
Relationship between Sensory Alterations and Repetitive Behaviours in Children with Autism Spectrum Disorders: A Parents’ Questionnaire Based Study

 , ,
, , 
Abstract
:1. Introduction
1.1. Restricted, Repetitive Behaviours, and Interests in Autism Spectrum Disorder
1.2. Sensory Integration, Sensory Processing, and Sensory Modulation in Autism Spectrum Disorder
1.3. Objectives of the Present Study
2. Materials and Methods
2.1. Participants
2.2. Measures
2.3. Data Collection and Analysis
3. Results
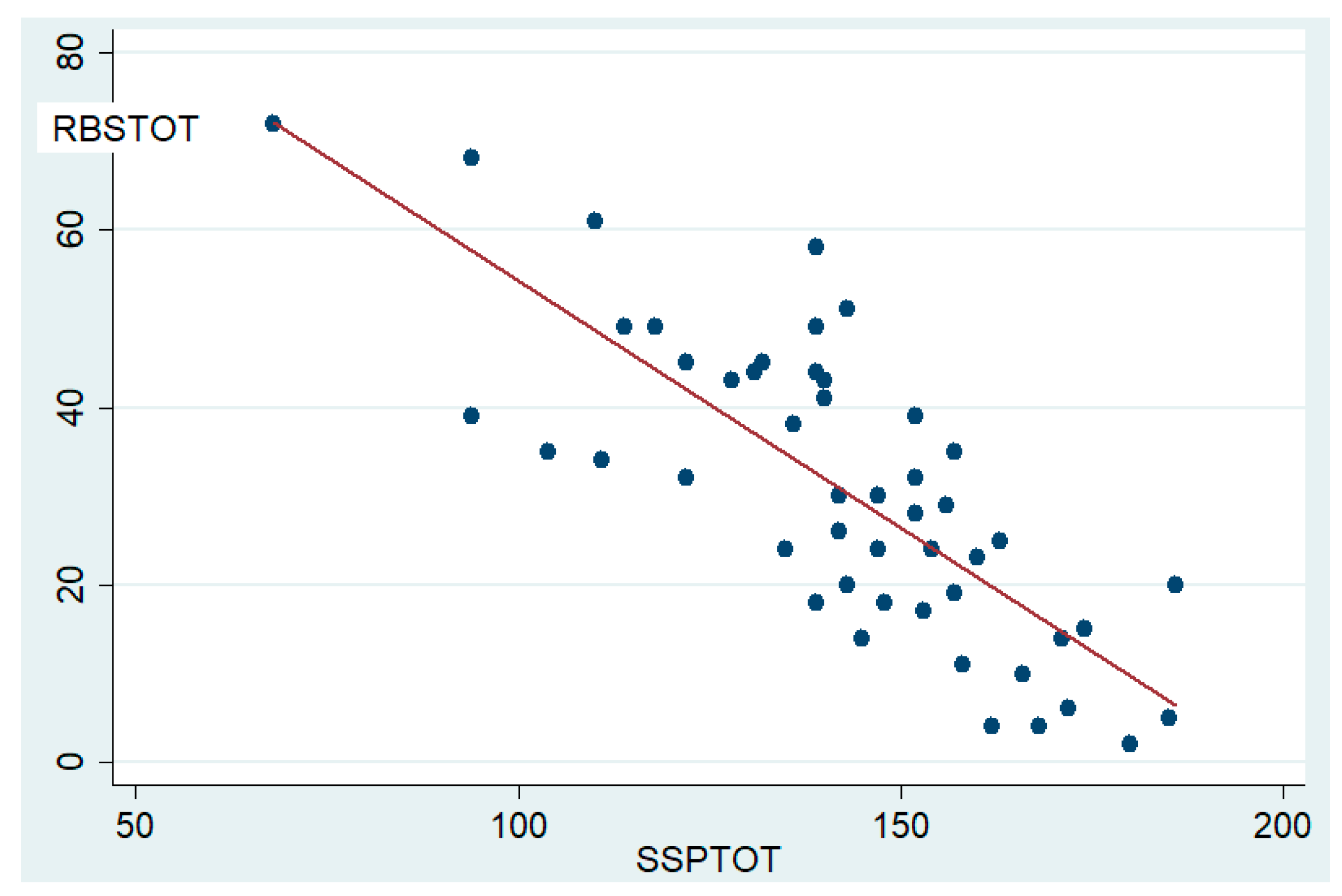
3.1. Sensory Profile, Repetitive Behaviours, and Their Mutual Correlation
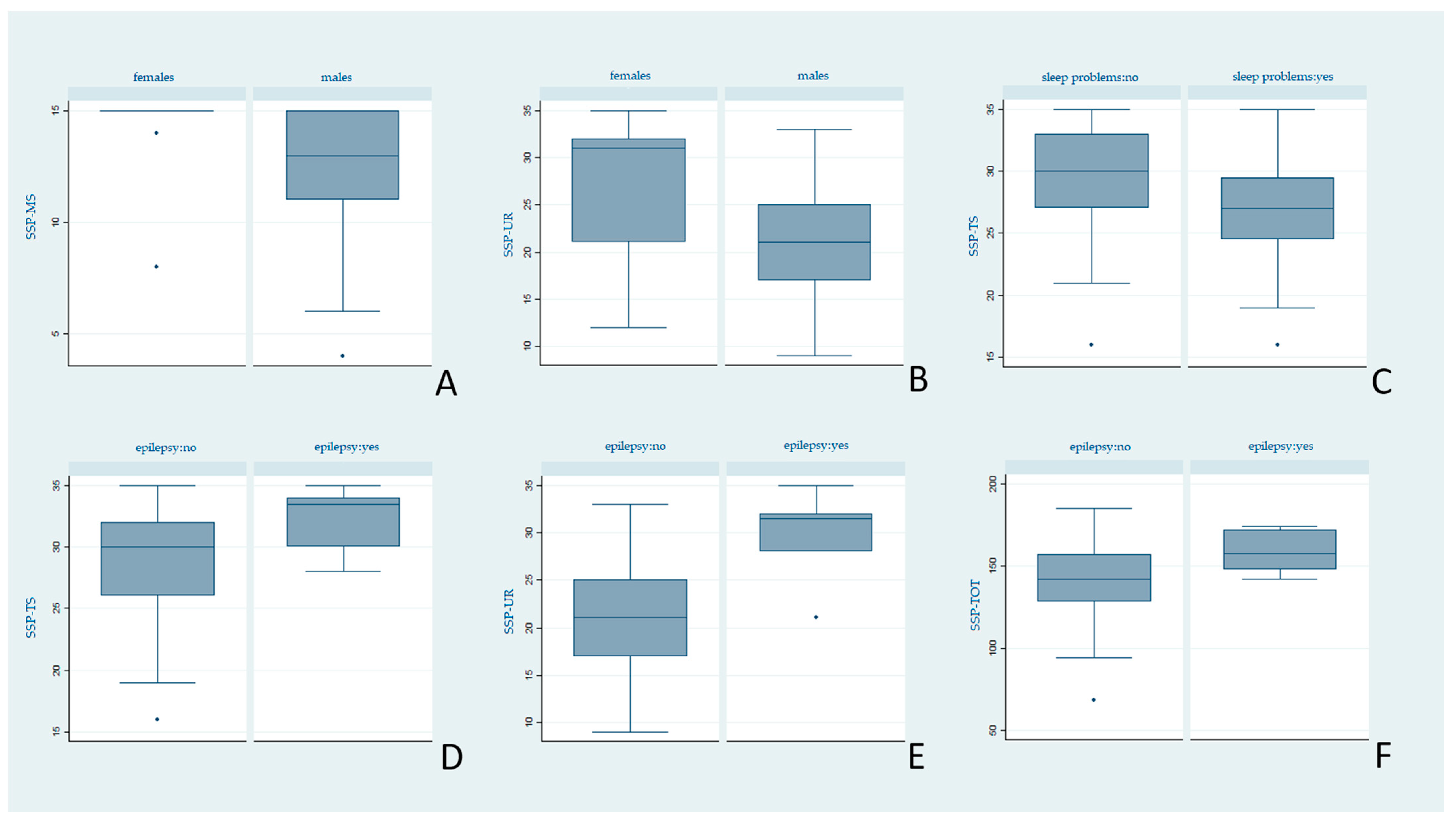
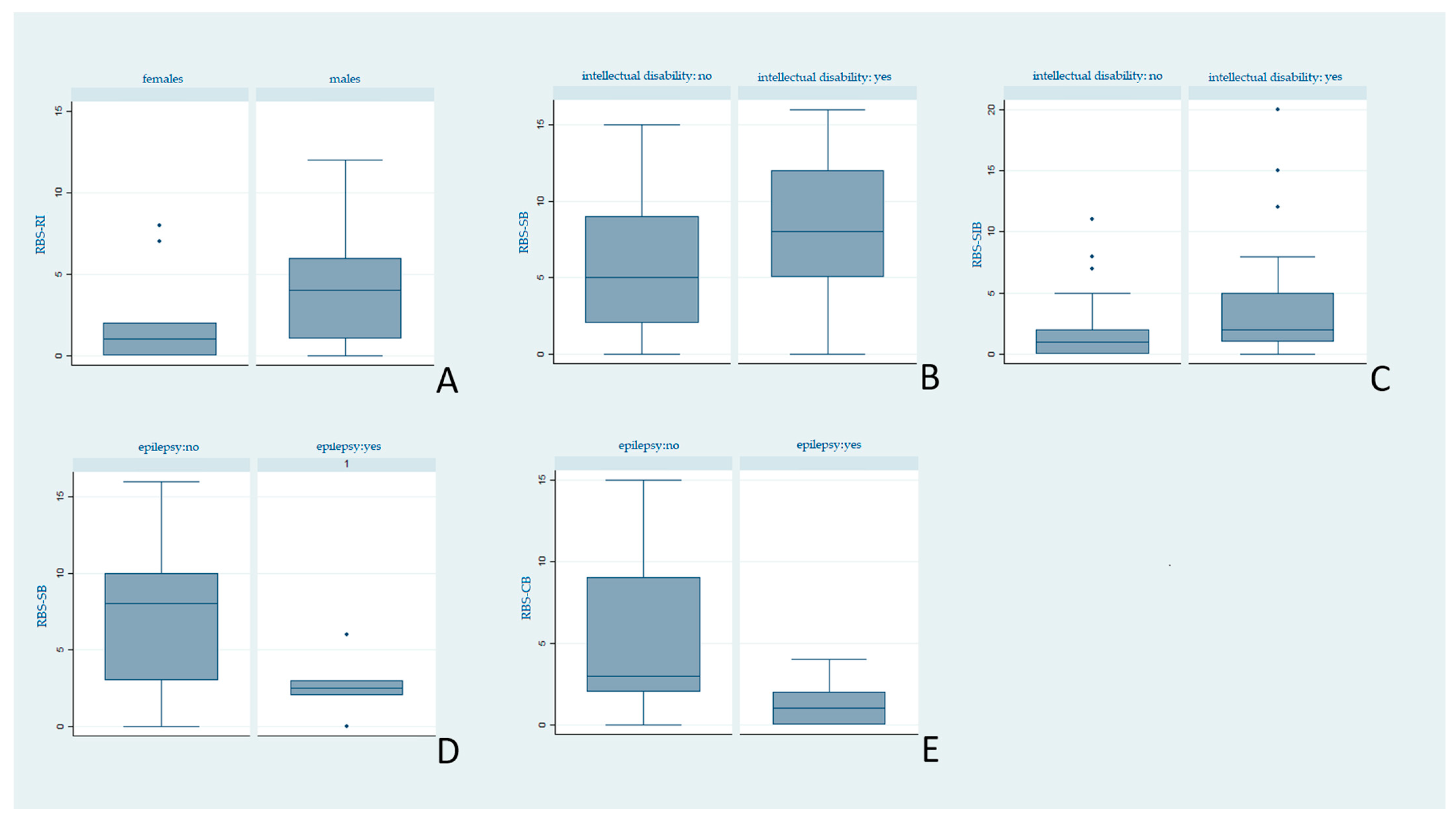
3.2. Influence of Demographic and Clinical Variables on Repetitive Behaviour and Sensory Alterations
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013; ISBN 978-0-89042-554-1.
- Lord, C.; Brugha, T.S.; Charman, T.; Cusack, J.; Dumas, G.; Frazier, T.; Jones, E.J.H.; Jones, R.M.; Pickles, A.; State, M.W.; et al. Autism Spectrum Disorder. Nat. Rev. Dis. Primers 2020, 6, 5. [Google Scholar] [CrossRef] [PubMed]
- Melo, C.; Ruano, L.; Jorge, J.; Pinto Ribeiro, T.; Oliveira, G.; Azevedo, L.; Temudo, T. Prevalence and Determinants of Motor Stereotypies in Autism Spectrum Disorder: A Systematic Review and Meta-Analysis. Autism 2019, 24, 569–590. [Google Scholar] [CrossRef]
- Posar, A.; Visconti, P. Sensory Abnormalities in Children with Autism Spectrum Disorder. J. Pediatr. 2018, 94, 342–350. [Google Scholar] [CrossRef] [PubMed]
- Thye, M.D.; Bednarz, H.M.; Herringshaw, A.J.; Sartin, E.B.; Kana, R.K. The Impact of Atypical Sensory Processing on Social Impairments in Autism Spectrum Disorder. Dev. Cogn. Neurosci. 2017, 29, 151–167. [Google Scholar] [CrossRef]
- Boyd, B.A.; McBee, M.; Holtzclaw, T.; Baranek, G.T.; Bodfish, J.W. Relationships among Repetitive Behaviors, Sensory Features, and Executive Functions in High Functioning Autism. Res. Autism Spectr. Disord. 2009, 3, 959–966. [Google Scholar] [CrossRef] [Green Version]
- Boyd, B.A.; Baranek, G.T.; Sideris, J.; Poe, M.D.; Watson, L.R.; Patten, E.; Miller, H. Sensory Features and Repetitive Behaviors in Children with Autism and Developmental Delays. Autism Res. 2010, 3, 78–87. [Google Scholar] [CrossRef] [PubMed]
- Goodall, J.E. Corbett Relationships Between Sensory Stimulation and Stereotyped Behaviour in Severely Mentally Retarded and Autistic Children. J. Intellect. Disabil. Res. 1982, 26, 163–175. [Google Scholar] [CrossRef]
- Gabriels, R.L.; Agnew, J.A.; Miller, L.J.; Gralla, J.; Pan, Z.; Goldson, E.; Ledbetter, J.C.; Dinkins, J.P.; Hooks, E. Is There a Relationship between Restricted, Repetitive, Stereotyped Behaviors and Interests and Abnormal Sensory Response in Children with Autism Spectrum Disorders? Res. Autism Spectr. Disord. 2008, 2, 660–670. [Google Scholar] [CrossRef]
- Gal, E.; Dyck, M.J.; Passmore, A. Relationships Between Stereotyped Movements and Sensory Processing Disorders in Children With and Without Developmental or Sensory Disorders. Am. J. Occup. Ther. 2010, 64, 453–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hutt, C.; Hutt, S.J. Effects of Environmental Complexity on Stereotyped Behaviours of Children. Anim. Behav. 1965, 13, 1–4. [Google Scholar] [CrossRef]
- Kirby, A.V.; Boyd, B.A.; Williams, K.L.; Faldowski, R.A.; Baranek, G.T. Sensory and Repetitive Behaviors among Children with Autism Spectrum Disorder at Home. Autism 2017, 21, 142–154. [Google Scholar] [CrossRef] [Green Version]
- Schulz, S.E.; Stevenson, R.A. Sensory Hypersensitivity Predicts Repetitive Behaviours in Autistic and Typically-Developing Children. Autism 2019, 23, 1028–1041. [Google Scholar] [CrossRef] [PubMed]
- Ausderau, K.; Sideris, J.; Furlong, M.; Little, L.M.; Bulluck, J.; Baranek, G.T. National Survey of Sensory Features in Children with ASD: Factor Structure of the Sensory Experience Questionnaire (3.0). J. Autism Dev. Disord. 2014, 44, 915–925. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liss, M.; Saulnier, C.; Fein, D.; Kinsbourne, M. Sensory and Attention Abnormalities in Autistic Spectrum Disorders. Autism 2006, 10, 155–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ben-Sasson, A.; Hen, L.; Fluss, R.; Cermak, S.A.; Engel-Yeger, B.; Gal, E. A Meta-Analysis of Sensory Modulation Symptoms in Individuals with Autism Spectrum Disorders. J. Autism Dev. Disord. 2009, 39, 1–11. [Google Scholar] [CrossRef]
- Gal, E.; Dyck, M.; Passmore, A. Sensory Differences and Stereotyped Movements in Children with Autism. Behav. Change 2002, 19, 207–219. [Google Scholar] [CrossRef] [Green Version]
- Ventola, P.E.; Yang, D.; Abdullahi, S.M.; Paisley, C.A.; Braconnier, M.L.; Sukhodolsky, D.G. Brief Report: Reduced Restricted and Repetitive Behaviors after Pivotal Response Treatment. J. Autism Dev. Disord. 2016, 46, 2813–2820. [Google Scholar] [CrossRef] [Green Version]
- Lam, K.S.L.; Aman, M.G. The Repetitive Behavior Scale-Revised: Independent Validation in Individuals with Autism Spectrum Disorders. J. Autism Dev. Disord. 2007, 37, 855–866. [Google Scholar] [CrossRef]
- Baum, S.H.; Stevenson, R.A.; Wallace, M.T. Behavioral, Perceptual, and Neural Alterations in Sensory and Multisensory Function in Autism Spectrum Disorder. Prog. Neurobiol. 2015, 134, 140–160. [Google Scholar] [CrossRef] [Green Version]
- Robertson, C.E.; Baron-Cohen, S. Sensory Perception in Autism. Nat. Rev. Neurosci. 2017, 18, 671–684. [Google Scholar] [CrossRef]
- Turner-Brown, L.M.; Baranek, G.T.; Reznick, J.S.; Watson, L.R.; Crais, E.R. The First Year Inventory: A Longitudinal Follow-up of 12-Month-Old to 3-Year-Old Children. Autism 2013, 17, 527–540. [Google Scholar] [CrossRef] [Green Version]
- Donaldson, C.K.; Stauder, J.E.A.; Donkers, F.C.L. Increased Sensory Processing Atypicalities in Parents of Multiplex ASD Families Versus Typically Developing and Simplex ASD Families. J. Autism Dev. Disord. 2017, 47, 535–548. [Google Scholar] [CrossRef] [Green Version]
- Ayres, A.J.; Robbins, J. Sensory Integration and the Child; Western Psychological Services: Los Angeles, CA, USA, 1979. [Google Scholar]
- Koziol, L.F.; Budding, D.E.; Chidekel, D. Sensory Integration, Sensory Processing, and Sensory Modulation Disorders: Putative Functional Neuroanatomic Underpinnings. Cerebellum 2011, 10, 770–792. [Google Scholar] [CrossRef] [PubMed]
- Pastor-Cerezuela, G.; Fernández-Andrés, M.-I.; Sanz-Cervera, P.; Marín-Suelves, D. The Impact of Sensory Processing on Executive and Cognitive Functions in Children with Autism Spectrum Disorder in the School Context. Res. Dev. Disabil. 2020, 96, 103540. [Google Scholar] [CrossRef]
- Dunn, W. The Impact of Sensory Processing Abilities on the Daily Lives of Young Children and Their Families: A Conceptual Model. Infants Young Child. 1997, 9, 23–35. [Google Scholar] [CrossRef]
- Miller, L.J.; Anzalone, M.E.; Lane, S.J.; Cermak, S.A.; Osten, E.T. Concept Evolution in Sensory Integration: A Proposed Nosology for Diagnosis. Am. J. Occup. Ther. 2007, 61, 135–140. [Google Scholar] [CrossRef] [Green Version]
- Miller, L.; Anzalone, M.; Cermak, S.; Lane, S.; Osten, B.; Wieder, S.; Greenspan, S. Diagnostic Manual for Infancy and Early Childhood; Interdisciplinary Council on Developmental and Learning Disorders: Bethesda, MD, USA, 2005. [Google Scholar]
- World Health Organisation International Classification of Disease, 10th ed.; World Health Organisation: Geneva, Switzerland, 1990.
- Kilroy, E.; Aziz-Zadeh, L.; Cermak, S. Ayres Theories of Autism and Sensory Integration Revisited: What Contemporary Neuroscience Has to Say. Brain Sci. 2019, 9, 68. [Google Scholar] [CrossRef] [Green Version]
- Baker, A.E.Z.; Lane, A.; Angley, M.T.; Young, R.L. The Relationship Between Sensory Processing Patterns and Behavioural Responsiveness in Autistic Disorder: A Pilot Study. J. Autism Dev. Disord. 2008, 38, 867–875. [Google Scholar] [CrossRef]
- Baranek, G.T.; David, F.J.; Poe, M.D.; Stone, W.L.; Watson, L.R. Sensory Experiences Questionnaire: Discriminating Sensory Features in Young Children with Autism, Developmental Delays, and Typical Development. J. Child Psychol. Psychiatry 2006, 47, 591–601. [Google Scholar] [CrossRef] [PubMed]
- Kay, S. Relationship between Sensory Processing and Self Care for Children with Autism Ages Two to Four. Ph.D. Thesis, Nova Southeastern University, Fort Lauderdale, FL, USA, 2001. [Google Scholar]
- Lane, A.E.; Molloy, C.A.; Bishop, S.L. Classification of Children With Autism Spectrum Disorder by Sensory Subtype: A Case for Sensory-Based Phenotypes. Autism Res. 2014, 7, 322–333. [Google Scholar] [CrossRef]
- Lord, C.; Rutter, M.; DiLavore, P.; Risi, S.; Gotham, K.; Bishop, S. (ADOS-2) Autism Diagnostic Observation Schedule, 2nd ed.; Western Psychological Corporation: Los Angeles, CA, USA, 2012; p. 284. [Google Scholar]
- Fisher, R.S.; Acevedo, C.; Arzimanoglou, A.; Bogacz, A.; Cross, J.H.; Elger, C.E.; Engel, J.; Forsgren, L.; French, J.A.; Glynn, M.; et al. ILAE Official Report: A Practical Clinical Definition of Epilepsy. Epilepsia 2014, 55, 475–482. [Google Scholar] [CrossRef] [Green Version]
- International Classification of Sleep Disorders. Diagnostic and Coding Manual, 2nd ed.; American Academy of Sleep Medicine: Westchester, IL, USA, 2005. [Google Scholar]
- Ophoff, D.; Slaats, M.A.; Boudewyns, A.; Glazemakers, I.; Van Hoorenbeeck, K.; Verhulst, S.L. Sleep Disorders during Childhood: A Practical Review. Eur. J. Pediatr. 2018, 177, 641–648. [Google Scholar] [CrossRef] [PubMed]
- McIntosh, D.N.; Miller, L.J.; Shyu, V. Development and Validation of the Short Sensory Profile. In Sensory Profile: User’s Manual; Dunn, W., Ed.; The Pscyhological: San Antonio, TX, USA, 1999; pp. 59–73. [Google Scholar]
- Bodfish, J.W.; Symons, F.W.; Lewis, M.H. The Repetitive Behavior Scale; Western Carolina Center Research Reports; Western Carolina Center: Morganton, NC, USA, 1999. [Google Scholar]
- Chen, Y.-H.; Rodgers, J.; McConachie, H. Restricted and Repetitive Behaviours, Sensory Processing and Cognitive Style in Children with Autism Spectrum Disorders. J. Autism Dev. Disord. 2009, 39, 635–642. [Google Scholar] [CrossRef]
- Jussila, K.; Junttila, M.; Kielinen, M.; Ebeling, H.; Joskitt, L.; Moilanen, I.; Mattila, M.-L. Sensory Abnormality and Quantitative Autism Traits in Children With and Without Autism Spectrum Disorder in an Epidemiological Population. J. Autism Dev. Disord. 2020, 50, 180–188. [Google Scholar] [CrossRef] [Green Version]
- Schulz, S.E.; Stevenson, R.A. Differentiating between Sensory Sensitivity and Sensory Reactivity in Relation to Restricted Interests and Repetitive Behaviours. Autism 2020, 24, 121–134. [Google Scholar] [CrossRef] [PubMed]
- Loh, A.; Soman, T.; Brian, J.; Bryson, S.E.; Roberts, W.; Szatmari, P.; Smith, I.M.; Zwaigenbaum, L. Stereotyped Motor Behaviors Associated with Autism in High-Risk Infants: A Pilot Videotape Analysis of a Sibling Sample. J. Autism Dev. Disord. 2007, 37, 25–36. [Google Scholar] [CrossRef]
- Goldman, S.; Wang, C.; Salgado, M.W.; Greene, P.E.; Kim, M.; Rapin, I. Motor Stereotypies in Children with Autism and Other Developmental Disorders. Dev. Med. Child Neurol. 2009, 51, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Baranek, G.T.; Foster, L.G.; Berkson, G. Tactile Defensiveness and Stereotyped Behaviors. Am. J. Occup. Ther. 1997, 51, 91–95. [Google Scholar] [CrossRef] [Green Version]
- Rapoport, J.L.; Inoff-Germain, G. Practitioner Review: Treatment of Obsessive-Compulsive Disorder in Children and Adolescents. J. Child Psychol. Psychiatry 2000, 41, 419–431. [Google Scholar] [CrossRef]
- Wigham, S.; Rodgers, J.; South, M.; McConachie, H.; Freeston, M. The Interplay Between Sensory Processing Abnormalities, Intolerance of Uncertainty, Anxiety and Restricted and Repetitive Behaviours in Autism Spectrum Disorder. J. Autism Dev. Disord. 2015, 45, 943–952. [Google Scholar] [CrossRef]
- Green, S.A.; Rudie, J.D.; Colich, N.L.; Wood, J.J.; Shirinyan, D.; Hernandez, L.; Tottenham, N.; Dapretto, M.; Bookheimer, S.Y. Overreactive Brain Responses to Sensory Stimuli in Youth With Autism Spectrum Disorders. J. Am. Acad. Child Adolesc. Psychiatry 2013, 52, 1158–1172. [Google Scholar] [CrossRef] [Green Version]
- Lee, P.S.; Foss-Feig, J.; Henderson, J.G.; Kenworthy, L.E.; Gilotty, L.; Gaillard, W.D.; Vaidya, C.J. Atypical Neural Substrates of Embedded Figures Task Performance in Children with Autism Spectrum Disorder. NeuroImage 2007, 38, 184–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leekam, S.R.; Nieto, C.; Libby, S.J.; Wing, L.; Gould, J. Describing the Sensory Abnormalities of Children and Adults with Autism. J. Autism Dev. Disord. 2007, 37, 894–910. [Google Scholar] [CrossRef]
- Cunningham, A.B.; Schreibman, L. Stereotypy in Autism: The Importance of Function. Res. Autism Spectr. Disord. 2008, 2, 469–479. [Google Scholar] [CrossRef] [Green Version]
- Lovaas, I.; Newsom, C.; Hickman, C. Self-Stimulatory Behavior and Perceptual Reinforcement. J. Appl. Behav. Anal. 1987, 20, 45–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fulceri, F.; Narzisi, A.; Apicella, F.; Balboni, G.; Baldini, S.; Brocchini, J.; Domenici, I.; Cerullo, S.; Igliozzi, R.; Cosenza, A.; et al. Application of the Repetitive Behavior Scale-Revised—Italian Version—in Preschoolers with Autism Spectrum Disorder. Res. Dev. Disabil. 2016, 48, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Green, R.M.; Travers, A.M.; Howe, Y.; McDougle, C.J. Women and Autism Spectrum Disorder: Diagnosis and Implications for Treatment of Adolescents and Adults. Curr. Psychiatry Rep. 2019, 21, 22. [Google Scholar] [CrossRef]
- Young, H.; Oreve, M.-J.; Speranza, M. Clinical Characteristics and Problems Diagnosing Autism Spectrum Disorder in Girls. Archives Pédiatrie 2018, 25, 399–403. [Google Scholar] [CrossRef]
- Baghdadli, A.; Pascal, C.; Grisi, S.; Aussilloux, C. Risk Factors for Self-Injurious Behaviours among 222 Young Children with Autistic Disorders. J. Intellect. Disabil. Res. 2003, 47, 622–627. [Google Scholar] [CrossRef]
- Shattuck, P.T.; Seltzer, M.M.; Greenberg, J.S.; Orsmond, G.I.; Bolt, D.; Kring, S.; Lounds, J.; Lord, C. Change in Autism Symptoms and Maladaptive Behaviors in Adolescents and Adults with an Autism Spectrum Disorder. J. Autism Dev. Disord. 2007, 37, 1735–1747. [Google Scholar] [CrossRef] [Green Version]
- Symons, F.J.; Sperry, L.A.; Dropik, P.L.; Bodfish, J.W. The Early Development of Stereotypy and Self-Injury: A Review of Research Methods. J. Intellect. Disabil. Res. 2005, 49, 144–158. [Google Scholar] [CrossRef] [PubMed]
- Matson, J.L.; Rivet, T.T. Characteristics of Challenging Behaviours in Adults with Autistic Disorder, PDD-NOS, and Intellectual Disability. J. Intellect. Dev. Disabil. 2008, 33, 323–329. [Google Scholar] [CrossRef] [PubMed]
- Richards, C.; Oliver, C.; Nelson, L.; Moss, J. Self-Injurious Behaviour in Individuals with Autism Spectrum Disorder and Intellectual Disability. J. Intellect. Disabil. Res. 2012, 56, 476–489. [Google Scholar] [CrossRef] [Green Version]
- Nigg, J.T. Neuropsychologic Theory and Findings in Attention-Deficit/Hyperactivity Disorder: The State of the Field and Salient Challenges for the Coming Decade. Biol. Psychiatry 2005, 57, 1424–1435. [Google Scholar] [CrossRef]
- Sonuga-Barke, E.J.S. Psychological Heterogeneity in AD/HD—A Dual Pathway Model of Behaviour and Cognition. Behav. Brain Res. 2002, 130, 29–36. [Google Scholar] [CrossRef]
- Oliver, C.; Licence, L.; Richards, C. Self-Injurious Behaviour in People with Intellectual Disability and Autism Spectrum Disorder. Curr. Opin. Psychiatry 2017, 30, 97–101. [Google Scholar] [CrossRef]
- Tzischinsky, O.; Meiri, G.; Manelis, L.; Bar-Sinai, A.; Flusser, H.; Michaelovski, A.; Zivan, O.; Ilan, M.; Faroy, M.; Menashe, I.; et al. Sleep Disturbances Are Associated with Specific Sensory Sensitivities in Children with Autism. Mol. Autism 2018, 9. [Google Scholar] [CrossRef] [Green Version]
- Chahin, S.S.; Apple, R.W.; Kuo, K.H.; Dickson, C.A. Autism Spectrum Disorder: Psychological and Functional Assessment, and Behavioral Treatment Approaches. Transl. Pediatr. 2020, 9, S66–S75. [Google Scholar] [CrossRef] [PubMed]
- Papavasiliou, A.S.; Nikaina, I.; Rizou, J.; Alexandrou, S. The Effect of a Psycho-Educational Program on CARS Scores and Short Sensory Profile in Autistic Children. Eur. J. Paediatr. Neurol. 2011, 15, 338–344. [Google Scholar] [CrossRef]
- Lewis, M.L.; Kesler, M.; Candy, S.A.; Rho, J.M.; Pittman, Q.J. Comorbid Epilepsy in Autism Spectrum Disorder: Implications of Postnatal Inflammation for Brain Excitability. Epilepsia 2018, 59, 1316–1326. [Google Scholar] [CrossRef] [Green Version]
- Van Campen, J.S.; Jansen, F.E.; Kleinrensink, N.J.; Joëls, M.; Braun, K.P.; Bruining, H. Sensory Modulation Disorders in Childhood Epilepsy. J. Neurodev. Disord. 2015, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mulligan, C.K.; Trauner, D.A. Incidence and Behavioral Correlates of Epileptiform Abnormalities in Autism Spectrum Disorders. J. Autism Dev. Disord. 2014, 44, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Takarae, Y.; Sweeney, J. Neural Hyperexcitability in Autism Spectrum Disorders. Brain Sci. 2017, 7, 129. [Google Scholar] [CrossRef] [PubMed]
- Hollander, E.; Chaplin, W.; Soorya, L.; Wasserman, S.; Novotny, S.; Rusoff, J.; Feirsen, N.; Pepa, L.; Anagnostou, E. Divalproex Sodium vs Placebo for the Treatment of Irritability in Children and Adolescents with Autism Spectrum Disorders. Neuropsychopharmacology 2010, 35, 990–998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aman, M.G.; Singh, N.N.; Stewart, A.W.; Field, C.J. The Aberrant Behavior Checklist: A Behavior Rating Scale for the Assessment of Treatment Effects. Am. J. Ment. Defic. 1985, 89, 485–491. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Variable (Sample Size) | N (%) | |
|---|---|---|
| Gender (50) | Female | 11 (22%) |
| Male | 39 (78%) | |
| ADOS-2: level of autism-related symptoms (50) | Low | 18 (36%) |
| Moderate | 22 (44%) | |
| High | 10 (20%) | |
| MRI (40) | Normal | 36 (90%) |
| Nonspecific structural alterations | 4 (10%) | |
| Epilepsy (49) | Yes | 43 (88%) |
| No | 6 (12%) | |
| Intellectual Disability (49) | Yes | 31 (63%) |
| No | 18 (37%) | |
| Sleep disorders (48) | Yes | 36 (75%) |
| No | 12 (25%) | |
| Rehabilitation therapy (48) | Yes | 12 (25%) |
| No | 36 (75%) |
| SSP Subscales | Mean (SD) |
|---|---|
| Tactile Sensitivity | 29.0 (4.7) |
| Taste/Smell Sensitivity | 14.0 (5.0) |
| Movement Sensitivity | 13.0 (2.6) |
| Under-Responsive/Seek Sensation | 22.6 (6.6) |
| Auditory Filtering | 20.0 (5.5) |
| Low Energy/Weak | 25.6 (5.6) |
| Visual/Auditory Sensitivity | 18.7 (4.4) |
| Total | 143 (24.0) |
| RBS-R Subscales | Mean (SD) |
|---|---|
| Stereotyped Behaviour | 6.4 (4.4) |
| Self-injurious Behaviour | 2.9 (4.0) |
| Compulsive Behaviour | 4.7 (4.4) |
| Ritualistic Behaviour | 4.6 (3.3) |
| Sameness Behaviour | 8.0 (5.7) |
| Restricted Interests | 3.8 (3.3) |
| Total | 30.3 (17.0) |
| RBS−SB | RBS−SIB | RBS−CB | RBS−RB | RBS−SAB | RBS−RI | RBS−TOT | |
|---|---|---|---|---|---|---|---|
| SSP−TS | −0.39 | −0.37 | −0.50 * | −0.34 | −0.53 * | −0.54 * | −0.58 * |
| SSP−TSS | −0.27 | −0.17 | −0.32 | −0.39 | −0.26 | −0.39 | −0.39 |
| SSP−MS | 0.02 | −0.19 | −0.04 | −0.28 | −0.34 | −0.38 | −0.28 |
| SSP−UR | −0.64 * | −0.39 | −0.46 | −0.21 | −0.41 | −0.50 * | −0.61 * |
| SSP−AF | −0.37 | −0.38 | −0.35 | −0.24 | −0.54 * | −0.46 | −0.54 * |
| SSP−LE | −0.10 | −0.01 | −0.11 | −0.24 | −0.37 | −0.43 | −0.27 |
| SSP−VA | −0.61 * | −0.44 | −0.53 * | −0.35 | −0.65 * | −0.47 | −0.79 * |
| SSP−TOT | −0.59 * | −0.40 | −0.59 * | −0.44 | −0.70 * | −0.70 * | −0.80 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fetta, A.; Carati, E.; Moneti, L.; Pignataro, V.; Angotti, M.; Bardasi, M.C.; Cordelli, D.M.; Franzoni, E.; Parmeggiani, A. Relationship between Sensory Alterations and Repetitive Behaviours in Children with Autism Spectrum Disorders: A Parents’ Questionnaire Based Study. Brain Sci. 2021, 11, 484. https://doi.org/10.3390/brainsci11040484
Fetta A, Carati E, Moneti L, Pignataro V, Angotti M, Bardasi MC, Cordelli DM, Franzoni E, Parmeggiani A. Relationship between Sensory Alterations and Repetitive Behaviours in Children with Autism Spectrum Disorders: A Parents’ Questionnaire Based Study. Brain Sciences. 2021; 11(4):484. https://doi.org/10.3390/brainsci11040484
Chicago/Turabian StyleFetta, Anna, Elisa Carati, Laura Moneti, Veronica Pignataro, Marida Angotti, Maria Chiara Bardasi, Duccio Maria Cordelli, Emilio Franzoni, and Antonia Parmeggiani. 2021. "Relationship between Sensory Alterations and Repetitive Behaviours in Children with Autism Spectrum Disorders: A Parents’ Questionnaire Based Study" Brain Sciences 11, no. 4: 484. https://doi.org/10.3390/brainsci11040484