The Role of Executive Functions in the Development of Empathy and Its Association with Externalizing Behaviors in Children with Neurodevelopmental Disorders and Other Psychiatric Comorbidities

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Participants and Diagnostic Procedures
2.2. Clinical Assessment
2.3. Data Analysis
3. Results
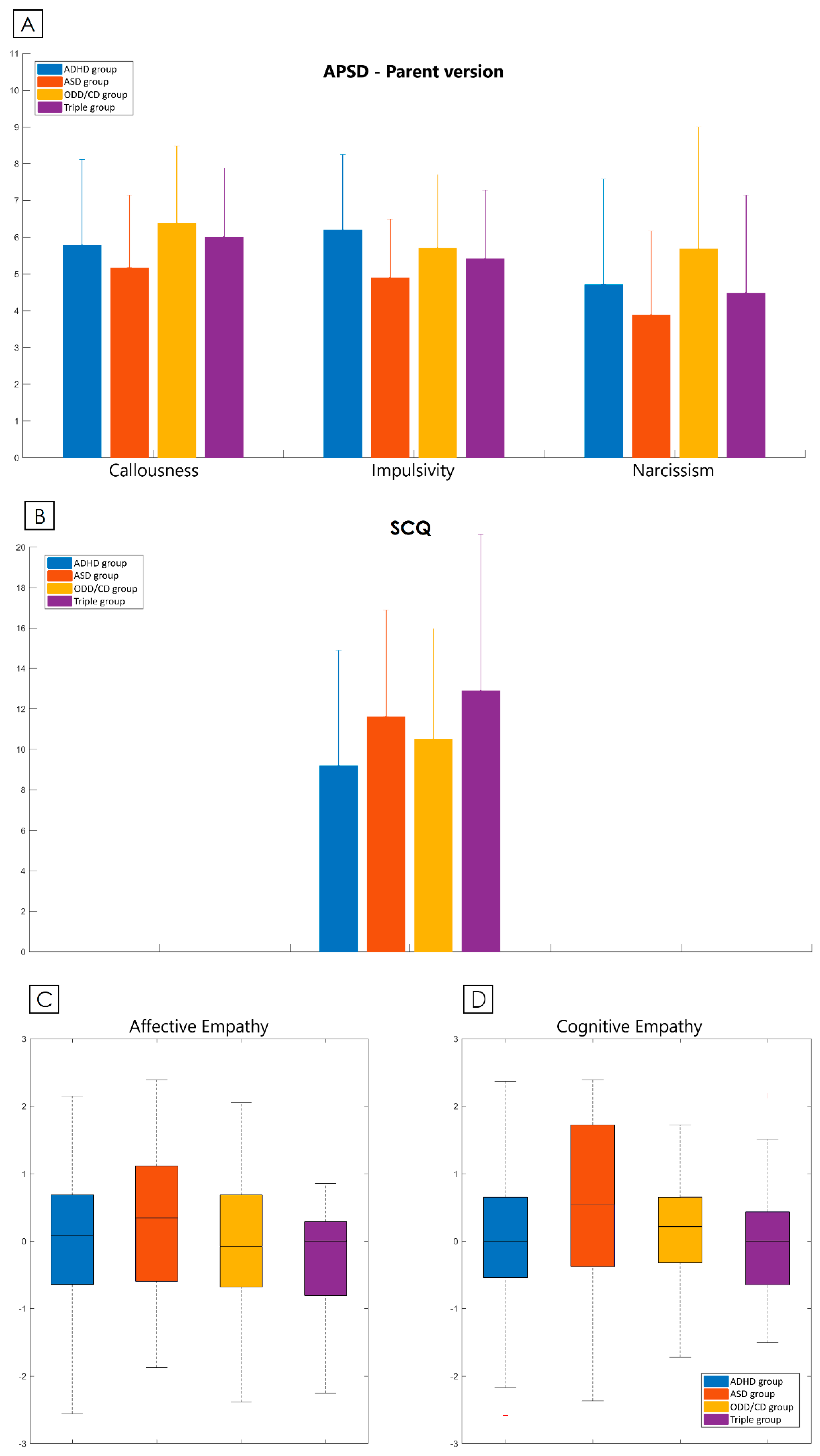
3.1. Questionnaires
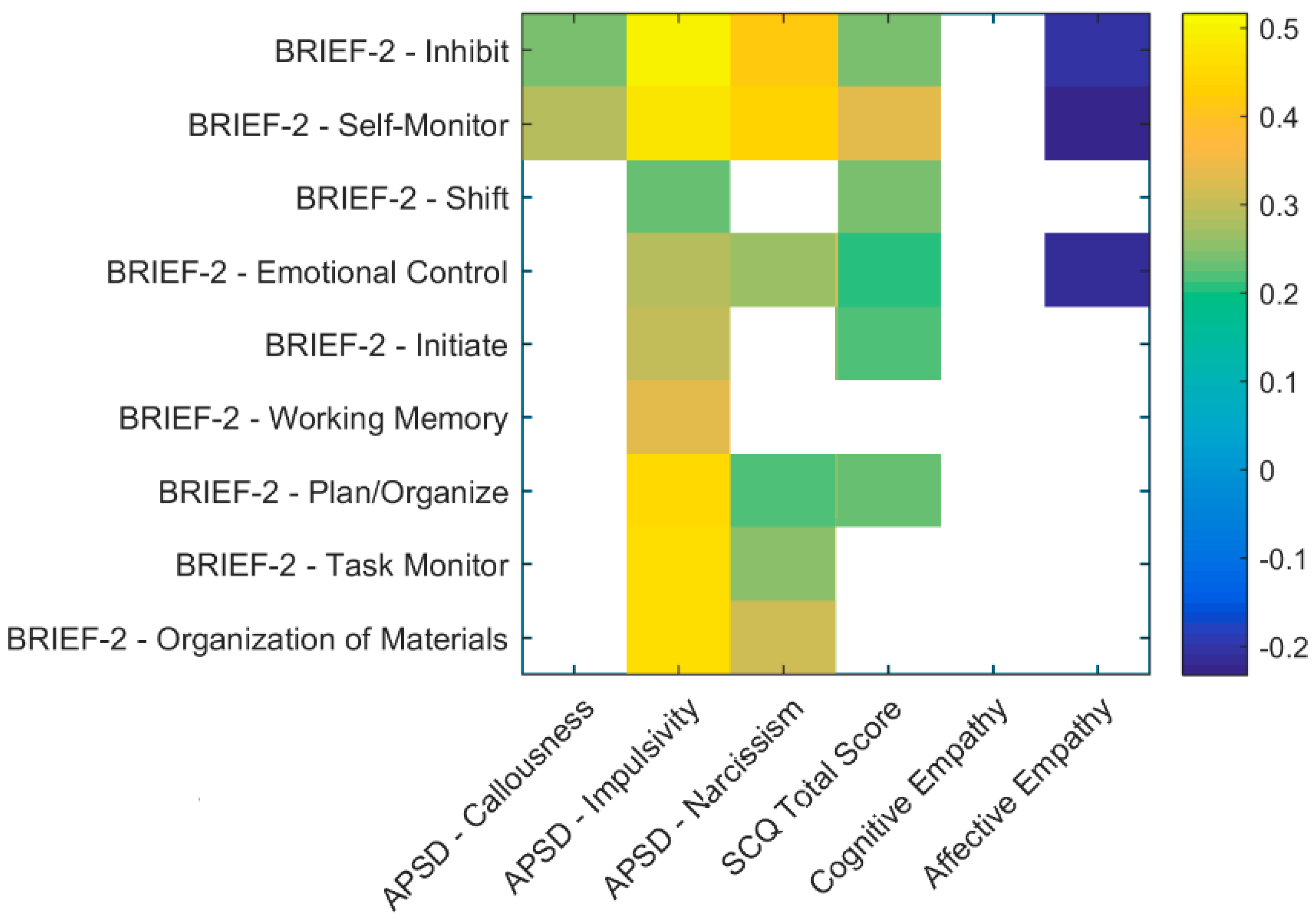
3.2. Correlations
3.3. Regression Models
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Decety, J.; Moriguchi, Y. The empathic brain and its dysfunction in psychiatric populations: Implications for intervention across different clinical conditions. Biopsychosoc. Med. 2007, 1, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zahn-Waxler, C.; Robinson, J.L.; Emde, R.N. The development of empathy in twins. Dev. Psychol. 1992, 28, 1038–1047. [Google Scholar] [CrossRef]
- Knafo, A.; Zahn-Waxler, C.; Van Hulle, C.; Robinson, J.A.L.; Rhee, S.H. The developmental origins of a disposition toward empathy: Genetic and environmental contributions. Emotion 2008, 8, 737–752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singer, T.; Seymour, B.; O’Doherty, J.P.; Stephan, K.E.; Dolan, R.J.; Frith, C.D. Empathic neural responses are modulated by the perceived fairness of others. Nature 2006, 439, 466–469. [Google Scholar] [CrossRef]
- Muratori, P.; Lochman, J.E.; Lai, E.; Milone, A.; Nocentini, A.; Pisano, S.; Righini, E.; Masi, G. Which dimension of parenting predicts the change of callous unemotional traits in children with disruptive behavior disorder? Compr. Psychiatry 2016, 69, 202–210. [Google Scholar] [CrossRef]
- Gonzalez-Liencres, C.; Shamay-Tsoory, S.G.; Brüne, M. Towards a neuroscience of empathy: Ontogeny, phylogeny, brain mechanisms, context and psychopathology. Neurosci. Biobehav. Rev. 2013, 37, 1537–1548. [Google Scholar] [CrossRef]
- Vellante, M.; Baron-Cohen, S.; Melis, M.; Marrone, M.; Petretto, D.R.; Masala, C.; Preti, A. The “Reading the Mind in the Eyes” test: Systematic review of psychometric properties and a validation study in Italy. Cogn. Neuropsychiatry 2013, 18, 326–354. [Google Scholar] [CrossRef]
- Preti, A.; Vellante, M.; Baron-Cohen, S.; Zucca, G.; Petretto, D.R.; Masala, C. The Empathy Quotient: A cross-cultural comparison of the Italian version. Cogn. Neuropsychiatry 2011, 16, 50–70. [Google Scholar] [CrossRef]
- Blair, R.J.R. Responding to the emotions of others: Dissociating forms of empathy through the study of typical and psychiatric populations. Conscious. Cogn. 2005, 14, 698–718. [Google Scholar] [CrossRef]
- Bons, D.; van den Broek, E.; Scheepers, F.; Herpers, P.; Rommelse, N.; Buitelaaar, J.K. Motor, emotional, and cognitive empathy in children and adolescents with autism spectrum disorder and conduct disorder. J. Abnorm. Child Psychol. 2013, 41, 425–443. [Google Scholar] [CrossRef]
- Mazza, M.; Pino, M.C.; Mariano, M.; Tempesta, D.; Ferrara, M.; De Berardis, D.; Masedu, F.; Valenti, M. Affective and cognitive empathy in adolescents with autism spectrum disorder. Front. Hum. Neurosci. 2014, 8, 791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jolliffe, D.; Farrington, D.P. Development and validation of the Basic Empathy Scale. J. Adolesc. 2006, 29, 589–611. [Google Scholar] [CrossRef] [PubMed]
- Loney, B.R.; Frick, P.J.; Clements, C.B.; Ellis, M.L.; Kerlin, K. Callous-Unemotional Traits, Impulsivity, and Emotional Processing in Adolescents With Antisocial Behavior Problems. J. Clin. Child Adolesc. Psychol. 2003, 32, 66–80. [Google Scholar] [CrossRef] [PubMed]
- Dadds, M.R.; Perry, Y.; Hawes, D.J.; Merz, S.; Riddell, A.C.; Haines, D.J.; Solak, E. Attention to the eyes and fear-recognition deficits in child psychopathy. Br. J. Psychiatry 2006, 189, 280–281. [Google Scholar] [CrossRef] [Green Version]
- Blair, R.J.R. Neurocognitive models of aggression, the antisocial personality disorders, and psychopathy. J. Neurol. Neurosurg. Psychiatry 2001, 71, 727–731. [Google Scholar] [CrossRef] [PubMed]
- Blair, R.J.R. The amygdala and ventromedial prefrontal cortex in morality and psychopathy n.d. Trends Cogn. Sci. 2007, 11, 387–392. [Google Scholar] [CrossRef]
- Milone, A.; Cerniglia, L.; Cristofani, C.; Inguaggiato, E.; Levantini, V.; Masi, G. Empathy in youths with conduct disorder and callous-unemotional traits. Neural Plast. 2019, 2019. [Google Scholar] [CrossRef] [Green Version]
- Jones, A.P.; Happé, F.G.E.; Gilbert, F.; Burnett, S.; Viding, E. Feeling, caring, knowing: Different types of empathy deficit in boys with psychopathic tendencies and autism spectrum disorder. J. Child Psychol. Psychiatry 2010, 51, 1188–1197. [Google Scholar] [CrossRef] [Green Version]
- Ashwin, C.; Chapman, E.; Colle, L.; Baron-Cohen, S. Impaired recognition of negative basic emotions in autism: A test of the amygdala theory. Soc. Neurosci. 2006, 1, 349–363. [Google Scholar] [CrossRef]
- Braaten, E.; Rosen, L.A. Self-regulation of affect in attention deficit-hyperactivity disorder (ADHD) and non-ADHD boys: Differences in empathic responding. J. Consult. Clin. Psychol. 2000, 68, 313–321. [Google Scholar] [CrossRef]
- Nijmeijer, J.S.; Minderaa, R.B.; Buitelaar, J.K.; Mulligan, A.; Hartman, C.A.; Hoekstra, P.J. Attention-deficit/hyperactivity disorder and social dysfunctioning. Clin. Psychol. Rev. 2008, 28, 692–708. [Google Scholar] [CrossRef] [PubMed]
- Abikoff, H.; Hechtman, L.; Klein, R.G.; Gallagher, R.; Fleiss, K.; Etcovitch, J.; Cousins, L.; Greenfield, B.; Martin, D.; Pollack, S. Social functioning in children with ADHD treated with long-term methylphenidate and multimodal psychosocial treatment. J. Am. Acad. Child Adolesc. Psychiatry 2004, 43, 820–829. [Google Scholar] [CrossRef] [PubMed]
- Cordier, R.; Bundy, A.; Hocking, C.; Einfeld, S. Empathy in the play of children with attention deficit hyperactivity disorder. OTJR Occup. Particip. Health 2010, 30, 122–132. [Google Scholar] [CrossRef]
- Maoz, H.; Gvirts, H.Z.; Sheffer, M.; Bloch, Y. Theory of Mind and Empathy in Children With ADHD. J. Atten. Disord. 2019, 23, 1331–1338. [Google Scholar] [CrossRef] [PubMed]
- Davis, A. multidimensional approach to individual difference in empathy. JSAS Cat. Sel. Doc. Psychol. 1980, 10, 85. [Google Scholar]
- Maoz, H.; Tsviban, L.; Gvirts, H.Z.; Shamay-Tsoory, S.G.; Levkovitz, Y.; Watemberg, N.; Bloch, Y. Stimulants improve theory of mind in children with attention deficit/hyperactivity disorder. J. Psychopharmacol. 2014, 28, 212–219. [Google Scholar] [CrossRef]
- Uekermann, J.; Kraemer, M.; Krankenhaus, A.K.; Abdel-Hamid, M.; Hebebrand, J.; Daum, I.; Wiltfang, J.; Kis, B. Social cognition in attention-deficit hyperactivity disorder (ADHD). Neurosci. Biobehav. Rev. 2009, 34, 734–743. [Google Scholar] [CrossRef]
- Barkley, R.A. The relevance of the Still lectures to attention-deficit/hyperactivity disorder: A commentary. J. Atten. Disord. 2006, 10, 137–140. [Google Scholar] [CrossRef]
- Yan, Z.; Hong, S.; Liu, F.; Su, Y. A meta-analysis of the relationship between empathy and executive function. PsyCh J. 2020, 9, 34–43. [Google Scholar] [CrossRef]
- Preston, S.D.; de Waal, F.B.M. Empathy: Its ultimate and proximate bases. Behav. Brain Sci. 2002, 25, 1–20. [Google Scholar] [CrossRef] [Green Version]
- de Waal, F.B.M.; Preston, S.D. Mammalian empathy: Behavioural manifestations and neural basis. Nat. Rev. Neurosci. 2017, 18, 498–509. [Google Scholar] [CrossRef] [PubMed]
- Decety, J.; Meyer, M. From emotion resonance to empathic understanding: A social developmental neuroscience account. Dev. Psychopathol. 2008, 20, 1053–1080. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heyes, C. Empathy is not in our genes. Neurosci. Biobehav. Rev. 2018, 95, 499–507. [Google Scholar] [CrossRef] [PubMed]
- de Waal, F.B.M. Putting the altruism back into altruism: The evolution of empathy. Annu. Rev. Psychol. 2008, 59, 279–300. [Google Scholar] [CrossRef]
- Hoffman, M.L. Prosocial behavior and empathy: Developmental processes. Int. Encycl. Soc. Behav. Sci. 2001, 12230–12233. [Google Scholar] [CrossRef]
- Shamay-Tsoory, S.G. The neural bases for empathy. Neuroscientist 2011, 17, 18–24. [Google Scholar] [CrossRef]
- Hoffman, M.L. The contribution of empathy to justice and moral judgment. In Empathy and Its Development; Eisenberg, N., Strayer, J., Eds.; University of Cambridge Press: Cambridge, UK, 1987; pp. 47–80. [Google Scholar]
- Ze, O.; Thoma, P.; Suchan, B. Cognitive and affective empathy in younger and older individuals. Aging Ment. Health 2014, 18, 929–935. [Google Scholar] [CrossRef]
- Valiente, C.; Eisenberg, N.; Fabes, R.A.; Shepard, S.A.; Cumberland, A.; Losoya, S.H. Prediction of children’s empathy-related responding from their effortful control and parents’ expressivity. Dev. Psychol. 2004, 40, 911–926. [Google Scholar] [CrossRef] [Green Version]
- Spinella, M. Self-rated executive function: Development of the executive function index. Int. J. Neurosci. 2005, 115, 649–667. [Google Scholar] [CrossRef]
- Eisenberg, N.; Okun, M.A. The relations of dispositional regulation and emotionality to elders’ empathy-related responding and affect while volunteering. J. Pers. 1996, 64, 157–183. [Google Scholar] [CrossRef]
- Gao, Z.; Ye, T.; Shen, M.; Perry, A. Working memory capacity of biological movements predicts empathy traits. Psychon. Bull. Rev. 2016, 23, 468–475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gökçen, E.; Petrides, K.V.; Hudry, K.; Frederickson, N.; Smillie, L.D. Sub-threshold autism traits: The role of trait emotional intelligence and cognitive flexibility. Br. J. Psychol. 2014, 105, 187–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gökçen, E.; Frederickson, N.; Petrides, K.V. Theory of mind and executive control deficits in typically developing adults and adolescents with high levels of autism traits. J. Autism Dev. Disord. 2016, 46, 2072–2087. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, H.; Su, Y.; Jin, J. Empathy-related responding in chinese toddlers: Factorial structure and cognitive contributors. Infant Child Dev. 2017, 26, e1983. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, L.N.; Demaray, M.K.; Tennant, J. Social, emotional, and cognitive factors associated with bullying. School Psych. Rev. 2017, 46, 42–64. [Google Scholar] [CrossRef]
- Abdel-Hamid, M.; Niklewski, F.; Heßmann, P.; Guberina, N.; Kownatka, M.; Kraemer, M.; Scherbaum, N.; Dziobek, I.; Bartels, C.; Wiltfang, J.; et al. Impaired empathy but no theory of mind deficits in adult attention deficit hyperactivity disorder. Brain Behav. 2019, 9, e01401. [Google Scholar] [CrossRef] [Green Version]
- Pineda-Alhucema, W.; Aristizabal, E.; Escudero-Cabarcas, J.; Acosta-López, J.E.; Vélez, J.I. Executive function and theory of mind in children with ADHD: A systematic review. Neuropsychol. Rev. 2018, 28, 341–358. [Google Scholar] [CrossRef]
- Andreou, M.; Skrimpa, V. Theory of mind deficits and neurophysiological operations in autism spectrum disorders: A review. Brain Sci. 2020, 10, 393. [Google Scholar] [CrossRef]
- Goldberg, E.; Podell, K. Adaptive decision making, ecological validity, and the frontal lobes. J. Clin. Exp. Neuropsychol. 2000, 22, 56–68. [Google Scholar] [CrossRef]
- Gioia, G.; Isquith, P.; Guy, S.; Kenworthy, L. BRIEF-2: Behavior Rating Inventory of Executive Function: Professional Manual; Psychological Assessment Resources: Lutz, FL, USA, 2015. [Google Scholar]
- Van der Meere, J.; Marzocchi, G.M.; De Meo, T. Response inhibition and attention deficit hyperactivity disorder with and without oppositional defiant disorder screened from a community sample. Dev. Neuropsychol. 2005, 28, 459–472. [Google Scholar] [CrossRef] [PubMed]
- Willcutt, E.G.; Doyle, A.E.; Nigg, J.T.; Faraone, S.V.; Pennington, B.F. Validity of the executive function theory of attention-deficit/hyperactivity disorder: A meta-analytic review. Biol. Psychiatry 2005, 57, 1336–1346. [Google Scholar] [CrossRef] [PubMed]
- Marton, I.; Wiener, J.; Rogers, M.; Moore, C.; Tannock, R. Empathy and social perspective taking in children with attention-deficit/ hyperactivity disorder. J. Abnorm. Child Psychol. 2009, 37, 107–118. [Google Scholar] [CrossRef] [PubMed]
- American Psychological Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychological Association: Washington, DC, USA, 2013. [Google Scholar]
- Kaufman, J.; Birmaher, B.; Brent, D.; Rao, U.; Flynn, C.; Moreci, P.; Williamson, D.; Ryan, N. Schedule for affective disorders and schizophrenia for school-age children-present and lifetime version (K-SADS-PL): Initial reliability and validity data. J. Am. Acad. Child Adolesc. Psychiatry 1997, 36, 980–988. [Google Scholar] [CrossRef]
- Pandolfi, V.; Magyar, C.I. Child behavior checklist for ages 6–18. In Encyclopedia of Autism Spectrum Disorders; Volkmar, F.R., Ed.; Springer: New York, NY, USA, 2013; pp. 581–587. [Google Scholar] [CrossRef]
- Achenbach, T.; Rescorla, L. Manual for the ASEBA School-Age Forms and Profiles: An Integrated System of Multi-Informant Assessment; Research Center for Children, Youth, & Families, University of Vermont: Burlington, VT, USA, 2001. [Google Scholar]
- Rutter, M.; Bailey, A.; Lord, C. The Social Communication Questionnaire Manual; Western Psychological Services: Los Angeles, CA, USA, 2003. [Google Scholar]
- Rutter, M.; LeCouteur, A.; Lord, C. Autism Diagnostic Interview-Revised; Western Psychological Services: Los Angeles, CA, USA, 2003. [Google Scholar]
- Lord, C.; Rutter, M.; DiLavore, P.; Risi, S.; Gotham, K.; Bishop, S. Autism Diagnostic Observation Schedule (ADOS-2), 2nd ed.; Western Psychological Services: Los Angeles, CA, USA, 2012; Available online: https://www.wpspublish.com/ados-2-autism-diagnostic-observation-schedule-second-edition (accessed on 22 February 2020).
- Frick, P.; Hare, R. Antisocial Process. Screening Device: APSD; Multi-Health Systems: Toronto, ON, Canada, 2001. [Google Scholar]
- Masi, G.; Milone, A.; Brovedani, P.; Pisano, S.; Muratori, P. Psychiatric evaluation of youths with disruptive behavior disorders and psychopathic traits: A critical review of assessment measures. Neurosci. Biobehav. Rev. 2018, 91, 21–33. [Google Scholar] [CrossRef] [PubMed]
- Litvack-Miller, W.; McDougall, D.; Romney, D.M. The structure of empathy during middle childhood and its relationship to prosocial behavior. Genet. Soc. Gen. Psychol. Monogr. 1997, 123, 303–324. [Google Scholar]
- Benjamini, Y.; Hochberg, Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J. R. Stat. Soc. 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Mouti, A.; Dryer, R.; Kohn, M. Differentiating autism spectrum disorder from ADHD using the social communication questionnaire. J. Atten. Disord. 2019, 23, 828–837. [Google Scholar] [CrossRef]
- Narzisi, A.; Posada, M.; Barbieri, F.; Chericoni, N.; Ciuffolini, D.; Pinzino, M.; Romano, R.; Scattoni, M.L.; Tancredi, R.; Calderoni, S.; et al. Prevalence of autism spectrum disorder in a large Italian catchment area: A school-based population study within the ASDEU project. Epidemiol. Psychiatr. Sci. 2018, 29, e5. [Google Scholar] [CrossRef]
- Tye, C.; Bedford, R.; Asherson, P.; Ashwood, K.L.; Azadi, B.; Bolton, P.; McLoughlin, G. Callous-unemotional traits moderate executive function in children with ASD and ADHD: A pilot event-related potential study. Dev. Cogn. Neurosci. 2017, 26, 84–90. [Google Scholar] [CrossRef]
- Herpers, P.C.M.; Rommelse, N.N.J.; Bons, D.M.A.; Buitelaar, J.K.; Scheepers, F.E. Callous-unemotional traits as a cross-disorders construct. Soc. Psychiatry Psychiatr. Epidemiol. 2012, 47, 2045–2064. [Google Scholar] [CrossRef] [Green Version]
- Ay, M.G.; Kiliç, B.G. Factors associated with empathy among adolescents with attention deficit hyperactivity disorder. Turk Psikiyatr. Derg. 2019, 30, 260–267. [Google Scholar] [CrossRef]
- Song, Y.; Nie, T.; Shi, W.; Zhao, X.; Yang, Y. Empathy impairment in individuals with autism spectrum conditions from a multidimensional perspective: A meta-analysis. Front. Psychol. 2019, 10, 1902. [Google Scholar] [CrossRef] [PubMed]
- Pijper, J.; de Wied, M.; van Rijn, S.; van Goozen, S.; Swaab, H.; Meeus, W. Executive attention and empathy-related responses in boys with oppositional defiant disorder or conduct disorder, with and without comorbid anxiety disorder. Child Psychiatry Hum. Dev. 2018, 49, 956–965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zelazo, P.D.; Carlson, S.M. Hot and cool executive function in childhood and adolescence: Development and plasticity. Child Dev. Perspect. 2012, 6, 354–360. [Google Scholar] [CrossRef]
- Zelazo, P.D. Executive function and psychopathology: A neurodevelopmental perspective. Annu. Rev. Clin. Psychol. 2020, 16, 431–454. [Google Scholar] [CrossRef] [Green Version]
- Miranda, A.; Berenguer, C.; Roselló, B.; Baixauli, I.; Colomer, C. Social cognition in children with high-functioning autism spectrum disorder and attention-deficit/hyperactivity disorder. associations with executive functions. Front. Psychol. 2017, 8, 1035. [Google Scholar] [CrossRef]
- Brooks, B.L.; Sherman, E.M.S.; Strauss, E. NEPSY-II: A Developmental neuropsychological assessment, second edition. Child Neuropsychol. 2010, 16, 80–101. [Google Scholar] [CrossRef]
- Fassino, S. Empatia e strategie dell’incoraggiamento nel processo di cambiamento. Riv. Psicol. Indiv. 2009, 63, 49–63. [Google Scholar]
- Rizeq, J.; Toplak, M.E.; Ledochowski, J.; Basile, A.; Andrade, B.F. Developmental neuropsychology callous-unemotional traits and executive functions are unique correlates of disruptive behavior in children. Dev. Neuropsychol. 2020, 45, 154–166. [Google Scholar] [CrossRef]
- Lambruschi, F.; Muratori, P. Psicopatologia e Psicoterapia dei Disturbi della Condotta; Carocci: Rome, Italy, 2013. [Google Scholar]
- Blair, R.J.R.; Peschardt, K.S.; Budhani, S.; Mitchell, D.G.V.; Pine, D.S. The development of psychopathy. J. Child Psychol. Psychiatry 2006, 47, 262–276. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| A. CBCL-AB | Estimates | β-Coefficients | Standard Errors | p-Values |
|---|---|---|---|---|
| Intercept | 26.3134 | 0.0000 | 4.9028 | 4.21 × 10−7 *** |
| BRIEF-2-BRI | 0.7645 | 0.3891 | 0.1843 | 6.49 × 10−5 *** |
| BRIEF-2-CRI | 0.0667 | 0.2932 | 0.0715 | 0.3525 |
| BRIEF-2-ERI | 0.4610 | 0.0753 | 0.1481 | 0.0023 ** |
| Affective Empathy | −1.2782 | −0.1137 | 0.9909 | 0.1996 |
| Cognitive Empathy | 0.6295 | 0.0580 | 0.9616 | 0.5139 |
| SCQ Score | −0.0541 | −0.0306 | 0.1317 | 0.6816 |
| B. CBCL-ODP | Estimates | β-Coefficients | Standard Errors | p-Values |
| Intercept | 35.6661 | 0.0000 | 3.8429 | 1.23 × 10−15 *** |
| BRIEF-2-BRI | 0.5471 | 0.3891 | 0.1445 | 0.0002 *** |
| BRIEF-2-CRI | 0.0535 | 0.2932 | 0.0560 | 0.3420 |
| BRIEF-2-ERI | 0.3042 | 0.0753 | 0.1161 | 0.0099 ** |
| Affective Empathy | −0.9299 | −0.1137 | 0.7767 | 0.2336 |
| Cognitive Empathy | 0.1635 | 0.0580 | 0.7537 | 0.8285 |
| SCQ Score | 0.0105 | −0.0306 | 0.1032 | 0.9186 |
| C. CBCL-RBB | Estimates | β-Coefficients | Standard Errors | p-Values |
| Intercept | 38.4738 | 0.0000 | 3.6169 | <2 × 10−16 *** |
| BRIEF-2-BRI | 0.6978 | 0.3891 | 0.1355 | 1.11 × 10−6 *** |
| BRIEF-2-CRI | 0.0355 | 0.2932 | 0.0526 | 0.5008 |
| BRIEF-2-ERI | 0.0637 | 0.0753 | 0.1091 | 0.5606 |
| Affective Empathy | −1.5698 | −0.1137 | 0.7326 | 0.0343 * |
| Cognitive Empathy | −0.0574 | 0.0580 | 0.7121 | 0.9359 |
| SCQ Score | −0.0296 | −0.0306 | 0.0968 | 0.7599 |
| D. CBCL-CP | Estimates | β-Coefficients | Standard Errors | p-Values |
| Intercept | 37.5833 | 0.0000 | 3.7916 | <2 × 10−16 *** |
| BRIEF-2-BRI | 0.7870 | 0.3891 | 0.1424 | 2.12 × 10−7 *** |
| BRIEF-2-CRI | −0.0062 | 0.2932 | 0.0547 | 0.9096 |
| BRIEF-2-ERI | 0.1749 | 0.0753 | 0.1165 | 0.1359 |
| Affective Empathy | −1.7449 | −0.1137 | 0.7665 | 0.0247 * |
| Cognitive Empathy | −0.3663 | 0.0580 | 0.7409 | 0.6220 |
| SCQ Score | −0.1235 | −0.0306 | 0.1008 | 0.2229 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cristofani, C.; Sesso, G.; Cristofani, P.; Fantozzi, P.; Inguaggiato, E.; Muratori, P.; Narzisi, A.; Pfanner, C.; Pisano, S.; Polidori, L.; et al. The Role of Executive Functions in the Development of Empathy and Its Association with Externalizing Behaviors in Children with Neurodevelopmental Disorders and Other Psychiatric Comorbidities. Brain Sci. 2020, 10, 489. https://doi.org/10.3390/brainsci10080489
Cristofani C, Sesso G, Cristofani P, Fantozzi P, Inguaggiato E, Muratori P, Narzisi A, Pfanner C, Pisano S, Polidori L, et al. The Role of Executive Functions in the Development of Empathy and Its Association with Externalizing Behaviors in Children with Neurodevelopmental Disorders and Other Psychiatric Comorbidities. Brain Sciences. 2020; 10(8):489. https://doi.org/10.3390/brainsci10080489
Chicago/Turabian StyleCristofani, Chiara, Gianluca Sesso, Paola Cristofani, Pamela Fantozzi, Emanuela Inguaggiato, Pietro Muratori, Antonio Narzisi, Chiara Pfanner, Simone Pisano, Lisa Polidori, and et al. 2020. "The Role of Executive Functions in the Development of Empathy and Its Association with Externalizing Behaviors in Children with Neurodevelopmental Disorders and Other Psychiatric Comorbidities" Brain Sciences 10, no. 8: 489. https://doi.org/10.3390/brainsci10080489