
Prevalence of Mental Disorders in 6–16-Year-Old Students in Sichuan Province, China

Abstract
:1. Introduction
2. Participants and Methods
2.1. Participants
2.2. Sociodemographic Characteristics
2.3. The Screening Tool
2.4. Diagnostic Criteria and Tools
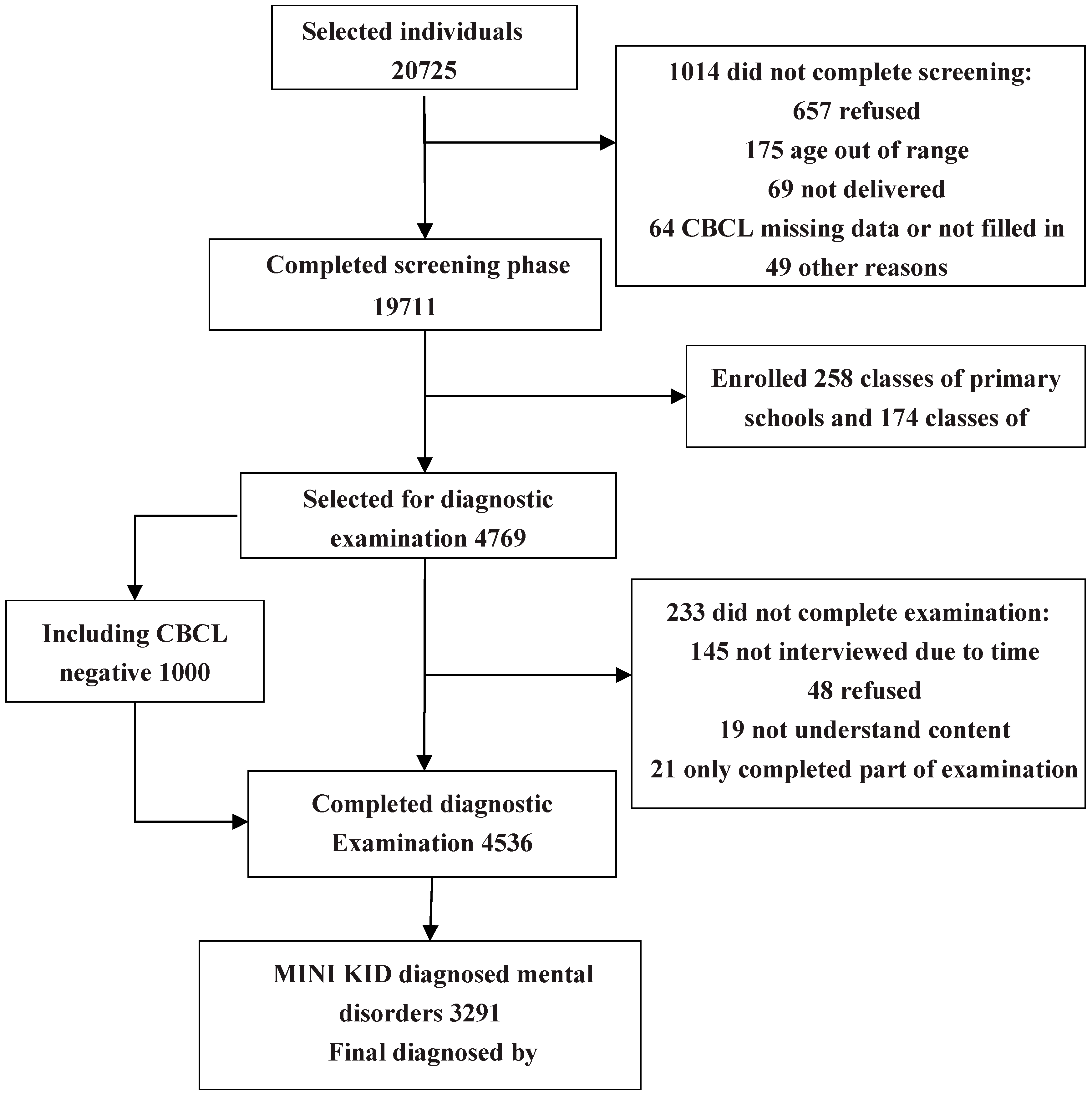
2.5. Study Procedures
2.6. Statistical Analysis
2.7. Ethical Approval

3. Results
3.1. Participant Characteristics
3.2. Detection of Behavioral Problems in Children

{kind=link}
| Variable | Sample | Rate (%) | χ2 | p Value | Cramer’s V |
|---|---|---|---|---|---|
| Gender ** | |||||
| Boys | 2164 | 21.78 | 91.27 | 0.003 | 0.068 |
| Girls | 1605 | 16.42 | |||
| Age * | |||||
| 6–7 | 356 | 14.23 | 51.98 | 0.026 | 0.051 |
| 8–10 | 898 | 20.16 | |||
| 11–13 | 1123 | 18.73 | |||
| 14–16 | 1392 | 20.60 | |||
| Community | |||||
| Rural | 2204 | 19.42 | 1.56 | 0.213 | 0.009 |
| Urban | 1565 | 18.71 | |||
| Caregiver ** | |||||
| Parents | 1362 | 11.00 | 1419.04 | 0.001 | 0.268 |
| Left-behind | 2407 | 32.83 | |||
| Cities * | |||||
| Chengdu | 801 | 16.95 | 32.47 | 0.014 | 0.041 |
| Neijiang | 924 | 18.36 | |||
| Dazhou | 959 | 19.82 | |||
| Bazhong | 1085 | 21.22 | |||
3.3. Overall Point Prevalence Distribution of Mental Disorders
| DSM-IV Disorders | n | % | 95% CI |
|---|---|---|---|
| Any disorders | 3003 | 15.24 | 14.74–15.74 |
| Affective disorders | 588 | 2.99 | 1.35–3.22 |
| Major depressive disorder | 375 | 1.90 | 1.71–2.09 |
| Dysthymia | 54 | 0.27 | 0.20–0.35 |
| Mania or hypomania | 159 | 0.81 | 0.68–0.93 |
| Anxiety disorders | 777 | 3.94 | 3.67–4.21 |
| Panic disorder | 29 | 0.15 | 0.09–0.19 |
| Agoraphobia without panic | 15 | 0.08 | 0.04–0.11 |
| Separation anxiety disorder | 95 | 0.48 | 0.39–0.58 |
| Social phobia | 138 | 0.70 | 0.58–0.82 |
| Specific phobia | 23 | 0.12 | 0.07–0.16 |
| Obsessive compulsive disorder | 215 | 1.09 | 0.96–1.24 |
| Posttraumatic stress disorder | 36 | 0.18 | 0.12–0.24 |
| Generalized anxiety | 226 | 1.15 | 0.98–1.30 |
| Substance use disorders | 199 | 1.01 | 0.87–1.14 |
| Alcohol dependence | 89 | 0.45 | 0.36–0.55 |
| Alcohol abuse | 12 | 0.06 | 0.03–0.10 |
| Substance dependence | 79 | 0.40 | 0.32–0.48 |
| Substance abuse | 19 | 0.10 | 0.06–0.14 |
| Tic disorder | 401 | 2.03 | 1.84–2.23 |
| Tourette disorder | 52 | 0.26 | 0.19–0.34 |
| Chronic motor tic disorder | 75 | 0.38 | 0.29–0.47 |
| Chronic vocal tic disorder | 74 | 0.38 | 0.29–0.47 |
| Transient tic disorder | 200 | 1.01 | 0.88–1.54 |
| Disruptive disorders | 1659 | 8.42 | 8.03–8.80 |
| ADHD disorder | 1059 | 5.37 | 5.06–5.69 |
| ADHD Combined | 282 | 1.43 | 1.24–1.60 |
| ADHD Inattentive | 630 | 3.20 | 2.95–3.44 |
| ADHD Hyperactive-impulsive | 147 | 0.75 | 0.63–0.87 |
| Conduct disorder | 299 | 1.52 | 1.35–1.69 |
| Oppositional defiant disorder | 594 | 3.01 | 2.78–3.25 |
| Other mental disorders | 240 | 1.22 | 1.06–1.37 |
| Psychotic disorders | 11 | 0.06 | 0.02–0.09 |
| Anorexia nervosa | 23 | 0.12 | 0.07–0.16 |
| Bulimia nervosa | 158 | 0.80 | 0.68–0.93 |
| Adjustment disorder | 42 | 0.21 | 0.15–0.28 |
| Pervasive developmental disorder | 6 | 0.03 | 0.00–0.05 |
| Comorbidity | |||
| Exactly 1 disorder | 1908 | 9.68 | 9.27–10.09 |
| Exactly 2 disorders | 1035 | 5.25 | 4.94–5.56 |
| 3 or more disorders | 60 | 0.30 | 0.23–0.38 |
3.4. Gender, Age and Urban-Rural Distribution of Disorders
| Genger | Male (n = 9938) | Female (n = 9773) | Odds Ratio (95% CI) | p Value |
|---|---|---|---|---|
| Affective disorders | 2.55 (2.24–2.86) | 3.43 (3.07–3.79) | 0.74 (0.63–0.87) | 0.001 ** |
| Anxiety disorders | 3.98 (3.60–4.37) | 3.90 (3.51–4.28) | 1.02 (0.89–1.17) | 0.756 |
| Disruptive disorders | 11.55 (10.92–12.18) | 5.23 (4.79–5.67) | 2.21 (2.00–2.44) | 0.001 ** |
| Substance disorders | 1.77 (1.51–2.03) | 0.24 (0.14–0.33) | 7.53 (4.88–11.61) | 0.001 ** |
| Tic disorders | 2.40 (2.10–2.71) | 1.66 (1.40–1.91) | 1.45 (1.19–1.77) | 0.001 ** |
| Other disorders | 0.26 (0.16–0.36) | 2.19 (1.90–2.48) | 0.12 (0.08–0.18) | 0.001 ** |
| Any disorders | 17.34 (16.59–18.08) | 13.10 (12.43–13.77) | 1.32 (1.24–1.42) | 0.001 ** |
| Age | Anxiety Disorders | Affective Disorders | Substance Disorders | Tic Disorders | Disruptive Disorders | Other Disorders | Any Disorders |
|---|---|---|---|---|---|---|---|
| 6years | 1.79 (1.01–2.57) | 1.07 (0.47–1.68) | 0 (0–0) | 2.06 (1.23–2.90) | 9.94 (8.18–11.69) | 0.27 (0.04–0.57) | 13.52 (11.51–15.53) |
| 7years | 1.37 (0.76–1.99) | 1.95 (1.22–2.68) | 0 (0–0) | 3.10 (2.19–4.02) | 9.82 (8.25–11.39) | 0.36 (0.04–0.68) | 14.44 (12.59–16.29) |
| 8years | 4.47 (3.32–5.61) | 1.27 (0.66–1.90) | 0 (0–0) | 3.03 (2.08–3.98) | 12.60 (10.77–14.45) | 0.32 (0.06–0.63) | 16.36 (14.31–18.41) |
| 9years | 5.00 (3.88–6.11) | 1.51 (0.88–2.13) | 0.14 (0.05–0.33) | 3.56 (2.61–4.51) | 11.29 (9.67–12.92) | 0.41 (0.08–0.74) | 17.11 (15.18–19.04) |
| 10years | 6.21 (5.07–7.34) | 1.55 (0.97–2.13) | 0.63 (0.26–1.00) | 3.74 (2.84–4.63) | 10.86 (9.40–12.33) | 0.17 (0.02–0.37) | 16.55 (14.80–18.30) |
| 11years | 5.41 (4.41–6.41) | 1.12 (0.66–1.59) | 0.51 (0.19–0.83) | 3.01 (2.25–3.71) | 9.95 (8.63–11.28) | 0.31 (0.06–0.55) | 15.01 (13.42–16.60) |
| 12years | 3.52 (2.68–4.37) | 1.90 (1.27–2.52) | 0.65 (0.28–1.02) | 3.25 (2.44–4.06) | 10.51 (9.11–11.92) | 0.81 (0.40–1.22) | 15.99 (14.32–17.67) |
| 13years | 3.74 (2.94–4.53) | 2.83 (2.13–3.52) | 0.59 (0.27–0.91) | 1.87 (1.30–2.49) | 9.17 (7.96–10.37) | 2.23 (1.62–2.85) | 15.60 (14.08–17.11) |
| 14years | 3.42 (2.69–4.15) | 2.95 (2.27–3.64) | 1.05 (0.64–1.47) | 0.42 (0.16–0.68) | 6.84 (5.82–7.85) | 2.87 (2.20–3.54) | 14.77 (13.33–16.20) |
| 15years | 3.56 (2.81–4.31) | 5.43 (4.51–6.34) | 1.91 (1.36–2.46) | 0.17 (0.03–0.34) | 3.60 (2.85–4.36) | 1.65 (1.14–2.17) | 12.68 (11.34–14.02) |
| 16years | 4.08 (3.23–4.95) | 8.23 (7.03–9.42) | 4.00 (3.14–4.84) | 0.30 (0.05–0.53) | 3.10 (2.35–3.86) | 2.07 (1.45–2.69) | 16.21 (14.60–17.81) |
| sum | 3.94 (3.67–4.21) | 2.98 (2.75–3.22) | 1.01 (0.87–1.15) | 2.03 (1.84–2.23) | 8.42 (8.03–8.80) | 1.21 (1.06–1.37) | 15.24 (14.74–15.74) |
| χ2 | 82.55 | 326.55 | 262.55 | 182.81 | 235.66 | 153.54 | 25.69 |
| p | 0.001 ** | 0.001 ** | 0.001 ** | 0.001 ** | 0.001 ** | 0.001 ** | 0.004 ** |
| Community | Rural (n = 11,348) | Urban (n = 8363) | Odds Ratio (95% CI) | p Value |
|---|---|---|---|---|
| Affective disorders | 3.89 (3.53–4.24) | 1.76 (1.48–2.04) | 2.21 (1.84–2.66) | 0.001 ** |
| Anxiety disorders | 3.91 (3.56–4.27) | 3.98 (3.56–4.40) | 0.98 (0.86–1.13) | 0.805 |
| Disruptive disorders | 7.62 (7.13–8.11) | 9.49 (8.87–10.12) | 0.80 (0.73–0.88) | 0.001 ** |
| Substance disorders | 1.43 (1.22–1.66) | 0.43 (0.29–0.57) | 3.34 (2.33–4.78) | 0.001 ** |
| Tic disorders | 1.73 (1.49–1.97) | 2.45 (2.12–2.78) | 0.71 (0.58–0.86) | 0.001 ** |
| Other mental disorders | 1.66 (1.42–1.89) | 0.62 (0.45–0.79) | 2.66 (1.96–3.62) | 0.001 ** |
| Any disorders | 15.84 (15.16–16.51) | 14.42 (13.67–15.17) | 1.10 (1.03–1.18) | 0.006 ** |
3.5. Prevalence of Mental Disorders in Left-Behind Children
| Caregiver | Left-Behind (n = 7331) | Parents (n = 12,380) | Odds Ratio (95% CI) | p Value |
|---|---|---|---|---|
| Affective disorders | 4.50 (4.03–4.98) | 2.08 (1.83–2.34) | 2.22 (1.88–2.61) | 0.001 ** |
| Anxiety disorders | 6.55 (5.98–7.11) | 2.40 (2.13–2.67) | 2.85 (2.46–3.30) | 0.001 ** |
| Disruptive disorders | 15.32 (14.49–16.14) | 4.33 (3.97–4.69) | 3.99 (3.59–4.45) | 0.001 ** |
| Substance disorders | 1.64 (1.35–1.92) | 0.64 (0.50–0.78) | 2.59 (1.95–3.45) | 0.001 ** |
| Tic disorders | 4.17 (3.72–4.63) | 0.77 (0.61–0.92) | 5.63 (4.47–7.10) | 0.001 ** |
| Other disorders | 1.69 (1.40–1.99) | 0.94 (0.77–1.11) | 1.82 (1.41–2.35) | 0.001 ** |
| Any disorders | 26.42 (25.42–27.43) | 8.61 (8.11–9.10) | 3.81 (3.51–4.14) | 0.003 ** |
3.6. Distribution of Mental Disorders According to City
| Cities | Chengdu (n = 4727) | Neijiang (n = 5033) | Dazhou (n = 4838) | Bazhong (n = 5113) | p Value |
|---|---|---|---|---|---|
| Affective disorders | 2.98 (2.50–3.47) | 2.44 (2.02–2.87) | 2.65 (2.19–3.10) | 3.83 (3.31–4.36) | 0.001 ** |
| Anxiety disorders | 3.45 (2.93–3.97) | 4.19 (3.64–4.75) | 3.95 (3.40–4.50) | 4.15 (3.60–4.69) | 0.218 |
| Disruptive disorders | 5.80 (5.13–6.46) | 8.54 (7.77–9.32) | 9.32 (8.50–10.14) | 9.86 (9.04–1067) | 0.001 ** |
| Substance disorders | 1.10 (0.80–1.40) | 0.70 (0.47–0.93) | 0.50 (0.30–0.69) | 1.72 (1.36–2.10) | 0.001 ** |
| Tic disorders | 1.95 (1.55–2.34) | 1.47 (1.14–1.80) | 2.34 (1.91–2.76) | 2.39 (1.97–2.80) | 0.004 ** |
| Other disorders | 1.14 (0.84–1.45) | 1.21 (0.91–1.51) | 1.16 (0.86–1.46) | 1.35 (1.03–1.67) | 0.775 |
| Any disorders | 12.61 (11.66–13.56) | 14.54 (13.57–15.52) | 15.50 (14.48–16.52) | 18.09 (17.04–19.15) | 0.001 ** |
3.7. Comorbidity
4. Discussion
4.1. Point Prevalence
4.2. Sex and Age
4.3. Regional Differences and Issues for Left-Behind Children
4.4. Comorbidity
4.5. Limitations
5. Conclusions
Acknowledgements
Author Contributions
Conflicts of Interest
References
- Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; American Psychiatric Association: Washington, DC, USA, 1994.
- Costello, E.J.; Egger, H.; Angold, A. 10-year research update review: The epidemiology of child and adolescent psychiatric disorders: I. methods and public health burden. J. Amer. Acad. Child Adolesc. Psy. 2005, 44, 972–986. [Google Scholar] [CrossRef]
- Hofstra, M.B.; vander Ende, J.; Verhulst, F.C. Child and adolescent problems predict DSM-IV disorders in adulthood: A 14-year follow-up of a Dutch epidemiological sample. Amer. Acad. Child Adolesc. Psy. 2002, 2, 182–189. [Google Scholar] [CrossRef]
- Viñas, P.F.; Jané, B.M.C.; Canals, S.J.; Esparó, H.G.; Ballespí, S.S.; Doménech-Llaberia, E. Assessment of psychopathology in Preschool age children through the early childhood inventory-4 (ECI-4): Agreement among parents and teachers. Psicothema 2008, 20, 481–486. [Google Scholar] [PubMed]
- Roberts, R.E.; Attkisson, C.C.; Rosenblatt, A. Prevalence of psychopathology among children and adolescents. Amer. J. Psychiat. 1998, 155, 715–725. [Google Scholar] [CrossRef] [PubMed]
- Angold, A.; Costello, E.J.; Erkanli, A. Comorbidity. J. Child. Psychol. Psychiat. 1999, 40, 57–87. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Amminger, G.P.; Aguilar-Gaxiola, S.; Alonso, J.; Lee, S.; Ustün, T.B. Age of onset of mental disorders: A review of recent literature. Curr. Opin. Psychiat. 2007, 20, 359–364. [Google Scholar] [CrossRef]
- Kessler, R.C.; Angermeyer, M.; Anthony, J.C.; de Graaf, R.; Demyttenaere, K.; Gasquet, I.; de Girolamo, G.; Gluzman, S.; Gureje, O.; Haro, J.M.; et al. Lifetime prevalence and age-of-onset distributions of mental disorders in the world health organization’s world mental health survey initiative. World Psychiat. 2007, 6, 168–176. [Google Scholar]
- Frigerio, A.; Rucci, P.; Goodman, R.; Ammaniti, M.; Carlet, O.; Cavolina, P.; De Girolamo, G.; Lenti, C.; Lucarelli, L.; Molteni, M.; et al. Prevalence and correlates of mental disorders among adolescents in Italy: The PrISMA study. Eur. Child Adolesc. Psychiatr. 2009, 18, 217–226. [Google Scholar] [CrossRef]
- Newacheck, P.W.; Kim, S.E.; Blumberg, S.J.; Rising, J.P. Who is at risk for special health care needs: Findings from the national survey of children’s health. Pediatrics 2008, 122, 347–359. [Google Scholar] [CrossRef] [PubMed]
- McDonnell, M.A.; Glod, C. Prevalence of psychopathology in preschool-age children. J. Child Adolesc. Psychiatr. Nurs. 2003, 16, 141–152. [Google Scholar] [CrossRef] [PubMed]
- Costello, E.J.; Mustillo, S.; Erkanli, A. Prevalence and development of psychiatric disorders in childhood and adolescence. Arch. Gen. Psychiat. 2003, 60, 837–844. [Google Scholar] [CrossRef]
- Petersen, D.J.; Bilenberg, N.; Hoerder, K.; Gillberg, C. The population prevalence of child psychiatric disorders in Danish 8- to 9-year-old children. Eur. Child Adolesc. Psychiatr. 2006, 15, 71–78. [Google Scholar] [CrossRef]
- Hart, C.; de Vet, R.; Moran, P.; Hatch, S.L.; Dean, K. A UK population-based study of the relationship between mental disorder and victimisation. Soc. Psychiatry Psychiatr. Epidemiol. 2012, 47, 1581–1590. [Google Scholar] [CrossRef] [PubMed]
- Kokaua, J.; Schaaf, D.; Wells, J.E.; Foliaki, S.A. Twelve-month prevalence, severity, and treatment contact of mental disorders in New Zealand born and migrant Pacific participants in Te Rau Hinengaro: The New Zealand mental health survey. Pac. Health Dialog. 2009, 15, 9–17. [Google Scholar] [PubMed]
- Heiervang, E.; Stormark, K.M.; Lundervold, A.J. Psychiatric disorders in Norwegian 8- to 10-year-olds: An epidemiological survey of prevalence, risk factors, and service use. J. Amer. Acad. Child Adolesc. Psy. 2007, 46, 438–447. [Google Scholar] [CrossRef]
- Canino, G.; Shrout, P.E.; Rubio-Stipec, M.; Bird, H.R. The DSM-IV rates of child and adolescent disorders in Puerto Rico: Prevalence, correlates, service use, and the effects of impairment. Arch. Gen. Psychiat. 2004, 61, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Faravelli, C.; Lo Sauro, C.; Castellini, G.; Ricca, V.; Pallanti, S. Prevalence and correlates of mental disorders in a school-survey sample. Clin. Pract. Epidemiol. Ment. Health 2009, 24, 1–8. [Google Scholar]
- Melissa, A.; Cortina, D.P.; Anisha, S.; Ramchandani, P.G. Prevalence of child mental health problems in Sub-Saharan Africa. Arch. Pediatr. Adolesc. Med. 2012, 166, 276–281. [Google Scholar] [CrossRef] [PubMed]
- Vicente, B.; Saldivia, S.; de la Barra, F.; Melipillán, R.; Valdivia, M.; Kohn, R. Prevalence of psychiatric disorders among Chilean children and adolescents. Rev. Med. Chile 2012, 140, 447–457. [Google Scholar] [CrossRef] [PubMed]
- Murray, J.; Anselmi, L.; Gallo, E.A.; Fleitlich-Bilyk, B.; Isabel, A.B. Epidemiology of childhood conduct problems in Brazil: Systematic review and meta-analysis. Soc. Psychiat. Psychiat. Epidem. 2013, 48, 1527–1538. [Google Scholar] [CrossRef]
- Srinath, S.; Girimaji, S.C.; Gururaj, G.; Seshadri, S.; Subbakrishna, D.K.; Bhola, P.; Kumar, N. Epidemiological study of child & adolescent psychiatric disorders in urban & rural areas of Bangalore, India. Indian J. Med. Res. 2005, 122, 67–79. [Google Scholar] [PubMed]
- Sanjay, J.; Samir, A.A.; Hilal, A.K.; Magdi, M.; Asya, A.R. Prevalence and age-of-onset distributions of DSM IV mental disorders and their severity among school going Omani adolescents and youths: WMH-CIDI findings. Child Adolesc. Psychiatr. Mental Health 2009, 3, 1–11. [Google Scholar] [CrossRef]
- Hai-ying, H.E.; Wang, L.; Wang, M.; Mai, H.F.; Chen, J.; Li, Q.M. Study on incident adolescent metal problems in Beihai. Chin. J. Child Health Care. 2006, 14, 581–582. [Google Scholar]
- Lu, L.; Shi, Q.J.; He, H.; Xu, S.J.; Chen, J.A. Occurrence of behavioral problems among 4 to 16-year-old children and teenagers in Wuhan city. Chin. J. Clin. Rehabil. 2005, 9, 114–116. [Google Scholar]
- Mo, W.; Zhou, J.; Chen, X.; Li, Y.; Lin, X.; Zhu, X. Investigation on behavioral problem of children aged 4–16 years old in Foshan district. Chin. J. Child Health Care. 2014, 21, 421–423. [Google Scholar]
- Guan, B.Q.; Luo, X.R.; Deng, Y.L.; Wei, Z.; Ye, H.S.; Yuan, X.H.; Ning, Z.J.; Yang, W.; Ding, J. Prevalence of psychiatric disorders in primary and middle school students in Hunan province. Zhongguo Dang Dai Er Ke Za Zhi 2010, 12, 123–127. (In Chinese) [Google Scholar] [PubMed]
- Zhang, W.F. Prevalence of psychiatric disorders among 6–17 year old school children in Liaoning province. Master Thesis, Dalian Medical University, Dalian, China, 2010. [Google Scholar]
- Zhou, J.; Cai, W.; Chen, C.; Wang, H.; Zhang, S.M.; Luo, Y.P.; Qiu, C.J.; Wang, X.P. Prevalence of mental disorders in the male juvenile detention centers of Hunan and Sichuan. Zhong Nan Da Xue Xue Bao Yi Xue Ban 2012, 37, 217–221. (In Chinese) [Google Scholar] [PubMed]
- Sheehan, D.; Lecrubier, Y.; Sheehan, H.; Amorim, P.; Janavs, J.; Weiller, E.; Hergueta, T.; Baker, R.; Dunbar, G.C. The mini international neuropsychiatric interview (MINI): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J. Clin. Psychiat. 1998, 59, 22–33. [Google Scholar]
- Sheehan, D.V.; Sheehan, K.H.; Shytle, R.D.; Janavs, J.; Bannon, Y.; Rogers, J.E.; Milo, K.M.; Stock, S.L.; Wilkinson, B. Reliability and validity of the Mini International Neuropsychiatric Interview for Children and Adolescents (MINI-KID). J. Clin. Psychiat. 2010, 71, 313–326. [Google Scholar] [CrossRef]
- Liu, Y.X.; Liu, J.; Wang, Y.F. Reliability and validity of Chinese version of the mini International neuropsychiatric interview for children and adolescents (parent version). Chin. Mental Hlth. J. 2010, 24, 921–925. [Google Scholar]
- Roberts, R.E.; Roberts, C.R.; Xing, Y. Rates of DSM-IV psychiatric disorders among adolescents in a large metropolitan area. J. Psychiat. Res. 2007, 41, 959–967. [Google Scholar] [CrossRef] [PubMed]
- Alyahria, G.R. The prevalence of DSM-IV psychiatric disorders among 7–10 year old Yemeni school children. Soc. Psychiat. Psychiat. Epidem. 2008, 43, 224–230. [Google Scholar] [CrossRef]
- Polanczyk, G.; de Lima, M.; Horta, B.; Biederman, J.; Rohde, L. The worldwide prevalence of ADHD: A systematic review and met regression analysis. Amer. J. Psychiat. 2007, 164, 942–948. [Google Scholar] [CrossRef] [PubMed]
- Lu, L.; Shi, Q.J.; Zhong, Y.F.; Wang, Z.M.; Chen, Z.Y. Attention deficit hyperactivity disorder and the related factors in children in Wuhan city: An anlysis of 2199 questionnaires coming from 12 grades. Chin. J. Clin. Rehabil. 2005, 9, 116–118. [Google Scholar]
- Zhang, W.; Liu, X.; Qun, G.U. An epidemiological investigation of ADHD in six cities. Chin. J. of Clin. Psychol. 2007, 15, 23–25. [Google Scholar]
- Merikangas, K.R. Vulnerability factors for anxiety disorders in children and adolescents. Child Adolesc. Psychiatr. Clin. 2005, 14, 649–679. [Google Scholar] [CrossRef]
- Cartwright-Hatton, S.; McNicol, K.; Doubleday, E. Anxiety in a neglected population: Prevalence of anxiety disorders in preadolescent children. Clin. Psychol. Rev. 2006, 26, 817–833. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Chen, L.; Wang, X.; Liu, Y.; Chui, C.H.; He, H.; Qu, Z.; Tian, D. The relationship between Internet addiction and depression among migrant children and left-behind children in China. Cyberpsychol. Behav. Soc. Netw. 2012, 15, 67–68. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.L.; Duan, C.R. Literature review on studies on left behind children. Pop. Res. 2006, 3, 16–17. [Google Scholar]
- Zhao, M.M.; Li, H.; Li, J.; Li, L.G.; Wang, C.L. Studying on the influence of migrant on mental health of their left-behind children in rural China. Chin. Health Serv. Manage. 2012, 1, 60–63. [Google Scholar]
- Liu, L.U.; Qu, C.; Qiu, Y.F. A survey and research on the relationship between psychological health and the way of those left-home children. China J. Health Psychol. 2007, 15, 1017–1119. [Google Scholar]
- Zhang, F.; Liu, Q.; Zhao, Y.; Sun, M.H.; Wang, H. Left-behind children’s mental health problems: A systematic review. Chin. J. Evid. Med. 2011, 11, 849–857. [Google Scholar]
- Weller, E.B.; Weller, R.A. Depression in adolescents growing pains or true morbidity? J. Affect. Disorders 2000, 61, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G.Y.; Yang, Y.C.; Sun, X.L.; Huang, Y.; Liu, S.J. Epidemiological investigation on depression among 6–16 years old children and adolescents in Chengdu. Chin. Mental Hlth. J. 2012, 24, 211–214. [Google Scholar]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qu, Y.; Jiang, H.; Zhang, N.; Wang, D.; Guo, L. Prevalence of Mental Disorders in 6–16-Year-Old Students in Sichuan Province, China. Int. J. Environ. Res. Public Health 2015, 12, 5090-5107. https://doi.org/10.3390/ijerph120505090
Qu Y, Jiang H, Zhang N, Wang D, Guo L. Prevalence of Mental Disorders in 6–16-Year-Old Students in Sichuan Province, China. International Journal of Environmental Research and Public Health. 2015; 12(5):5090-5107. https://doi.org/10.3390/ijerph120505090
Chicago/Turabian StyleQu, Yuan, Hongyun Jiang, Ni Zhang, Dahai Wang, and Lanting Guo. 2015. "Prevalence of Mental Disorders in 6–16-Year-Old Students in Sichuan Province, China" International Journal of Environmental Research and Public Health 12, no. 5: 5090-5107. https://doi.org/10.3390/ijerph120505090