Self-Reported Autistic Traits Using the AQ: A Comparison between Individuals with ASD, Psychosis, and Non-Clinical Controls

 , , , and
, , , and
Abstract
:1. Introduction
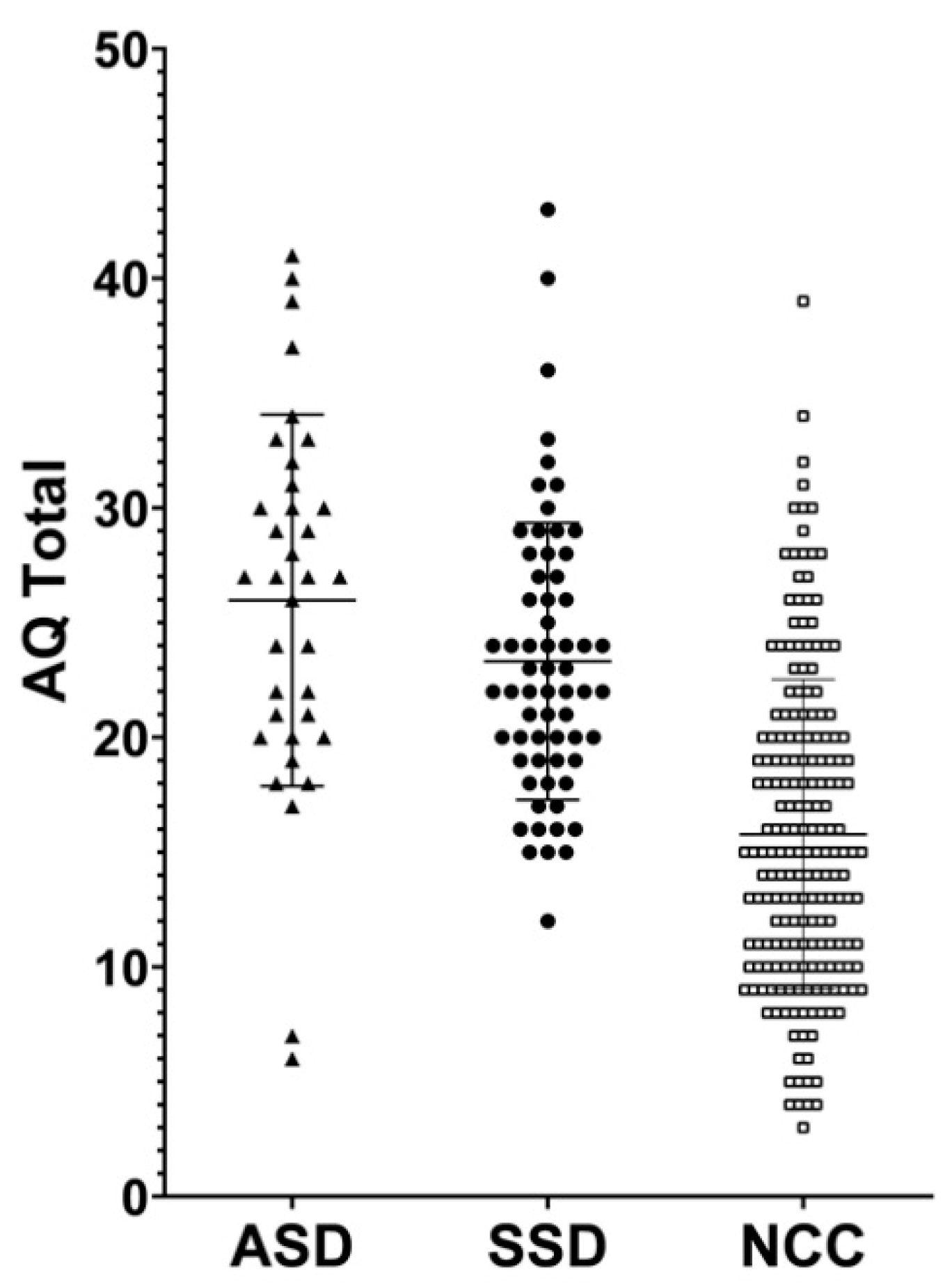
- Investigate the differences in self-reported autistic traits between adults with ASD, SSD and a non-clinical control group (NCC) from the general population;
- Analyze the accuracy of AQ in discriminating between ASD and SSD, as well as between ASD and NCC.
- Correlate the AQ scores with ADOS-2 scores in the ASD population.
2. Materials and Methods
2.1. Setting and Procedures
2.2. Participants
2.3. Autism-Spectrum Quotient (AQ)
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Sample
3.2. Differences in AQ Scores
3.3. Analysis of Accuracy
3.4. Correlation between AQ and ADOS-2 Scores
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bleuler, E. Dementia Praecox or the Group of Schizophrenias; International Universities Press: New York, NY, USA, 1950. [Google Scholar]
- Kanner, L. Autistic disturbances of affective contact. Nerv. Child 1943, 2, 217–250. [Google Scholar]
- Rutter, M. Childhood schizophrenia reconsidered. J. Autism Child. Schizophr. 1972, 2, 315–337. [Google Scholar] [CrossRef]
- Kolvin, I. Studies in the childhood psychoses i. Diagnostic criteria and classification. Br. J. Psychiatry 1971, 118, 381–384. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Pub: Washington, DC, USA, 2013. [Google Scholar]
- Fusar-Poli, L.; Brondino, N.; Rocchetti, M.; Panisi, C.; Provenzani, U.; Damiani, S.; Politi, P. Diagnosing ASD in adults without ID: Accuracy of the ADOS-2 and the ADI-R. J. Autism Dev. Disord. 2017, 47, 3370–3379. [Google Scholar] [CrossRef] [PubMed]
- Baxter, A.J.; Brugha, T.; Erskine, H.E.; Scheurer, R.W.; Vos, T.; Scott, J.G. The epidemiology and global burden of autism spectrum disorders. Psychol. Med. 2015, 45, 601–613. [Google Scholar] [CrossRef] [PubMed]
- Narzisi, A.; Posada, M.; Barbieri, F.; Chericoni, N.; Ciuffolini, D.; Pinzino, M.; Romano, R.; Scattoni, M.; Tancredi, R.; Calderoni, S. Prevalence of autism spectrum disorder in a large Italian catchment area: A school-based population study within the asdeu project. Epidemiol. Psychiatr. Sci. 2020, 29, e5. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Küstner, B.; Martín, C.; Pastor, L. Prevalence of psychotic disorders and its association with methodological issues. A systematic review and meta-analyses. PLoS ONE 2018, 13, e0195687. [Google Scholar] [CrossRef]
- Crespi, B.; Stead, P.; Elliot, M. Comparative genomics of autism and schizophrenia. Proc. Natl. Acad. Sci. USA 2010, 107, 1736–1741. [Google Scholar] [CrossRef] [Green Version]
- St Pourcain, B.; Robinson, E.B.; Anttila, V.; Sullivan, B.B.; Maller, J.; Golding, J.; Skuse, D.; Ring, S.; Evans, D.M.; Zammit, S. ASD and schizophrenia show distinct developmental profiles in common genetic overlap with population-based social communication difficulties. Mol. Psychiatry 2018, 23, 263–270. [Google Scholar] [CrossRef] [Green Version]
- Grossi, E.; Veggo, F.; Narzisi, A.; Compare, A.; Muratori, F. Pregnancy risk factors in autism: A pilot study with artificial neural networks. Pediatr. Res. 2016, 79, 339–347. [Google Scholar] [CrossRef]
- Davies, C.; Segre, G.; Estrade, A.; Radua, J.; De Micheli, A.; Provenzani, U.; Oliver, D.; Salazar de Pablo, G.; Ramella-Cravaro, V.; Besozzi, M.; et al. Prenatal and perinatal risk and protective factors for psychosis: A systematic review and meta-analysis. Lancet Psychiatry 2020, 7, 399–410. [Google Scholar] [CrossRef]
- Cheung, C.; Yu, K.; Fung, G.; Leung, M.; Wong, C.; Li, Q.; Sham, P.; Chua, S.; McAlonan, G. Autistic disorders and schizophrenia: Related or remote? An anatomical likelihood estimation. PLoS ONE 2010, 5, e12233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sugranyes, G.; Kyriakopoulos, M.; Corrigall, R.; Taylor, E.; Frangou, S. Autism spectrum disorders and schizophrenia: Meta-analysis of the neural correlates of social cognition. PLoS ONE 2011, 6, e25322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pavăl, D. A dopamine hypothesis of autism spectrum disorder. Dev. Neurosci. 2017, 39, 355–360. [Google Scholar] [CrossRef]
- Howes, O.D.; McCutcheon, R.; Owen, M.J.; Murray, R.M. The role of genes, stress, and dopamine in the development of schizophrenia. Biol. Psychiatry 2017, 81, 9–20. [Google Scholar] [CrossRef] [Green Version]
- Prata, J.; Santos, S.G.; Almeida, M.I.; Coelho, R.; Barbosa, M.A. Bridging autism spectrum disorders and schizophrenia through inflammation and biomarkers-pre-clinical and clinical investigations. J. Neuroinflamm. 2017, 14, 179. [Google Scholar] [CrossRef] [Green Version]
- Chisholm, K.; Lin, A.; Abu-Akel, A.; Wood, S.J. The association between autism and schizophrenia spectrum disorders: A review of eight alternate models of co-occurrence. Neurosci. Biobehav. Rev. 2015, 55, 173–183. [Google Scholar] [CrossRef] [Green Version]
- Spain, D.; Sin, J.; Freeman, D. Conceptualising paranoia in ASD: A systematic review and development of a theoretical framework. Res. Autism Spectr. Disord. 2016, 25, 97–111. [Google Scholar] [CrossRef]
- Nylander, L. Autism and schizophrenia in adults: Clinical considerations on comorbidity and differential diagnosis. In Comprehensive Guide to Autism; Springer: New York, NY, USA, 2014; pp. 263–281. [Google Scholar]
- Fernandes, J.M.; Cajão, R.; Lopes, R.; Jerónimo, R.; Barahona-Corrêa, J.B. Social cognition in schizophrenia and autism spectrum disorders: A systematic review and meta-analysis of direct comparisons. Front. Psychiatry 2018, 9, 504. [Google Scholar] [CrossRef] [Green Version]
- Lin, C.-H.; Huang, C.-L.; Chang, Y.-C.; Chen, P.-W.; Lin, C.-Y.; Tsai, G.E.; Lane, H.-Y. Clinical symptoms, mainly negative symptoms, mediate the influence of neurocognition and social cognition on functional outcome of schizophrenia. Schizophr. Res. 2013, 146, 231–237. [Google Scholar] [CrossRef]
- Damiani, S.; Fusar-Poli, L.; Brondino, N.; Provenzani, U.; Baldwin, H.; Fusar-Poli, P.; Politi, P. World/self ambivalence: A shared mechanism in different subsets of psychotic experiences? Linking symptoms with resting-state fmri. Psychiatry Res. Neuroimaging 2020, 299, 111068. [Google Scholar] [CrossRef] [PubMed]
- Noel, J.-P.; Cascio, C.J.; Wallace, M.T.; Park, S. The spatial self in schizophrenia and autism spectrum disorder. Schizophr. Res. 2017, 179, 8–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marco, E.J.; Hinkley, L.B.; Hill, S.S.; Nagarajan, S.S. Sensory processing in autism: A review of neurophysiologic findings. Pediatr. Res. 2011, 69, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Muratori, F.; Tonacci, A.; Billeci, L.; Catalucci, T.; Igliozzi, R.; Calderoni, S.; Narzisi, A. Olfactory processing in male children with autism: Atypical odor threshold and identification. J. Autism Dev. Disord. 2017, 47, 3243–3251. [Google Scholar] [CrossRef] [PubMed]
- Wolf, J.M.; Ventola, P. Assessment and treatment planning in adults with autism spectrum disorders. In Adolescents and Adults with Autism Spectrum Disorders; Springer: New York, NY, USA, 2014; pp. 283–298. [Google Scholar]
- Kaufmann, C.; Agalawatta, N.; Malhi, G.S. Catatonia: Stereotypies, mannerisms and perseverations. Aust. N. Z. J. Psychiatry 2018, 52, 391–393. [Google Scholar] [CrossRef]
- Kapp, S.K.; Steward, R.; Crane, L.; Elliott, D.; Elphick, C.; Pellicano, E.; Russell, G. ‘People should be allowed to do what they like’: Autistic adults’ views and experiences of stimming. Autism Int. J. Res. Pract. 2019, 23, 1782–1792. [Google Scholar] [CrossRef] [Green Version]
- Geurts, H.M.; Jansen, M.D. A retrospective chart study: The pathway to a diagnosis for adults referred for ASD assessment. Autism Int. J. Res. Pract. 2012, 16, 299–305. [Google Scholar] [CrossRef]
- Nylander, L.; Gillberg, C. Screening for autism spectrum disorders in adult psychiatric out-patients: A preliminary report. Acta Psychiatr. Scand. 2001, 103, 428–434. [Google Scholar] [CrossRef]
- Lai, M.-C.; Kassee, C.; Besney, R.; Bonato, S.; Hull, L.; Mandy, W.; Szatmari, P.; Ameis, S.H. Prevalence of co-occurring mental health diagnoses in the autism population: A systematic review and meta-analysis. Lancet Psychiatry 2019, 6, 819–829. [Google Scholar] [CrossRef]
- Marín, J.L.; Rodríguez-Franco, M.A.; Chugani, V.M.; Maganto, M.M.; Villoria, E.D.; Bedia, R.C. Prevalence of schizophrenia spectrum disorders in average-iq adults with autism spectrum disorders: A meta-analysis. J. Autism Dev. Disord. 2018, 48, 239–250. [Google Scholar] [CrossRef]
- De Giorgi, R.; De Crescenzo, F.; D’Alò, G.; Rizzo Pesci, N.; Di Franco, V.; Sandini, C.; Armando, M. Prevalence of schizophrenia spectrum disorders in individuals with autism spectrum disorders: A systematic review. J. Clin. Med. 2019, 8, 1304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kincaid, D.L.; Doris, M.; Shannon, C.; Mulholland, C. What is the prevalence of autism spectrum disorder and ASD traits in psychosis? A systematic review. Psychiatry Res. 2017, 250, 99–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lord, C.; Rutter, M.; DiLavore, P.; Risi, S.; Gotham, K.; Bishop, S. (ADOS-2) Autism Diagnostic Observation Schedule, 2nd ed.; Western Psychological Corporation: Los Angeles, CA, USA, 2012. [Google Scholar]
- Bastiaansen, J.A.; Meffert, H.; Hein, S.; Huizinga, P.; Ketelaars, C.; Pijnenborg, M.; Bartels, A.; Minderaa, R.; Keysers, C.; De Bildt, A. Diagnosing autism spectrum disorders in adults: The use of autism diagnostic observation schedule (ADOS) module 4. J. Autism Dev. Disord. 2011, 41, 1256–1266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barlati, S.; Deste, G.; Gregorelli, M.; Vita, A. Autistic traits in a sample of adult patients with schizophrenia: Prevalence and correlates. Psychol. Med. 2019, 49, 140–148. [Google Scholar] [CrossRef] [PubMed]
- Pilling, S.; Baron-Cohen, S.; Megnin-Viggars, O.; Lee, R.; Taylor, C. Recognition, referral, diagnosis, and management of adults with autism: Summary of nice guidance. BMJ 2012, 344, e4082. [Google Scholar] [CrossRef] [Green Version]
- Baron-Cohen, S.; Wheelwright, S.; Skinner, R.; Martin, J.; Clubley, E. The autism-spectrum quotient (AQ): Evidence from asperger syndrome/high-functioning autism, malesand females, scientists and mathematicians. J. Autism Dev. Disord. 2001, 31, 5–17. [Google Scholar] [CrossRef]
- Ruzich, E.; Allison, C.; Smith, P.; Watson, P.; Auyeung, B.; Ring, H.; Baron-Cohen, S. Measuring autistic traits in the general population: A systematic review of the autism-spectrum quotient (AQ) in a nonclinical population sample of 6,900 typical adult males and females. Mol. Autism 2015, 6, 2. [Google Scholar] [CrossRef] [Green Version]
- Allison, C.; Auyeung, B.; Baron-Cohen, S. Toward brief “red flags” for autism screening: The short autism spectrum quotient and the short quantitative checklist in 1000 cases and 3000 controls. J. Am. Acad. Child Adolesc. Psychiatry 2012, 51, 202–212.e7. [Google Scholar] [CrossRef]
- Woodbury-Smith, M.R.; Robinson, J.; Wheelwright, S.; Baron-Cohen, S. Screening adults for Asperger syndrome using the AQ: A preliminary study of its diagnostic validity in clinical practice. J. Autism Dev. Disord. 2005, 35, 331–335. [Google Scholar] [CrossRef]
- Sizoo, B.B.; Horwitz, E.; Teunisse, J.; Kan, C.; Vissers, C.T.W.; Forceville, E.; Van Voorst, A.; Geurts, H. Predictive validity of self-report questionnaires in the assessment of autism spectrum disorders in adults. Autism Int. J. Res. Pract. 2015, 19, 842–849. [Google Scholar] [CrossRef] [Green Version]
- Gantman, A.; Kapp, S.K.; Orenski, K.; Laugeson, E.A. Social skills training for young adults with high-functioning autism spectrum disorders: A randomized controlled pilot study. J. Autism Dev. Disord. 2012, 42, 1094–1103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laugeson, E.A.; Gantman, A.; Kapp, S.K.; Orenski, K.; Ellingsen, R. A randomized controlled trial to improve social skills in young adults with autism spectrum disorder: The ucla peers® program. J. Autism Dev. Disord. 2015, 45, 3978–3989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashwood, K.L.; Gillan, N.; Horder, J.; Hayward, H.; Woodhouse, E.; McEwen, F.S.; Findon, J.; Eklund, H.; Spain, D.; Wilson, C.E.; et al. Predicting the diagnosis of autism in adults using the autism-spectrum quotient (AQ) questionnaire. Psychol. Med. 2016, 46, 2595–2604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Crescenzo, F.; Postorino, V.; Siracusano, M.; Riccioni, A.; Armando, M.; Curatolo, P.; Mazzone, L. Autistic symptoms in schizophrenia spectrum disorders: A systematic review and meta-analysis. Front. Psychiatry 2019, 10, 78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baghdadli, A.; Russet, F.; Mottron, L. Measurement properties of screening and diagnostic tools for autism spectrum adults of mean normal intelligence: A systematic review. Eur. Psychiatry 2017, 44, 104–124. [Google Scholar] [CrossRef] [PubMed]
- Wigham, S.; Rodgers, J.; Berney, T.; Le Couteur, A.; Ingham, B.; Parr, J.R. Psychometric properties of questionnaires and diagnostic measures for autism spectrum disorders in adults: A systematic review. Autism Int. J. Res. Pract. 2019, 23, 287–305. [Google Scholar] [CrossRef] [PubMed]
- Brugha, T.; McManus, S.; Smith, J.; Scott, F.; Meltzer, H.; Purdon, S.; Berney, T.; Tantam, D.; Robinson, J.; Radley, J. Validating two survey methods for identifying cases of autism spectrum disorder among adults in the community. Psychol. Med. 2012, 42, 647–656. [Google Scholar] [CrossRef] [PubMed]
- Naito, K.; Matsui, Y.; Maeda, K.; Tanaka, K. Evaluation of the validity of the autism spectrum quotient (AQ) in differentiating high-functioning autistic spectrum disorder from schizophrenia. Kobe J. Med. Sci. 2010, 56, 116–124. [Google Scholar]
- Wouters, S.G.; Spek, A.A. The use of the autism-spectrum quotient in differentiating high-functioning adults with autism, adults with schizophrenia and a neurotypical adult control group. Res. Autism Spectr. Disord. 2011, 5, 1169–1175. [Google Scholar] [CrossRef]
- Lugnegård, T.; Hallerbäck, M.U.; Gillberg, C. Asperger syndrome and schizophrenia: Overlap of self-reported autistic traits using the autism-spectrum quotient (AQ). Nord. J. Psychiatry 2015, 69, 268–274. [Google Scholar] [CrossRef]
- Zhang, L.; Sun, Y.; Chen, F.; Wu, D.; Tang, J.; Han, X.; Ye, J.; Wang, K. Psychometric properties of the autism-spectrum quotient in both clinical and non-clinical samples: Chinese version for mainland China. BMC Psychiatry 2016, 16, 213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- First, M.; Williams, J.; Karg, R.; Spitzer, R. Structured Clinical Interview for DSM-5—Research Version (scid-5 for DSM-5, Research version; Scid-5-rv); American Psychiatric Association: Arlington, VA, USA, 2015; pp. 1–94. [Google Scholar]
- Hosmer, D.W., Jr.; Lemeshow, S.; Sturdivant, R.X. Applied Logistic Regression; John Wiley & Sons: Hoboken, NJ, USA, 2013. [Google Scholar]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Narzisi, A.; Muratori, F.; Calderoni, S.; Fabbro, F.; Urgesi, C. Neuropsychological profile in high functioning autism spectrum disorders. J. Autism Dev. Disord. 2013, 43, 1895–1909. [Google Scholar] [CrossRef] [PubMed]
- Reed, P.; McCarthy, J. Cross-modal attention-switching is impaired in autism spectrum disorders. J. Autism Dev. Disord. 2012, 42, 947–953. [Google Scholar] [CrossRef]
- Smid, H.G.O.M.; Martens, S.; de Witte, M.R.; Bruggeman, R. Inflexible minds: Impaired attention switching in recent-onset schizophrenia. PLoS ONE 2013, 8, e78062. [Google Scholar] [CrossRef] [Green Version]
- Crespi, B.; Leach, E.; Dinsdale, N.; Mokkonen, M.; Hurd, P. Imagination in human social cognition, autism, and psychotic-affective conditions. Cognition 2016, 150, 181–199. [Google Scholar] [CrossRef]
- Crespi, B.; Badcock, C. Psychosis and autism as diametrical disorders of the social brain. Behav. Brain Sci. 2008, 31, 241–261. [Google Scholar] [CrossRef]
- Spek, A.A.; Wouters, S.G. Autism and schizophrenia in high functioning adults: Behavioral differences and overlap. Res. Autism Spectr. Disord. 2010, 4, 709–717. [Google Scholar] [CrossRef]
- Brébion, G.; Ohlsen, R.I.; Pilowsky, L.S.; David, A.S. Visual hallucinations in schizophrenia: Confusion between imagination and perception. Neuropsychology 2008, 22, 383. [Google Scholar] [CrossRef]
- Bell, M.; Fiszdon, J.; Richardson, R.; Lysaker, P.; Bryson, G. Are self-reports valid for schizophrenia patients with poor insight? Relationship of unawareness of illness to psychological self-report instruments. Psychiatry Res. 2007, 151, 37–46. [Google Scholar] [CrossRef]
- Karow, A.; Pajonk, F.-G.; Reimer, J.; Hirdes, F.; Osterwald, C.; Naber, D.; Moritz, S. The dilemma of insight into illness in schizophrenia: Self-and expert-rated insight and quality of life. Eur. Arch. Psychiatry Clin. Neurosci. 2008, 258, 152. [Google Scholar] [CrossRef] [PubMed]
- Frith, U.; Happé, F. Theory of mind and self-consciousness: What is it like to be autistic? Mind Lang. 1999, 14, 82–89. [Google Scholar] [CrossRef]
- Mazefsky, C.; Kao, J.; Oswald, D. Preliminary evidence suggesting caution in the use of psychiatric self-report measures with adolescents with high-functioning autism spectrum disorders. Res. Autism Spectr. Disord. 2011, 5, 164–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bishop, S.L.; Seltzer, M.M. Self-reported autism symptoms in adults with autism spectrum disorders. J. Autism Dev. Disord. 2012, 42, 2354–2363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morrier, M.J.; Ousley, O.Y.; Caceres-Gamundi, G.A.; Segall, M.J.; Cubells, J.F.; Young, L.J.; Andari, E. Brief report: Relationship between ADOS-2, module 4 calibrated severity scores (CSS) and social and non-social standardized assessment measures in adult males with autism spectrum disorder (ASD). J. Autism Dev. Disord. 2017, 47, 4018–4024. [Google Scholar] [CrossRef] [PubMed]
- Roestorf, A.; Gaigg, S.; Williams, D.; Bowler, D. Self-Reports vs. Observer Ratings of Autistic Traits: A Comparison of Their Validity over the Adult Lifespan. In Proceedings of the International Society for Autism Research (INSAR) Annual Meeting, Rotterdam, The Netherlands, 9–12 May 2018. [Google Scholar]
- Hull, L.; Petrides, K.; Mandy, W. The female autism phenotype and camouflaging: A narrative review. Rev. J. Autism Dev. Disord. 2020, 1–12. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| ASD Group (n = 35) | SSD Group (n = 64) | NCC (n = 198) | p-Value | |
|---|---|---|---|---|
| Sex, male (%) | 22 (62.9) | 39 (60.9) | 96 (48.5) | 0.1 |
| Age, mean ± SD (range) | 26.15 ± 6.55 (18–45) | 39.10 ± 14.48 (18–77) | 34.01 ± 11.99 (19–67) | <0.001 * |
| Educational level, n (%) | <0.001 * | |||
| Primary school | 0 (0) | 8 (12.5) | 0 (0) | |
| Secondary school | 12 (34.3) | 27 (42.2) | 6 (3) | |
| High school | 18 (5.4) | 23 (35.9) | 24 (12.1) | |
| University | 5 (14.3) | 6 (9.4) | 168 (84.8) | |
| Occupational status, n (%) | <0.001 * | |||
| Full-time | 5 (14.3) | 9 (14.1) | 114 (57.6) | |
| Part-time | 4 (11.4) | 0 (0) | 14 (7.1) | |
| Unemployed | 14 (40) | 41 (64.1) | 11 (5.6) | |
| Student | 12 (34.3) | 8 (12.5) | 54 (27.3) | |
| Retired | 0 (0) | 6 (9.4) | 5 (2.5) | |
| Marital status, n (%) | 0.004 * | |||
| Single | 33 (94.3) | 43 (67.2) | 129 (65.2) | |
| In a domestic partnership | 1 (2.9) | 2 (3.1) | 22 (11.1) | |
| Married | 1 (2.9) | 11 (17.2) | 38 (19.2) | |
| Divorced | 0 (0) | 7 (10.9) | 6 (3) | |
| Widowed | 0 (0) | 1 (1.6) | 3 (1.5) | |
| ADOS-2, mean ± SD | ||||
| Communication | 3.62 ± 1.59 (0–6) | - | - | - |
| Social Interaction | 6.74 ± 2.94 (2–16) | - | - | - |
| Communication + Social Interaction | 10.4 ± 4.23 (2–22) | - | - | - |
| Imagination/Creativity | 0.86 ± 0.65 (0–2) | - | - | - |
| Restricted Interests and Repetitive Behaviors | 1.80 ± 1.30 (0–5) | - | - | - |
| Overall | ASD vs. SSD | ASD vs. NCC | SSD vs. NCC | |||||
|---|---|---|---|---|---|---|---|---|
| AQ Scores, Mean ± SD (range) | ASD (n = 35) | SSD (n = 64) | NCC (n = 198) | F | p | p | p | p |
| AQ total | 25.97 ± 8.09 (6–41) | 23.31 ± 6.03 (12–43) | 15.77 ± 6.75 (3–39) | 53.42 | <0.001 * | 0.15 | <0.001 * | <0.001 * |
| Social skills | 5.06 ± 2.55 (0–10) | 4.02 ± 2.41 (0–10) | 2.44 ± 2.23 (0–9) | 25.73 | <0.001 * | 0.08 | <0.001 * | <0.001 * |
| Attention switching | 6.31 ± 2.42 (0–10) | 5.66 ± 2.00 (1–10) | 4.03 ± 2.15 (0–9) | 25.59 | <0.001 * | 0.32 | <0.001 * | <0.001 * |
| Attention to detail | 4.97 ± 2.17 (1–9) | 4.56 ± 2.22 (1–10) | 4.47 ± 2.21 (0–10) | 0.77 | 0.46 | 0.65 | 0.43 | 0.95 |
| Communication | 5.31 ± 2.31 (0–10) | 4.48 ± 2.21 (1–10) | 2.11 ± 1.93 (0–9) | 58.63 | <0.001 * | 0.13 | <0.001 * | <0.001 * |
| Imagination | 4.31 ± 1.74 (1–7) | 4.59 ± 1.81 (0–8) | 2.73 ± 2.00 (0–10) | 27.74 | <0.001 * | 0.77 | <0.001 * | <0.001 * |
| AUC (95% CI) | Sensitivity | Specificity | PPV | NPV | Cohen’s k | |
|---|---|---|---|---|---|---|
| ASD vs. SSD | 0.63 (0.51–0.75) | 22.9% | 92.2% | 61.5% | 68.6% | 0.04 |
| ASD vs. NCC | 0.84 (0.76–0.92) | 57.1% | 90.4% | 51.3% | 92.3% | 0.45 |
| ADOS-2 | ||||||
|---|---|---|---|---|---|---|
| Communication | Social Interaction | Communication + Social Interaction | Imagination/ Creativity | Repetitive Behaviors | ||
| AQ | Total | −0.09 p = 0.59 | −0.01 p = 0.93 | −0.03 p = 0.84 | −0.09 p = 0.59 | −0.02 p = 0.89 |
| Social skills | −0.32 p = 0.06 | −0.24 p = 0.16 | −0.29 p = 0.09 | −0.28 p = 0.11 | −0.22 p = 0.21 | |
| Attention switching | −0.03 p = 0.87 | −0.01 p = 0.99 | −0.01 p = 0.96 | −0.09 p = 0.59 | 0.1 p = 0.57 | |
| Attention to detail | 0.001 p = 0.99 | −0.05 p = 0.76 | −0.01 p = 0.98 | −0.11 p = 0.54 | 0.03 p = 0.87 | |
| Communication | 0.11 p = 0.53 | 0.03 p = 0.87 | −0.02 p = 0.91 | −0.09 p = 0.59 | −0.15 p = 0.40 | |
| Imagination | 0.21 p = 0.21 | 0.37 p = 0.03 * | 0.35 p = 0.04 * | 0.43 p = 0.01 * | 0.29 p = 0.09 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fusar-Poli, L.; Ciancio, A.; Gabbiadini, A.; Meo, V.; Patania, F.; Rodolico, A.; Saitta, G.; Vozza, L.; Petralia, A.; Signorelli, M.S.; et al. Self-Reported Autistic Traits Using the AQ: A Comparison between Individuals with ASD, Psychosis, and Non-Clinical Controls. Brain Sci. 2020, 10, 291. https://doi.org/10.3390/brainsci10050291
Fusar-Poli L, Ciancio A, Gabbiadini A, Meo V, Patania F, Rodolico A, Saitta G, Vozza L, Petralia A, Signorelli MS, et al. Self-Reported Autistic Traits Using the AQ: A Comparison between Individuals with ASD, Psychosis, and Non-Clinical Controls. Brain Sciences. 2020; 10(5):291. https://doi.org/10.3390/brainsci10050291
Chicago/Turabian StyleFusar-Poli, Laura, Alessia Ciancio, Alberto Gabbiadini, Valeria Meo, Federica Patania, Alessandro Rodolico, Giulia Saitta, Lucia Vozza, Antonino Petralia, Maria Salvina Signorelli, and et al. 2020. "Self-Reported Autistic Traits Using the AQ: A Comparison between Individuals with ASD, Psychosis, and Non-Clinical Controls" Brain Sciences 10, no. 5: 291. https://doi.org/10.3390/brainsci10050291