar] [CrossRef] [PubMed]
- Grow, H.M.; Saelens, B.E.; Kerr, J.; Durant, N.H.; Norman, G.J.; Sallis, J.F. Where are youth active? Roles of proximity, active transport, and built environment. Med. Sci. Sports Exerc. 2008, 40, 2071–2079. [Google Scholar] [CrossRef] [PubMed]
- Hanggi, J.M.; Phillips, L.R.; Rowlands, A.V. Validation of the GT3X ActiGraph in children and comparison with the GT1M ActiGraph. J. Sci. Med. Sport/Sports Med. Aust. 2013, 16, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Robusto, K.M.; Trost, S.G. Comparison of three generations of ActiGraph activity monitors in children and adolescents. J. Sports Sci. 2012, 30, 1429–1435. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, J.E.; John, D.; Freedson, P.S. Validation and comparison of ActiGraph activity monitors. J. Sci. Med. Sport/Sports Med. Aust. 2011, 14, 411–416. [Google Scholar] [CrossRef] [PubMed]
- Vanhelst, J.; Mikulovic, J.; Bui-Xuan, G.; Dieu, O.; Blondeau, T.; Fardy, P.; Beghin, L. Comparison of two ActiGraph accelerometer generations in the assessment of physical activity in free living conditions. BMC Res. Notes 2012, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, L.; Liu, Z.; Matthews, C.E.; Buchowski, M.S. Validation of accelerometer wear and nonwear time classification algorithm. Med. Sci. Sports Exerc. 2011, 43, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Evenson, K.R.; Catellier, D.J.; Gill, K.; Ondrak, K.S.; McMurray, R.G. Calibration of two objective measures of physical activity for children. J. Sports Sci. 2008, 26, 1557–1565. [Google Scholar] [CrossRef] [PubMed]
- Jekauc, D.; Wagner, M.O.; Kahlert, D.; Woll, A. Reliability and validity of MoMo-Physical-Activity-Questionnaire for Adolescents (MoMo-AFB). Diagnostica 2013, 59, 100–111. [Google Scholar] [CrossRef]
- Tukey, J. Exploratory Data Analysis; Addison-Wesley: Reading, MA, USA, 1977. [Google Scholar]
- Landis, J.T.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed]
- Ridgers, N.D.; Stratton, G.; Fairclough, S.J.; Twisk, J.W.R. Children’s physical activity levels during school recess a quasi-experimental intervention study. Int. J. Behav. Nutr. Phys. Act. 2007, 4. [Google Scholar] [CrossRef] [PubMed]
- Lampert, T.; Mensink, G.B.; Romahn, N.; Woll, A. Physical activity among children and adolescents in Germany. Results of the German Health Interview and Examination Survey for Children and Adolescents (KiGGS). Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2007, 50, 634–642. [Google Scholar] [CrossRef] [PubMed]
- Nader, P.R.; Bradley, R.H.; Houts, R.M.; McRitchie, S.L.; O’Brien, M. Moderate-to-vigorous physical activity from ages 9 to 15 years. JAMA 2008, 300, 295–305. [Google Scholar] [CrossRef] [PubMed]
- Guinhouya, B.C.; Samouda, H.; de Beaufort, C. Level of physical activity among children and adolescents in Europe: A review of physical activity assessed objectively by accelerometry. Public Health 2013, 127, 301–311. [Google Scholar] [CrossRef] [PubMed]
- Klinker, C.D.; Schipperijn, J.; Christian, H.; Kerr, J.; Ersboll, A.K.; Troelsen, J. Using accelerometers and global positioning system devices to assess gender and age differences in children’s school, transport, leisure and home based physical activity. Int. J. Behav. Nutr. Phys. Act. 2014, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rowlands, A.V.; Eston, R.G. The measurement and interpretation of children’s physical activity. J. Sports Sci. Med. 2007, 6, 270–276. [Google Scholar] [PubMed]
- Corder, K.; Ekelund, U.; Steele, R.M.; Wareham, N.J.; Brage, S. Assessment of physical activity in youth. J. Appl. Physiol. 2008, 105, 977–987. [Google Scholar] [CrossRef] [PubMed]
- Cain, K.L.; Sallis, J.F.; Conway, T.L.; Van Dyck, D.; Calhoon, L. Using accelerometers in youth physical activity studies: A review of methods. J. Phys. Act. Health 2013, 10, 437–450. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Sociodemographic Data | Girls (n = 141) | Boys (n = 157) | Children (6–10 Years) (n = 207) | Adolescents (11–17 Years) (n = 91) | Weekdays | Weekend Days | All (n = 298) |
|---|---|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | ||||
| Age (years) | 10.1 (2.6) | 10.5 (2.8) | 8.5 (1.1) | 13.6 (1.3) | - | - | 10.4 (2.9) |
| BMI (kg/m2) | 17.2 (3.1) | 17.8 (3.8) | 16.1 (2) | 20.2 (4) | - | - | 17.6 (3.5) |
| ISCED 1 | |||||||
| Low/medium (%) | 24.8 | 26.1 | 20.3 | 34.8 | - | - | 25.5 |
| High (%) | 61.7 | 62.4 | 75.5 | 37.7 | - | - | 62.1 |
| Accelerometry | |||||||
| Wear-time (days) | 6.1 (1) | 6.1 (1.1) | 6.2 (0.9) | 6 (1.2) | 4.5 (0.8) | 1.6 (0.5) | 6.1 (1) |
| Wear-time (min/day) | 776 (53) | 789 (98) | 766 (71) | 814 (85) | 799 (80) | 739 (108) | 783 (80) |
| SED (min/day) | 555 (77) | 548 (116) | 512 (77) | 623 (96) | 556 (102) | 539 (117) | 551 (100) |
| LPA (min/day) | 159 (34) | 166 (38) | 179 (28) | 134 (31) | 170 (37) | 145 (43) | 163 (36) |
| MVPA (min/day) | 62 (18) | 74 (24) | 75 (20) | 56 (21) | 73 (24) | 55 (28) | 68 (22) |
| >60 min MVPA (%) | 52 | 70 | 76 | 36 | 69 | 41 | 62 |
| Questionnaire | |||||||
| SED (min/day) | 463 (110) | 463 (112) | 435 (94) | 523 (121) | 477 (132) | 439 (164) | 463 (111) |
| LPA (min/day) | 207 (81) | 180 (91) | 195 (88) | 189 (87) | 166 (91) | 258 (159) | 193 (87) |
| MVPA (min/day) | 100 (81) | 131 (85) | 118 (78) | 113 (94) | 112 (81) | 125 (127) | 116 (84) |
| >60 min MVPA (%) | 62 | 76 | 74 | 61 | 71 | 59 | 70 |
| Domain | SED PAQ | SED ACC | LPA PAQ | LPA ACC | MVPA PAQ | MVPA ACC | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean (SD) | % (Day) | Mean (SD) | % (Day) | Mean (SD) | % (Day) | Mean (SD) | % (Day) | Mean (SD) | % (Day) | Mean (SD) | % (Day) | |
| Transport (min/day) | 3 (9) | 1 | 13 (6) | 3 | 20 (13) | 11 | 11 (4) | 5 | 2 (7) | 1 | 7 (4) | 7 |
| School time (min/day) | 247 (114) | 52 | 271 (38) | 55 | 50 (41) | 27 | 103 (22) | 53 | 35 (39) | 20 | 41 (14) | 46 |
| Physical education (min/week) | 36 (42) | 1 | 66 (44) | 2 | 17 (50) | 2 | 50 (28) | 4 | 116 (72) | 13 | 39 (23) | 8 |
| Leisure time (min/day) | 183 (94) | 39 | 182 (50) | 37 | 98 (70) | 56 | 56 (16) | 29 | 49 (57) | 30 | 21 (9) | 23 |
| Organized sports activities (min/week) | 56 (39) | 7 | 41 (36) | 4 | 12 (41) | 4 | 37 (27) | 9 | 100 (80) | 35 | 32 (28) | 16 |
| Age Group | SED | LPA | MVPA | >60 Min MVPA | ||||
|---|---|---|---|---|---|---|---|---|
| rS | 95% CI | rS | 95% CI | rS | 95% CI | κ | 95% CI | |
| Children (n = 207) | 0.28 | 0.15–0.41 | 0.14 | −0.01–0.28 | 0.20 | 0.06–0.34 | 0.04 | −0.11–0.18 |
| Adolescents (n = 91) | 0.35 | 0.15–0.52 | −0.03 | −0.22–0.16 | 0.21 | 0.02–0.39 | 0.24 | 0.08–0.40 |
| All (n = 298) | 0.44 | 0.34–0.53 | 0.09 | −0.03–0.20 | 0.21 | 0.10–0.32 | 0.17 | 0.06–0.28 |
| Domain | SED | LPA | MVPA | |||
|---|---|---|---|---|---|---|
| rS | 95% CI | rS | 95% CI | rS | 95% CI | |
| Transport | 0.24 | 0.11–0.37 | 0.59 | 0.49–0.67 | 0.12 | −0.01–0.26 |
| School time | 0.18 | 0.04–0.31 | 0.14 | −0.01–0.27 | 0.16 | 0.02–0.29 |
| Physical education | 0.03 | −0.12–0.18 | −0.03 | −0.18–0.12 | 0.18 | 0.03–0.32 |
| Leisure time | 0.34 | 0.21–0.46 | 0.07 | −0.07–0.21 | 0.12 | −0.02–0.25 |
| Organized sports activities | −0.11 | −0.30–0.10 | −0.01 | −0.22–0.19 | 0.54 | 0.38–0.67 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sprengeler, O.; Wirsik, N.; Hebestreit, A.; Herrmann, D.; Ahrens, W. Domain-Specific Self-Reported and Objectively Measured Physical Activity in Children. Int. J. Environ. Res. Public Health 2017, 14, 242. https://doi.org/10.3390/ijerph14030242
Sprengeler O, Wirsik N, Hebestreit A, Herrmann D, Ahrens W. Domain-Specific Self-Reported and Objectively Measured Physical Activity in Children. International Journal of Environmental Research and Public Health. 2017; 14(3):242. https://doi.org/10.3390/ijerph14030242
Chicago/Turabian StyleSprengeler, Ole, Norman Wirsik, Antje Hebestreit, Diana Herrmann, and Wolfgang Ahrens. 2017. "Domain-Specific Self-Reported and Objectively Measured Physical Activity in Children" International Journal of Environmental Research and Public Health 14, no. 3: 242. https://doi.org/10.3390/ijerph14030242