 Xiaoqun Liu1
Xiaoqun Liu1 Chang Peng
Chang Peng Yizhen Yu
Yizhen Yu- 1Department of Maternal and Child Health, Xiangya School of Public Health, Central South University, Changsha, China
- 2Department of Maternal, Child and Adolescent Health, School of Public Health, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China
- 3Department of Student Affairs, Hunan University of Finance and Economics, Changsha, China
- 4Institute of Higher Education, Hunan University of Science and Engineering, Yongzhou, China
- 5Institute of Education, Hunan Agricultural University, Changsha, China
Sibling bullying is a common phenomenon in childhood and adolescence worldwide and has a significant association with mental health distress. However, there have been few studies that have examined the associations between any specific sub-type of sibling bullying and depression as well as anxiety. Besides, the association between sibling bullying and psychological well-being was never explored among the Chinese population. The purpose of this cross-sectional study was to examine the associations between the number of sub-types of sibling bullying involvement and depression as well as anxiety among Chinese children and adolescents. Multi-stage stratified cluster sampling was used to recruit 5,926 participants aged 10 to 18 who had at least one sibling living in the household. Different sub-types of sibling bullying involvement were determined by using Olweus Bully/Victim Questionnaire (OBVQ). The nine-item Patient Health Questionnaire (PHQ-9) and the seven-item Generalized Anxiety Disorder Scale (GAD-7) were used to screen clinical ranges of major depression and generalized anxiety disorder, respectively. Of the participants, 1,235 (20.8%) were bullied by siblings, and 1,230 (20.8%) perpetrated bullying behavior against siblings over the past 6 months. After controlling potential confounders, adjusted model of logistic regression analyses indicated that all three sub-types of sibling victimization and perpetration were significantly associated with both depression and anxiety. There were linear associations between the number of sub-types of sibling bullying victimization and depression (adjusted OR = 1.49, 95% CI 1.32 to 1.68) as well as anxiety (adjusted OR = 1.68, 95% CI 1.48 to 1.90). Besides, linear trends were found between the number of sub-types of sibling bullying perpetration and depression (adjusted OR = 1.44, 95% CI 1.26 to 1.64) as well as anxiety (adjusted OR = 1.63, 95% CI 1.42 to 1.87). The findings underline dose–response relationships between the number of sub-types of sibling bullying involvement and mental health distress. Intervention programs should be conducted to focus on developing mental health status of those children and adolescents who are involved in multiple sub-types of sibling victimization or perpetration.
Introduction
Sibling bullying refers to any unwanted, repeated, and harmful aggressive behavior among siblings (1), and it encompasses three major sub-types, including verbal (e.g., name-calling, teasing), physical (e.g., kicking, hitting), and relational (e.g., excluding from social situation, spreading rumors) bullying (2, 3). Compared to a substantial body of studies related to peer bullying, bullying behavior among siblings has received less research attention (4, 5). However, if all sub-types are considered, the prevalence of sibling bullying is much higher than that of peer bullying, which is perpetrated by a peer or a group of peers (6, 7). According to a systematic review including four quantitative studies conducted in different countries, nearly 50% of children are involved in sibling bullying every month, and 16% to 20% of them experience sibling bullying more than once a week (7–9). Though sibling bullying is usually considered by the parents as a normal or harmless phenomenon (10, 11), there is ample evidence that sibling bullying increases the odds of reporting a number of psychological and adjustment problems in childhood or early adulthood, which include depression (12, 13), anxiety (14, 15), emotional and conduct problems (9, 16), self-harm behavior (13), and even suicide (12). In addition, given the overlap of sibling and peer interactions in childhood and adolescence, previous studies have found that sibling bullying has significant association with peer bullying (3, 6).
Depression and anxiety are two of the most common psychiatric symptoms (17, 18). Many research studies have examined the associations between sibling bullying and depression or anxiety on the overall experiences of victimization (being bullied by siblings) or perpetration (perpetrating bullying behaviors to siblings) (13, 19). Yet, there were few studies to examine the associations based on any specific sub-type of sibling bullying involvement (15, 20). The previous studies suggest that associations between peer bullying and mental health problems are varied and complex since peer bullying involvement was categorized into different sub-types, including verbal, physical, and relational bullying (21, 22). In a cross-sectional study, Yen et al. found that only physical peer victimization was significantly associated with all dimensions of anxiety symptoms (17). Therefore, there is an important clinical implication to explore whether different sub-types of sibling bullying have distinct or similar association with depression as well as anxiety.
Existing literature has shown that there is a dose–effect relationship between the frequency of sibling bullying involvement and mental health distress. Indeed, those children and adolescents who were involved in sibling bullying victimization or perpetration several times a month or a week were at a particular risk of suffering psychological distress compared with those who never experienced sibling bullying or were involved in sibling bullying only ever once or twice (13, 19). Likewise, involvement in both sibling and peer victimization exhibited a dose–response association with psychological problems (6), with those were bullied both at home and at school having the highest odds for psychotic disorder (19). However, to the best of our knowledge, there is no study to explore the association between the number of sub-types of sibling bullying involvement and mental health problems. A previous study indicated that children and adolescents who were involved in multiple sub-types of sibling bullying victimization had reported greater mental health distress compared with those who experienced only one sub-type of sibling bullying victimization (15), and the effects seem to be cumulative (3). From this perspective, it is reasonable to explore if there is a dose–response association between the number of sub-types of sibling bullying involvement and depression or anxiety.
Aggressive behavior between siblings being a common form of family violence in childhood and adolescence worldwide and the fact that sibling bullying involvement can predict mental health problems (1, 23), in eastern countries, a small group of studies have analyzed the prevalence and risk of bullying, aggression, or violence betweem siblings (24, 25). Besides, there is no previous literature that has examined the link between sibling bullying and psychological well-being among a Chinese population (26). Although the one-child policy had been in effect in China since 1980, the implementation of the policy was less stringent in rural areas. People who lived in remote regions might be allowed to have more than one child when their first child was a girl or a disabled boy (27). On the other hand, the one-child policy was replaced by a universal two-child policy in 2015, and the number of families with two or more kids in both rural and urban areas is expected to increase reasonably (28). Therefore, it is necessary to explore the characteristics and potential risks of sibling bullying among Chinese population.
Taken together, there is a paucity of studies considering the association between different sub-types of sibling bullying involvement and mental health distress. Hence, we conducted a cross-sectional study with a large sample of Chinese children and adolescents to investigate (1) associations between three major sub-types (verbal, physical, and relational) of sibling bullying involvement (victimization and perpetration) and mental health distress (depression and anxiety) as well as (2) the associations between the number of sub-types of sibling bullying involvement and depression as well as anxiety. To this effect, we made some hypotheses: (1) all three major sub-types of sibling bullying have significant associations with mental health distress; and (2) there might be dose–response associations between the number of sub-types of sibling bullying involvement and depression as well as anxiety.
Materials and Methods
Procedures
This study was a cross-sectional survey conducted from April to July 2018. The participants were recruited from Hunan Province, China, by using multi-stage cluster sampling. We used a geography-based stratified sampling frame, which included three cities selected randomly from southern, central, and northern parts of the province, respectively. Three junior high schools and three senior high schools were selected randomly from each chosen city, and all the students of grade 7 to 12 were invited to the research. Before the field investigation, we requested permission from the principals of each school. Once the permissions were granted, investigators conducted the research in each class with the help of the form teachers. All participants signed informed consent forms, and the purpose of the study as well as the questionnaire sections were explained to them by investigators. The students were assured of the anonymity and confidentiality of the information provided in the self-reported questionnaires, and the respondents were free to discontinue their participation at any time of the study. The study received the approval from the ethical committee of Xiangya School of Public Health, Central South University.
The data collection was carried out by double input and through logical verification and sampling inspection of 10% of the input data to control the quality of data collection. If there was a problem with the input data, the researcher would check the original questionnaires in time to ensure the accuracy and reliability of the data.
Participants
Questionnaires were sent out to 8,918 students from 18 sampled schools; of these, 8,520 (95.5%) completed the survey without apparent logical errors, and missing items were fewer than 15% of those in the questionnaire. Participants with no siblings (N = 2,415) and those aged 18 or above (N = 179) were excluded. The current study focused on 5,926 children and adolescents aged 10 to 18 who had at least one brother or sister living in the household at the time of the survey. Of the sample, 2,667 were boys (45.0%) and 3,259 were girls (55.0%). The average age was 14.55 ± 1.63. Most participants lived in a two-parent family (89.9%), while 566 children were from a single-parent family or other (9.6%). Of the 5,926 students, 4,518 had one sibling (76.2%), 1,114 had two siblings (18.8%), and 294 had three or more siblings (5.0%). Furthermore, 2,815 were the first child of their family (47.5%), 2,641 were the second-born child (44.6%), and 446 were the third-born or other birth order child in the household (7.5%).
Assessment of Sibling and Peer Bullying
Sibling bullying was surveyed via the Chinese version of Olweus Bully/Victim Questionnaire (OBVQ). First, participants were provided with a definition of bullying according to Olweus that sibling bullying refers to any unwanted, repeated, and harmful aggressive behavior among siblings (29). Second, sibling bulling victimization was assessed by asking the participants whether they had ever been bullied by siblings in the last 6 months using the following six items: (1) having been hit, kicked, pushed, or shoved; (2) having belongings been taken or damaged; (3) having been called nasty name; (4) having been made fun of; (5) having been kept out of things on purpose, excluded from the group, or completely ignored; or (6) having had lies or rumors been spread about you and/or having had their sibling(s) try to make others dislike you. Then, sibling bullying perpetration was measured by asking whether the participant had even bullied their sibling(s) over the past half a year using the six items above. Items (1) and (2) relate to physical sibling bullying, (3) and (4) relate to verbal sibling bullying, and (5) and (6) relate to relational sibling bullying. The frequency was coded on a five-point scale ranging from 1 to 5 (1= never happened, 2 = only once or twice, 3 = two or three times a month, 4 = about once a week, and 5 = several times a week) (30). Children and adolescents were considered to be involved in any sub-type of sibling bullying victimization or perpetration if the frequency of bullying behavior mentioned above happened more than two or three times a month (2, 19).
For the status of sibling bullying, a pure victim was defined as his/her being involving in victimization but not engaging in perpetration, a pure bully was classified as his/her perpetrating bullying behavior but not being bullied, and a bully-victim was defined as his/her experiencing both victimization and perpetration of bullying. Those who neither bullied siblings nor were bullied by siblings were classified as “non-involved” (31).
Peer bullying was assessed by the Chinese version of OBVQ in the same way as sibling bullying, while the questions were adjusted for bullying behaviors between peers. Participants were asked whether they have had other students or friends bully them and had they ever bullied other students or their friends in the last 6 months using the six items as mentioned above. The Chinese version of Olweus Bully/Victim Questionnaire showed good reliability according to the existing literature (32).
In this study, the range of the internal consistency reliability (alpha Cronbach) for sub-scales of sibling bullying is from 0.76 to 0.83, and the Cronbach's alpha for sub-scales of peer bullying ranged from 0.77 to 0.84.
Depression
The Chinese version of the nine-item Patient Health Questionnaire (PHQ-9) was used to screen depression of participants (33). The PHQ-9 has nine questions with a score ranging from 0 to 3 for each item and total score ranging from 0 to 27. A higher score indicates that the participant has more depressive symptoms. A total score of 10 or more is considered to meet the clinical range of major depression (1 = Yes, 0 = No) (34, 35). The prior study showed good reliability of the Chinese version of PHQ-9 in children and adolescent population (36). In the present study, the Cronbach's alpha of PHQ-9 was 0.88.
Anxiety
The Chinese version of the seven-item Generalized Anxiety Disorder Scale (GAD-7) was used to assess anxiety disorders of children (37). The GAD-7 has seven questions with a score ranging from 0 to 3 for each item. Therefore, total score of GAD-7 ranges from 0 to 21 (38). A total score ≥ 10 of the GAD-7 is considered to meet the criterion for diagnosing generalized anxiety disorder (1 = Yes, 0 = No) (38, 39). The Chinese version of GAD-7 had good reliability among Chinese population according to early findings (40). In this study, the alpha Cronbach for GAD-7 was 0.93.
Confounding Variables
Potential confounding factors were selected based on the literature with regard to the association between sibling bullying and psychological problems (12, 13), which included gender, age, number of siblings (one, two, or more than three), birth order (the first, the second, the third, or other), family composition (living in a two-parent family or a one-parent family), maternal education (primary school or less, junior high school, senior high school, college, or higher). Besides, parental conflict and parental abuse were considered as confounding variables in this study according to prior work (14, 25). Parental conflict and parental abuse were measured by asking participants “how often your parents fight with each other” and “how often your parents hit or abused you”. The frequency coded on a five-point scale in the last half year, ranging from 1 to 5 (1= never happened, 2 = only once or twice, 3 = two or three times a month, 4 = about once a week, and 5 = several times a week). Peer bullying (0 = not involved and 1 = involved in victimization or perpetration).
Statistical Analysis
In our analyses, if the participant completed the survey with the missing items more than 15% in the questionnaire, we would exclude the whole information of the participant.
First, prevalence of participants involved in sibling bullying involvement was summarized by descriptive statistics [n (%)]. To assess associations between sibling bullying status (pure victim, pure bully, and bully-victim) and major depression as well as generalized anxiety disorder, two adjusted model of logistic regression analyses were performed separately. Second, for examining whether there were associations between different sub-types of sibling bullying and depression as well as anxiety, a set of adjusted model of logistic regression analyses were conducted to assess the associations after excluding those participants who were involved in any two or three sub-types of sibling bullying victimization or perpetration. Then, in order to examine the associations between the number of sub-types of sibling bullying involvement and depression or anxiety, a set of adjusted model of logistic regression analyses were performed with all participants who were categorized into four sub-groups (0 = participants not involved in any types of sibling bullying, 1 = participants involved in any one type of sibling bullying, 2 = participants involved in any two types of sibling bullying, and 3 = participants involved in all three types of sibling bullying). Finally, for testing if there is a dose–response relationship between the number of sub-types of sibling bullying involvement and depression or anxiety, we ran a set of adjusted model of logistic regression analyses again with the number treated as a continuous term.
Dependent variables of all adjusted logistic regression analyses mentioned above were major depression (total score ≥ 10) and generalized anxiety disorder (total score ≥ 10) separately. To address possible bias, potential confounding variables included gender, age, family composition, maternal education, number of siblings, birth order, parental conflict, parental abuse, and peer bullying. The associations were reported via adjusted odd ratios (OR) and 95% confidence intervals (95% CI). The significance level was set at p < 0.05. All of the statistical analyses were conducted by SPSS 22.0.
Results
Of the 5,926 children and adolescents, 1,235 (20.8%) reported at least one sub-type of sibling bullying victimization over the past 6 months. The prevalence of three sub-types of sibling bullying victimization was 13.8% (verbal), 7.6% (physical), and 4.0% (relational). In addition, 1,230 (20.8%) participants had bullied their siblings with any sub-type of sibling bullying in the last half a year. The prevalence of three sub-types of sibling bullying perpetration were 14.5% (verbal), 6.5% (physical), and 2.8% (relational). With respect to sibling bullying status, 448 (7.6%) of children were pure victim, 443 (7.5%) were pure bully, and 787 (13.3%) were bully-victim.
In mental health distress, 1,171 (19.8%) and 875 (14.8%) children met a threshold score of diagnosing major depression and generalized anxiety disorder respectively (Table 1).
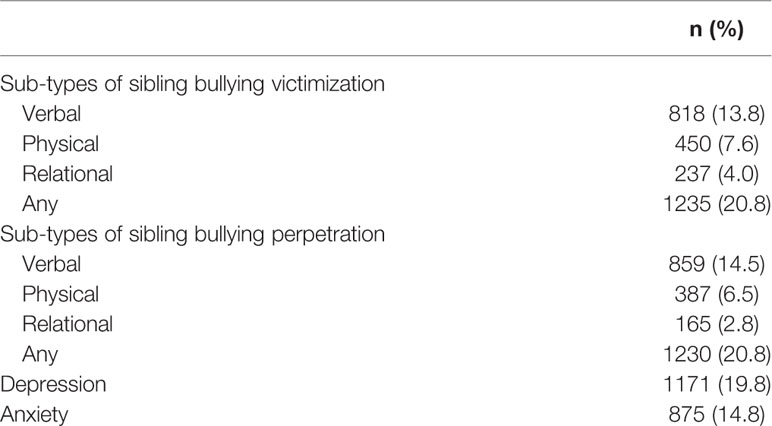
Table 1 The prevalence of sub-types of sibling bullying involvement, depression, and anxiety (N = 5,926).
Associations Between Sibling Bullying Status and Depression and Anxiety
When looking at the status involved in sibling bullying (pure victim, pure bully, and bully-victim), results of adjusted logistic regression analyses indicated that any role of sibling bullying involvement was significantly associated with both depression and anxiety (Table 2).
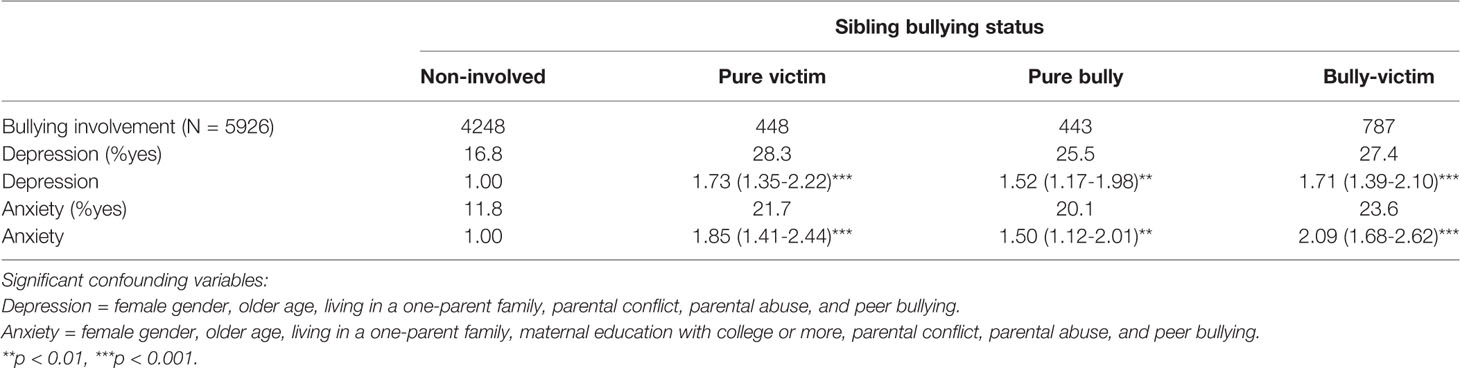
Table 2 The associations between sibling bullying status and depression and anxiety [Adjusted OR (95% CI)].
Associations Between Three Sub-types of Sibling Bullying Involvement and Depression and Anxiety
In victimization, after excluding 150 participants who experienced any two sub-types of sibling bullying victimization and 60 who were involved in all three sub-types of sibling bullying victimization, results of adjusted logistic regression analyses indicated that all verbal, physical, and relational victimization of sibling bullying were significantly associated with both depression and anxiety.
In terms of perpetration, after excluding 111 children or adolescents who acted any two sub-types of sibling bullying to their siblings and 35 who perpetrated all three sub-types of sibling bullying, there were significant associations between all three major sub-types of sibling bullying perpetration and depression as well as anxiety (Table 3).

Table 3 The associations between different sub-types of sibling bullying involvement and depression and anxiety [Adjusted OR (95% CI)].
Associations Between the Number of Sub-types of Sibling Bullying Involvement and Depression and Anxiety
The adjusted model of logistic regression analyses indicated that children and adolescents had more risk of experiencing major depression when they reported being bullied by siblings with any one, two, or three sub-types of sibling bullying than those who were not involved in sibling bullying victimization. Meanwhile, there were significant associations between any number of sub-types of sibling bullying victimization and anxiety. What is more, a linear trend was found between the number of sub-types of sibling bullying victimization and depression (adjusted OR = 1.49, 95% CI 1.32 to 1.68, p < 0.001) as well as anxiety (adjusted OR = 1.68, 95% CI 1.48 to 1.90, p < 0.001).
The results of adjusted logistic regression analyses illustrated that participants who perpetrated any one, two, or three sub-types of sibling bullying would be more likely to report major depression than those who never acted bullying behavior to their siblings. Children and adolescents who acted any number of sub-types of sibling bullying had greater risk of anxiety compared to those who did not report sibling bullying perpetration. Afterwards, the number of sub-types of sibling bullying was treated as a continuous variable for logistic regression analyses. Liner associations were found between the number of sub-types of sibling bullying perpetration and depression (adjusted OR = 1.44, 95% CI 1.26 to 1.64, p < 0.001) as well as anxiety (adjusted OR = 1.63, 95% CI 1.42 to 1.87, p < 0.001) (Table 4).
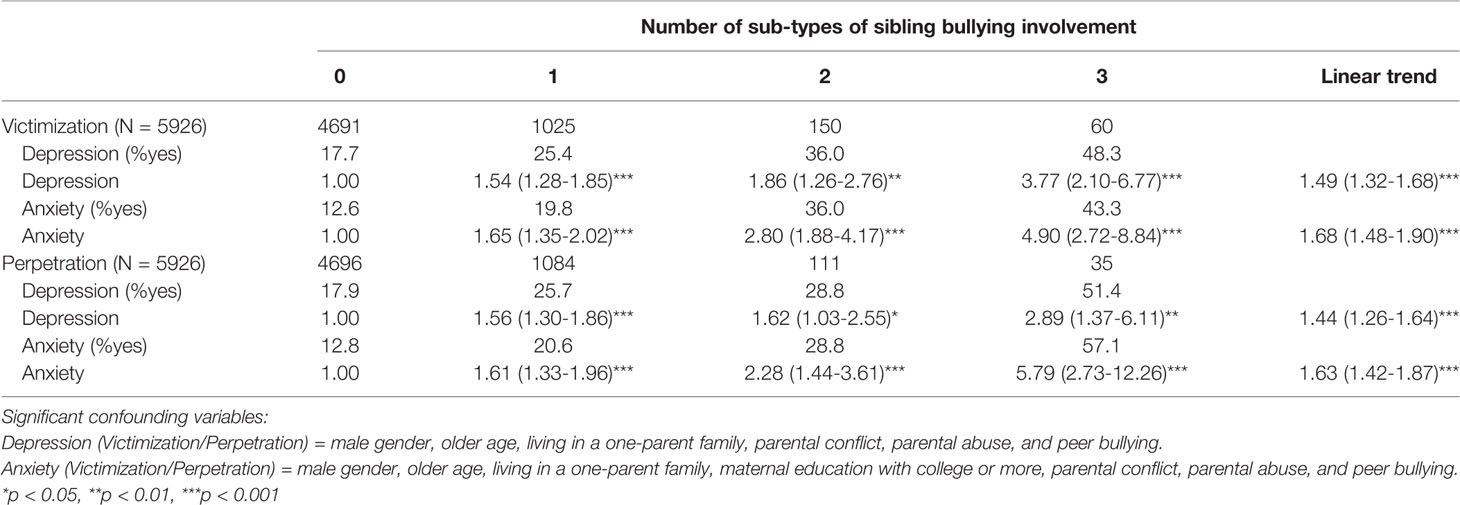
Table 4 The associations between the number of sub-types of sibling bullying involvement and depression and anxiety [Adjusted OR (95% CI)].
Discussion
This is the first study to examine the association between sibling bullying and mental health distress via a large and random sample in a non-western country. Moreover, the current study contributes new information with regard to the association from specific sub-type of sibling bullying involvement. The findings highlight the associations between three major sub-types of sibling bullying involvement and mental health problems. After controlling potential confounding variables, including individual characteristics, family characteristics, and other forms of family violence, we found that all verbal, physical, and relational victimization and perpetration of sibling bullying were associated with major depression as well as generalized anxiety disorder. More importantly, the number of sub-types of sibling bullying involvement is significantly associated with mental health distress in a dose–response fashion.
Confirmed our hypothesis, linear associations were found between the number of sub-types of sibling bullying involvement and depression and anxiety. Children and adolescents had higher odds of suffering major depression and generalized anxiety disorder with the number increasing, and those who were involved in all three sub-types of sibling bullying victimization or perpetration were at the highest risk of experiencing mental health distress. The finding extends existing studies that have identified dose–effect relationships between the frequency, the role, and the context of bullying involvement and mental health problems (13, 19). Therefore, target population of anti-bullying programs and mental health promotion must include not only those children who are involved in frequent bullying behavior (13), those who are bully-victims (a child that is both bully and victim) (2, 9), and those who are bullied by both siblings and peers (6) but also those who are involved in multiple types of victimization or perpetration.
Our work provides a new insight into the measurement of sibling bullying when examining the associations between bullying behavior among siblings and negative health outcomes. According to previous studies, sibling bullying involvement was generally treated as a binary term, and a victim or a bully of sibling bullying could be identified as long as any one item of the questionnaire met the cutoff value (13, 19). For example, a child would be classified as a victim when he or she had been hit by a brother or sister several times a month over the past half a year. Meanwhile, another child who had been hit, completely ignored, and made fun of by his or her siblings several times a month in the last 6 months was also identified as a victim of sibling bullying (19). From the findings of this study, the two children mentioned above may have different odds of experiencing mental health distress. Thus, future research should to treat sibling bullying involvement as a continuous variable according to the number of sub-types of sibling bullying in which participants are involved.
On the other hand, the cutoff value of sibling bullying in this study was “more than two or three times a month” (2, 19), which is different from some studies using the more stringent cutoff value, such as “more than once a week” (12, 31). When we chose “about once a week” as cutoff value in the study, the prevalence of sibling bullying was less than 5%, and it is much lower than 30.8% that reported in some western country (12). The difference might stem from different culture and concept of sibling relationship. Sibling bullying is a new issue but not a well-accepted topic in China in recent years. Chinese children and adolescents would avoid revealing their frequent aggressive behaviors among siblings because of traditional family values, which underline harmony and endurance.
Despite the potential contribution to the literature of sibling bullying, there are several limitations to this study. First, the nature of a cross-sectional survey limits our study to draw causality between sibling bullying and mental health distress. Moreover, there may be a bidirectional relationship between sibling bullying and depression or anxiety, which had been identified as the relationship between peer bullying and poor mental health outcomes (21, 41). Therefore, future longitudinal studies need to explore whether there is a bidirectional model between sibling bullying and mental health distress. Second, the study recruited children and adolescents aged 10 to 18 due to the fact that children aged under 10 may be unable to understand the questionnaire completely. However, the prevalence of sibling bullying peaks in childhood according to previous studies (6, 42). In the future study, we might invite younger children as our sample and information of investigation will be provided by their caregivers. In addition, the prevalence of sibling bullying in this study was measured by one of the siblings in a family through self-reported questionnaire, and there might be a information bias. Future research should consider the characteristics of sibling bullying behaviors and conduct research within a family and investigate bullying behaviors among all siblings. Finally, although the sample size of this study was rather large, the present study was conducted in a limited geographical setting. The extent to which this sample represents is unclear due to that the data of participants was only collected from students in Hunan Province, central China. Future research can recruit more children and adolescents in different regions of China.
Although there are limitations in some aspects of this study, our findings provide practical implications for clinicians, professionals, and policy makers. First, measure of sibling bullying should include specific sub-types of bullying behavior since they may have a cumulative effect on mental health outcomes. What is more, future research could take more sub-types of bullying into consideration, such as cyber bullying. At the same time, mental health education and promotion could be provided first to those children who are involved in multiple sub-types of sibling victimization or perpetration as they are at particular greater risk of mental health distress. In addition, since both sibling bullying and peer bullying are associated with depression as well as anxiety, effective preventive programs of anti-bullying should be conducted at home and at school simultaneously.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The protocol was reviewed and approved by National Office for Philosophy and Social Science (Beijing, China). The study received the approval from the ethical committee of Xiangya School of Public Health, Central South University (grant number is XYGW-2017-056). Informed consents were obtained from the principal of each chosen school, the students who participated in the study, and their parents.
Author Contributions
XL, as the first author, developed the initial manuscript. XL and MY were also responsible for the data collection and the data analysis. CP guided the overall design of the study. CP and YY also negotiated for program management of data and field access. ZQ, XQ, and XY contributed substantially to the revision and refinement of the final manuscript. All authors have read and approved the final manuscript.
Funding
This work was supported by The National Social Science Fund of China (grant number is BBA170061).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors thank students who took part in the research, parents and teachers who supported and assisted with the research, and investigators who have contributed to the field implementation of this study, including Hong Lin from Central South University, Dongfang Wang, and Shu Wang from Hunan Agricultural University.
References
1. Wolke D, Tippett N, Dantchev S. Bullying in the family: sibling bullying. Lancet Psychiat (2015) 2(10):917–29. doi: 10.1016/S2215-0366(15)00262-X
2. Wolke D, Samara MM. Bullied by siblings: association with peer victimisation and behaviour problems in Israeli lower secondary school children. J Child Psychol Psychiatry (2004) 45(5):1015–29. doi: 10.1111/j.1469-7610.2004.t01-1-00293.x
3. Tippett N, Wolke D. Aggression between siblings: Associations with the home environment and peer bullying. Aggress Behav (2015) 41(1):14–24. doi: 10.1002/ab.21557
4. Skinner JA, Kowalski RM. Profiles of Sibling Bullying. J Interpers Violence (2013) 28(8):1726–36. doi: 10.1177/0886260512468327
5. Eriksen S, Jensen V. A push or a punch: distinguishing the severity of sibling violence. J Interpers Violence (2009) 24(1):183–208. doi: 10.1177/0886260508316298
6. Tucker CJ, Finkelhor D, Turner H, Shattuck AM. Sibling and peer victimization in childhood and adolescence. Child Abuse Negl (2014) 38(10):1599–606. doi: 10.1016/j.chiabu.2014.05.007
7. Wolke D, Skew AJ. Bullying among siblings. Int J Adolesc Med Health (2012) 24(1):17–25. doi: 10.1515/ijamh.2012.004
8. Menesini E, Camodeca M, Nocentini A. Bullying among siblings: the role of personality and relational variables. Br J Dev Psychol (2010) 28 (Pt 4):921–39. doi: 10.1348/026151009X479402
9. Wolke D, Skew A. Bullied at home and at school: Relationship to Behaviour Problems and Unhappiness. Understanding Soc (2011) pp:23–32.
10. Dale J, Russell R, Wolke D. Intervening in primary care against childhood bullying: an increasingly pressing public health need. J Roy Soc Med (2014) 107(6):219–23. doi: 10.1177/0141076814525071
11. Kettrey HH, Emery BC. The discourse of sibling violence. J Fam Violence (2006) 21(6):407–16. doi: 10.1007/s10896-006-9036-0
12. Bar-Zomer J, Klomek AB. Attachment to Parents As a Moderator in the Association between Sibling Bullying and Depression or Suicidal Ideation among Children and Adolescents. Front Psychiatry (2018) 9(72):1–9. doi: 10.3389/Fpsyt.2018.00072
13. Bowes L, Wolke D, Joinson C, Lereya ST, Lewis G. Sibling Bullying and Risk of Depression, Anxiety, and Self-Harm: A Prospective Cohort Study. Pediatrics (2014) 134(4):E1032–9. doi: 10.1542/peds.2014-0832
14. van Berkel SR, Tucker CJ, Finkelhor D. The Combination of Sibling Victimization and Parental Child Maltreatment on Mental Health Problems and Delinquency. Child Maltreatment (2018) 23(3):244–53. doi: 10.1177/1077559517751670
15. Tucker CJ, Finkelhor D, Turner H, Shattuck A. Association of Sibling Aggression With Child and Adolescent Mental Health. Pediatrics (2013) 132(1):79–84. doi: 10.1542/peds.2012-3801
16. Mathis G, Mueller C. Childhood Sibling Aggression and Emotional Difficulties and Aggressive Behavior in Adulthood. J Fam Violence (2015) 30(3):315–27. doi: 10.1007/s10896-015-9670-5
17. Yen CF, Huang MF, Kim YS, Wang PW, Tang TC, Yeh YC, et al. Association between types of involvement in school bullying and different dimensions of anxiety symptoms and the moderating effects of age and gender in Taiwanese adolescents. Child Abuse Negl (2013) 37(4):263–72. doi: 10.1016/j.chiabu.2013.01.004
18. Arroll B, Goodyear-Smith F, Crengle S, Gunn J, Kerse N, Fishman T, et al. Validation of PHQ-2 and PHQ-9 to screen for major depression in the primary care population. Ann Fam Med (2010) 8(4):348–53. doi: 10.1370/afm.1139
19. Dantchev S, Zammit S, Wolke D. Sibling bullying in middle childhood and psychotic disorder at 18 years: a prospective cohort study. Psychol Med (2018) 48(14):2321–8. doi: 10.1017/S0033291717003841
20. Gallagher AM, Updegraff KA, Padilla J, McHale SM. Longitudinal Associations Between Sibling Relational Aggression and Adolescent Adjustment. J Youth Adolesc (2018) 47(10):2100–13. doi: 10.1007/s10964-018-0871-0
21. Brunstein KA, Barzilay S, Apter A, Carli VH, Christina W, Sarchiapone M, et al. Bi-directional longitudinal associations between different types of bullying victimization, suicide ideation/attempts, and depression among a large sample of European adolescents. J Child Psychol Psychiatry (2018) 60(2):209–15. doi: 10.1111/jcpp.12951
22. Barzilay S, Brunstein KA, Apter A, Carli V, Wasserman C, Hadlaczky G, et al. Bullying Victimization and Suicide Ideation and Behavior Among Adolescents in Europe: A 10-Country Study. J Adolesc Health (2017) 61(2):179–86. doi: 10.1016/j.jadohealth.2017.02.002
23. Krienert JL, Walsh JA. My Brother's Keeper: A Contemporary Examination of Reported Sibling Violence Using National Level Data, 2000-2005. J Fam Violence (2011) 26(5):331–42. doi: 10.1007/s10896-011-9367-3
24. Yu JJ, Lim GO, Gamble WC. Big Five Personality Traits and Physical Aggression between Siblings in South Korea: an Actor-Partner Interdependence Analysis. J Fam Violence (2017) 32(2):257–67. doi: 10.1007/s10896-016-9825-z
25. Chen M, Ling CK. Parental absence, child victimization, and psychological well-being in rural China. Child Abuse Negl (2016) 59:45–54. doi: 10.1016/j.chiabu.2016.07.009
26. Peng C, Luo JY, Qin ZH, Qiu XY, Wen LH, Liu XQ. Prevalence of sibling violence among primary and middle school students in rural areas. Chin Ment Health J (2018) 32(10):849–54. doi: 10.3969/j.issn.1000-6729.2018.10.008
27. Kubo M, Chaudhuri A. Gender Gap in Health Status of Children in the Context of One Child Policy in China: Is it Sibling Rivalry or Son Preference? J Fam Econ Iss (2017) 38(2):204–17. doi: 10.1007/s10834-016-9506-3
28. Zeng Y, Hesketh T. The effects of China's universal two-child policy. Lancet (2016) 388(10054):1930–8. doi: 10.1016/S0140-6736(16)31405-2
29. Olweus D. Bullying at school: basic facts and effects of a school based intervention program. J Child Psychol Psychiatry (1994) 35(7):1171–90. doi: 10.1111/j.1469-7610.1994.tb01229.x
30. Gothwal VK, Sumalini R, Irfan SM, Giridhar A, Bharani S. Revised Olweus Bully/Victim Questionnaire: Evaluation in Visually Impaired. Optometry Vision Sci (2013) 90(8):828–35. doi: 10.1097/OPX.0b013e3182959b52
31. Toseeb U, McChesney G, Wolke D. The Prevalence and Psychopathological Correlates of Sibling Bullying in Children with and without Autism Spectrum Disorder. J Autism Dev Disord (2018) 48(7):2308–18. doi: 10.1007/s10803-018-3484-2
32. Zhang WX, Wu JF. Revision of the Chinese version of the Olweus Child Bullying Questionnaire. Psychol Dev Educ (1999) 38(2):8–12. doi: 10.16187/j.cnki.issn1001-4918.1999.02.002
33. Nease DJ, Maloin JM. Depression screening: a practical strategy. J Fam Pract (2003) 52(2):118–24. doi: 10.1080/02813430310000582
34. Adewuya AO, Ola BA, Afolabi OO. Validity of the patient health questionnaire (PHQ-9) as a screening tool for depression amongst Nigerian university students. J Affect Disord (2006) 96(1-2):89–93. doi: 10.1016/j.jad.2006.05.021
35. Min BQ, Zhou AH, Liang F, Jia JP. Clinical application of Patient Health Questionnaire for self-administered measurement (PHQ-9) as screening tool for depression. J Neurosci Ment Health (2013) 13(6):569–72. doi: 10.3969/j.issn.1009-6574.2013.06.009
36. Hu XC, Zhang YL, Liang W, Zhang HM, Yang SC. Reliability and validity of the patient health questionnaire-9 in Chinese adolescents. Sichuan Ment Health (2014) 27(4):357–60. doi: 10.3969/j.issn.1007-3256.2014.04.021
37. Kroenke K, Spitzer RL, Williams JBW, Monahan PO, Lowe B. Anxiety disorders in primary care: Prevalence, impairment, comorbidity, and detection. Ann Intern Med (2007) 146(5):317–25. doi: 10.7326/0003-4819-146-5-200703060-00004
38. Spitzer RL, Kroenke K, Williams JBW, Lowe B. A brief measure for assessing generalized anxiety disorder - The GAD-7. Arch Intern Med (2006) 166(10):1092–7. doi: 10.1001/archinte.166.10.1092
39. Loewe B, Decker O, Mueller S, Brahler E, Schellberg D, Herzog W, et al. Validation and standardization of the generalized anxiety disorder screener (GAD-7) in the general population. Med Care (2008) 46(3):266–74. doi: 10.1097/MLR.0b013e318160d093
40. Zeng QZ, He YL, Liu H, Miao JM, Chen JX, Xu HN, et al. Reliability and validity of Chinese version of the Generalized Anxiety Disorder 7-item (GAD-7) scale in screening anxiety disorders in outpatients from traditional Chinese internal department. Chin Ment Health J (2013) 27(3):163–8. doi: 10.3969/j.issn.1000-6729.2013.03.001
41. Kelleher I, Keeley H, Corcoran P, Ramsay H, Wasserman C, Car V, et al. Childhood trauma and psychosis in a prospective cohort study: cause, effect, and directionality. Am J Psychiatry (2013) 170(7):734–41. doi: 10.1176/appi.ajp.2012.12091169
Keywords: sibling bullying, mental health, depression, anxiety, adolescents
Citation: Liu X, Peng C, Yu Y, Yang M, Qing Z, Qiu X and Yang X (2020) Association Between Sub-types of Sibling Bullying and Mental Health Distress Among Chinese Children and Adolescents. Front. Psychiatry 11:368. doi: 10.3389/fpsyt.2020.00368
Received: 02 February 2019; Accepted: 14 April 2020;
Published: 14 May 2020.
Edited by:
Anat Brunstein Klomek, Interdisciplinary Center Herzliya, IsraelReviewed by:
Cheng-Fang Yen, Kaohsiung Medical University, TaiwanMaya Iohan Barak, Schneider Children's Medical Center, Israel
Copyright © 2020 Liu, Peng, Yu, Yang, Qing, Qiu and Yang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chang Peng, pengchang333@hust.edu.cn