Phase 2 and Later of COVID-19 Lockdown: Is it Possible to Perform Remote Diagnosis and Intervention for Autism Spectrum Disorder? An Online-Mediated Approach

{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Material and Methods
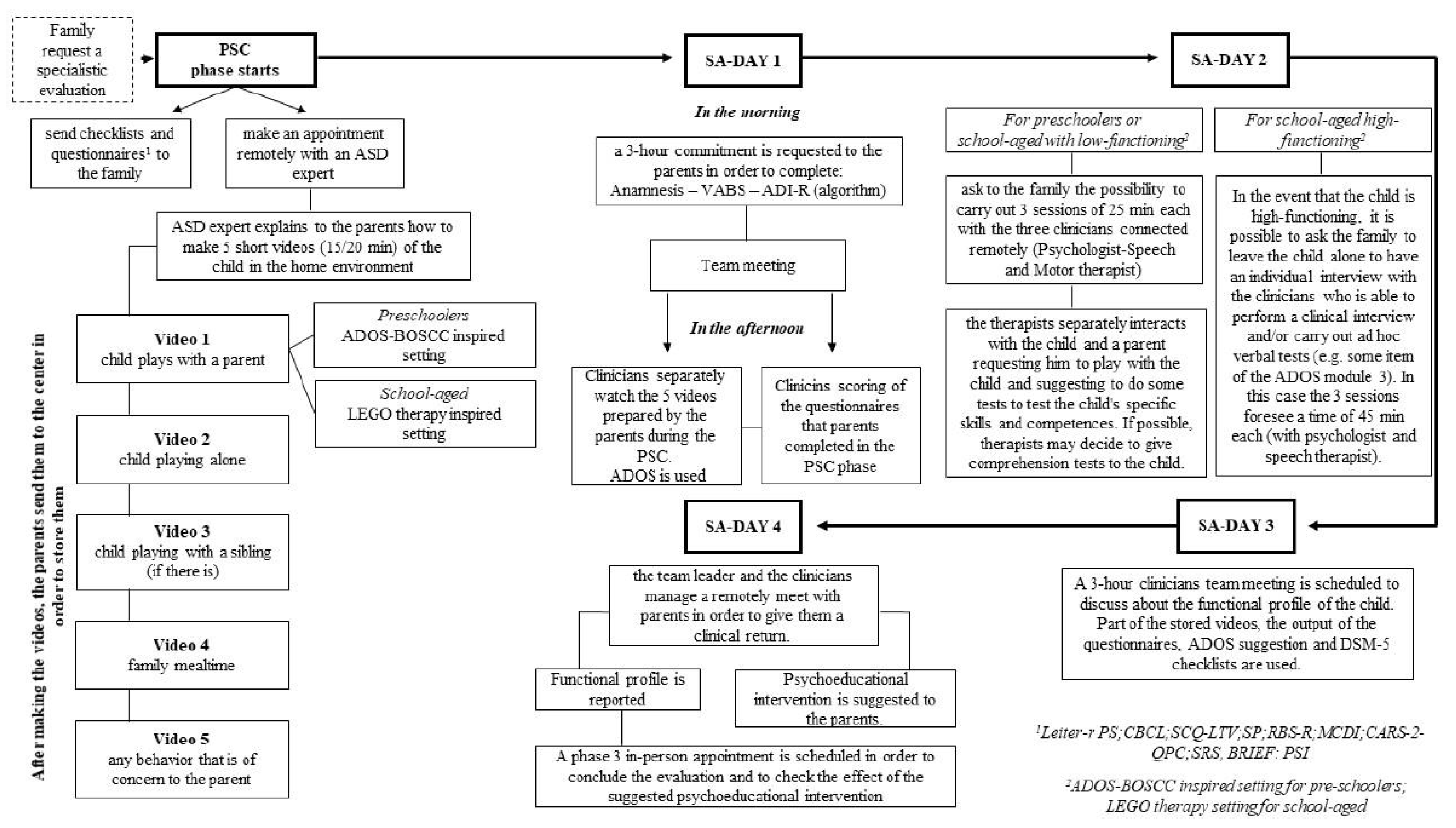
2.1. A Telemedicine Working Model for Diagnosis
2.1.1. Pre-Specialistic Consultation (PSC)
2.1.2. Questionnaire and Checklists
2.1.3. Meeting with an Expert Psychologist in the Field of the Diagnosis of ASD
2.2. Specialistic Assessment (SA)
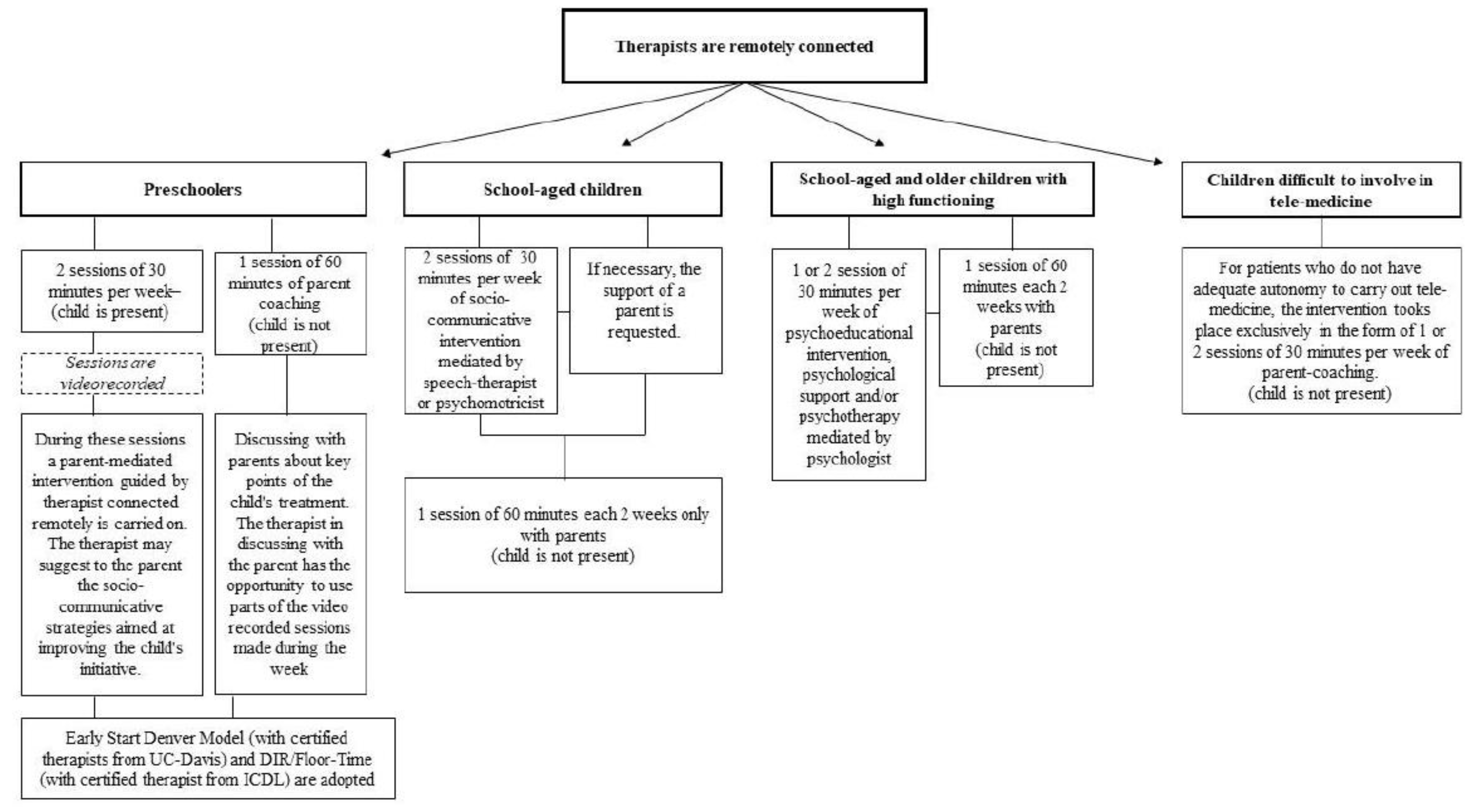
3. A Telemedicine Working Model for Intervention
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Narzisi, A. Handle the Autism Spectrum Condition during Coronavirus (COVID-19) Stay at Home period: Ten Tips for Helping Parents and Caregivers of Young Children. Brain Sci. 2020, 1, 10. [Google Scholar]
- Maenner, M.J.; Shaw, K.A.; Baio, J.; Washington, A.; Patrick, M.; DiRienzo, M.; Christensen, D.L.; Wiggins, L.D.; Pettygrove, S.; Andrews, J.G.; et al. Prevalence of Autism Spectrum Disorder Among Children Aged 8 Years—Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2016. Mmwr Surveill. Summ. 2020, 69, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Narzisi, A.; Posada, M.; Barbieri, F.; Chericoni, N.; Ciuffolini, D.; Pinzino, M.; Romano, R.; Scattoni, M.L.; Tancredi, R.; Calderoni, S.; et al. Prevalence of Autism Spectrum Disorder in a large Italian catchment area, A school-based population study within the ASDEU project. Epidemiol. Psychiatr. Sci. 2018, 29, e5. [Google Scholar] [CrossRef] [PubMed]
- Juárez, A.P.; Weitlauf, A.S.; Nicholson, A.; Pasternak, A.; Broderick, N.; Hine, J.; Stainbook, J.A.; Warren, Z. Early Identification of ASD through Telemedicine: Potential Value for Underserved Populations. J. Autism Dev. Disord. 2018, 48, 2601–2610. [Google Scholar] [CrossRef] [PubMed]
- Sutherland, R.; Trembath, D.; Hodge, M.A.; Rose, V.; Roberts, J. Telehealth and autism: Are telehealth language assessments reliable and feasible for children with autism? Int. J. Lang. Commun. Disord. 2019, 54, 281–291. [Google Scholar] [CrossRef]
- Smith, C.; Rozga, A.; Matthews, N.; Oberleitner, R.; Nazneen, N.; Abowd, G. Investigating the accuracy of a novel telehealth diagnostic approach for Autism Spectrum Disorder. Psychol Assess. 2017, 29, 245–252. [Google Scholar] [CrossRef]
- Nazneen, N.; Rozga, A.; Smith, C.; Oberleitner, R.; Abowd, G.; Arriaga, R. A Novel System for Supporting Autism Diagnosis Using Home Videos: Iterative Development and Evaluation of System Design. J. Mir Mhealth Uhealth. 2015, 3, e68. [Google Scholar] [CrossRef] [Green Version]
- Sutantio, J.D.; Pusponegoro, H.D.; Sekartini, R. Validity of Telemedicine for Diagnosing Autism Spectrum Disorder: Protocol-Guided Video Recording Evaluation. Telemed. E-Health 2020. [Google Scholar] [CrossRef]
- Fusaro, V.A.; Daniels, J.; Duda, M.; DeLuca, T.F.; D’Angelo, O.; Tamburello, J.; Maniscalco, J.; Wall, D.P. The Potential of Accelerating Early Detection of Autism through Content Analysis of YouTube Videos. PLoS ONE 2014, 9, e93533. [Google Scholar] [CrossRef] [Green Version]
- Lord, C.; Luyster, R.; Gotham, K.; Guthrie, W. (ADOS-2) Manual (Part II): Toddler Module. In Autism Diagnostic Observation Schedule, 2nd ed.; Western Psychological Services: Torrence, CA, USA, 2012. [Google Scholar]
- Johnsson, G.; Kerslake, R.; Crook, S. Delivering allied health services to regional and remote participants on the autism spectrum via video-conferencing technology: Lessons learned. Rural Remote Health. 2019, 19, 5358. [Google Scholar] [CrossRef] [Green Version]
- Carter, A.S.; Messinger, D.S.; Stone, W.L.; Celimli, S.; Nahmias, A.S.; Yoder, P. Randomized controlled trial of Hanen’s ‘More Than Words’ in toddlers with early autism symptoms. Child Psychol. Psychiatry 2011, 52, 741–752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bearss, K.; Burrell, T.L.; Challa, S.A.; Postorino, V.; Gillespie, S.E.; Crooks, C.; Scahill, L. Feasibility of Parent Training via Telehealth for Children with Autism Spectrum Disorder and Disruptive Behavior: A Demonstration Pilot. J. Autism Dev. Disord. 2018, 48, 1020–1030. [Google Scholar] [CrossRef] [PubMed]
- Vismara, L.; McCormick, C.; Wagner, A.; Monlux, K.; Nadhan, A.; Young, G. Telehealth Parent Training in the Early Start Denver Model: Results From a Randomized Controlled Study. Focus Autism Other Dev. Disabil. 2018, 33, 2. [Google Scholar] [CrossRef]
- Green, J.; Charman, T.; McConachie, H.; Aldred, C.; Slonims, V.; Howlin, P.; Le Couteur, A.; Leadbitter, K.; Hudry, K.; Byford, S.; et al. Parent-mediated communication-focused treatment in children with autism (PACT): A randomised controlled trial. Lancet 2010, 19, 2152–2160. [Google Scholar] [CrossRef] [Green Version]
- Roid, G.L. Leiter international performance scale-revised: Examiner’s manual. In Leiter International Performance Scale-Revised; Roid, G.H., Miller, L.J., Eds.; Stoelting: Wood Dale, IL, USA, 1997. [Google Scholar]
- Greene, J.A.; Trujillo, S.; Isquith, P.K.; Gioia, G.A.; Espy, K.A. Enhanced Interpretation of the Behavior Rating Inventory of Executive Function–Preschool Version (BRIEF-P) (White Paper); PAR: Lutz, FL, USA, 2019. [Google Scholar]
- Gioia, G.A.; Isquith, P.K.; Guy, S.C.; Kenworthy, L. Behavior Rating Inventory of Executive Function® (BRIEF®2), 2nd, ed.; PAR Inc.: Lutz, FL, USA, 2015. [Google Scholar]
- Achenbach, T.M.; Rescorla, L. Manual for the ASEBA Preschool Forms and Profile; Univeristy of Vermont: Burlington, VT, USA, 2000. [Google Scholar]
- Fenson, L.; Pethick, S.; Renda, C.; Cox, J.L.; Dale, P.S.; Reznick, J.S. Short-form versions of the MacArthur Communicative Developmental Inventories. Appl. Psycholinguist. 2000, 21, 95–116. [Google Scholar] [CrossRef]
- Schopler, E.; Van Bourgondien, M.E.; Wellman, G.J.; Love, S.R. Childhood Autism Rating Scale, 2nd ed.; Western Psychological Services: Los Angeles, CA, USA, 2010. [Google Scholar]
- Lam, K.S.; Aman, M.G. The Repetitive Behavior Scale-Revised: Independent validation in individuals with autism spectrum disorders. J. Autism Dev. Disord. 2007, 37, 855–866. [Google Scholar] [CrossRef] [PubMed]
- Rutter, M.; Bailey, A.; Lord, C. Social Communication Questionnaire (SCQ) Manual; Western Psychological Services: Los Angeles, CA, USA, 2000. [Google Scholar]
- Dunn, W. Sensory Profile; Harcourt Assessment: San Antonio, TX, USA, 1999. [Google Scholar]
- James, K.; Lucy, J.; Millera, L.J.; Schaaf, R.; Nielsene, D.M.; Schoena, S.A. Phenotypes within sensory modulation dysfunction. Compr. Psychiatry 2011, 52, 715–724. [Google Scholar] [CrossRef] [PubMed]
- Constantino, J.; Gruber, J. Social Responsiveness Scale (SRS) Manual; Western Psychological Services: Los Angeles, CA, USA, 2005. [Google Scholar]
- Abidin, R.R. Parenting Stress Index, 4th ed.; PAR: Lutz, FL, USA, 2012. [Google Scholar]
- Grzadzinski, R.; Carr, T.; Colombi, C.; McGuire, K.; Dufek, S.; Pickles, A.; Lord, C. Measuring Changes in Social Communication Behaviors: Preliminary Development of the Brief Observation of Social Communication Change (BOSCC). J. Autism Dev. Disord. 2016, 46, 2464–2479. [Google Scholar] [CrossRef] [Green Version]
- Ausderau, K.K.; St John, B.; Kwaterski, K.N.; Nieuwenhuis, B.; Bradley, E. Parents’ Strategies to Support Mealtime Participation of Their Children With Autism Spectrum Disorder. Am. J. Occup. Ther. 2019, 73, 7301205070p1–7301205070p10. [Google Scholar] [CrossRef]
- Peckett, H.; MacCallum, F.; Knibbs, J. Maternal experience of Lego Therapy in families with children with autism spectrum conditions: What is the impact on family relationships? Autism 2016, 20, 879–887. [Google Scholar] [CrossRef] [Green Version]
- Lord, C.; Rutter, M.; Le Couteur, A. Autism Diagnostic Interview-Revised: A revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders. J. Autism Dev. Disord. 1994, 24, 659–685. [Google Scholar] [CrossRef] [PubMed]
- Sparrow, S.S.; Balla, D.A.; Cicchetti, D.V.; Doll, E.D. Vineland-II: Vineland Adaptive Behavior Scales: Survey Forms Manual; American Guidance Service: Circle Pines, MN, USA, 2005. [Google Scholar]
- Balboni, G.; Tasso, A.; Muratori, F.; Cubelli, R. The Vineland-II in preschool children with Autism Spectrum Disorders: An item content category analysis. J. Autism Dev. Disord. 2016, 46, 42–52. [Google Scholar] [CrossRef] [PubMed]
- Balboni, G.; Belacchi, C.; Bonichini, S.; Coscarelli, A. Vineland-II. Vineland Adaptive Behavior Scales Second Edition Survey Interview Form; Giunti OS Organizzazioni Speciali: Firenze, Italy, 2016. [Google Scholar]
- Gotham, K.; Risi, S.; Pickles, A.; Lord, C. The Autism Diagnostic Observation Schedule: Revised Algorithms for Improved Diagnostic Validity. J. Autism Dev. Disord. 2007, 37, 613–627. [Google Scholar] [CrossRef] [PubMed]
- Schutte, J.L.; McCue, M.P.; Parmanto, B.; McGonigle, J.; Handen, B.; Lewis, A.; Pulantara, I.W.; Saptono, A. Usability and Reliability of a Remotely Administered Adult Autism Assessment, the Autism Diagnostic Observation Schedule (ADOS) Module 4. Telemed J. E Health 2015, 21, 176–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- APA. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Schreibman, L.; Dawson, G.; Stahmer, A.C.; Landa, R.; Rogers, S.J.; McGee, G.G.; Kasari, C.; Ingersoll, B.; Kaiser, A.P.; Bruinsma, Y.; et al. Naturalistic Developmental Behavioral Interventions: Empirically Validated Treatments for Autism Spectrum Disorder. J. Autism Dev. Disord. 2015, 45, 2411–2428. [Google Scholar] [CrossRef] [Green Version]
- Dawson, G.; Rogers, S.; Munson, J.; Smith, M.; Winter, J.; Greenson, J.; Donaldson, A.; Varley, J. Randomized, controlled trial of an intervention for toddlers with autism: The Early Start Denver Model. Pediatrics 2010, 125, e17–e23. [Google Scholar] [CrossRef] [Green Version]
- Colombi, C.; Narzisi, A.; Ruta, L.; Cigala, V.; Gagliano, A.; Pioggia, G.; Siracusano, R.; Rogers, S.J.; Muratori, F.; Prima Pietra Team. Implementation of the Early Start Denver Model in an Italian community. Autism 2018, 22, 126–133. [Google Scholar] [CrossRef]
- Greenspan, S.I.; Wieder, S.; Simons, R. The Child with Special Needs: Encouraging Intellectual and Emotional Growth; Addison-Wesley/Addison Wesley Longman: Boston, MA, USA, 1998. [Google Scholar]
- Rogers, S.J.; Dawson, G.; Vismara, L.A. An Early Start for Your Child with Autism: Using Everyday Activities to Help Kids Connect, Communicate, and Learn; Guilford Press: New York, NY, USA, 2012. [Google Scholar]
- Towey, M.P. Speech Telepractice: Installing a Speech Therapy Upgrade for the 21st Century. Int. J. Telerehabilitation 2012, 4, 73–78. [Google Scholar] [CrossRef] [Green Version]
- Lai, M.C.; Kassee, C.; Besney, R.; Bonato, S.; Hull, L.; Mandy, W.; Szatmari, P.; Ameis, S.H. Prevalence of co-occurring mental health diagnoses in the autism population: A systematic review and meta-analysis. Lancet Psychiatry 2019, 6, 819–829. [Google Scholar] [CrossRef]
- CASP. The Council of Autism. Organizational Guidelines and Standards. Available online: www.casproviders.org (accessed on 21 May 2020).
- Parsons, D.; Cordier, R.; Vaz, S.; Lee, H.C. Parent-Mediated Intervention Training Delivered Remotely for Children With Autism Spectrum Disorder Living Outside of Urban Areas: Systematic Review. J. Med. Internet Res. 2017, 14, e198. [Google Scholar] [CrossRef]
- Hepburn, S.L.; Blakeley-Smith, A.; Wolff, B.; Reaven, J.A. Telehealth delivery of cognitive-behavioral intervention to youth with autism spectrum disorder and anxiety: A pilot study. Autism 2016, 20, 207–218. [Google Scholar] [CrossRef] [PubMed]
- Ingersoll, B.; Berger, N.I. Parent Engagement with a Telehealth-Based Parent-Mediated Intervention Program for Children with Autism Spectrum Disorders: Predictors of Program Use and Parent Outcomes. J. Med. Internet Res. 2015, 6, e227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Townsend, E.; Nielsen, E.; Allister, R.; Cassidy, S.A. Key ethical questions for research during the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 381–383. [Google Scholar] [CrossRef]
- Stainbrook, J.A.; Weitlauf, A.S.; Juárez, A.P.; Taylor, J.L.; Hine, J.; Broderick, N.; Nicholson, A.; Zachary, W. Measuring the service system impact of a novel telediagnostic service program for young children with autism spectrum disorder. Autism 2019, 23, 1051–1056. [Google Scholar] [CrossRef]


© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Narzisi, A. Phase 2 and Later of COVID-19 Lockdown: Is it Possible to Perform Remote Diagnosis and Intervention for Autism Spectrum Disorder? An Online-Mediated Approach. J. Clin. Med. 2020, 9, 1850. https://doi.org/10.3390/jcm9061850
Narzisi A. Phase 2 and Later of COVID-19 Lockdown: Is it Possible to Perform Remote Diagnosis and Intervention for Autism Spectrum Disorder? An Online-Mediated Approach. Journal of Clinical Medicine. 2020; 9(6):1850. https://doi.org/10.3390/jcm9061850
Chicago/Turabian StyleNarzisi, Antonio. 2020. "Phase 2 and Later of COVID-19 Lockdown: Is it Possible to Perform Remote Diagnosis and Intervention for Autism Spectrum Disorder? An Online-Mediated Approach" Journal of Clinical Medicine 9, no. 6: 1850. https://doi.org/10.3390/jcm9061850