
Non-Pharmaceutical Interventions for Self-Regulatory Failures in Adolescents Suffering from Externalizing Symptoms: A Scoping Review

 ,
,
Abstract
:1. Introduction
1.1. Externalizing Symptoms
1.2. Self-Regulation Processes
1.3. SR Failures and EXT Symptoms
1.4. Adolescence
1.5. The Current Scoping Review
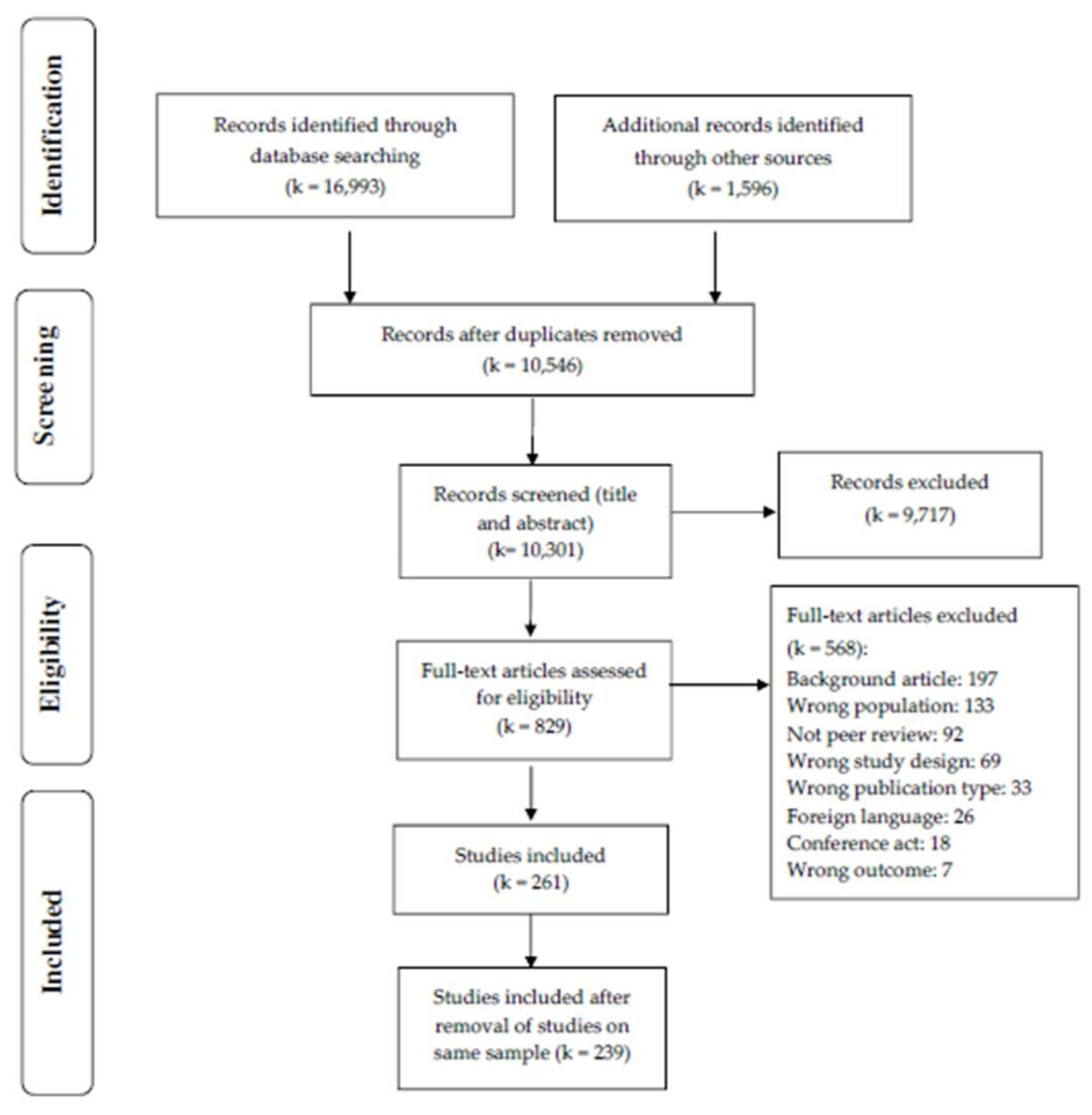
2. Materials and Methods
2.1. Procedure
2.2. Search Strategy
2.3. Study Categorization
2.3.1. Type of Samples
2.3.2. SR Processes
2.3.3. Psychopathological Symptoms
2.3.4. Intervention Type
2.4. Data Synthesis
3. Results
3.1. Descriptive
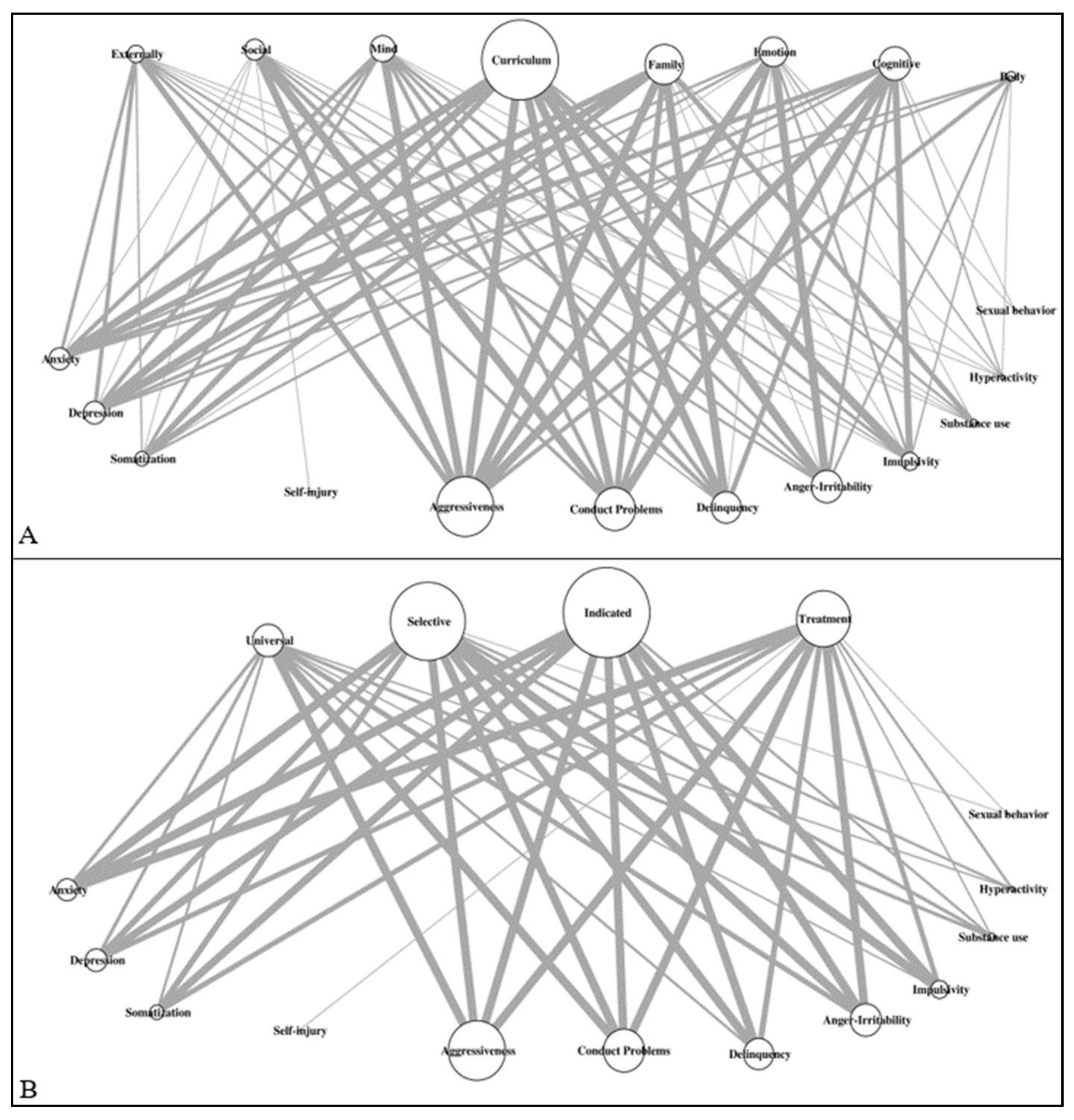
3.2. Crossing Information and Network Analyses
3.2.1. Intervention Stage by Origin
3.2.2. Intervention Stage by Intervention Type
3.2.3. Intervention Type by Psychopathological Symptoms and SR Processes
3.2.4. Intervention Stage by SR Processes and Psychopathological Symptoms
4. Discussion
4.1. Hubs
4.2. Origin Bias and Cultural Aspects
4.3. Gaps and Recommendation of Research Agenda
4.4. Comparison with Previous Reviews and Meta-Analyses
4.5. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Agnew, R. An integrated theory of the adolescent peak in offending. Youth Soc. 2003, 34, 263–299. [Google Scholar] [CrossRef]
- Cohen, M.A.; Piquero, A.R. New evidence on the monetary value of saving a high risk youth. J. Quant. Criminol. 2008, 25, 25–49. [Google Scholar] [CrossRef]
- Storz, R. Evolution de la Délinquance Juvénile: Jugements Pénaux Des Adolescents, de 1946 à 2004; Office Fédérale de la Statistique: Neuchâtel, Switzerland, 2007.
- Campbell, S.B. Behavior problems in preschool children: A review of recent research. J. Child Psychol. Psychiatry 1995, 36, 113–149. [Google Scholar] [CrossRef]
- Fairchild, G.; Passamonti, L.; Hurford, G.; Hagan, C.; von dem Hagen, E.; Van Goozen, S.H.; Goodyer, I.M.; Calder, A.J. Brain structure abnormalities in early-onset and adolescent-onset conduct disorder. Am. J. Psychiatry 2011, 168, 624–633. [Google Scholar] [CrossRef] [Green Version]
- Frick, P.J.; Viding, E. Antisocial behavior from a developmental psychopathology perspective. Dev. Psychopathol. 2009, 21, 1111–1131. [Google Scholar] [CrossRef]
- Frick, P.J.; White, S.F. Research Review: The importance of callous-unemotional traits for developmental models of aggressive and antisocial behavior. J. Child Psychol. Psychiatry 2008, 49, 359–375. [Google Scholar] [CrossRef]
- Moffitt, T.E. Life-course persistent and adolescence-limited antisocial behavior: A 10-year research review and research agenda. In Causes of Conduct Disorder and Juvenile Delinquency; Lahey, B.B., Moffitt, T.E., Caspi, A., Eds.; Guilford: New York, NY, USA, 2003; pp. 49–75. [Google Scholar]
- Moffitt, T.E. Life-course persistent versus adolescence-limited antisocial behavior. In Developemental Psychaphtology, Risk, Disorder, and Adaptation, 2nd ed.; Cicchetti, D., Cohen, J., Eds.; Wiley: New York, NY, USA, 2006; pp. 570–598. [Google Scholar]
- Pardini, D.A.; Frick, P.J. Multiple developmental pathways to conduct disorder: Current conceptualizations and clinical implications. J. Can. Acad. Child Adolesc. Psychiatry 2013, 22, 20–25. [Google Scholar]
- Gottfredson, M.R.; Hirschi, T. A General Theory of Crime; Stanford University Press: Stanford, CA, USA, 1990. [Google Scholar]
- Heatherton, T.F.; Wagner, D.D. Cognitive neuroscience of self-regulation failure. Trends Cogn. Sci. 2011, 15, 132–139. [Google Scholar] [CrossRef] [Green Version]
- Perry, N.B.; Calkins, S.D.; Dollar, J.M.; Keane, S.P.; Shanahan, L. Self-regulation as a predictor of patterns of change in externalizing behaviors from infancy to adolescence. Dev. Psychopathol. 2017, 30, 497–510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vazsonyi, A.T.; Mikuška, J.; Kelley, E.L. It’s time: A meta-analysis on the self-control-deviance link. J. Crim. Justice 2017, 48, 48–63. [Google Scholar] [CrossRef]
- Odgers, C.L.; Moffitt, T.E.; Broadbent, J.M.; Dickson, N.; Hancox, R.J.; Harrington, H.; Poulton, R.; Sears, M.R.; Thomson, W.M.; Caspi, A. Female and male antisocial trajectories: From childhood origins to adult outcomes. Dev. Psychopathol. 2008, 20, 673–716. [Google Scholar] [CrossRef]
- Frick, P.J.; Thornton, L.C. A Brief history of the diagnostic classification of childhood externalizing disorders. In The Wiley Handbook of Developmental Psychopathology; Centifanti, L.C., Williams, D.M., Eds.; Wiley Blackwell: Hoboken, NJ, USA, 2017; pp. 475–495. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Arlington, VA, USA, 2013. [Google Scholar]
- Kotov, R.; Krueger, R.F.; Watson, D.; Achenbach, T.M.; Althoff, R.R.; Bagby, R.M.; Brown, T.A.; Carpenter, W.T.; Caspi, A.; Clark, L.A.; et al. The Hierarchical Taxonomy of Psychopathology (HiTOP): A dimensional alternative to traditional nosologies. J. Abnorm. Psychol. 2017, 126, 454–477. [Google Scholar] [CrossRef] [Green Version]
- Insel, T.R. The NIMH research domain criteria (RDoC) project: Precision medicine for psychiatry. Am. J. Psychiatry 2014, 171, 395–397. [Google Scholar] [CrossRef] [Green Version]
- Coccaro, E.F. Intermittent explosive disorder as a disorder of impulsive aggression for DSM-5. Am. J. Psychiatry 2012, 169, 577–588. [Google Scholar] [CrossRef]
- Nigg, J.T. Annual Research Review: On the relations among self-regulation, self-control, executive functioning, effortful control, cognitive control, impulsivity, risk-taking, and inhibition for developmental psychopathology. J. Child Psychol. Psychiatry 2016, 58, 361–383. [Google Scholar] [CrossRef] [PubMed]
- Porges, S.W. The polyvagal perspective. Biol. Psychol. 2007, 74, 116–143. [Google Scholar] [CrossRef] [PubMed]
- Piquero, A.R.; Jennings, W.G.; Farrington, D.P.; Diamond, B.; Gonzalez, J.M.R. A meta-analysis update on the effectiveness of early self-control improvement programs to improve self-control and reduce delinquency. J. Exp. Criminol. 2016, 12, 249–264. [Google Scholar] [CrossRef]
- Beauchaine, T.P.; Gatzke-Kopp, L.; Mead, H.K. Polyvagal Theory and developmental psychopathology: Emotion dysregulation and conduct problems from preschool to adolescence. Biol. Psychol. 2007, 74, 174–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beauchaine, T.P.; Neuhaus, E.; Brenner, S.L.; Gatzke-Kopp, L. Ten good reasons to consider biological processes in prevention and intervention research. Dev. Psychopathol. 2008, 20, 745–774. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Habersaat, S.; Boonmann, C.; Schmeck, K.; Stéphan, P.; Francescotti, E.; Fegert, J.M.; Perler, C.; Gasser, J.; Schmid, M.; Urben, S. Differences and similarities in predictors of externalizing behavior problems between boys and girls: A 1-year follow-up study. Crim. Justice Behav. 2018, 45, 1852–1870. [Google Scholar] [CrossRef] [Green Version]
- Urben, S.; Stéphan, P.; Habersaat, S.; Francescotti, E.; Fegert, J.M.; Schmeck, K.; Perler, C.; Gasser, J.; Schmid, M. Examination of the importance of age of onset, callous-unemotional traits and anger dysregulation in youths with antisocial behaviors. Eur. Child Adolesc. Psychiatry 2016, 26, 87–97. [Google Scholar] [CrossRef] [Green Version]
- Mantzouranis, G.; Zimmermann, G. Prendre des risques, ça rapporte? Conduites à risques et perception des risques chez des adolescents tout-venant. Neuropsychiatr. De L’enfance Et De L’adolescence 2010, 58, 488–494. [Google Scholar] [CrossRef] [Green Version]
- Steinberg, L. A social neuroscience perspective on adolescent risk-taking. Dev. Rev. 2008, 28, 78–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Somerville, L.H.; Jones, R.M.; Casey, B.J. A time of change: Behavioral and neural correlates of adolescent sensitivity to appetitive and aversive environmental cues. Brain Cogn. 2010, 72, 124–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuhrmann, D.; Knoll, L.J.; Blakemore, S.-J. Adolescence as a sensitive period of brain development. Trends Cogn. Sci. 2015, 19, 558–566. [Google Scholar] [CrossRef] [Green Version]
- Correll, C.U.; Cortese, S.; Croatto, G.; Monaco, F.; Krinitski, D.; Arrondo, G.; Ostinelli, E.G.; Zangani, C.; Fornaro, M.; Estradé, A.; et al. Efficacy and acceptability of pharmacological, psychosocial, and brain stimulation interventions in children and adolescents with mental disorders: An umbrella review. World Psychiatry 2021, 20, 244–275. [Google Scholar] [CrossRef] [PubMed]
- Ipser, J.; Stein, D.J. Systematic review of pharmacotherapy of disruptive behavior disorders in children and adolescents. Psychopharmacology 2006, 191, 127–140. [Google Scholar] [CrossRef] [PubMed]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Grant, M.J.; Booth, A. A typology of reviews: An analysis of 14 review types and associated methodologies. Heal. Inf. Libr. J. 2009, 26, 91–108. [Google Scholar] [CrossRef]
- Munn, Z.; Stern, C.; Aromataris, E.; Lockwood, C.; Jordan, Z. What kind of systematic review should I conduct? A proposed typology and guidance for systematic reviewers in the medical and health sciences. BMC Med Res. Methodol. 2018, 18, 1–9. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daudt, H.M.L.; Van Mossel, C.; Scott, S.J. Enhancing the scoping study methodology: A large, inter-professional team’s experience with Arksey and O’Malley’s framework. BMC Med Res. Methodol. 2013, 13, 48. [Google Scholar] [CrossRef] [Green Version]
- Csardi, G.; Nepusz, T. The igraph software package for complex network research. Int. J. Complex Syst. 2006, 1695, 1–9. [Google Scholar]
- Team R Core. R. A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2018. [Google Scholar]
- World Health Organization. Politiques et Plans Relatifs à la Santé Mentale de L’Enfant et de L’Adolescent; Organisation Mondiale de la Santé: Genève, Switzerland, 2005. [Google Scholar]
- Costello, E.J.; Mustillo, S.; Erkanli, A.; Keeler, G.; Angold, A. Prevalence and development of psychiatric disorders in childhood and adolescence. Arch. Gen. Psychiatry 2003, 60, 837–844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wai-Chung, Y.H. Redressing the geographical bias in social science knowledge. Environ. Plan. A Econ. Space 2001, 33, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Fanelli, D.; Costas, R.; Ioannidis, J.P.A. Meta-assessment of bias in science. Proc. Natl. Acad. Sci. USA 2017, 114, 3714–3719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fanelli, D.; Ioannidis, J.P.A. US studies may overestimate effect sizes in softer research. Proc. Natl. Acad. Sci. USA 2013, 110, 15031–15036. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Völlm, B.A.; Clarke, M.; Herrando, V.T.; Seppänen, A.O.; Gosek, P.; Heitzman, J.; Bulten, E. European Psychiatric Association (EPA) guidance on forensic psychiatry: Evidence based assessment and treatment of mentally disordered offenders. Eur. Psychiatry 2017, 51, 58–73. [Google Scholar] [CrossRef] [Green Version]
- Rowlands, A.; Fisher, M.; Mishra, J.; Nahum, M.; Brandrett, B.; Reinke, M.; Caldwell, M.; Kiehl, K.A.; Vinogradov, S. Cognitive training for very high risk incarcerated adolescent males. Front. Psychiatry 2020, 11, 225. [Google Scholar] [CrossRef] [Green Version]
- Morgan, A.B.; Lilienfeld, S.O. A meta-analytic review of the relation between antisocial behavior and neuropsychological measures of executive function. Clin. Psychol. Rev. 2000, 20, 113–136. [Google Scholar] [CrossRef]
- Ogilvie, J.M.; Stewart, A.L.; Chan, R.C.K.; Shum, D.H.K. Neuropsychological measures of executive function and antisocial behavior: A meta-analysis*. Criminology 2011, 49, 1063–1107. [Google Scholar] [CrossRef] [Green Version]
- Baskin-Sommers, A.R.; Curtin, J.J.; Newman, J.P. Altering the cognitive-affective dysfunctions of psychopathic and externalizing offender subtypes with cognitive remediation. Clin. Psychol. Sci. 2015, 3, 45–57. [Google Scholar] [CrossRef] [Green Version]
- Bootsman, F. Neurobiological intervention and prediction of treatment outcome in the juvenile criminal justice system. J. Crim. Justice 2019, 65, 101554. [Google Scholar] [CrossRef]
- Haapasalo, J.; Tremblay, R.E. Physically aggressive boys from ages 6 to 12: Family background, parenting behavior, and prediction of delinquency. J. Consult. Clin. Psychol. 1994, 62, 1044–1052. [Google Scholar] [CrossRef] [PubMed]
- Pandey, A.; Hale, D.; Das, S.; Goddings, A.-L.; Blakemore, S.-J.; Viner, R.M. Effectiveness of universal self-regulation–based interventions in children and adolescents. A systematic review and meta-analysis. JAMA Pediatr. 2018, 172, 566–575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friese, M.; Frankenbach, J.; Job, V.; Loschelder, D.D. Does self-control training improve self-control? A meta-analysis. Perspect. Psychol. Sci. 2017, 12, 1077–1099. [Google Scholar] [CrossRef]
- Hagger, M.S.; Wood, C.; Stiff, C.; Chatzisarantis, N.L.D. Ego depletion and the strength model of self-control: A meta-analysis. Psychol. Bull. 2010, 136, 495–525. [Google Scholar] [CrossRef] [PubMed]
- Inzlicht, M.; Berkman, E. Six questions for the resource model of control (and some answers). Soc. Pers. Psychol. Compass 2015, 9, 511–524. [Google Scholar] [CrossRef] [Green Version]
- Mason, W.A.; Fleming, C.B.; Ringle, J.L.; Thompson, R.W.; Haggerty, K.P.; Snyder, J.J. Reducing risks for problem behaviors during the high school transition: Proximal outcomes in the common sense parenting trial. J. Child Fam. Stud. 2014, 24, 2568–2578. [Google Scholar] [CrossRef] [Green Version]
- Webster-Stratton, C.; Reid, M.J.; Stoolmiller, M. Preventing conduct problems and improving school readiness: Evaluation of the Incredible Years Teacher and Child Training Programs in high-risk schools. J. Child Psychol. Psychiatry 2008, 49, 471–488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smedler, A.-C.; Hjern, A.; Wiklund, S.; Anttila, S.; Pettersson, A. Programs for prevention of externalizing problems in children: Limited evidence for effect beyond 6 months post intervention. Child Youth Care Forum 2014, 44, 251–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Variables | Categories | n (%) of Studies |
|---|---|---|
| Publication’s year | 1968–1980 | 24 (10.0) |
| 1981–1990 | 32 (13.4) | |
| 1991–2000 | 39 (16.3) | |
| 2001–2010 | 48 (20.1) | |
| 2011–2020 | 96 (40.1) | |
| Study’s origin | North America | 170 (71.1) |
| Europe | 32 (13.4) | |
| Asia | 15 (6.3) | |
| Australia | 12 (5.0) | |
| Africa | 3 (1.3) | |
| South America | 1 (0.4) | |
| Not reported | 6 (2.5) | |
| Study design | Randomized controlled trial | 96 (40.2) |
| Open label | 50 (20.9) | |
| Controlled trial | 42 (17.6) | |
| ABAB design | 17 (7.1) | |
| Single case | 11 (4.6) | |
| Multiple cases | 9 (3.8) | |
| Qualitative | 5 (2.1) | |
| ABBA crossover | 3 (1.3) | |
| Others | 6 (2.5) | |
| Intervention stage | Universal prevention | 30 (12.6) |
| Selective prevention | 75 (31.4) | |
| Indicated prevention | 87 (36.4) | |
| Treatment | 47 (19.7) | |
| Intervention type | Curriculum-based interventions | 75 (31.4) |
| Cognitive-based interventions | 43 (18.0) | |
| Family-based interventions | 27 (11.3) | |
| Emotional-based interventions | 26 (10.9) | |
| Social-based interventions | 24 (10.0) | |
| Mind-based interventions | 21 (8.8) | |
| Externally mediated interventions | 12 (5.0) | |
| Body-based interventions | 11 (4.6) | |
| SR process * | Cognition | 192 (47.7) |
| Emotion | 103 (25.6) | |
| Social | 98 (24.4) | |
| Physiological | 9 (2.2) | |
| EXT symptom * | Aggressiveness | 105 (29.8) |
| Conduct problems | 76 (21.6) | |
| Irritability/anger dysregulation | 57 (16.2) | |
| Delinquency/offending | 55 (15.6) | |
| Impulsivity | 32 (9.1) | |
| Substance use | 16 (4.5) | |
| Hyperactivity | 9 (2.6) | |
| Sexual risky behaviors | 2 (0.6) | |
| INT symptom * | Depressive symptoms | 39 (37.8) |
| Anxiety | 38 (36.9) | |
| Somatization | 25 (24.3) | |
| Self-injurious behaviors | 1 (1.0) |
| Type of Intervention | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Body | Cognitive | Curriculum | Emotional | Externally Mediated | Family | Mind | Social | Total | ||
| Stage | Universal | 1/0.4 | 1/0.4 | 9/3.8 | 2/0.8 | 0/0 | 8/3.3 | 5/2.1 | 4/1.7 | 30/12.6 |
| Selective | 2/0.8 | 17/7.1 | 24/10.0 | 14/5.9 | 4/1.7 | 5/2.1 | 4/1.7 | 5/2.1 | 75/31.4 | |
| Indicated | 6/2.5 | 14/5.9 | 28/11.7 | 5/2.1 | 5/2.1 | 11/4.6 | 7/2.9 | 11/4.6 | 87/36.4 | |
| Treatment | 2/0.8 | 11/4.6 | 14/5.9 | 5/2.1 | 3/1.3 | 3/1.3 | 5/2.1 | 4/1.7 | 47/19.7 | |
| Total | 11/4.5 | 43/18 | 75/31.4 | 26/10.9 | 12/5.1 | 27/11.3 | 21/8.8 | 24/10.1 | 239/100 | |
| Intervention Type | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Body | Cognitive | Curriculum | Emotional | Externally Mediated | Family | Mind | Social | Total | ||
| Self-regulation | Cognition | 7/1.7 | 42/10.4 | 68/17.0 | 14/3.5 | 6/1.5 | 17/4.2 | 19/4.7 | 19/4.7 | 192/47.8 |
| Social | 2/0.5 | 8/2.0 | 33/8.2 | 5/1.2 | 7/1.7 | 21/5.2 | 4/1.0 | 18/4.5 | 98/24.4 | |
| Emotion | 5/1.2 | 9/2.2 | 36/9.0 | 23/5.7 | 9/2.2 | 9/2.2 | 11/2.7 | 1/0.2 | 103/25.6 | |
| Physiological | 5/1.2 | 0/0 | 2/0.5 | 1/0.2 | 0/0 | 0/0 | 1/0.2 | 0/0 | 9/2.2 | |
| Total | 19/4.7 | 59/14.7 | 139/34.6 | 43/10.7 | 22/5.5 | 47/11. | 35/8.7 | 38/9.4 | 402/100 | |
| Symptoms | Aggressiveness | 5/1.1 | 12/2.6 | 34/7.5 | 12/2.6 | 7/1.5 | 14/3.1 | 12/2.6 | 9/2.0 | 105/23.2 |
| Conduct problems | 0/0 | 12/2.6 | 27/6.0 | 7/1.5 | 4/0.9 | 8/1.8 | 6/1.3 | 12/2.6 | 76/16.8 | |
| Delinquency | 0/0 | 6/1.3 | 19/4.2 | 1/0.2 | 2/0.4 | 16/3.5 | 5/1.1 | 5/1.1 | 54/11.9 | |
| Hyperactivity | 1/0.2 | 2/0.4 | 0/0 | 2/0.4 | 1/0.2 | 1/0.2 | 2/0.4 | 0/0 | 9/2.0 | |
| Impulsivity | 2/0.4 | 8/1.8 | 11/2.4 | 3/0.7 | 1/0.2 | 1/0.2 | 4/0.9 | 2/0.4 | 32/7.1 | |
| Irritability/anger dys. | 3/0.7 | 4/0.9 | 21/4.6 | 17/3.8 | 3/0.7 | 1/0.2 | 4/0.9 | 3/0.7 | 56/12.4 | |
| Substance use | 0/0 | 0/0 | 4/0.9 | 1/0.2 | 1/0.2 | 8/1.8 | 1/0.2 | 1/0.2 | 16/3.5 | |
| Sexual risky behaviors | 0/0 | 1/0.2 | 0/0 | 1/0.2 | 0/0 | 0/0 | 0/0 | 0/0 | 2/0.4 | |
| Self-injurious behaviors | 0/0 | 0/0 | 0/0 | 0/0 | 0/0 | 0/0 | 0/0 | 1/0.2 | 1/0.2 | |
| Anxiety | 3/0.7 | 6/1.3 | 9/2.0 | 3/0.7 | 4/0.9 | 7/1.5 | 5/1.1 | 1/0.2 | 38/8.4 | |
| Depressive symptoms | 3/0.7 | 4/0.9 | 9/2.0 | 3/0.7 | 5/1.1 | 9/2.0 | 5/1.1 | 1/0.2 | 39/8.6 | |
| Somatization | 0/0 | 3/0.7 | 7/1.5 | 1/0.2 | 2/0.4 | 7/1.5 | 4/0.9 | 1/0.2 | 25/5.5 | |
| Total | 17/3.8 | 58/12.8 | 141/31.1 | 51/11.3 | 30/6.6 | 72/15.9 | 48/10.6 | 36/7.9 | 453/100 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Constanty, L.; Lepage, C.; Rosselet Amoussou, J.; Wouters, E.; Decoro, V.; De-Paz, L.; Hans, C.; Ergüneş, H.; Sangra, J.; Plessen, K.J.; et al. Non-Pharmaceutical Interventions for Self-Regulatory Failures in Adolescents Suffering from Externalizing Symptoms: A Scoping Review. Biomedicines 2021, 9, 1081. https://doi.org/10.3390/biomedicines9091081
Constanty L, Lepage C, Rosselet Amoussou J, Wouters E, Decoro V, De-Paz L, Hans C, Ergüneş H, Sangra J, Plessen KJ, et al. Non-Pharmaceutical Interventions for Self-Regulatory Failures in Adolescents Suffering from Externalizing Symptoms: A Scoping Review. Biomedicines. 2021; 9(9):1081. https://doi.org/10.3390/biomedicines9091081
Chicago/Turabian StyleConstanty, Lauriane, Caroline Lepage, Joëlle Rosselet Amoussou, Emilie Wouters, Velia Decoro, Lisa De-Paz, Charlotte Hans, Hazal Ergüneş, Jonas Sangra, Kerstin Jessica Plessen, and et al. 2021. "Non-Pharmaceutical Interventions for Self-Regulatory Failures in Adolescents Suffering from Externalizing Symptoms: A Scoping Review" Biomedicines 9, no. 9: 1081. https://doi.org/10.3390/biomedicines9091081