Objective Patterns of Face Recognition Deficits in 165 Adults with Self-Reported Developmental Prosopagnosia

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Materials
2.2.1. Background Neuropsychological Screening
2.2.2. Face-Processing
2.3. Procedure
2.4. Statistical Analyses
3. Results
3.1. Control Performance
3.2. DPs: Initial Exclusions
3.3. Diagnosis of DP
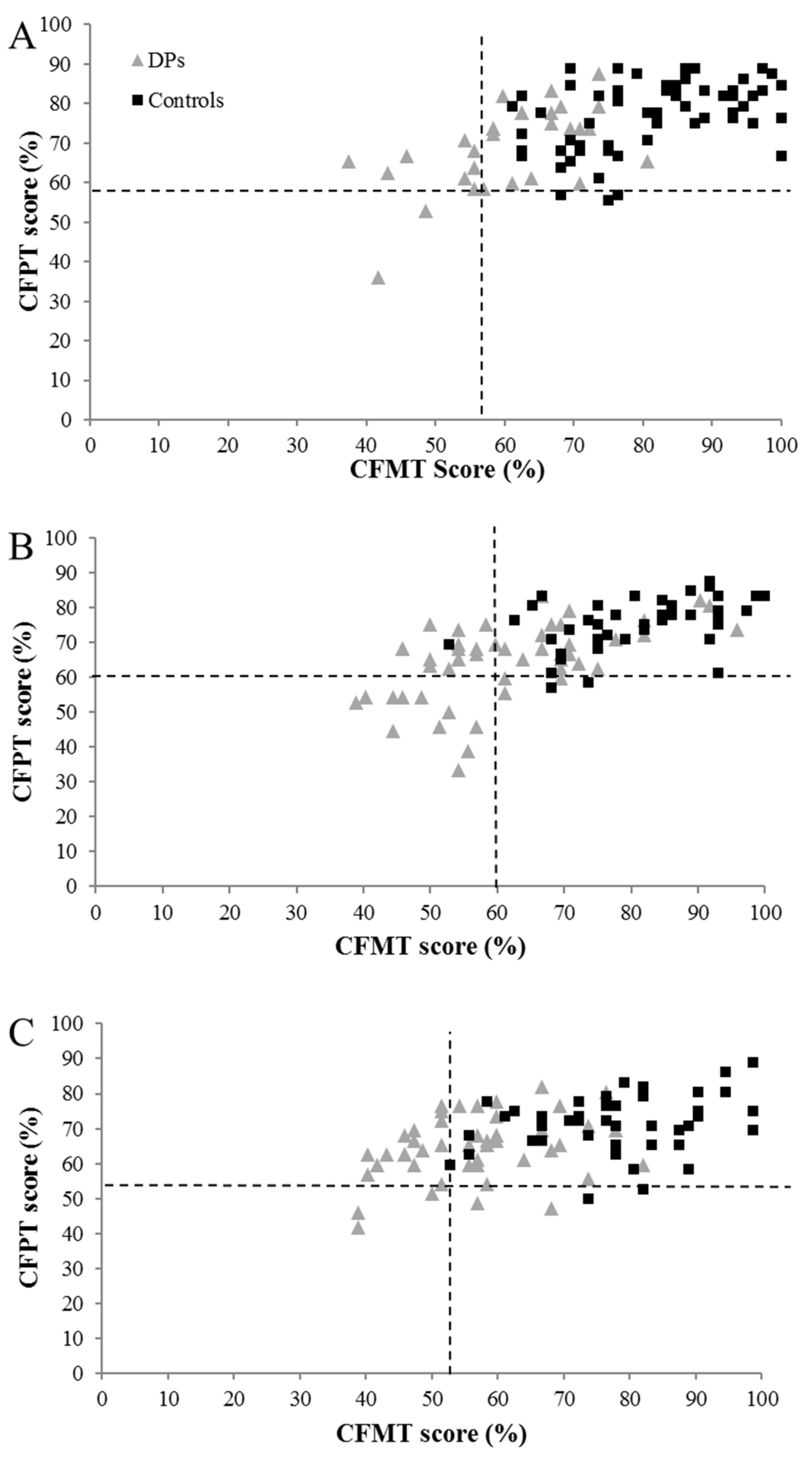
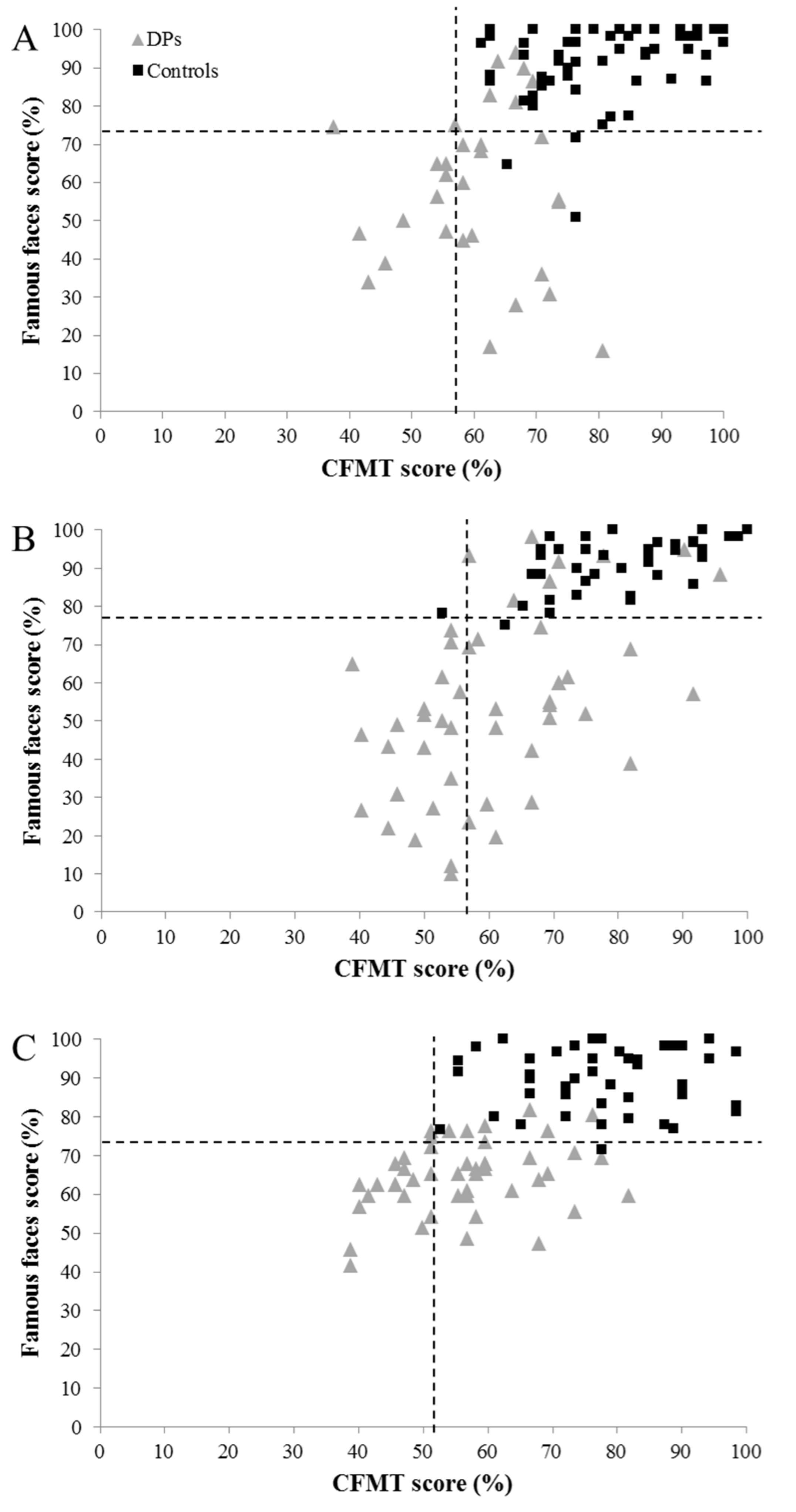
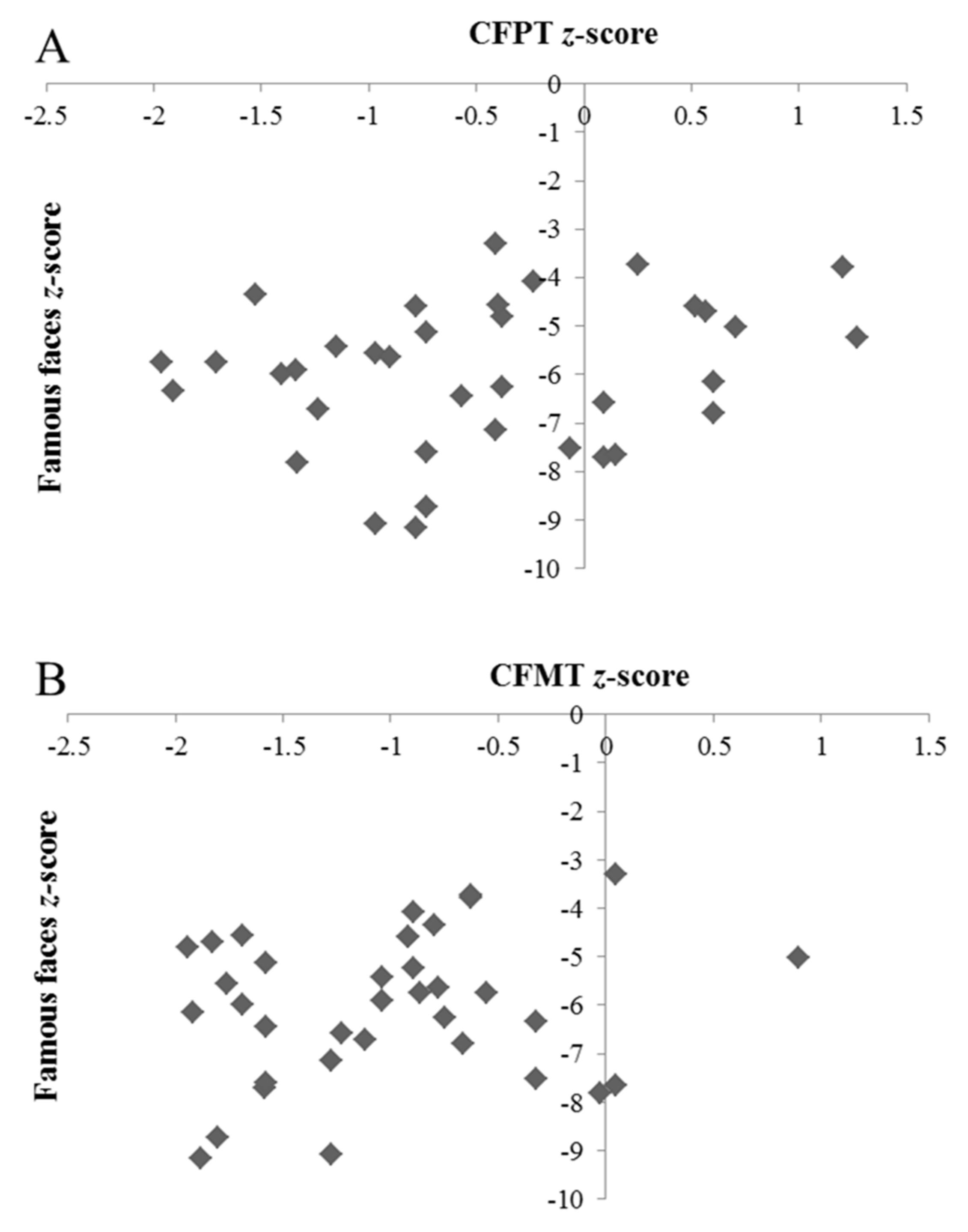
3.4. Dissociating Different Patterns of DP Presentation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Susilo, T.; Duchaine, B. Advances in developmental prosopagnosia research. Curr. Opin. Neurobiol. 2013, 23, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Bowles, D.C.; McKone, E.; Dawel, A.; Duchaine, B.; Palermo, R.; Schmalzl, L.; Rivolta, D.; Wilson, E.; Yovel, G. Diagnosing prosopagnosia: Effects of aging, sex, and participant-stimulus ethnic match on the Cambridge Face Memory Test and the Cambridge Face Perception Test. Cogn. Neuropsych. 2009, 26, 423–455. [Google Scholar] [CrossRef] [PubMed]
- Bennetts, R.J.; Murray, E.; Boyce, T.; Bate, S. Prevalence of face recognition deficits in middle childhood. Q. J. Exp. Psychol. 2017, 70, 234–258. [Google Scholar] [CrossRef] [PubMed]
- Barton, J.J.S.; Corrow, S.L. The problem of being bad at faces. Neuropsychologia 2016, 89, 119–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bate, S.; Tree, J.J. The definition and diagnosis of developmental prosopagnosia. Q. J. Exp. Psychol. 2017, 70, 193–200. [Google Scholar] [CrossRef] [PubMed]
- McConachie, H.R. Developmental prosopagnosia: A single case report. Cortex 1976, 12, 76–82. [Google Scholar] [CrossRef]
- Robotham, R.J.; Starrfelt, R. Tests of whole upright face processing in prosopagnosia: A literature review. Neuropsychologia 2018, 121, 106–121. [Google Scholar] [CrossRef] [PubMed]
- Kennerknecht, I.; Grueter, T.; Welling, B.; Wentzek, S.; Horst, J.; Edwards, S.; Grueter, M. First report of prevalence of non-syndromic hereditary prosopagnosia (HPA). Am. J. Med. Genet. 2006, 140, 1617–1622. [Google Scholar] [CrossRef]
- Shah, P.; Gaule, A.; Sowden, S.; Bird, G.; Cook, R. The 20-item prosopagnosia index (PI20): A self-report instrument for identifying developmental prosopagnosia. Roy. Soc. Open Sci. 2015, 2, 140343. [Google Scholar] [CrossRef]
- Murray, E.; Hills, P.J.; Bennetts, R.J.; Bate, S. Identifying hallmark symptoms of developmental prosopagnosia for non-experts. Sci. Rep. UK 2018, 8, 1690. [Google Scholar] [CrossRef]
- Murray, E.; Bate, S. Self-ratings of face recognition ability are influenced by gender but not prosopagnosia severity. Psychol. Assessment 2019, 31, 828–832. [Google Scholar] [CrossRef] [PubMed]
- Dalrymple, K.A.; Palermo, R. Guidelines for studying developmental prosopagnosia in adults and children. WIREs Cogn. Sci. 2016, 7, 73–87. [Google Scholar] [CrossRef] [PubMed]
- Parry, F.M.; Young, A.W.; Shona, J.; Saul, M.; Moss, A. Dissociable face processing impairments after brain injury. J. Clin. Exp. Neuropsyc. 1991, 13, 545–558. [Google Scholar] [CrossRef] [PubMed]
- Young, A.W.; Newcombe, F.; de Haan, E.H.F.; Small, M.; Hay, D.C. Face perception after brain injury. Brain 1993, 116, 941–959. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takahashi, N.; Kawamura, M.; Hirayama, K.; Shiota, J.I.; Isono, O. Prosopagnosia: A clinical and anatomical study of four patients. Cortex 1995, 31, 317–329. [Google Scholar] [CrossRef]
- Warrington, E.K. Recognition Memory Test; NFER-Nelson: Windsor, UK, 1984. [Google Scholar]
- Benton, A.L.; Sivan, A.B.; Hamsher, K.; De, S.; Varney, N.R.; Spreen, O. Contribution to Neuropsychological Assessment; Oxford University Press: New York, NY, USA, 1983. [Google Scholar]
- Burns, E.J.; Bennetts, R.J.; Bate, S.; Wright, V.C.; Weidemann, C.T.; Tree, J.J. Intact word processing in developmental prosopagnosia. Sci. Rep. UK 2017, 7, 1683. [Google Scholar] [CrossRef] [PubMed]
- Towler, J.; Fisher, K.; Eimer, M. Holistic face perception is impaired in developmental prosopagnosia. Cortex 2018, 108, 112–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duchaine, B.; Weidenfeld, A. An evaluation of two commonly used tests of unfamiliar face recognition. Neuropsychologia 2003, 41, 713–720. [Google Scholar] [CrossRef]
- Duchaine, B.; Nakayama, K. The Cambridge Face Memory Test: Results for neurologically intact individuals and an investigation of its validity using inverted face stimuli and prosopagnosic participants. Neuropsychologia 2006, 44, 576–585. [Google Scholar] [CrossRef] [PubMed]
- Duchaine, B.; Germine, L.; Nakayama, K. Family resemblance: Ten family members with prosopagnosia and within-class object agnosia. Cogn. Neuropsych. 2007, 24, 419–430. [Google Scholar] [CrossRef] [PubMed]
- Bate, S.; Bennetts, R.; Mole, J.A.; Ainge, J.A.; Gregory, N.J.; Bobak, A.K.; Bussunt, A. Rehabilitation of face-processing skills in an adolescent with prosopagnosia: Evaluation of an online perceptual training programme. Neuropsychol. Rehabil. 2015, 25, 733–762. [Google Scholar] [CrossRef] [PubMed]
- Barton, J.J.S. Structure and function in acquired prosopagnosia: Lessons from a series of 10 patients with brain damage. J. Neuropsychol. 2008, 2, 197–225. [Google Scholar] [CrossRef] [PubMed]
- Gainotti, G.; Barbier, A.; Marra, C. Slowly progressive defect in recognition of familiar people in a patient with right anterior temporal atrophy. Brain 2003, 126, 792–803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruce, V.; Young, A. Understanding face recognition. Brit. J. Psychol. 1986, 77, 305–327. [Google Scholar] [CrossRef] [PubMed]
- Haxby, J.V.; Hoffman, E.A.; Gobbini, M.I. The distributed human neural system for face perception. Trends Cogn. Sci. 2000, 4, 223–233. [Google Scholar] [CrossRef]
- De Renzi, E.; Faglioni, P.; Grossi, D.; Nichelli, P. Apperceptive and associative forms of prosopagnosia. Cortex 1991, 27, 213–221. [Google Scholar] [CrossRef]
- Barton, J.J.; Cherkasova, M.V.; Hefter, R.; Cox, T.A.; O’Connor, M.; Manoach, D.S. Are patients with social developmental disorders prosopagnosic? Perceptual heterogeneity in the Asperger and socio-emotional processing disorders. Brain 2004, 127, 1706–1716. [Google Scholar] [CrossRef] [Green Version]
- Menghini, D.; Finzi, A.; Benassi, M.; Bolzani, R.; Facoetti, A.; Giovagnoli, S.; Ruffino, M.; Vicari, S. Different underlying neurocognitive deficits in developmental dyslexia: A comparative study. Neuropsychologia 2010, 48, 863–872. [Google Scholar] [CrossRef]
- Wallace, S.; Coleman, M.; Bailey, A. Face and object processing in autism spectrum disorders. Autism Res. 2008, 1, 43–51. [Google Scholar] [CrossRef]
- Weigelt, S.; Koldewyn, K.; Dilks, D.; Balas, B.; McKone, E.; Kanwisher, N. Domain-specific development of face memory but not face perception. Dev. Sci. 2014, 17, 47–58. [Google Scholar] [CrossRef]
- Bate, S.; Bennetts, R. The independence of expression and identity in face-processing: Evidence from neuropsychological case studies. Front. Psychol. 2015, 6, 770. [Google Scholar] [CrossRef] [PubMed]
- Bate, S.; Cook, S.J. Covert recognition relies on affective valence in developmental prosopagnosia: Evidence from the skin conductance response. Neuropsychology 2012, 26, 670–674. [Google Scholar] [CrossRef] [PubMed]
- Dalrymple, K.A.; Garrido, L.; Duchaine, B. Dissociation between face perception and face memory in adults, but not children, with developmental prosopagnosia. Dev. Cogn. Neuros. Neth. 2014, 10, 10–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biotti, F.; Gray, K.L.H.; Cook, R. Is developmental prosopagnosia best characterised as an apperceptive or mnemonic condition? Neuropsychologia 2019, 124, 285–298. [Google Scholar] [CrossRef] [PubMed]
- McKone, E.; Hall, A.; Pidcock, M.; Palermo, R.; Wilkinson, R.; Rivolta, D.; O’Connor, K. Face ethnicity and measurement reliability affect face recognition performance in developmental prosopagnosia: Evidence from the Cambridge Face Memory Test—Australian. Cogn. Neuropsychol. 2011, 28, 109–146. [Google Scholar] [CrossRef] [PubMed]
- Holdnack, H.A. Wechsler Test of Adult Reading: WTAR; Psychological Corporation: San Antonio, TX, USA, 2001. [Google Scholar]
- Connolly, H.L.; Young, A.W.; Lewis, G.J. Recognition of facial expression and identity in part reflects a common ability, independent of general intelligence and visual short-term memory. Cogn. Emot. 2018, 18, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Li, J.; Fang, H.; Tian, M.; Liu, J. Individual differences in holistic processing predict face recognition ability. Psychol. Sci. 2012, 23, 169–177. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Larner, A.J. Screening utility of the Montreal Cognitive Assessment (MoCA): In place of—Or as well As–the MMSE? Int. Psychogeriatr. 2012, 24, 391–396. [Google Scholar] [CrossRef]
- Humphreys, G.; Riddoch, M.J. Birmingham Object Recognition Battery; Lawrence Erlbaum Associates: Hove, UK, 1993. [Google Scholar]
- Bobak, A.K.; Parris, B.A.; Gregory, N.J.; Bennetts, R.J.; Bate, S. Eye-movement strategies in developmental prosopagnosia and “super” face recognition. Q. J. Exp. Psychol. 2017, 70, 201–217. [Google Scholar] [CrossRef]
- Gainotti, G. Is the right anterior temporal variant of prosopagnosia a form of ‘associative prosopagnosia’ or a form of ‘multimodal person recognition disorder’? Neuropsychol. Rev. 2013, 23, 99–110. [Google Scholar] [CrossRef] [PubMed]
- Weigelt, S.; Koldewyn, K.; Kanwisher, N. Face identity recognition in autism spectrum disorders: A review of behavioral studies. Neurosci. Biobehav. Rev. 2012, 36, 1060–1084. [Google Scholar] [CrossRef] [PubMed]
- Baron-Cohen, S.; Wheelwright, S.; Skinner, R.; Martin, J.; Clubley, E. The Autism-Spectrum Quotient (AQ): Evidence from Asperger Syndrome/High-Functioning Autism, males and females, scientists and mathematicians. J. Autism Dev. Disord. 2001, 31, 5–17. [Google Scholar] [CrossRef] [PubMed]
- Avidan, G.; Tanzer, M.; Behrmann, M. Impaired holistic processing in congenital prosopagnosia. Neuropsychologia 2011, 49, 2541–2552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeGutis, J.; Cohan, S.; Mercado, R.J.; Wilmer, J.; Nakayama, K. Holistic processing of the mouth but not the eyes in developmental prosopagnosia. Cogn. Neuropsych. 2012, 29, 419–446. [Google Scholar] [CrossRef] [PubMed]
- Rezlescu, C.; Pitcher, D.; Duchaine, B. Acquired prosopagnosia with spared within-class object recognition but impaired recognition of degraded basic-level objects. Cogn. Neuropsych. 2012, 29, 325–347. [Google Scholar] [CrossRef] [PubMed]
- Wilmer, J.B.; Germine, L.; Chabris, C.F.; Chatterjee, G.; Williams, M.; Loken, E.; Nakayama, K.; Duchaine, B. Human face recognition ability is specific and highly heritable. Proc. Natl. Acad. Sci. USA 2010, 107, 5238–5241. [Google Scholar] [CrossRef] [Green Version]
- Crawford, J.R.; Howell, D.C. Comparing an individual’s test score against norms derived from small samples. Clin. Neuropsychol. 1998, 12, 482–486. [Google Scholar] [CrossRef]
- Crawford, J.R.; Garthwaite, P.H. Testing for suspected impairments and dissociations in single-case studies in neuropsychology: Evaluation of alternatives using Monte Carlo simulations and revised tests for dissociations. Neuropsychology 2005, 19, 318–331. [Google Scholar] [CrossRef]
- Gainotti, G.; Marra, C. Differential contribution of right and left temporo-occipital and anterior temporal lesions to face recognition disorders. Front. Hum. Neurosci. 2011, 5, 55. [Google Scholar] [CrossRef]
- Dobel, C.; Bölte, J.; Aicher, M.; Schweinberger, S.R. Prosopagnosia without apparent cause: Overview and diagnosis of six cases. Cortex 2007, 43, 718–733. [Google Scholar] [CrossRef]
- Bobak, A.K.; Pampoulov, P.; Bate, S. Detecting superior face recognition skills in a large sample of young British adults. Front. Psychol. 2016, 7, 1378. [Google Scholar] [CrossRef] [PubMed]
- Farah, M.J. Visual Agnosia; MIT Press: Cambridge, UK, 1990. [Google Scholar]
- Eimer, M.; Gosling, A.; Duchaine, B. Electrophysiological markers of covert face recognition in developmental prosopagnosia. Brain 2012, 135, 542–554. [Google Scholar] [CrossRef] [PubMed]
- Bate, S.; Haslam, C.; Tree, J.J.; Hodgson, T.L. Evidence of an eye-movement based memory effect in developmental prosopagnosia. Cortex 2008, 44, 806–819. [Google Scholar] [CrossRef] [PubMed]
- Rossion, B.; Michel, C. Normative accuracy and response time data for the computerized Benton Facial Recognition Test (BFRT-c). Behav. Res. Methods 2018, 50, 2442–2460. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, R.; White, D.; Van Montfort, X.; Burton, A.M. Variability in photos of the same face. Cognition 2011, 121, 313–323. [Google Scholar] [CrossRef] [PubMed]
- Arizpe, J.M.; Saad, E.; Douglas, A.O.; Germine, L.; Wilmer, J.B.; DeGutis, J.M. Self-reported face recognition is highly valid, but alone is not highly discriminative of prosopagnosia-level performance on objective assessments. Behav. Res. Methods 2019, 51, 1102–1116. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Age Group (Years) | N (% Female) | Age | IQ | CFPT | CFMT | FFT |
|---|---|---|---|---|---|---|
| 18–34 | 62 (53.2) | 24.3 (4.2) | 113.9 (8.9) | 76.95 (8.77) | 80.85 (11.57) | 91.92 (9.74) |
| 35–49 | 44 (56.8) | 42.0 (4.5) | 111.6 (8.8) | 75.28 (7.47) | 81.38 (11.52) | 92.04 (6.96) |
| 50–59 | 43 (65.1) | 54.5 (2.9) | 110.7 (9.5) | 71.38 (8.30) | 77.52 (12.17) | 89.54 (8.04) |
| 60–69 | 52 (61.5) | 64.4 (2.8) | 117.3 (8.3) | 70.33 (7.64) | 73.13 (13.56) | 88.73 (9.58) |
| 70–79 | 40 (57.5) | 73.5 (2.3) | 118.1 (7.2) | 63.33 (10.07) | 63.37 (12.51) | 75.21 (13.14) |
| Age Group | N | All | CFPT and CFMT | CFPT and FFT | CFMT and FFT | CFPT Only | CFMT Only | FFT Only | None |
|---|---|---|---|---|---|---|---|---|---|
| 18–34 | 62 | 0 | 0 | 0 | 0 | 3 | 0 | 3 | 56 |
| 35–49 | 44 | 0 | 0 | 0 | 0 | 2 | 1 | 1 | 40 |
| 50–59 | 43 | 0 | 0 | 0 | 0 | 2 | 0 | 1 | 40 |
| 60–69 | 52 | 0 | 0 | 0 | 0 | 2 | 0 | 1 | 49 |
| 70–79 | 40 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 38 |
| Total | 241 | 0 | 1 | 0 | 0 | 10 | 1 | 6 | 223 |
| Age Group | N (% Female) | All | CFPT and CFMT | CFPT and FFT | CFMT and FFT | CFPT Only | CFMT Only | FFT Only | None |
|---|---|---|---|---|---|---|---|---|---|
| 18–34 | 31 (64.5) | 3 | 1 | 0 | 6 | 0 | 1 | 14 | 6 |
| 35–49 | 51 (72.5) | 11 | 1 | 3 | 13 | 0 | 0 | 15 | 8 |
| 50–59 | 48 (68.8) | 4 | 0 | 2 | 11 | 1 | 4 | 21 | 5 |
| 60–69 | 27 (63.0) | 2 | 0 | 5 | 1 | 0 | 0 | 10 | 9 |
| 70–79 | 8 (50.0) | 0 | 0 | 0 | 0 | 0 | 0 | 3 | 5 |
| Total | 165 | 20 | 2 | 10 | 31 | 1 | 5 | 63 | 33 |
| Component | 1 | 2 |
|---|---|---|
| CFPT | 0.84 | |
| CFMT | 0.86 | |
| FFT | 0.98 |
| CFPT | CFMT | FFT | |
|---|---|---|---|
| CFPT | 1 | 0.51 * | 0.35 * |
| CFMT | 1 | 0.35 * | |
| FFT | 1 |
| Case | % Correct | CFPT v CFMT | CFPT v FFT | ||||||
|---|---|---|---|---|---|---|---|---|---|
| CFPT | CFMT | FFT | t | p | % More Extreme | t | p | % More Extreme | |
| DP032 | 68.06 | 45.83 | 30.91 | 2.04 | 0.05 | 2.37 | 5.77 | 0.001 | 0.01 |
| DP036 | 68.06 | 45.83 | 30.91 | 2.04 | 0.05 | 2.37 | 5.77 | 0.001 | 0.01 |
| DP042 | 73.61 | 54.17 | 10.00 | 2.06 | 0.05 | 2.27 | 8.50 | 0.001 | 0.01 |
| DP054 | 75.00 | 50.00 | 43.10 | 2.59 | 0.01 | 0.66 | 5.16 | 0.001 | 0.01 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bate, S.; Bennetts, R.J.; Gregory, N.; Tree, J.J.; Murray, E.; Adams, A.; Bobak, A.K.; Penton, T.; Yang, T.; Banissy, M.J. Objective Patterns of Face Recognition Deficits in 165 Adults with Self-Reported Developmental Prosopagnosia. Brain Sci. 2019, 9, 133. https://doi.org/10.3390/brainsci9060133
Bate S, Bennetts RJ, Gregory N, Tree JJ, Murray E, Adams A, Bobak AK, Penton T, Yang T, Banissy MJ. Objective Patterns of Face Recognition Deficits in 165 Adults with Self-Reported Developmental Prosopagnosia. Brain Sciences. 2019; 9(6):133. https://doi.org/10.3390/brainsci9060133
Chicago/Turabian StyleBate, Sarah, Rachel J. Bennetts, Nicola Gregory, Jeremy J. Tree, Ebony Murray, Amanda Adams, Anna K. Bobak, Tegan Penton, Tao Yang, and Michael J. Banissy. 2019. "Objective Patterns of Face Recognition Deficits in 165 Adults with Self-Reported Developmental Prosopagnosia" Brain Sciences 9, no. 6: 133. https://doi.org/10.3390/brainsci9060133