
A Theory-Based Approach for Developing Interventions to Change Patient Behaviours: A Medication Adherence Example from Paediatric Secondary Care

Abstract
:1. Introduction
1.1. An Introduction to Behaviour Change Interventions
1.2. An Introduction to the Illustrative Example
2. The Process of Intervention Development

{kind=link}
| Stages of Intervention Development | Brief Description of Each Stage |
|---|---|
| Conducting a needs assessment | Develop understanding of why and how the target population needs to change. Specify the health problem and it associated consequences and the target problem behaviour(s). |
| Identifying determinants of the target behaviour | Develop an understanding of what is influencing or causing the problematic behaviour. Try to identify factors leading to or inhibiting that behaviour. |
| Setting intervention objectives | Set goals for your intervention in terms of changing the target behaviour, behavioural determinants and associated health outcomes. |
| Selecting behaviour change techniques (BCTs) | Choose behaviour change techniques that can be used in your intervention programme to help achieve your intervention goals. |
| Developing practical plans | Select methods for delivering your intervention that will be acceptable and engaging for the target population. Consider how you will assess intervention effectiveness. |
| Reporting intervention outcomes | Communicate the effects of your intervention to relevant others (e.g., health practitioners, researchers, commissioners, patients). |
2.1. Stage One: Conducting a Needs Assessment
Adolescent patients (aged 12 to 16 years) receiving secondary outpatient care for asthma, who experience frequent symptoms despite being prescribed appropriate medications, who are not suspected to have refractory asthma, who are suspected or known to have poor adherence to medicines (e.g., taking inhalers infrequently or at the wrong dosage level), and who have no contraindications for receiving the intervention, such as social, psychological or communication issues.
“Control of asthmatic condition indicated by presence of daily symptoms (including coughing, wheezing, chest tightness and breathlessness), sleep disturbance, frequency of exacerbations, use of rescue medication, and the extent to which activities are limited”.
Taking medications as prescribed, including “preventer” inhalers, “rescue” inhalers, and any given tablets or other medicines; taking these at the prescribed dosage using the correct inhalation technique or consumption method; taking them at the required intervals and at the required times without missing any doses; and refilling prescriptions when necessary to ensure no doses are missed.
2.2. Stage Two: Identifying Determinants of the Target Behaviour
2.2.1. Determinants in the Target Population
| 1. Beliefs and Attitudes |
| Beliefs about asthma (e.g., cause, severity, controllability) |
| Beliefs about medicines |
| Attitude towards clinic visits |
| Attitude towards non-adherence (e.g., anticipated regret) |
| 2. Experiences |
| Perceived impact of asthma and medicines on daily life |
| Experience of symptoms |
| Previous experience of adherence and management |
| Prior experience of consequences (e.g., hospitalization) |
| 3. Knowledge |
| Knowledge and understanding of asthma and medicines |
| Knowledge of appropriate response in acute attacks |
| Recognising danger signals and symptoms |
| 4. Social Influences |
| Peer group influences (e.g., feeling normal, embarrassed, perceived support) |
| Family factors (e.g., parent involvement in medicine-taking) |
| Relationships with healthcare professionals |
| 5. Motivations and Intention |
| Motivation to manage asthma |
| Tolerance of current illness state |
| Prioritising asthma and treatment |
| Intention to take medications |
| Preference for alternative therapies |
| 6. Capability |
| Skills to use the medication devices |
| Organisational and scheduling abilities |
| Self-efficacy (e.g., perceived ability, confidence) |
| Practical barriers (e.g., lost medicines) |
| 7. Self-Perceptions |
| Self-identity |
| Perceived autonomy in taking medications |
| Feelings of responsibility for health |
| 8. Emotions and Psychological Wellbeing (e.g., fear of asthma exacerbations) |
| 9. Forgetting and Confusion |
2.2.2. Individual Determinants
| Example Qualitative Questions |
|---|
|
|
|
|
|
|
|
|
|
|
|
2.2.3. Organising Framework
2.3. Stage Three: Setting Behaviour Change Intervention Objectives
2.3.1. Health and Behaviour Change Objectives
- -
- Health objective: To achieve a decrease in general asthma symptoms (coughing, wheezing, chest tightness, breathlessness) from 1 to 2 days per week to no days per week.
- -
- Behavioural objective: To achieve a decrease in the frequency of missed doses of (named medication) from once per week to no times per week.
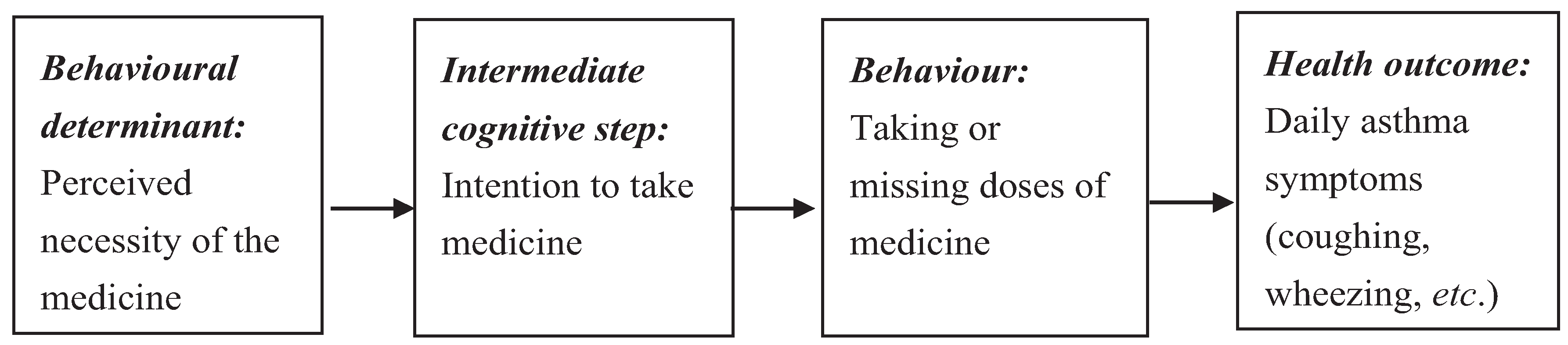
2.3.2. Behavioural Determinant Change Objectives
2.3.3. Mapping Determinants to Theory
Determinant change objective: The patient will demonstrate an increase in perceived necessity of (named medication) for maintaining health and reducing symptoms (measured by the Beliefs about Medicines Questionnaire).

2.4. Stage Four: Selecting Behaviour Change Techniques
2.5. Stage Five: Developing Practical Plans
Planning an Evaluation
2.6. Stage Six: Reporting the Intervention
3. Discussion and Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- General Medical Council. Tomorrow’s Doctors: Outcomes and Standards for Undergraduate Medical Education; General Medical Council: Manchester, UK, 2009. [Google Scholar]
- Bartholomew, L.K.; Mullen, P.D. Five roles for using theory and evidence in the design and testing of behavior change interventions. J. Public Health Dent. 2011, 71, S20–S33. [Google Scholar] [CrossRef] [PubMed]
- British Psychological Society. Careers: Your Journey into Psychology. Available online: http://careers.bps.org.uk/ (accessed on 8 October 2015).
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. BMJ 2008. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; Prestwich, A. Are interventions theory-based? Development of a theory coding scheme. Health Psychol. 2010, 29, 1–8. [Google Scholar] [PubMed]
- National Institute for Health and Care Excellence. Behaviour Change: Individual Approaches, in NICE Public Health Guidance. Available online: https://www.nice.org.uk/guidance/ph49 (accessed on 8 October 2015).
- Becker, M.H. The health belief model and personal health behavior. Health Educ. Behav. 1974, 2, 354–386. [Google Scholar] [CrossRef]
- Brug, J.; Oenema, A.; Ferreira, I. Theory, evidence and Intervention Mapping to improve behavior nutrition and physical activity interventions. Int. J. Behav. Nutr. Phys. Act. 2005, 2, 2–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartholomew, L.K.; Parcel, G.S.; Kok, G.; Gottlieb, N.H. Planning Health Promotion Programmes: An Intervention Mapping Approach, 3rd ed.; John Wiley & Sons: San Francisco, CA, USA, 2011. [Google Scholar]
- Cameron, E. Behaviour change intervention competence, stage two qualification in health psychology. Unpublished report. 2014. [Google Scholar]
- Horne, R. Compliance, adherence, and concordance: Implications for asthma treatment. CHEST J. 2006, 130, 65S–72S. [Google Scholar] [CrossRef] [PubMed]
- British Thoracic Society Scottish Intercollegiate Guidelines Network. British Guideline on the Management of Asthma: A National Clinical Guideline. Available online: https://www.brit-thoracic.org.uk/document-library/clinical-information/asthma/btssign-guideline-on-the-management-of-asthma/ (accessed on 8 October 2015).
- Horne, R.; Weinman, J.; Hankins, M. The beliefs about medicines questionnaire: The development and evaluation of a new method for assessing the cognitive representation of medication. Psychol. Health 1999, 14, 1–24. [Google Scholar] [CrossRef]
- Broadbent, E.; Petrie, K.J.; Main, J.; Weinman, J. The brief illness perception questionnaire. J. Psychosom. Res. 2006, 60, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Luszczynska, A.; Schwarzer, R. Social cognitive theory. In Predicting Health Behaviour; Connor, M., Norman, P., Eds.; Open University Press: Berkshire, UK, 2005. [Google Scholar]
- Bursch, B.; Schwankovsky, L.; Gilbert, J.; Zeiger, R. Construction and validation of four childhood asthma self-management scales: Parent barriers, child and parent self-efficacy, and parent belief in treatment efficacy. J. Asthma 1999, 36, 115–128. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; Johnston, M.; Abraham, C.; Lawton, R.; Parker, D.; Walker, A. Making psychological theory useful for implementing evidence based practice: A consensus approach. Qual. Saf. Health Care 2005, 14, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Cane, J.; O’Connor, D.; Michie, S. Validation of the theoretical domains framework for use in behaviour change and implementation research. Implement. Sci. 2012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Webb, T.; Joseph, J.; Yardley, L.; Michie, S. Using the internet to promote health behavior change: A systematic review and meta-analysis of the impact of theoretical basis, use of behavior change techniques, and mode of delivery on efficacy. J. Med. Internet Res. 2010. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Social Foundations of Thought and Action: A Social Cognitive Theory; Prentice-Hall, Inc.: Englewood, NJ, USA, 1986. [Google Scholar]
- Leventhal, H.; Leventhal, E.; Contrada, R.J. Self-regulation, health, and behaviour: A perceptual-cognitive approach. Psychol. Health 1998, 13, 717–733. [Google Scholar] [CrossRef]
- Horne, R.; Weinman, J. Self-regulation and self-management in asthma: Exploring the role of illness perceptions and treatment beliefs in explaining non-adherence to preventer medication. Psychol. Health 2002, 17, 17–32. [Google Scholar] [CrossRef]
- Abraham, C. Interventions to change health-related behaviour patterns. In Health Psychology; French, D., Vedhara, K., Kaptein, A.A., Weinma, J., Eds.; BPS Blackwell: Oxford, UK, 2010; pp. 99–110. [Google Scholar]
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.P.; Cane, J.; Wood, C.E. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Ann. Behav. Med. 2013, 46, 81–95. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Self Efficacy: The Exercise of Control; W.H. Freeman and Company: New York, NY, USA, 1997. [Google Scholar]
- Michie, S.; Johnston, M.; Francis, J.; Hardeman, W.; Eccles, M. From theory to intervention: Mapping theoretically derived behavioural determinants to behaviour change techniques. Appl. Psychol. 2008, 57, 660–680. [Google Scholar] [CrossRef]
- Michie, S.; Atkins, L.; West, R. The Behaviour Change Wheel: A Guide to Designing Interventions; University College London Press: London, UK, 2014. [Google Scholar]
- Michie, S.; Johnston, M. Theories and techniques of behaviour change: Developing a cumulative science of behaviour change. Health Psychol. Rev. 2012, 6, 1–6. [Google Scholar] [CrossRef]
- Rand, C.S.; Wise, R.A. Measuring adherence to asthma medication regimens. Am. J. Respir. Crit. Care Med. 1994, 149, S69–S76. [Google Scholar] [CrossRef] [PubMed]
- Abraham, C.; Michie, S. A taxonomy of behaviour change techniques used in interventions. Health Psychol. 2008, 27, 379–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Barbour, V.; Macdonald, H.; Johnston, M.; Lamb, S.E.; et al. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014. [Google Scholar] [CrossRef] [Green Version]
- Davidoff, F.; Batalden, P.; Stevens, D.; Ogrinc, G.; Mooney, S. Publication guidelines for quality improvement in health care: Evolution of the SQUIRE project. Qual. Saf. Health Care 2008, 17, i3–i9. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heath, G.; Cooke, R.; Cameron, E. A Theory-Based Approach for Developing Interventions to Change Patient Behaviours: A Medication Adherence Example from Paediatric Secondary Care. Healthcare 2015, 3, 1228-1242. https://doi.org/10.3390/healthcare3041228
Heath G, Cooke R, Cameron E. A Theory-Based Approach for Developing Interventions to Change Patient Behaviours: A Medication Adherence Example from Paediatric Secondary Care. Healthcare. 2015; 3(4):1228-1242. https://doi.org/10.3390/healthcare3041228
Chicago/Turabian StyleHeath, Gemma, Richard Cooke, and Elaine Cameron. 2015. "A Theory-Based Approach for Developing Interventions to Change Patient Behaviours: A Medication Adherence Example from Paediatric Secondary Care" Healthcare 3, no. 4: 1228-1242. https://doi.org/10.3390/healthcare3041228