Detection Rate of 18F-Labeled PSMA PET/CT in Biochemical Recurrent Prostate Cancer: A Systematic Review and a Meta-Analysis

 ,
,  and
and
Abstract
:1. Introduction
2. Methods
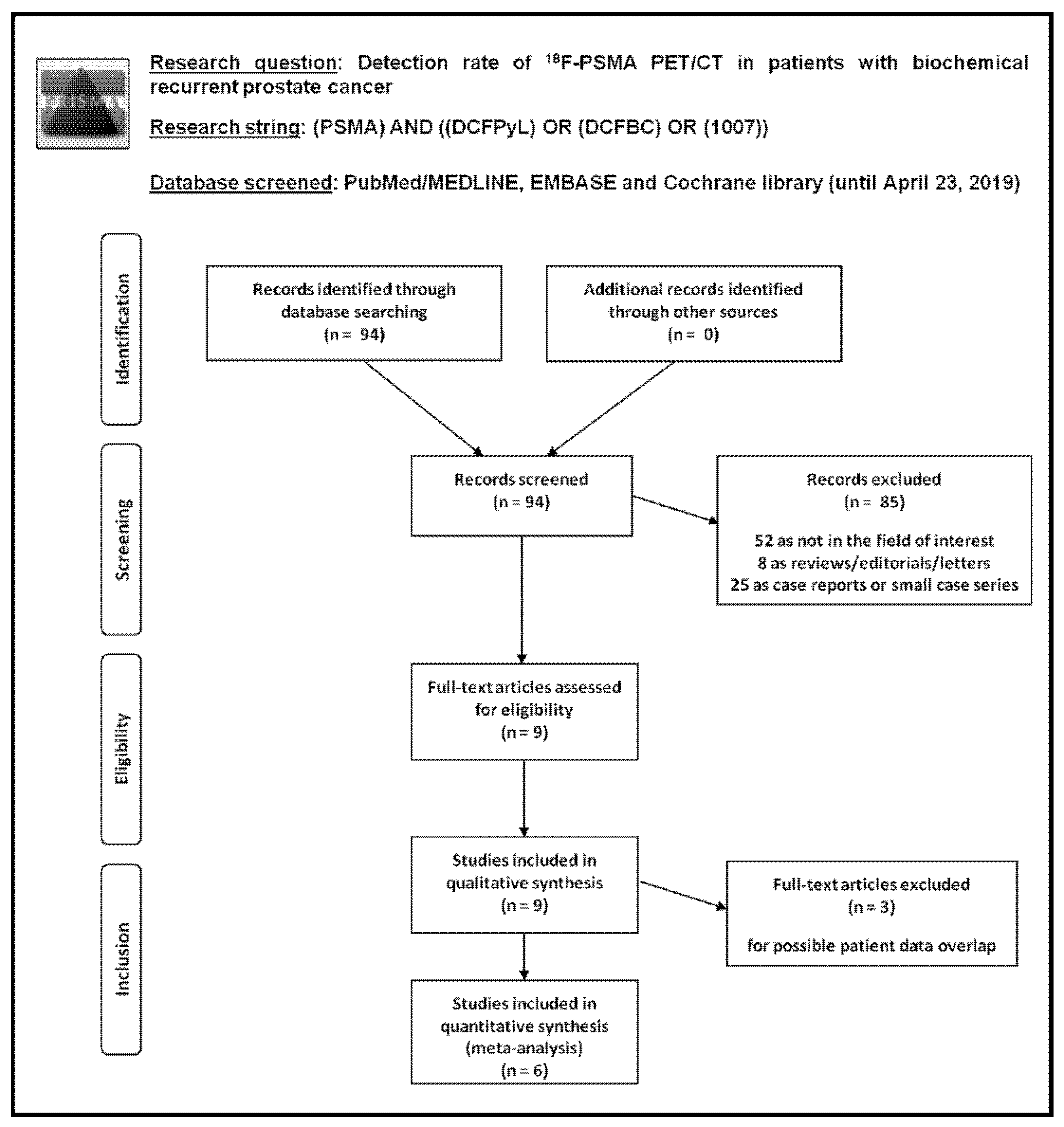
2.1. Search Strategy
2.2. Study Selection
2.3. Data Extraction
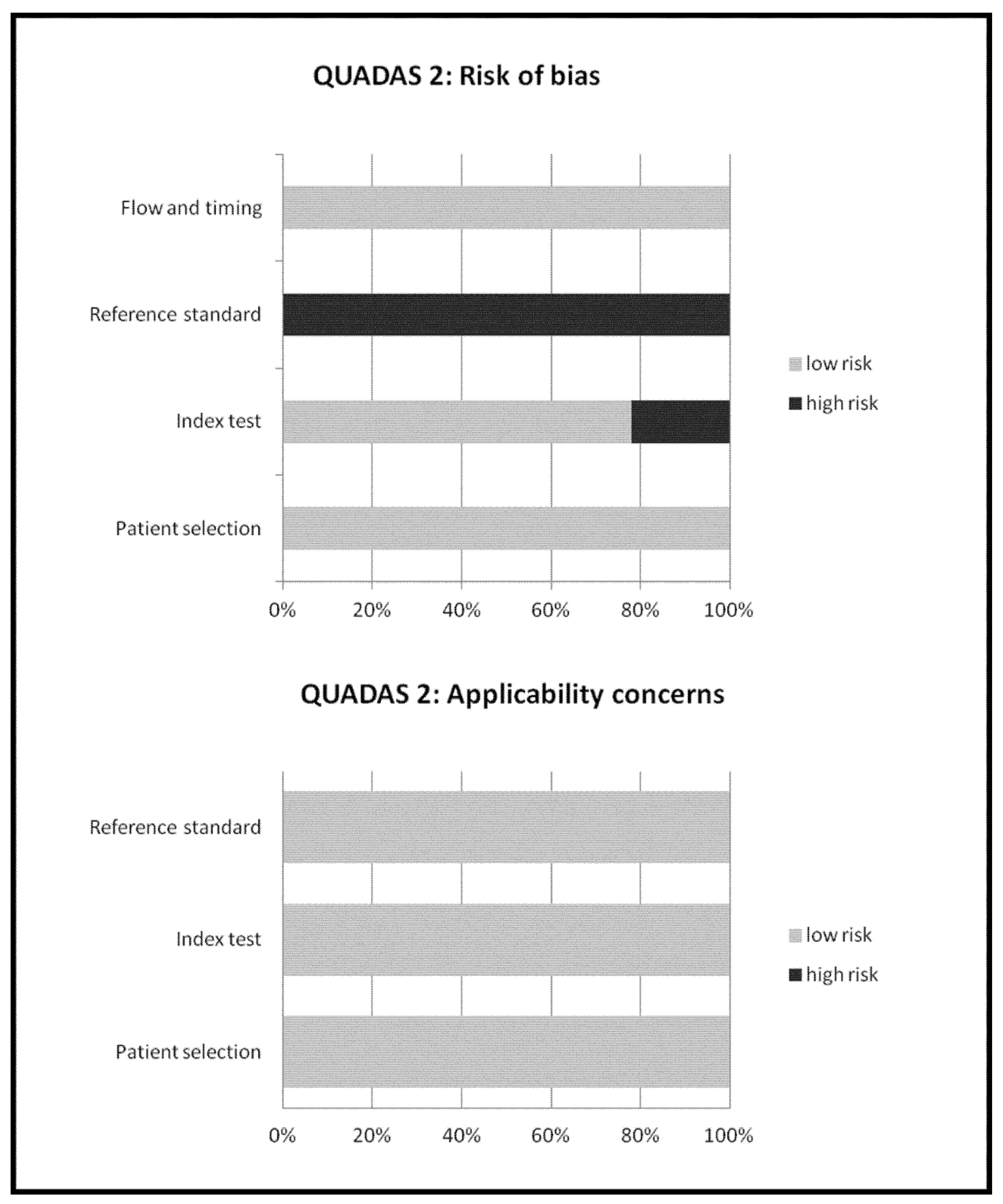
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
3.1. Literature Search
3.2. Qualitative Analysis (Systematic Review)
3.2.1. Basic Study and Patient Characteristics
3.2.2. Technical Aspects
3.2.3. Main Findings
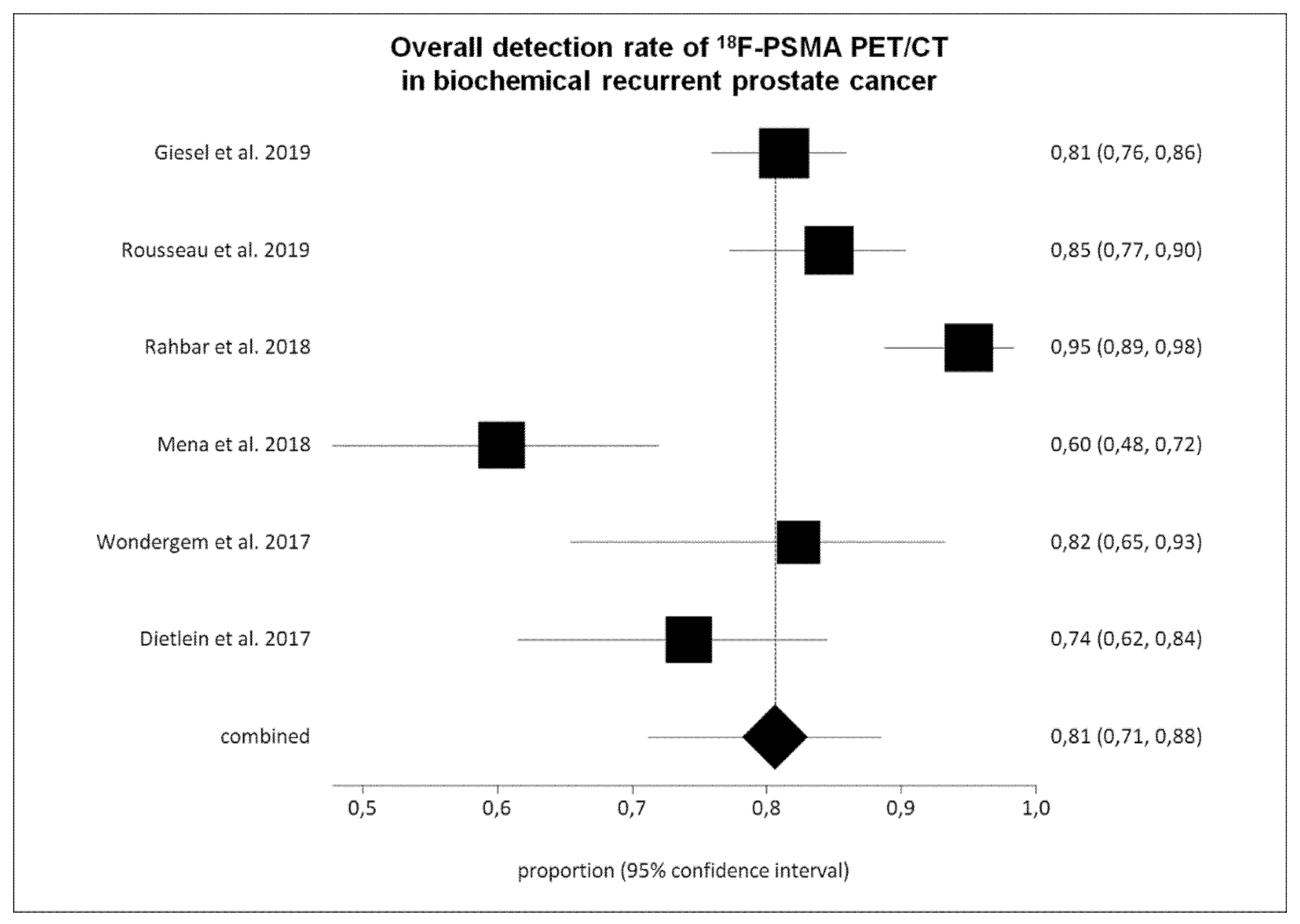
3.3. Quantitative Analysis (Meta-Analysis)
4. Discussion
5. Conclusions
- 18F-labeled PSMA PET/CT demonstrated a good DR in BRPCa, in particular using 18F-PSMA-1007 and 18F-DCFPyL, with similar results compared to those reported in the literature with 68Ga-labeled PSMA PET/CT.
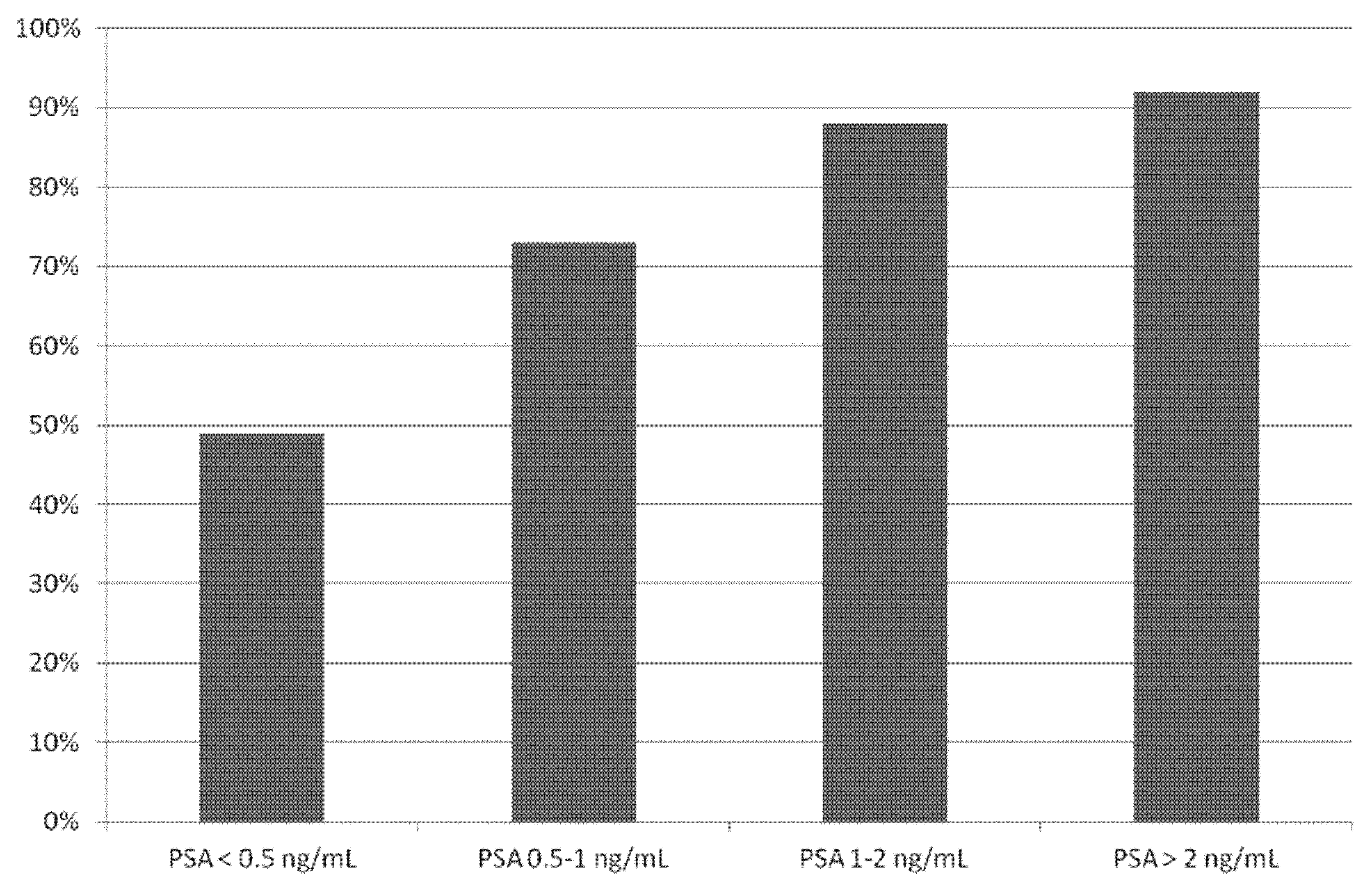
- The DR of 18F-labeled PSMA PET/CT is related to PSA values with significant lower DR in patients with PSA < 0.5 ng/mL.
- Prospective multicentric trials are needed to confirm these findings; nevertheless, 18F-labeled PSMA PET/CT seems to be a promising cost-effective alternative to 68Ga-labeled PSMA PET/CT in BRPCa.
Author Contributions
Funding
Conflicts of Interest
References
- Fanti, S.; Minozzi, S.; Antoch, G.; Banks, I.; Briganti, A.; Carrio, I.; Chiti, A.; Clarke, N.; Eiber, M.; De Bono, J.; et al. Consensus on molecular imaging and theranostics in prostate cancer. Lancet Oncol. 2018, 19, e696–e708. [Google Scholar] [CrossRef]
- Tangel, M.R.; Rastinehad, A.R. Advances in prostate cancer imaging. F1000Research 2018, 7. [Google Scholar] [CrossRef] [PubMed]
- O’Keefe, D.S.; Bacich, D.J.; Huang, S.S.; Heston, W.D.W. A Perspective on the Evolving Story of PSMA Biology, PSMA-Based Imaging, and Endoradiotherapeutic Strategies. J. Nucl. Med. 2018, 59, 1007–1013. [Google Scholar] [CrossRef] [PubMed]
- Ceci, F.; Castellucci, P.; Fanti, S. Current application and future perspectives of PSMA PET imaging in prostate cancer. Q. J. Nucl. Med. Mol. Imaging 2019, 63, 7–18. [Google Scholar] [CrossRef]
- Giovacchini, G.; Giovannini, E.; Riondato, M.; Ciarmiello, A. PET/CT With (68)Ga-PSMA in Prostate Cancer: Radiopharmaceutical Background and Clinical Implications. Curr. Radiopharm. 2018, 11, 4–13. [Google Scholar] [CrossRef]
- Gourni, E.; Henriksen, G. Metal-Based PSMA Radioligands. Molecules 2017, 22, 523. [Google Scholar] [CrossRef]
- Czarniecki, M.; Mena, E.; Lindenberg, L.; Cacko, M.; Harmon, S.; Radtke, J.P.; Giesel, F.; Turkbey, B.; Choyke, P.L. Keeping up with the prostate-specific membrane antigens (PSMAs): An introduction to a new class of positron emission tomography (PET) imaging agents. Transl. Androl. Urol. 2018, 7, 831–843. [Google Scholar] [CrossRef]
- Eiber, M.; Fendler, W.P.; Rowe, S.P.; Calais, J.; Hofman, M.S.; Maurer, T.; Schwarzenboeck, S.M.; Kratowchil, C.; Herrmann, K.; Giesel, F.L. Prostate-Specific Membrane Antigen Ligands for Imaging and Therapy. J. Nucl. Med. 2017, 58, 67S–76S. [Google Scholar] [CrossRef] [Green Version]
- Tan, N.; Bavadian, N.; Calais, J.; Oyoyo, U.; Kim, J.; Turkbey, I.B.; Mena, E.; Davenport, M.S. Imaging of PSMA-targeted Radiotracers for the Detection of Prostate Cancer Biochemical Recurrence After Definitive Therapy: A Systematic Review and Meta-analysis. J. Urol. 2019. [Google Scholar] [CrossRef]
- Perera, M.; Papa, N.; Roberts, M.; Williams, M.; Udovicich, C.; Vela, I.; Christidis, D.; Bolton, D.; Hofman, M.S.; Lawrentschuk, N.; et al. Gallium-68 Prostate-specific Membrane Antigen Positron Emission Tomography in Advanced Prostate Cancer-Updated Diagnostic Utility, Sensitivity, Specificity, and Distribution of Prostate-specific Membrane Antigen-avid Lesions: A Systematic Review and Meta-analysis. Eur. Urol. 2019. [Google Scholar] [CrossRef]
- Pereira Mestre, R.; Treglia, G.; Ferrari, M.; Pascale, M.; Mazzara, C.; Azinwi, N.C.; Llado’, A.; Stathis, A.; Giovanella, L.; Roggero, E. Correlation between PSA kinetics and PSMA-PET in prostate cancer restaging: A meta-analysis. Eur. J. Clin. Investig. 2019, 49, e13063. [Google Scholar] [CrossRef]
- Hope, T.A.; Goodman, J.Z.; Allen, I.E.; Calais, J.; Fendler, W.P.; Carroll, P.R. Meta-analysis of (68)Ga-PSMA-11 PET Accuracy for the Detection of Prostate Cancer Validated by Histopathology. J. Nucl. Med. 2018. [Google Scholar] [CrossRef]
- Sathianathen, N.J.; Butaney, M.; Konety, B.R. The utility of PET-based imaging for prostate cancer biochemical recurrence: A systematic review and meta-analysis. World J. Urol. 2018. [Google Scholar] [CrossRef]
- Eissa, A.; Elsherbiny, A.; Coelho, R.F.; Rassweiler, J.; Davis, J.W.; Porpiglia, F.; Patel, V.R.; Prandini, N.; Micali, S.; Sighinolfi, M.C.; et al. The role of 68Ga-PSMA PET/CT scan in biochemical recurrence after primary treatment for prostate cancer: A systematic review of the literature. Minerva Urol. Nefrol. 2018, 70, 462–478. [Google Scholar] [CrossRef]
- von Eyben, F.E.; Picchio, M.; von Eyben, R.; Rhee, H.; Bauman, G. (68)Ga-Labeled Prostate-specific Membrane Antigen Ligand Positron Emission Tomography/Computed Tomography for Prostate Cancer: A Systematic Review and Meta-analysis. Eur. Urol. Focus 2018, 4, 686–693. [Google Scholar] [CrossRef]
- McInnes, M.D.F.; Moher, D.; Thombs, B.D.; McGrath, T.A.; Bossuyt, P.M.; the PRISMA-DTA Group; Clifford, T.; Cohen, J.F.; Deeks, J.J.; Gatsonis, C.; et al. Preferred Reporting Items for a Systematic Review and Meta-analysis of Diagnostic Test Accuracy Studies: The PRISMA-DTA Statement. JAMA 2018, 319, 388–396. [Google Scholar] [CrossRef]
- Sadeghi, R.; Treglia, G. Systematic reviews and meta-analyses of diagnostic studies: A practical guideline. Clin. Transl. Imaging 2017, 5, 83–87. [Google Scholar] [CrossRef]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M. QUADAS-2 Group. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Harbord, R.M.; Egger, M.; Sterne, J.A. A modified test for small-study effects in meta-analyses of controlled trials with binary endpoints. Stat. Med. 2006, 25, 3443–3457. [Google Scholar] [CrossRef]
- Dietlein, M.; Kobe, C.; Kuhnert, G.; Stockter, S.; Fischer, T.; Schomäcker, K.; Schmidt, M.; Dietlein, F.; Zlatopolskiy, B.D.; Krapf, P.; et al. Comparison of [(18)F]DCFPyL and [(68)Ga]Ga-PSMA-HBED-CC for PSMA-PET Imaging in Patients with Relapsed Prostate Cancer. Mol. Imaging Biol. 2015, 17, 575–584. [Google Scholar] [CrossRef]
- Dietlein, F.; Kobe, C.; Neubauer, S.; Schmidt, M.; Stockter, S.; Fischer, T.; Schomäcker, K.; Heidenreich, A.; Zlatopolskiy, B.D.; Neumaier, B.; et al. PSA-Stratified Performance of (18)F- and (68)Ga-PSMA PET in Patients with Biochemical Recurrence of Prostate Cancer. J. Nucl. Med. 2017, 58, 947–952. [Google Scholar] [CrossRef]
- Wondergem, M.; van der Zant, F.M.; Knol, R.J.J.; Lazarenko, S.V.; Pruim, J.; de Jong, I.J. (18)F-DCFPyL PET/CT in the Detection of Prostate Cancer at 60 and 120 Minutes: Detection Rate, Image Quality, Activity Kinetics, and Biodistribution. J. Nucl. Med. 2017, 58, 1797–1804. [Google Scholar] [CrossRef] [PubMed]
- Mena, E.; Lindenberg, M.L.; Shih, J.H.; Adler, S.; Harmon, S.; Bergvall, E.; Citrin, D.; Dahut, W.; Ton, A.T.; McKinney, Y.; et al. Clinical impact of PSMA-based (18)F-DCFBC PET/CT imaging in patients with biochemically recurrent prostate cancer after primary local therapy. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Rahbar, K.; Afshar-Oromieh, A.; Bögemann, M.; Wagner, S.; Schäfers, M.; Stegger, L.; Weckesser, M. (18)F-PSMA-1007 PET/CT at 60 and 120 minutes in patients with prostate cancer: Biodistribution, tumour detection and activity kinetics. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 1329–1334. [Google Scholar] [CrossRef] [PubMed]
- Giesel, F.L.; Will, L.; Kesch, C.; Freitag, M.; Kremer, C.; Merkle, J.; Neels, O.C.; Cardinale, J.; Hadaschik, B.; Hohenfellner, M.; et al. Biochemical Recurrence of Prostate Cancer: Initial Results with [(18)F]PSMA-1007 PET/CT. J. Nucl. Med. 2018, 59, 632–635. [Google Scholar] [CrossRef]
- Rahbar, K.; Afshar-Oromieh, A.; Seifert, R.; Wagner, S.; Schäfers, M.; Bögemann, M.; Weckesser, M. Diagnostic performance of (18)F-PSMA-1007 PET/CT in patients with biochemical recurrent prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 2055–2061. [Google Scholar] [CrossRef]
- Rousseau, E.; Wilson, D.; Lacroix-Poisson, F.; Krauze, A.; Chi, K.; Gleave, M.; McKenzie, M.; Tyldesley, S.; Goldenberg, S.L.; Bénard, F. A Prospective Study on (18)F-DCFPyL PSMA PET/CT Imaging in Biochemical Recurrence of Prostate Cancer. J. Nucl. Med. 2019. [Google Scholar] [CrossRef] [PubMed]
- Giesel, F.L.; Knorr, K.; Spohn, F.; Will, L.; Maurer, T.; Flechsig, P.; Neels, O.; Schiller, K.; Amaral, H.; Weber, W.A.; et al. Detection Efficacy of (18)F-PSMA-1007 PET/CT in 251 Patients with Biochemical Recurrence of Prostate Cancer After Radical Prostatectomy. J. Nucl. Med. 2019, 60, 362–368. [Google Scholar] [CrossRef] [PubMed]
- Han, S.; Woo, S.; Kim, Y.J.; Suh, C.H. Impact of (68)Ga-PSMA PET on the Management of Patients with Prostate Cancer: A Systematic Review and Meta-analysis. Eur. Urol. 2018, 74, 179–190. [Google Scholar] [CrossRef] [PubMed]
- Giesel, F.L.; Will, L.; Lawal, I.; Lengana, T.; Kratochwil, C.; Vorster, M.; Neels, O.; Reyneke, F.; Haberkon, U.; Kopka, K.; et al. Intraindividual Comparison of (18)F-PSMA-1007 and (18)F-DCFPyL PET/CT in the Prospective Evaluation of Patients with Newly Diagnosed Prostate Carcinoma: A Pilot Study. J. Nucl. Med. 2018, 59, 1076–1080. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | Year | Country | Study Design | Type of Patients Evaluated | No. of BRPCa Patients Performing 18F-PSMA PET/CT | Mean/Median Age (Years) | Gleason Score(Percentage) | Mean/Median PSA Values before PET/CT (ng/mL) | Mean/Median PSA Doubling Time before PET/CT (Months) |
|---|---|---|---|---|---|---|---|---|---|
| Giesel et al. [29] | 2019 | Germany and Chile | Retrospective multicentric | Patients with BRPCa previously treated with RP (100%) with or without additional RT or ADT. | 251 | Median: 70 (48–86) | ≤6: 5% 7: 50% ≥8: 34% unknown: 11% | Median: 1.2 (0.2–228) | NA |
| Rousseau et al. [28] | 2019 | Canada | Prospective single-center | Patients with BRPCa previously treated with RP (72.3%) or RT (34.6%) with or without additional ADT. | 130 | Mean: 69.1 ± 6.5 | ≤6: 13% 7: 50% ≥8: 37% | Mean: 5.2 ± 6.5 | Mean: 12.2 ± 11.8 |
| Rahbar et al. [27] | 2018 | Germany | Retrospective single-center | Patients with BRPCa previously treated with RP (92%) or RT (45%) with or without additional ADT. | 100 | Mean: 68.7 ± 7.6 Median: 70.4 (47–85) | ≤6: 6% 7: 43% ≥8: 28% unknown: 23% | Mean: 3.36 ± 6.11 Median: 1.34 (0.04–41.3) | NA |
| Giesel et al. [26] | 2018 | Germany | Retrospective single-center | Patients with BRPCa previously treated with RP (83%) or RT (67%) | 12 | Mean: 68 (54–79) | ≤6: 8% 7: 50% ≥8: 42% | Median: 0.6 (0.08–6.5) | NA |
| Rahbar et al. [25] | 2018 | Germany | Retrospective single-center | Subgroup of patients with BRPCa after primary treatment | 28 | NA | NA | NA | NA |
| Mena et al. [24] | 2018 | USA | Prospective single-center | Patients with BRPCa previously treated with RP (87%) or RT (26%) | 68 | Mean: 64 (51–74) | NA | Mean: 4.4 ± 7.3 (0.2–37.4) | Mean: 4.8 ± 3.8 |
| Wondergem et al. [23] | 2017 | Netherlands | Retrospective single-center | Subgroup of patients with BRPCa after primary treatment | 34 | NA | NA | NA | NA |
| Dietlein et al. [22] | 2017 | Germany | Retrospective single-center | Subgroup of patients with BRPCa after RP (61%) or RT (39%) | 62 | Mean: 70 | ≤6: 7% 7: 56% ≥8: 37% | Mean: 3.2 | NA |
| Dietlein et al. [21] | 2015 | Germany | Retrospective single-center | Patients with BRPCa previously treated with RP or RT | 14 | Mean: 68 | NA | NA | NA |
| Authors | Radiotracer | Hybrid Imaging Modality | Fasting before Radiotracer Injection | Mean Radiotracer Injected Activity | Time Interval between Radiotracer Injection and Image Acquisition | Image Analysis | Other Imaging Performed for Comparison |
|---|---|---|---|---|---|---|---|
| Giesel et al. [29] | 18F-PSMA-1007 | PET/CT with low-dose CT | NR | 301 ± 46 (154–453) MBq | 92 ± 26 min | visual | - |
| Rousseau et al. [28] | 18F-DCFPyL | PET/CT with low-dose CT | yes (at least 4 h) | 369.2 ± 47.2 (237–474) MBq | 120 min | visual and semi-quantitative (SUVmax, SUVpeak, SUL, TLG, SUVratio) | - |
| Rahbar et al. [27] | 18F-PSMA-1007 | PET/CT with low-dose or contrast enhanced CT | NR | 338 ± 44.31 MBq (4 MBq/kg) | 120 min | visual and semi-quantitative (SUVmax) | - |
| Giesel et al. [26] | 18F-PSMA-1007 | PET/CT with low-dose CT | NR | 251.5 (154–326) MBq | 60 + 180 min | visual and semi-quantitative (SUVmax and SUVratio) | - |
| Rahbar et al. [25] | 18F-PSMA-1007 | PET/CT with low-dose or contrast enhanced CT | NR | 336.7 ± 46 MBq (4 MBq/kg) | 60 + 120 min | visual and semi-quantitative (SUVmax) | - |
| Mena et al. [24] | 18F-DCFBC | PET/CT with low-dose CT | NR | 292.3 (255.3–299.7) MBq | 60 + 120 min | visual and semi-quantitative (SUVmax) | mpMRI |
| Wondergem et al. [23] | 18F-DCFPyL | PET/CT with contrast enhanced CT | NR | 314 (243–369) MBq | 60 + 120 min | visual and semi-quantitative (SUVmax and SUVratio) | - |
| Dietlein et al. [22] | 18F-DCFPyL | PET/CT with low-dose CT | yes (at least 4 h) | 269.8 ± 81.8 MBq | 120 min | visual and semi-quantitative (SUVmax) | 68Ga-PSMA-11 PET/CT |
| Dietlein et al. [21] | 18F-DCFPyL | PET/CT with low-dose CT | yes (at least 4 h) | 318.4 ± 59.0 MBq | 120 min | visual and semi-quantitative (SUVmax and SUVratio) | 68Ga-PSMA-11 PET/CT |
| Authors | Overall DR on a Per Patient-Based Analysis | DR in Patients with PSA < 0.5 ng/mL | DR in Patients with PSA ≥ 0.5 ng/mL | DR in Patients with PSA between 0.5 and 1 ng/mL | DR in Patients with PSA between 1 and 2 ng/mL | DR in Patients with PSA ≥ 2 ng/mL | Mean PSA in Patients with Positive PET/CT (ng/mL) | Mean PSA in Patients with Negative PET/CT (ng/mL) | Change of Management by Using PET/CT |
|---|---|---|---|---|---|---|---|---|---|
| Giesel et al. [29] | 204/251 (81.3%) | 40/65 (61.5%) | 164/186 (88.2%) | 35/47 (74.5%) | 50/55 (90.1%) | 79/84 (94%) | 6.8 ± 22.4 | 0.95 ± 1.56 | NR |
| Rousseau et al. [28] | 110/130 (84.6%) | 3/5 (60%) | 107/125 (85.6%) | 18/23 (78.3) | 18/25 (72%) | 71/77 (92.2%) | 5.8 ± 6.87 | 1.86 ± 1.62 | 87% |
| Rahbar et al. [27] | 95/100 (95%) | 18/21 (85.7%) | 77/79 (97.5%) | 16/18 (88.9%) | 22/22 (100%) | 39/39 (100%) | NR | NR | NR |
| Mena et al. [24] | 41/68 (60.3%) | 2/13 (15.4%) | 39/55(70.9%) | 6/13 (46.2%) | 10/12 (83.3%) | 23/30 (76.7%) | 6.6 ± 8.89 | 1.22 ± 1.37 | 50% |
| Wondergem et al. [23] | 28/34 (77.8%) | NR | NR | NR | NR | NR | NR | NR | NR |
| Dietlein et al. [22] | 46/62 (74.2%) | 1/8 (12.5%) | 45/54 (83.3%) | NR | NR | NR | NR | NR | NR |
| Pooled values (95% confidence interval) | 81% (71–88) | 49% (23–74) | 86% (78–93) | 73% (59–85) | 88% (73–97) | 92% (83–98) | Weighted mean PSA difference: 4.5 (3.3–5.7) | - | |
| I2 | 86% | 83% | 82% | 54% | 72% | 77% | 0% | - | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Treglia, G.; Annunziata, S.; Pizzuto, D.A.; Giovanella, L.; Prior, J.O.; Ceriani, L. Detection Rate of 18F-Labeled PSMA PET/CT in Biochemical Recurrent Prostate Cancer: A Systematic Review and a Meta-Analysis. Cancers 2019, 11, 710. https://doi.org/10.3390/cancers11050710
Treglia G, Annunziata S, Pizzuto DA, Giovanella L, Prior JO, Ceriani L. Detection Rate of 18F-Labeled PSMA PET/CT in Biochemical Recurrent Prostate Cancer: A Systematic Review and a Meta-Analysis. Cancers. 2019; 11(5):710. https://doi.org/10.3390/cancers11050710
Chicago/Turabian StyleTreglia, Giorgio, Salvatore Annunziata, Daniele A. Pizzuto, Luca Giovanella, John O. Prior, and Luca Ceriani. 2019. "Detection Rate of 18F-Labeled PSMA PET/CT in Biochemical Recurrent Prostate Cancer: A Systematic Review and a Meta-Analysis" Cancers 11, no. 5: 710. https://doi.org/10.3390/cancers11050710