Where to Go from Here? An Exploratory Meta-Analysis of the Most Promising Approaches to Depression Prevention Programs for Children and Adolescents

Abstract
:1. Introduction
2. Materials and Methods

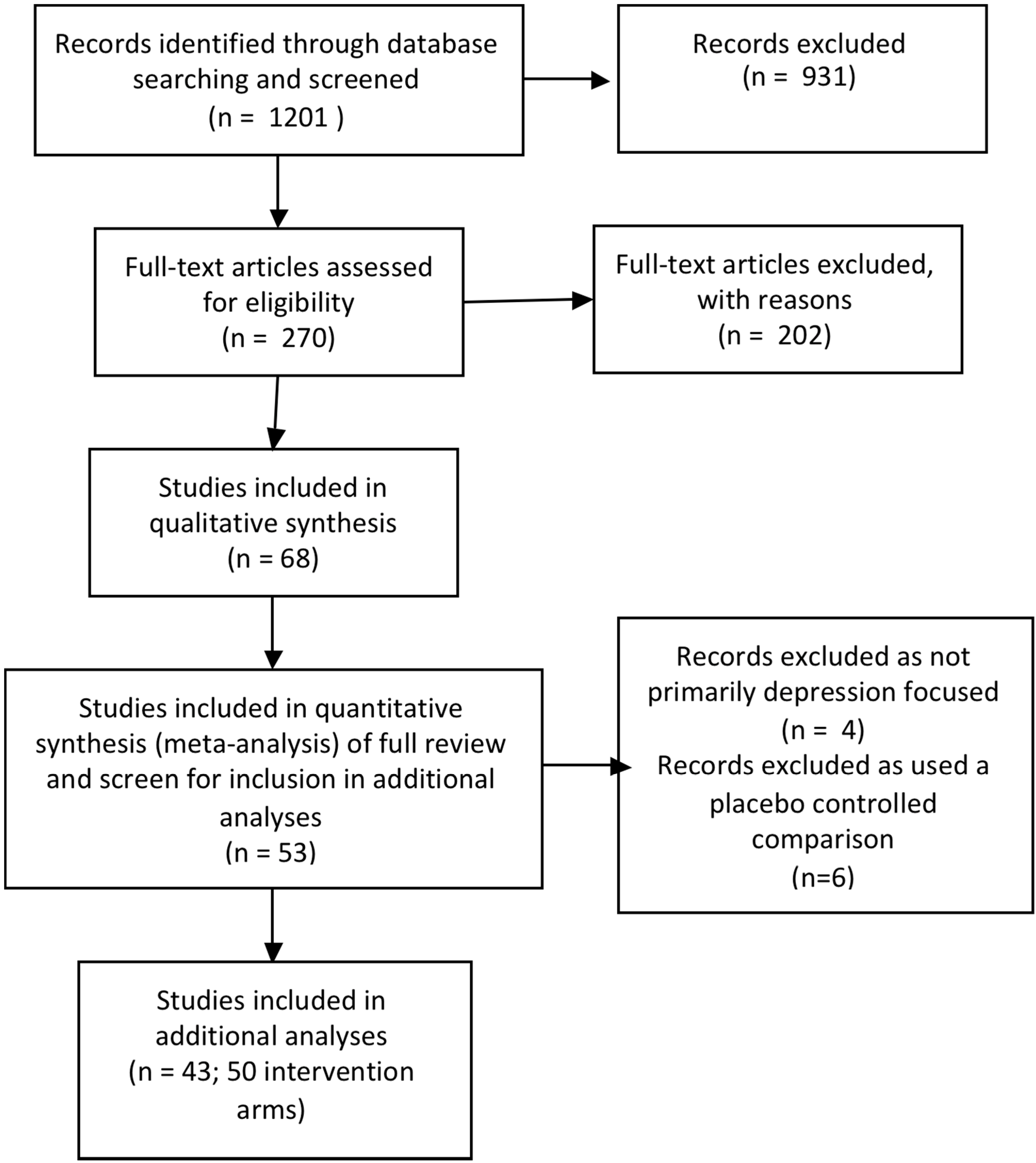
2.1. Search Strategy
2.2. Study Selection
2.3. Assessment of Risk of Bias
2.4. Statistical Analyses
2.5. Subgroup Analysis

{kind=link}
| Study Name | Description | Therapeutic Approach | Specific CBT Program Name |
|---|---|---|---|
| Arnarson 2009 [20] | Based on a number of previous programs including the Coping with Depression and its derivative Coping with Stress program. The focus was on the development of adaptive coping skills to enhance self-esteem and well-being. Stated it incorporated principles of interpersonal therapy, problem solving, behavioural, and cognitive models (pg 581). | CBT & IPT | Unspecified |
| Balle 2009 [21] | Based on the FRIENDS program; includes education about anxiety, cognitive restructuring, emotional regulation techniques (activation control strategies, controlled breathing, relaxation and cognitive distraction), and gradual exposure to feared situations. | CBT | FRIENDS |
| Berry 2009 [22] | The Confident Kids program focuses on anxiety and included psychoeducation, cognitive restructuring and graded exposure. Also included education about bullying, coping strategies for bullying situations and sessions on social skill and self esteem enhancement. | CBT | Confident Kids |
| Barnet 2007 [23] | Trained home visitors provided parenting curriculum (child development, parenting skills, appropriate health care use), encouraged contraceptive use, connected adolescent with primary care, school continuation, provided mentoring and case management, sought to identify depression, partner abuse and school drop out and follow-up of these issues. | Other | |
| Bond 2004 [24] | The Gatehouse project is a school health promotion program with both individual and ‘whole school’ focused components. The individual component focused on teaching students to identify difficult/conflicting emotional responses to common social situations and develop strategies for responding. The whole school component included a school based adolescent health team as well as interventions to address identified risk and protective factors in the schools social and learning environment. | Other | |
| Cabiya 2008 [25] | Primarily social problem solving that included teaching adolescents how to understand social cues, how to make accurate interpretations of these cues; how to generate a variety of solutions to a problem they perceive in the social setting; how to decide which solution to enact and how to enact the chosen solution. | CBT | Unspecified |
| Calear 2009 [26] | MoodGYM is an online CBT program that includes cognitive restructuring, interpersonal skills, relaxation and problem solving. It is fully automated and self-directed. | CBT - online | MoodGYM |
| Cardemil 2002 a [27]-African American | The Penn Resiliency Program (PRP) includes cognitive restructuring, relaxation and emotion regulation, assertiveness, coping skills, negotiation, social skills, creative and social problem solving, and decision-making. | CBT | PRP |
| Cardemil 2002 b [27]-Latina | Penn Resiliency Program (PRP) | CBT | PRP |
| Chaplin a 2006 [28]-girls only | Penn Resiliency Program (PRP) | CBT | PRP |
| Chaplin b2006 [28]-co-ed | Penn Resiliency Program (PRP) | CBT | PRP |
| Clarke 1993 [29] | Behavioural skill training intervention that focused on increasing daily rates of pleasant activities. | CBT | Unspecified |
| Clarke 1995 [30] | The Adolescent Coping with Stress program teaches cognitive restructuring and problem solving skills. The course was based on the “Adolescent Coping with Depression Course” (Clarke et al. 1990). Specifically it teaches adolescents to (a) monitor daily moods; (b) identify activating events; (c) discover, challenge, realistically evaluate, and revise negative beliefs; (d) recognize the connections among activating events, beliefs, and consequences (e.g., affect and behaviours); and (e) problem solve and cope with stressful events. | CBT | Coping with Stress |
| Clarke 2001 [31] | Adolescent Coping with Stress program | CBT | Coping with Stress |
| Garber 2009 [32] | Adolescent Coping with Stress program with behavioural activation, relaxation and assertiveness training as part of the continuation phase | CBT | Coping with Stress |
| Gillham 1995 [33] | Included cognitive restructuring, and social problem solving. The social problem solving component focused on conduct problems and interpersonal problems often associated with depression and included teaching children to thinking about their goals before acting, generating a list of possible solutions for problems and making decisions about which solution to enact based on pro’s and con’s of each. They were also taught skills to help cope with parental conflict, and behavioural techniques to enhance assertiveness, negotiation and relaxation. | CBT | PRP |
| Gillham & Reivich 2006 [34] | Penn Resiliency Program (PRP) with parent component included based on the theory that children learn interpretive and coping styles from their parents, and that helping to prevent or reduce depression in parents interrupts transmission from parents to children. | CBT | PRP |
| Gillham & Hamilton 2006 [35] | Penn Resiliency Program (PRP) | CBT | PRP |
| Gillham 2007 [36] | Penn Resiliency Program (PRP) | CBT | PRP |
| Hains 1990 [37] | Based on cognitive-behavioural stress-inoculation training model developed by Meichenbaum (1985). Included cognitive restructuring around common self defeating cognitions lead to stress and anger. | CBT | Stress Inoculation |
| Hains 1992 [38] | One group received stress inoculation as in Hains 1990; the second group received anxiety management training following the Suinn 1986 manual that includes learning how to recognise cues that signal the onset of anxiety and the use of relaxation skills to relieve anxiety. | CBT | Stress Inoculation |
| Horowitz a 2007 [39] | Derived from the Adolescent Coping with Stress program | CBT | Coping with Stress |
| Horowitz b 2007 [39] | Derived from the IPT–AST (Young & Mufson, 2003) course. IPT-AST includes two individual sessions and 8 group sessions delivering psychoeducation about the relationship between interpersonal difficulties and depression and skill building including communication and interpersonal strategies related to three interpersonal problem areas: interpersonal role disputes, role transitions, and interpersonal deficits. | IPT | IPT-AST |
| Hyun 2005 [40] | The program integrated cognitive and behavioral components. The cognitive components included identifying reasons for running away from home, identifying high-risk situations including negative emotional states, cognitive distortions and dysfunctional coping strategies, and behavioral components included developing coping strategies such as pleasant activities and relaxation and planning for future life. | CBT | Unspecified |
| Kraag 2009 [41] | The Learn Young, Learn Fair program addressed stress, stress awareness and coping skills. | CBT | Learn Young, Learn Fair |
| Lock 2003 [42] | The FRIENDS program (Barrett 2000) was originally based on the Coping Cat (Kendall, 1990) and Coping Koala (Barrett, 1998) programs. It included education about anxiety, cognitive restructuring, emotional regulation techniques (activation control strategies, controlled breathing, relaxation and cognitive distraction), and gradual exposure to feared situations (including interoceptive exposure). | CBT | FRIENDS |
| Lowry-Webster 2001 [43] | FRIENDS program. | CBT | FRIENDS |
| Pössel 2004 [44] | The Ease of Handling Social Aspects in Everyday Life-Training (LISA-T) program is based on cognitive behavioural therapy and includes cognitive restructuring as well as a social focus with models of assertiveness and social competence training which targets students ability to develop and maintain social contacts. | CBT | LISA-T |
| Pössel 2008 [45] | LISA-T | CBT | LISA-T |
| Puskar 2003 [46] | The Teaching Kids to Cope program is aimed to teach skills that help young people cope with problems and stress. It includes cognitive restructuring but has more emphasis on behavioural skill building including social skills training, assertiveness training, conflict resolution and relaxation. It uniquely includes bibliotherapy, role-playing, and group exercises such as ‘trust-fall’, buddy assignments, and role playing situations from school as well as art activities. | CBT | Teaching Kids to Cope |
| Quayle 2001 [47] | Adapted PRP and called the Optimism and Life Skills Program | CBT | PRP |
| Rivet-Duval 2010 [48] | The Resourceful Adolescent Program (RAP) integrates elements of cognitive behavioural therapy (CBT) and interpersonal therapy. It includes behavioural activation with a focus on activities that increase self-esteem, cognitive restructuring, relaxation techniques, problem solving and conflict resolution. | CBT & IPT | RAP |
| Roberts 2003 [49] | Penn Resiliency Program (PRP) | CBT | PRP |
| Roberts 2010 [50] | The Aussie Optimism Program (AOP) program is based on PRP but targets anxiety as well as depression. | CBT | PRP |
| Rooney 2006 [51] | The Positive Thinking Program (PTP) program is based in part on the Aussie Optimism Program (AOP). It includes cognitive restructuring, and training in relaxation and distraction skills. | CBT | Positive Thinking Program |
| Sawyer 2010 [52] | The beyondblue schools research initiative utilised individual and ‘whole school’ focused components. The individual component aimed to improve problem solving and social skills, resilient thinking style and coping strategies. The whole school component included enhancements to the school climate to improve the quality of social interactions amongst all members of the school; improvements to care pathways to improve adolescents access to support and professional services; and community forums to provide adolescents, their families and school personnel to information about recognising problems and how to seek help. | CBT | beyondblue Schools Research Initiative |
| Seligman 1999 [53] | Intervention is based on CBT and similar PRP and includes cognitive restructuring, behavioural activation interventions including graded task breakdown, time management, anti-procrastination techniques, creative problem solving, assertiveness training, interpersonal skills including active listening, taking each other’s perspectives, controlling emotions, passive vs. assertive vs. aggressive behaviours, and relaxation training. | CBT | Unspecified |
| Seligman 2007 [54] | Replication of Seligman 1999 intervention with additional of web-based material and e-coaching primarily aimed at maintaining intervention effects over time. | CBT-partly online | Unspecified |
| Shatte 1997 [55] | Penn Resiliency Program (PRP) | CBT | PRP |
| Sheffield 2006 [56] | The Universal intervention included cognitive restructuring as well as problem solving interventions and was similar to the intervention described in Spence 2003. The indicated prevention program included these elements but also included interpersonal skills such as assertiveness, conflict resolution and negotiation and self-reward. | CBT | Problem Solving for Life |
| Spence 2003 [57] | The Problem Solving for Life (PSFL) program integrates cognitive restructuring and problem-solving skills training. | CBT | Problem Solving for Life |
| Stice a 2007 [58] | Based on the Coping with Stress program and focused on building rapport, increasing pleasant activities and cognitive restructuring. | CBT | Blues Program |
| Stice b 2007 [58] | Supportive-expressive group therapy, which aimed to establish and maintain rapport, provide support, and help the client identify and express emotions. | Other | |
| Stice c 2007 [58] | Bibliotherapy, which is the prescription of books for the treatment of a disorder. | Other | |
| Stice d 2007 [58] | Expressive writing in which participants write about issues of emotional significance to them. | Other | |
| Stice e 2007 [58] | Journalling | Other | |
| Stice a 2008 [59] | Based on the Coping with Stress program and focused on building rapport, increasing pleasant activities and cognitive restructuring | CBT | Blues Program |
| Stice b 2008 [59] | Supportive-expressive group therapy, which aims to establish and maintain rapport, provide support, and help the client identify and express emotions. | Other | |
| Stice c 2008 [59] | Cognitive Behavioural Bibliotherapy | Other | |
| Yu 2002 [60] | Chinese version of the Penn Resiliency Program (PRP) | CBT | PRP |
| Young 2006 [61] | The Interpersonal Therapy-Adolescent Skills Training (IPT–AST) program was created as an extension of interpersonal therapy. IPT–AST teaches communication and social skills necessary to develop and maintain positive relationships. | IPT |
- Interventions were delivered to universal versus targeted populations;
- Interventions were delivered by a mental health clinician (including graduate level school counselors, school psychologists, cognitive and other therapists, clinical and other psychologists, psychiatric nurses, psychiatrist and mental health clinicians) versus students being trained in any of these mental health professions versus non mental health personnel;
- Interventions included eight sessions or more versus less than eight sessions;
- Outcomes were measured by the CDI/BDI versus the CES-D versus the RADS versus other measures.
2.6. Unit of Analysis Issues
2.7. Heterogeneity
3. Results
3.1. Description of Studies
3.2. Assessment of Risk of Bias
3.3. Effects of Intervention
3.3.1. By Type of Intervention
CBT
| Study Name | Size | Format | Targeted or Universal | Therapeutic Approach | Specific CBT Program Name | Number of Sessions | Manualised | Parent Component | Delivered by | Inclusion Criteria for Targeted Populations | Depression Outcome Measure | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Arnarson 2009 [20] | 171 | Group | Targeted | CBT & IPT | Unspecified | 14 | Yes | No | Mental Health clinician | 75th–90th percentile on CDI or >75th percentile on negative composite of the CASQ | CDI | |
| Balle 2009 [21] | 145 | Group | Targeted | CBT | FRIENDS | 6 | Yes | No | Student mental health clinicians | High anxiety sensitivity | CDI | |
| Berry 2009 [22] | 54 | Group | Targeted | CBT | Confident Kids | 8 | Yes | Yes | Student mental health clinicians | Anxiety symptoms | CES-D | |
| Barnet 2007 [23] | 84 | Group | Targeted | Other | 36 | Yes | Yes | Non mental health personnel | Pregnant adolescents | CES-D | ||
| Bond 2004 [24] | 2678 | Group | Universal | Other | 20 | Yes | No | School teachers | NA | CIS-R | ||
| Cabiya 2008 [25] | 278 | Group | Targeted | CBT | Unspecified | 12 | Yes | No | Student mental health clinicians | Disruptive behaviour disorders | CDI | |
| Calear 2009 [26] | 1384 | Individual | Universal | CBT-online | MoodGYM | 5 | Yes | No | Internet-based | NA | CES-D | |
| Cardemil 2002 [27] | Trial 1: 49; Trial 2: 103 | Group | Universal | CBT | PRP | 12 | Yes | No | Student mental health clinicians | NA | CDI | |
| Chaplin 2006 [28] | 234 | Group | Universal | CBT | PRP | 12 | Yes | No | Both mental and non mental health personnel | NA | CDI | |
| Clarke 1993 [29] | 622 | Group | Universal | CBT | 3 | Yes | No | Non mental health personnel | NA | CES-D | ||
| Clarke 1995 [30] | 125 | Group | Targeted | CBT | Coping with Stress | 15 | Yes | No | Mental health clinician | CES-D score of >=24 | CES-D | |
| Clarke 2001 [31] | 94 | Group | Targeted | CBT | Coping with Stress | 15 | Yes | Yes | Mental health clinician | CES-D score of ≥ 24 & parent with previous or current depressive episode | CES-D | |
| Garber 2009 [32] | 316 | Group | Targeted | CBT | Coping with Stress | 14 | Unclear | Yes | Mental health clinician | CES-D score of ≥ 20 & parent with previous or current depressive episode | CES-D | |
| Gillham 1995 [33] | 143 | Group | Targeted | CBT | PRP | 12 | Unclear | Yes. In the child-parent group only. | Student mental health clinicians | Children with summed z scores of ≤ 0.50 on CDI & CPQ | CDI | |
| Gillham & Reivich 2006 [34] | 44 | Group | Targeted | CBT | PRP | 8 | Yes | Yes | Mental health clinician | High levels of depression and anxiety | CDI | |
| Gillham & Hamilton 2006 [35] | 271 | Group | Targeted | CBT | PRP | 12 | Yes | No | Mental health clinician | CDI scores ≥ 7 for girls and ≥ 9 for boys | CDI | |
| Gillham 2007 [36] | 697 | Group | Universal | CBT | PRP | 12 | Yes | No | Mental and non mental health personnel and students | NA | CDI | |
| Hains 1990 [37] | 24 | Group | Universal | CBT | Stress Inoculation | 5 | Unclear | No | Mental health clinician | NA | BDI | |
| Hains 1992 [38] | 25 | Group (plus 1 individual session) | Universal | CBT | Stress Inoculation | 4 | Unclear | No | Mental health clinician | NA | RADS | |
| Horowitz a 2007 [39] | 112 | Group | Universal | CBT | Coping with Stress | 8 | Yes | No | Student mental health clinicians | NA | CES-D | |
| Horowitz b 2007 [39] | 99 | Group | Universal | IPT | IPT-AST | 8 | Yes | No | Student mental health clinicians | NA | CES-D | |
| Hyun 2005 [40] | 32 | Group | Targeted | CBT | Unspecified | 8 | Unclear | No | Mental health clinician | Runaway youth | BDI | |
| Kraag 2009 [41] | 1437 | Group | Universal | CBT | Learn Young, Learn Fair | 13 | Yes | No | Non mental health personnel | NA | SDIC | |
| Lock 2003 [42] | 977 | Group | Universal | CBT | FRIENDS | 10 | Yes | No | Student mental health clinicians | NA | CDI | |
| Lowry-Webster 2001 [43] | 594 | Group | Universal | CBT | FRIENDS | 10 | Yes | Yes | Non mental health personnel | NA | CDI | |
| Pössel 2004 [44] | 342 | Group | Universal | CBT | LISA-T | 10 | Yes | No | Mental health clinician | NA | CES-D | |
| Pössel 2008 [45] | 301 | Group | Universal | CBT | LISA-T | 10 | Yes | No | Non mental health personnel with student mental health professionals | NA | SBB-DES | |
| Puskar 2003 [46] | 89 | Group | Targeted | CBT | Teaching Kids to Cope | 10 | Unclear | No | Mental health clinician | RADS score ≥ 60 | RADS | |
| Quayle 2001 [47] | 47 | Group | Universal | CBT | PRP | 8 | Yes | No | Student mental health clinician | NA | CDI | |
| Rivet-Duval 2010 [48] | 160 | Group | Universal | CBT & IPT | RAP | 11 | Yes | No | Non mental health personnel | NA | RADS | |
| Roberts 2003 [49] | 189 | Group | Targeted | CBT | PRP | 12 | Yes | No | Mental health clinician | Elevated scores on the CDI | CDI | |
| Roberts 2010 [50] | 496 | Group | Universal | CBT | Aussie Optimism Program | 10 | Yes | No | Non mental health personnel | NA | CDI | |
| Rooney 2006 [51] | 136 | Group | Universal | CBT | Positive Thinking Program | 8 | Yes | No | Mental health clinician | NA | CDI | |
| Sawyer 2010 [52] | 5634 | Group | Universal | CBT | beyondblue Schools Research Initiative | 30 | Yes | No | Non mental health personnel | NA | CES-D | |
| Seligman 1999 [53] | 231 | Group | Targeted | CBT | Unspecified | 8 | Yes | No | Mental health clinician | Scored in the pessimistic quarter of the ASQ | BDI | |
| Seligman 2007 [54] | 227 | Group | Targeted | CBT-partly online | Unspecified | 8 | Yes | No | Mental health clinician | BDI score of 9–24 | BDI | |
| Shatte 1997 [55] | 152 | Group | Universal | CBT | PRP | 12 | Yes | No | Non mental health personnel with student mental health professionals | NA | CDI | |
| Sheffield 2006 [56] | 2606 | Group | Universal and targeted | CBT | Problem Solving for Life | 8 | Yes | No | Non mental health personnel for Universal; Mental health clinician for targeted | Score in the top 20% on the combined scores on the CDI & CES-D. | CDI | |
| Spence 2003 [57] | 1234 | Group | Universal | CBT | Problem Solving for Life | 8 | Yes | No | Non mental health personnel | NA | BDI | |
| Stice a 2007 [58] | 50 | Group (CBT) | Targeted | CBT | Blues Program | 4 | Yes | No | Student mental health clinician | CES-D score of ≥ 20 | BDI | |
| Stice b 2007 [58] | 19 | Group (Supportive expressive) | Targeted | Other | 4 | Yes | No | Student mental health clinician | CES-D score of ≥ 20 | BDI | ||
| Stice c 2007 [58] | 28 | Individual (Bibliotherapy) | Targeted | Other | Not specified | Yes | No | Self-led | CES-D score of ≥ 20 | BDI | ||
| Stice d 2007 [58] | 27 | Individual (Expressive writing) | Targeted | Other | 4 | Yes | No | Self-led | CES-D score of ≥ 20 | BDI | ||
| Stice e 2007 [58] | 34 | Individual (Journaling) | Targeted | Other | Not specified | Yes | No | Self-led | CES-D score of ≥ 20 | BDI | ||
| Stice a 2008 [59] | 89 | Group (CBT) | Targeted | CBT | Blues Program | 6 | Yes | No | Student mental health clinician | CES-D score of ≥ 20 | CES-D | |
| Stice b 2008 [59] | 88 | Group (Supportive Expressive) | Targeted | Other | 6 | Yes | No | Student mental health clinician | CES-D score of ≥ 20 | CES-D | ||
| Stice c 2008 [59] | 80 | Individual (Bibliotherapy) | Targeted | Other | Not specified | Yes | No | Self-led | CES-D score of ≥ 20 | CES-D | ||
| Yu 2002 [60] | 270 | Group | Targeted | CBT | PRP | 10 | Yes | No | Non mental health personnel | Elevated scores on the CDI and the Cohesion and Conflict subscales of the Family Environment scale | CDI | |
| Young 2006 [61] | 41 | Group | Targeted | IPT | 10 | Yes | No | Mental health clinician | CES-D score of 16–39 | CES-D | ||
IPT
Other
Test for Differences between Types of Intervention
| Program | Post Intervention | 3–9 Month Follow-up | 12-Month Follow-up | |||
|---|---|---|---|---|---|---|
| Depressive disorder (RD) | Depression symptoms (SMD) | Depressive disorder (RD) | Depression symptoms (SMD) | Depressive disorder (RD) | Depression symptoms (SMD) | |
| CBT | 14 studies; 16 intervention arms; N = 1776 RD −0.11; 95% CI −0.17 to −0.05 I2 = 66% | 39 studies; 39 intervention arms; N = 11630 SMD −0.12; 95% CI −0.24 to −0.01 I2 = 86% | 14 studies; 18 intervention arms; N = 2254 RD −0.11; 95% CI −0.15 to −0.06 I2 = 46% | 27 studies; 33 intervention arms; N = 6351 SMD −0.09; 95% CI −0.25 to 0.07 I2 = 87% | 9 studies; 10 intervention arms; N = 1149 RD−0.08; 95% CI −0.16 to -0.00 I2 = 75% | 16 studies; 21 intervention arms; N = 5047 SMD −0.11; 95% CI −0.17 to −0.04 I2 = 13% |
| IPT | 2 studies; 2 intervention arms; N = 265 RD 0.09; 95% CI −0.35 to 0.17 | 3 studies; 3 intervention arms; N = 327SMD −0.54; 95% CI −0.94 to −0.13 I2 = 67% | 2 studies; 2 intervention arms; N = 252 RD −011; 95% CI −0.19 to −0.04 I2 = 0% | 3 studies; 4 intervention arms; N = 327 SMD −0.26 [−0.62, 0.10] | NA | 1 study; 1 intervention; N = 41 SMD −0.56 [−1.22, 0.10] |
| Other | 4 studies; 5 intervention arms; N = 1843 RD −0.01; 95% CI −0.05 to 0.02 | 5 studies; 9 intervention arms; N = 2178 SMD −0.21; 95% CI −0.39 to −0.03 I2 = 52% | 3 studies; 5 intervention arms; N = 623 RD −0.02; 95% CI −0.11 to 0.07 | 4 studies; 9 intervention arms; N = 766 SMD −0.08; 95% CI −0.23 to 0.07 | 2 studies; 2 intervention arms; N = 1363 RD 0.01; 95% CI −0.03, 0.05 | 2 studies; 2 intervention arms; N = 1375 SMD 0.14; 95% CI 0.03 to 0.24 I2 =0% |
| Subgroup differences | χ2 = 8.86, | χ2 = 2.85, | χ2 = 3.18, | χ2 = 0.83, | χ2 = 4.13, | χ2 = 17.07, |
| p = 0.01 | p = 0.24 | p = 0.20 | p = 0.66 | p = 0.04 | p = 0.0002 | |
3.3.2. By CBT Program Type
Penn Resiliency Program (PRP)
Coping with Stress
| Program | Post Intervention | 3–9 Month Follow-up | 12-Month Follow-up | |||
|---|---|---|---|---|---|---|
| Depressive disorder (RD) | Depression symptoms (SMD) | Depressive disorder (RD) | Depression symptoms (SMD) | Depressive disorder (RD) | Depression symptoms (SMD) | |
| PRP | 6 studies; 8 intervention arms; N = 483 RD −0.18 [−0.31, −0.05] I2 = 74% | 11 studies; 12 intervention arms; N = 1628 SMD 0.11 [−0.21, 0.00] I2 = 0% | 5 studies; 6 intervention arms; N = 363 RD −0.19 [−0.36, −0.01] I2 = 84% | 10 studies; 13 intervention arms; N = 1206 SMD −0.17 [−0.29, −0.05] I2 = 0% | 4 studies; 5 intervention arms; N = 273 RD −0.05 [−0.14, −0.03] I2 = 16% | 7 studies; 10 intervention arms; N = 926 SMD −0.18 [−0.31, -0.05] I2 = 0% |
| Coping with Stress | 2 studies; 2 intervention arms; N = 215 RD −0.16 [−0.27, −0.04] I2 = 49% | 4 studies; 4 intervention arms; N = 598 SMD −0.34 [−0.50, −0.17] I2 = 0% | 2 studies; 2 intervention arms; N = 427 RD −0.12 [−0.19, −0.04] I2 = 0% | 3 studies; 3 intervention arms; N = 494 SMD −0.14 [−0.32, 0.04] | 2 studies; 2 intervention arms; N = 195 RD −0.12 [−0.24, −0.01] I2 = 0% | 2 studies; 2 intervention arms; N = 196 SMD −0.25 [−0.77, 0.27] |
| Friends | 1 study; 1 intervention arm; N = 239 RD −0.06 [−0.17, 0.04] | 3 studies; 3 intervention arms; N = 486 SMD −0.09 [−0.28, 0.09] | NA | 1 study; 1 intervention arm; N = 68 SMD 0.19 [−0.29, 0.67] | 2 studies; 2 intervention arms; N = 452 RD −0.12 [−0.57, 0.33] | 2 studies; 2 intervention arms; N = 418 SMD −0.27 [−0.47, −0.06] I2 = 0% |
| Positive Thinking Program | 1 study; 1 intervention arm; N = 76 RD −0.10 [−0.25, 0.05] | 1 study; 1 intervention arm; N = 76 SMD −0.57 [−1.04, −0.10] | 1 study; 1 intervention arm; N = 75 RD −0.21 [−0.37, −0.05] | 1 study; 1 intervention arm; N = 75 SMD −0.25 [−0.71, 0.21] | NA | NA |
| Blues Program | NA | 2 studies; 2 intervention arms; N = 153 SMD −0.65 [−1.03, −0.26] I2 = 0% | 1 study; 1 intervention arm; N = 100 RD −0.09 [−0.25, 0.07] | 2 studies; 2 intervention arms; N = 153 SMD −0.38 [−0.76, −0.00] I2 = 0% | NA | |
| Aussie Optimism Program | NA | 1 study; 1 intervention arm; N = 427 SMD 0.14 [−0.05, 0.33] | NA | 1 study; 1 intervention arm; N = 395 SMD 0.12 [−0.08, 0.32] | NA | |
| Stress focus | NA | 2 studies; 2 intervention arms; N = 38 SMD −0.47 [−1.17, 0.23] | NA | NA | NA | NA |
| Confident kids | NA | 1 study; 1 intervention arm; N = 44 SMD −0.66 [−1.58, 0.25] | NA | NA | NA | NA |
| Learn Young Learn Fair | NA | 1 study; 1 intervention arm; N = 1102 SMD 0.00 [−0.12, 0.12] | NA | NA | NA | 1 study; 1 intervention arm; N = 1011 SMD −0.02 [−0.15, 0.10] |
| Teaching Kids to Cope | NA | 1 study; 1 intervention arm; N = 80 SMD −0.47 [−0.92, −0.03] | NA | 1 study; 1 intervention arm; N = 76 SMD −0.49 [−0.95, −0.04] | NA | 1 study; 1 intervention arm; N = 70 SMD −0.30 [−0.77, 0.17] |
| Moodgym | NA | 1 study; 1 intervention arm; N = 719 SMD −0.15 [−0.30, 0.00] | NA | 1 study; 1 intervention arm; N = 690 SMD −0.13 [−0.28, 0.03] | NA | NA |
| LISA-T | NA | 2 studies; 2 intervention arms; N = 446 SMD −0.07 [−0.26, 0.11] | NA | 2 studies; 2 intervention arms; N = 435 SMD −0.23 [−0.65, 0.20] | NA | NA |
| Problem solving for Life | NA | 2 studies; 4 intervention arms; N = 2310 SMD −0.14 [−0.25, −0.04] I2 = 29% | 1 study; 3 intervention arms; N = 714 RD −0.06 [−0.12, 0.01] | 1 study; 3 intervention arm; N = 1843 SMD −0.03 [−0.14, 0.08] | 1 study; 1 intervention arm; N = 229 RD 0.01 [−0.06, 0.09] | 2 studies; 4 intervention arms; N = 2207 SMD 0.00 [−0.09, 0.10] |
| RAP | 1 study; 1 intervention arm; N = 116 RD −0.17 [−0.33, −0.01] | 1 study; 1 intervention arm; N = 116 SMD −0.32 [−0.68, 0.05] | 1 study; 1 intervention arm; N = 116 RD −0.10 [−0.28, 0.07] | 1 study; 1 intervention arm; N = 116 SMD −0.03 [−0.39, 0.34] | NA | NA |
| Unspecified | 3 studies; 4 intervention arm; N = 667 RD −0.03 [−0.06, 0.01] | 5 studies; 7 intervention arms; N = 956 SMD −0.26 [−0.50, −0.02] I2 = 63% | 2 studies; 3 intervention arms; N = 409 RD −0.09 [−0.15, −0.03] I2 = 0% | 3 studies; 4 intervention arms; N = 717 SMD −0.24 [−0.54, −0.05] | NA | 1 study; 1 intervention arm; N = 219 SMD −0.25 [−0.52, 0.02] |
| Subgroup differences | χ2 = 10.64, | χ2 = 36.31, | χ2 = 4.96, | χ2 = 16.18, | χ2 = 4.47, | χ2 = 13.05, |
Friends
Positive Thinking Program
Blues Program
Aussie Optimism Program
Stress Inoculation (General)
Confident Kids
Learn Young, Learn Fair
Teaching Kids to Cope
MOOD-GYM
LISA-T
Problem Solving for Life
RAP
Unspecified
Test for Differences Between Types of Named Programs
3.4. Sensitivity Analyses
| Program | Post Intervention | 3–9 Month Follow-up | 12-Month Follow-up | |||
|---|---|---|---|---|---|---|
| Depressive disorder (RD) | Depression symptoms (SMD) | Depressive disorder (RD) | Depression symptoms (SMD) | Depressive disorder (RD) | Depression symptoms (SMD) | |
| Universal | 8 studies; 9 intervention arm; N = 1025 RD −0.14 [−0.23, −0.06] I2 = 68% | 21 studies; 26 intervention arm; N = 6519 SMD −0.05 [−0.23, 0.13] | 8 studies; 10 intervention arm; N = 1228 RD −0.13 [−0.21, −0.06] I2 = 70% | 14 studies; 18 intervention arm; N = 4077 SMD −0.02 [−0.27, 0.23] | 6 studies; 7 intervention arm; N = 910 RD −0.06 [−0.15, 0.03] | 10 studies; 14 intervention arm; N = 3737 SMD −0.08 [−0.14, −0.01] I2 = 68% |
| Targeted | 6 studies; 7 intervention arms; N = 751 RD −0.09 [−0.16, −0.01] I2 = 53% | 18 studies; 21 intervention arms; N = 3363 SMD −0.25 [−0.37, −0.14] I2 = 44% | 7 studies; 9 intervention arms; N = 1255 RD −0.09 [−0.14, −0.05] I2 = 0% | 13 studies; 16 intervention arms; N = 2880 SMD −0.18 [−0.30, −0.07] I2 = 41% | 3 studies; 3 intervention arm; N = 239 RD −0.14 [−0.24, −0.04] I2 = 0% | 7 studies; 8 intervention arm; N = 1902 SMD −0.14 [−0.28, 0.00] I2 = 41% |
| Subgroup differences | χ2 = 0.99, | χ2 = 3.37, | χ2 = 0.75, | χ2 = 1.39, | χ2 = 1.38, | χ2 = 0.61, |
| Sessions | Post Intervention | 3–9 Month Follow-up | 12-Month Follow-up | |||
|---|---|---|---|---|---|---|
| Depressive disorder (RD) | Depression symptoms (SMD) | Depressive disorder (RD) | Depression symptoms (SMD) | Depressive disorder (RD) | Depression symptoms (SMD) | |
| 8 or more | 13 studies; 15 intervention arm; N = 1503 RD −0.13 [−0.20, −0.07] I2 = 71% | 32 studies; 39 intervention arm; N = 8014 SMD −0.13 [−0.28, 0.01] | 12 studies; 16 intervention arm; N = 1881 RD −0.12 [−0.17, −0.07] I2 = 55% | 22 studies; 28 intervention arm; N = 5167 SMD −0.09 [−0.28, 0.10] | 9 studies; 10 intervention arms; N = 1149 RD −0.08 [−0.16, −0.00] I2= 75% | 16 studies; 21 intervention arm; N = 5047 SMD −0.11 [−0.17, −0.04] |
| <8 | 1 study; 1 intervention arm; N = 273 RD −0.01 [−0.11, 0.09] | 7 studies; 7 intervention arms; N = 1251 SMD −0.17 [−0.36, 0.02] | 2 studies; 2 intervention arms; N = 373 RD −0.07 [−0.14, 0.01] | 5 studies; 5 intervention arms; N = 1184 SMD −0.13 [−0.26, 0.00] | 0 studies | 0 studies |
| Depressive disorder (RD) | Depression symptoms (SMD) | Depressive disorder (RD) | Depression symptoms (SMD) | Depressive disorder (RD) | Depression symptoms (SMD) | |
| Subgroup differences | χ2 = 4.50, p = 0.03 | χ2 = 0.09, p = 0.76 | χ2 = 1.28, p = 0.26 | χ2 = 0.09, p = 0.76 | NA | NA |
| Delivery | Post Intervention | 3–9 Month Follow-up | 12-Month Follow-up | |||
|---|---|---|---|---|---|---|
| Depressive disorder (RD) | Depression symptoms (SMD) | Depressive disorder (RD) | Depression symptoms (SMD) | Depressive disorder (RD) | Depression symptoms (SMD) | |
| Mental health expert | 5 studies; 5 intervention arm; N = 665 RD −0.10 [−0.18, −0.01] I2 = 71% | 15 studies; 15 intervention arm; N = 2649 SMD −0.24 [−0.37, −0.11] I2 = 54% | 5 studies; 5 intervention arm; N = 883 RD −0.11 [−0.16, −0.06] I2 = 0% | 12 studies; 12 intervention arm; N = 2612SMD −0.21 [−0.33, −0.09] I2 = 52% | 2 studies; 2 intervention arm; N = 195 RD −0.12 [−0.24, −0.01] I2 = 0% | 8 studies; 8 intervention arm; N = 1718SMD −0.17 [−0.29, −0.05] I2 = 21% |
| Non mental health expert | 4 studies; 4 intervention arms; N = 597 RD −0.18 [−0.35, −0.02] I2 = 80% | 14 studies; 15 intervention arms; N = 5267 SMD 0.04 [−0.20, 0.28] | 5 studies; 5 intervention arms; N = 1065 RD -0.13 [−0.22, −0.05] I2 = 63% | 8 studies; 8 intervention arms; N = 2861 SMD 0.12 [−0.24, 0.47] | 4 studies; 4 intervention arm; N = 595 RD −0.02 [−0.09, 0.04] | 7 studies; 8 intervention arm; N = 3397 SMD −0.06 [−0.13, 0.01] |
| Student | 5 studies; 5 intervention arms; N = 514 RD −0.08 [−0.13, −0.03] I2 = 0% | 12 studies; 13 interventionarms; N = 1143 SMD −0.24 [−0.41, −0.07] I2 = 36% | 5 studies; 5 intervention arms; N = 306 RD −0.08 [−0.18, 0.02] | 8 studies; 9 intervention arms; N = 597 SMD −0.19 [−0.37, −0.00] I2 = 15% | 3 studies; 3 intervention arm; N = 359 RD −0.09 [−0.28, 0.11] | 3 studies; 3 intervention arms; N = 340 SMD −0.21 [−0.53, 0.10] |
| Subgroup differences | χ2 = 1.30, p = 0.52 | χ2 = 4.44, p = 0.11 | χ2 = 0.55, p = 0.76 | χ2 = 2.82, p = 0.24 | χ2 = 2.55, p = 0.28 | χ2 = 2.79, p = 0.25 |
| Tool | Post Intervention | 3–9 Month Follow-up | 12-Month Follow-up |
|---|---|---|---|
| Depression Symptoms (SMD) | Depression Symptoms (SMD) | Depression Symptoms (SMD) | |
| CDI/BDI | 24 studies; 30 intervention arm; N = 5686 SMD −0.06 [−0.26, 0.13] I2 = 90% | 17 studies; 22 intervention arm; N = 4085 SMD −0.05 [−0.29, 0.19]I2 = 91% | 12 studies; 17 intervention arm; N = 3770 SMD −0.10 [−0.18, -0.03] I2 = 4% |
| CES-D | 9 studies; 10 intervention arms; N = 2022 SMD −0.24 [−0.35, −0.13] I2 = 17% | 7 studies; 8 intervention arms; N = 1832 SMD −0.18 [−0.29, −0.06] I2 = 23% | 2 studies; 2 intervention arm; N = 196 SMD −0.25 [−0.77, 0.27] |
| RADS | 3 studies; 3 intervention arms; N = 213SMD −0.42 [−0.69, −0.14]I2 = 0% | 2 studies; 2 intervention arms; N = 192SMD −0.24 [−0.69, 0.22] | 1 study; 1 intervention arms; N = 70 SMD −0.30 [−0.77, 0.17] |
| Other | 3 studies; 3 intervention arms; N = 1344 SMD −0.00 [−0.11, 0.11] | 1 study; 1 intervention arm; N = 242 SMD −0.02 [−0.27, 0.24] | 1 study; 1 intervention arm; N = 1011 SMD −0.02 [−0.15, 0.10] |
| Subgroup differences | χ2 = 14.45, p = 0.002 | χ2 = 2.11, p = 0.55 | χ2 = 2.46, p = 0.48 |
4. Discussion
4.1. Principal Findings
4.2. Strengths and Weakness of the Study
4.3. Strengths and Weaknesses in Relation to other Studies, Discussing Important Differences in Results
4.4. Implications
5. Conclusions
Acknowledgements
Author Contributions
Conflicts of Interest
References
- Costello, J.E.; Erkanli, A.; Angold, A. Is there an epidemic of child or adolescent depression? J. Child Psychol. Psychiatry 2006, 47, 1263–1271. [Google Scholar] [PubMed]
- Kessler, R.C.; Kessler, R.C.; Berglund, P.; Demler, O.; Jin, R.; Merikangas, K.R.; Walters, E.E. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey replication. Arch. General Psychiatry 2005, 62, 593–602. [Google Scholar] [CrossRef]
- Belsher, G.; Costello, C.G. Relapse after recovery from unipolar depression: A critical review. Psychol. Bull. 1988, 104, 84–96. [Google Scholar] [CrossRef] [PubMed]
- Birmaher, B.; Ryan, N.D.; Williamson, D.E.; Brent, D.A.; Kaufman, J.; Dahl, R.E.; Perel, J.; Nelson, B.L. Childhood and adolescent depression: A review of the past 10 years: Part 1. J. Am. Acad. Child Adolesc. Psychiatry 1996, 35, 1427–1439. [Google Scholar] [CrossRef] [PubMed]
- Lewinsohn, P.M.; Rohde, P.; Seeley, J.R. Major depressive disorder in older adolescents: Prevalence, risk factors and clinical implications. Clin. Psychol. Rev. 1998, 18, 765–794. [Google Scholar] [CrossRef] [PubMed]
- Gould, M.S.; King, R.; Greenwald, S.; Fisher, P.; Schwab-Stone, M.; Kramer, R.; Flisher, A.J.; Goodman, S.; Canino, G.; Shaffer, D. Psychopathology associated with suicidal ideation and attempts among children and adolescents. J. Am. Acad. Child Adolesc. Psychiatry 1998, 37, 915–923. [Google Scholar] [CrossRef] [PubMed]
- Stice, E.; Shaw, H.; Bohon, C.; Marti, C.N.; Rohde, P. A meta-analytic review of depression prevention programs for children and adolescents: Factors that predict magnitude of intervention effects. J. Consult. Clin. Psychol. 2009, 77, 486–503. [Google Scholar] [CrossRef] [PubMed]
- Horowitz, J.; Garber, J. The prevention of depressive symptoms in children and adolescents: A meta-analytic review. J. Consult. Clin. Psychol. 2006, 74, 401–415. [Google Scholar] [CrossRef] [PubMed]
- Neil, A.L.; Christensen, H. Australian school-based prevention and early intervention programs for anxiety and depression: A systematic review. Med. J. Aust. 2007, 186. [Google Scholar] [CrossRef] [PubMed]
- Gillham, J.E.; Shatté, A.J.; Freres, D.R. Preventing depression: A review of cognitive-behavioral and family interventions. Appl. Prev. Psychol. 2000, 9, 63–88. [Google Scholar] [CrossRef]
- Gladstone, T.; Beardslee, W. The prevention of depression in children and adolescents: A review. Can. J. Psychiatry 2009, 54, 212–221. [Google Scholar] [PubMed]
- Merry, S.N.; Hetrick, S.E.; Cox, G.R.; Brudevold-Iversen, T.; Bir, J.J.; McDowell, H. Psychological and educational interventions for preventing depression in children and adolescents. Cochrane Database Syst. Rev. 2011. [Google Scholar] [CrossRef]
- Stellard, P.; Sayal, K.; Phillips, R.; Taylor, J.A.; Spears, M.; Anderson, R.; Araya, R.; Lewis, G.; Milings, A.; Montgomery, A.A. Classroom based cognitive behavioural therapy in reducing symptoms of depression in high risk adolescents: Pragmatic cluster randomised controlled trial. Br. Med. J. 2012, 345. [Google Scholar] [CrossRef]
- Harnett, P.H.; Dadds, M.R. Training school personnel to implement a universal school-based prevention of depression program under real-world conditions. J. School Psychol. 2004, 42, 343–357. [Google Scholar] [CrossRef]
- Brunwasser, S.M.; Gillham, J.E.; Kim, E.S. A meta-analytic review of the Penn Resiliency Program’s effect on depressive symptoms. J. Consult. Clin. Psychol. 2009, 77, 1042–1054. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. 2011. Available online: http://www.cochrane-handbook.org (accessed on 18 March 2011).
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343. [Google Scholar] [CrossRef] [Green Version]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. Introduction to Meta-Analysis; John WIley & Sons: Chichister, UK, 2008. [Google Scholar]
- RevMan. In Review Manager (RevMan). Version 5.0; The Nordic Cochrane Centre, The Cochrane Collaboration: Copenhagen, Denmark, 2008.
- Arnarson, E.Ö.; Craighead, W.E. Prevention of depression among Icelandic adolescents. Behav. Res. Therapy 2009, 47, 577–585. [Google Scholar]
- Balle, M.; Tortella-Feliu, M. Efficacy of a brief school-based program for selective prevention of childhood anxiety. Anxiety Stress Coping 2010, 23, 71–85. [Google Scholar] [CrossRef]
- Berry, K.; Hunt, C.J. Evaluation of an intervention program for anxious adolescent boys who are bullied at school. J. Adolesc. Health 2009, 45, 376–382. [Google Scholar] [CrossRef]
- Barnet, B.; Liu, J.; DeVoe, M.; Alperovitz-Bichell, K.; Duggan, A.K. Home visiting for adolescent mothers: Effects on parenting, maternal life course, and primary care linkage. Ann. Fam. Med. 2007, 5, 224–232. [Google Scholar] [CrossRef] [PubMed]
- Bond, L.; Patton, G.; Glover, S.; Carlin, J.B.; Butler, H.; Thomas, L.; Bowes, G. The gatehouse project: Can a multilevel school intervention affect emotional wellbeing and health risk behaviours? J. Epidemiol. Community Health 2004, 58, 997–1003. [Google Scholar] [CrossRef] [PubMed]
- Cabiya, J.J.; Padilla-Cotto, L.; Gonzalez, K.; Sanchez-Cestero, J.; Martinez-Taboas, A.; Sayers, S. Effectiveness of a cognitive-behavioral intervention for Puerto Rican children. Rev. Interam. Psicol. 2008, 42, 195–202. [Google Scholar]
- Calear, A.L.; Christensen, H.; Mackinnon, A.; Griffiths, K.M.; O’Kearney, R. The YouthMood Project: A cluster randomized controlled trial of an online cognitive behavioral program with adolescents [ISRCTN67189839]. J. Consult. Clin. Psychol. 2009, 77, 1021–1032. [Google Scholar] [CrossRef]
- Cardemil, E.V.; Reivich, K.J.; Seligman, M. The prevention of depressive symptoms in low-income minority middle school students. Prev. Treat. 2002, 5. [Google Scholar] [CrossRef]
- Chaplin, T.M.; Gillham, J.E.; Reivich, K.; Elkon, A.G.; Samuels, B.; Freres, D.R.; Winder, B.; Seligman, M.E. Depression prevention for early adolescent girls a pilot study of all girls versus co-ed groups. J. Early Adolesc. 2006, 26, 110–126. [Google Scholar] [CrossRef]
- Clarke, G.N.; Hawkins, W.; Murphy, M.; Sheeber, L. School-based primary prevention of depressive symptomatology in adolescents findings from two studies. J. Adolesc. Res. 1993, 8, 183–204. [Google Scholar] [CrossRef]
- Clarke, G.N.; Hawkins, W.; Murphy, M.; Sheeber, L.B.; Lewinsohn, P.M.; Seeley, J.R. Targeted prevention of unipolar depressive disorder in an at-risk sample of high school adolescents: A randomized trial of group cognitive intervention. J. Am. Acad. Child Adolesc. Psychiatry 1995, 34, 312–321. [Google Scholar] [CrossRef]
- Clarke, G.N.; Hornbrook, M.; Lynch, F.; Polen, M.; Gale, J.; Beardslee, W.; O’Connor, E.; Seeley, J.R. A randomized trial of a group cognitive intervention for preventing depression in adolescent offspring of depressed parents. Arch. Gen. Psychiatry 2001, 58, 1127–1134. [Google Scholar] [CrossRef] [PubMed]
- Garber, J.; Clarke, G.N.; Weersing, V.R.; Beardslee, W.R.; Brent, D.A.; Gladstone, T.R.G.; DeBar, L.L.; Lynch, F.L.; Hollon, S.D.; Shamseddeen, D.; et al. Prevention of Depression in at-risk adolescents: A randomized controlled trial. JAMA 2009, 301, 2215–2224. [Google Scholar]
- Gillham, J.E.; Reivich, K.J.; Jaycox, L.H.; Seligman, M.E. Prevention of depressive symptoms in schoolchildren: Two-year follow-up. Psychol. Sci. 1995, 6, 343–351. [Google Scholar] [CrossRef]
- Gillham, J.E.; Reivich, K.J.; Freres, D.R.; Lascher, M.; Litzinger, S.; Shatté, A.; Seligman, M.E. School-based prevention of depression and anxiety symptoms in early adolescence: A pilot of a parent intervention component. School Psychol. Q. 2006, 21, 323–348. [Google Scholar] [CrossRef]
- Gillham, J.E.; Hamilton, J.; Freres, D.R.; Patton, K.; Gallop, R. Preventing depression among early adolescents in the primary care setting: A randomized controlled study of the Penn Resiliency Program. J. Abnorm. Child Psychol. 2006, 34, 203–219. [Google Scholar] [CrossRef] [PubMed]
- Gillham, J.E.; Reivich, K.J.; Freres, D.R.; Chaplin, T.M.; Shatté, A.J.; Samuels, B.; Elkon, A.G.L.; Litzinger, S.; Lascher, M.; Gallop, R.; et al. School-based prevention of depressive symptoms: A randomized controlled study of the effectiveness and specificity of the Penn Resiliency Program. J. Consult. Clin. Psychol. 2007, 75. [Google Scholar] [CrossRef]
- Hains, A.A.; Szyjakowski, M. A cognitive stress-reduction intervention program for adolescents. J. Couns. Psychol. 1990, 27, 79–84. [Google Scholar] [CrossRef]
- Hains, A. Comparison of cognitive-behavioural stress management techniques with adolescent boys. J. Cons. Dev. 1992, 70, 600–605. [Google Scholar] [CrossRef]
- Horowitz, J.L.; Garber, J.; Ciesla, J.A.; Young, J.F.; Mufson, L. Prevention of depressive symptoms in adolescents: A randomized trial of cognitive-behavioral and interpersonal prevention programs. J. Consult. Clin. Psychol. 2007, 75, 693–706. [Google Scholar] [CrossRef] [PubMed]
- Hyun, M.; Chung, H.I.; Lee, Y.J. The effect of cognitive-behavioral group therapy on the self-esteem, depression, and self-efficacy of runaway adolescents in a shelter in South Korea. Appl. Nurs. Res. 2005, 18, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Kraag, G.; Van Breukelen, G.J.P.; Kok, G.; Hosman, C. “Learn Young, Learn Fair”, a stress management program for fifth and sixth graders: Longitudinal results from an experimental study. J. Child Psychol. Psychiatry 2009, 50, 1185–1195. [Google Scholar] [CrossRef] [PubMed]
- Lock, S.; Barrett, P.M. A longitudinal study of developmental differences in universal preventive intervention for child anxiety. Behav. Chang. 2003, 20, 183–199. [Google Scholar] [CrossRef]
- Lowry-Webster, H.M.; Barrett, P.M.; Lock, S. A universal prevention trial of anxiety symptomology during childhood: Results at 1-year follow-up. Behav. Chang. 2003, 20, 25–43. [Google Scholar] [CrossRef]
- Pössel, P.; Horn, A.B.; Groen, G.; Hautzinger, M. School-based prevention of depressive symptoms in adolescents: A 6-month follow-up. J. Am. Acad. Child Adolesc. Psychiatry 2004, 43, 1003–1010. [Google Scholar] [CrossRef] [PubMed]
- Pössel, P.; Seemann, S.; Hautzinger, M. Impact of comorbidity in prevention of adolescent depressive symptoms. J. Couns. Psychol. 2008, 55, 106–117. [Google Scholar] [CrossRef]
- Puskar, K.; Sereika, S.; Tusaie Mumford, K. Effect of the Teaching Kids to Cope (TKC©) program on outcomes of depression and coping among rural adolescents. J. Child Adolesc. Psychiatr. Nurs. 2003, 16, 71–80. [Google Scholar] [CrossRef] [PubMed]
- Quayle, D.; Dziurawiec, S.; Roberts, C.; Kane, R.; Ebsworthy, G. The effect of an optimism and lifeskills program on depressive symptoms in preadolescence. Behav. Chang. 2001, 18, 194–203. [Google Scholar] [CrossRef]
- Rivet-Duval, E.; Heriot, S.; Hunt, C. Preventing adolescent depression in Mauritius: A universal school-based program. Child Adolesc. Mental Health 2010, 16, 86–91. [Google Scholar] [CrossRef]
- Roberts, C.; Kane, R.; Thomson, H.; Bishop, B.; Hart, B. The prevention of depressive symptoms in rural school children: A randomized controlled trial. J. Consult. Clin. Psychol. 2003, 71, 622–628. [Google Scholar] [CrossRef] [PubMed]
- Roberts, C.M.; Kane, R.; Bishop, B.; Cross, D.; Fenton, J.; Hart, B. The prevention of anxiety and depression in children from disadvantaged schools. Behav. Res. Therapy 2010, 48, 68–73. [Google Scholar] [CrossRef]
- The Prevention of Depression in 8- to 9-Year-Old Children: A Pilot Study. Available online: http://espace.library.curtin.edu.au/R/?func=dbin-jump-full&object_id=148912&local_base=GEN01-ERA02 (accessed on 6 August 2014).
- Sawyer, M.G.; Pfeiffer, S.; Spence, S.H.; Bond, L.; Graetz, B.; Kay, D.; Sheffield, J. School based prevention of depression: A randomised controlled study of the beyondblue schools research initiative. J. Child Psychol. Psychiatry 2010, 51, 199–209. [Google Scholar] [CrossRef] [PubMed]
- The Prevention of Depression and Anxiety. Available online: http://www.ppc.sas.upenn.edu/depprevseligman1999.pdf (accessed on 6 August 2014).
- Seligman, M.E.P.; Schulman, P.; Tryon, A.M. Group prevention of depression and anxiety symptoms. Behav. Res. Therapy 2007, 45, 1111–1126. [Google Scholar] [CrossRef]
- Shatte, A.J. Prevention of depressive symtpoms in adolescents: Issues of dissemination and mechanisms of change. Diss. Abstr. Int. Sect. B: Sci. Eng. 1997, 57. [Google Scholar] [CrossRef]
- Sheffield, J.K.; Spence, S.H.; Rapee, R.M.; Kowalenko, N.; Wignall, A.; Davis, A.; McLoone, J. Evaluation of universal, indicated, and combined cognitive-behavioral approaches to the prevention of depression among adolescents. J. Consult. Clin. Psychol. 2006, 74, 66–79. [Google Scholar] [CrossRef] [PubMed]
- Spence, S.H.; Sheffield, J.K.; Donovan, C.L. Preventing adolescent depression: An evaluation of the problem solving for life program. J. Consult. Clin. Psychol. 2003, 71, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Stice, E.; Burton, E.; Bearman, S.K.; Rohde, P. Randomized trial of a brief depression prevention program: An elusive search for a psychosocial placebo control condition. Behav. Res. Therapy 2007, 45, 863–876. [Google Scholar] [CrossRef]
- Stice, E.; Rohde, P.; Seeley, J.R.; Gau, J.M. Brief cognitive-behavioral depression prevention program for high-risk adolescents outperforms two alternative interventions: A randomized efficacy trial. J. Consult. Clin. Psychol. 2008, 76, 595–606. [Google Scholar] [CrossRef] [PubMed]
- Yu, D.L.; Seligman, M.E. Preventing depressive symptoms in Chinese children. Prev. Treat. 2002, 5. [Google Scholar] [CrossRef]
- Young, J.F.; Mufson, L.; Davies, M. Efficacy of interpersonal psychotherapyadolescent skills training: An indicated preventive intervention for depression. J. Child Psychol. Psychiatry 2006, 47, 1254–1262. [Google Scholar] [PubMed]
- Araya, R.; Fritsch, R.; Soears, M.; Rojas, G.; Martinez, V.; Barroihet, S.; Vohringer, V.; Gunnell, D.; Stallard, P.; Guajardo, V.; et al. School intervention to improve mental health of students in Santiago, Chile. JAMA Pediatr. 2013, 167, 1004–1010. [Google Scholar] [CrossRef] [PubMed]
- Rose, G. The Strategy of Preventive Medicine, 1st ed.; Oxford University Press: Oxford, UK, 1992. [Google Scholar]
- Merry, S.; McDowell, H.; Wild, C.; Bir, J.; Cunliffe, R. A randomized placebo-controlled trial of a school-based depression prevention program. J. Am. Acad. Child Adolesc. Psychiatry 2004, 43, 538–547. [Google Scholar] [CrossRef] [PubMed]
- Van Voorhees, B.W.; Fogel, J.; Reinecke, M.A.; Gladstone, T.; Stuart, S.; Gollan, J.; Bradford, N.; Domanico, R.; Fagan, B.; Ross, R.; et al. Randomized clinical trial of an Internet-based depression prevention program for adolescents (Project CATCH-IT) in primary care: 12-Week outcomes. J. Dev. Behav. Pediatr. 2009, 30, 123–137. [Google Scholar] [CrossRef]
- McCarty, C.A.; Weisz, J.R. Effects of psychotherapy for depression in children and adolescents: What we can (and can’t) learn from meta-analysis and component profiling. J. Am. Acad. Child Adolesc. Psychiatry 2007, 46, 879–886. [Google Scholar] [CrossRef] [PubMed]
- Whittaker, R.; Merry, S.M.; Stasiak, K.; McDowell, H.; Doherty, I.; Shepherd, M.; Dorey, E.; Parag, V.; Ameratunga, S.; Rodgers, A. MEMO—A mobile phone depression prevention intervention for adolescents: Development process and postprogram findings on acceptability from a randomized controlled trial. J. Med. Internet Res. 2012, 14. [Google Scholar] [CrossRef]
- Weersing, V.R.; Rozenman, M.; Gonzalez, A. Core components of therapy in youth: Do we know what to disseminate? Behav. Modif. 2009, 33, 24–47. [Google Scholar] [CrossRef] [PubMed]
- Hetrick, S.E.; Cox, G.R.; Fisher, C.A.; Bhar, S.S.; Rice, S.M.; Davey, C.G.; Parker, A.G. Back to basics: Could behavioural therapy be a better treatment option for youth depression? A critical review. Early Interv. Psychiatry 2015, 9, 93–99. [Google Scholar] [CrossRef]
- Pennant, M.E.; Loucas, C.E.; Whittington, C.; Creswell, C.; Fonagy, P.; Fuggle, P.; Kelvin, P.; Naqvi, S.; Stockton, S.; Kendall, T. Computerised therapies for anxiety and depression in children and young people: A systematic review and meta-analysis. Behav. Res. Ther. 2015, 67, 1–18. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hetrick, S.E.; Cox, G.R.; Merry, S.N. Where to Go from Here? An Exploratory Meta-Analysis of the Most Promising Approaches to Depression Prevention Programs for Children and Adolescents. Int. J. Environ. Res. Public Health 2015, 12, 4758-4795. https://doi.org/10.3390/ijerph120504758
Hetrick SE, Cox GR, Merry SN. Where to Go from Here? An Exploratory Meta-Analysis of the Most Promising Approaches to Depression Prevention Programs for Children and Adolescents. International Journal of Environmental Research and Public Health. 2015; 12(5):4758-4795. https://doi.org/10.3390/ijerph120504758
Chicago/Turabian StyleHetrick, Sarah E., Georgina R. Cox, and Sally N. Merry. 2015. "Where to Go from Here? An Exploratory Meta-Analysis of the Most Promising Approaches to Depression Prevention Programs for Children and Adolescents" International Journal of Environmental Research and Public Health 12, no. 5: 4758-4795. https://doi.org/10.3390/ijerph120504758