 Christine Heinisch1*†
Christine Heinisch1*† Mirijam-Griseldis Galeris1,2†
Mirijam-Griseldis Galeris1,2† Sandra Gabler1
Sandra Gabler1 Susanne Simen3Juliane Junge-Hoffmeister4
Susanne Simen3Juliane Junge-Hoffmeister4 Judith Fößel1
Judith Fößel1 Gottfried Spangler1
Gottfried Spangler1- 1Developmental and Educational Psychology, Institute of Psychology, Friedrich-Alexander University Erlangen-Nürnberg, Erlangen, Germany
- 2Department of Paediatric Psychiatry, Psychotherapy and Psychosomatics, Universitätsklinikum Leipzig, Leipzig, Germany
- 3Klinik für Psychiatrie und Psychotherapie, Universitätsklinik der Paracelsus Medizinischen Privatuniversität, Klinikum Nürnberg Süd, Nürnberg, Germany
- 4Klinik für Psychotherapie und Psychosomatik des Universitätsklinikums Carl Gustav Carus der Technischen Universität Dresden, Dresden, Germany
About 15% of mothers suffer from postpartum psychiatric disorders, such as depression, anxiety, or psychosis. Numerous studies have shown maternal caregiving behavior to be negatively affected under these circumstances. The current study sets out to shed light on specific caregiving behaviors of affected mothers in the context of parental mental illness at an early stage. There are several methods to assess maternal caregiving behavior in terms of sensitivity. However, all of them have limitations regarding the peculiarities of mothers with postpartum disorders, that is, changes in affect regulation, and the early onset of the disorder postpartum. With the current study, we provide an adapted method to assess maternal sensitivity based on methods recently approved in attachment research. Two groups of mothers, who were either healthy or had different postpartum disorders, were recorded on video during interactions with their infants. Behaviors were rated regarding responsiveness, promptness, appropriateness, intrusiveness, and positive and negative affect. A first analysis revealed an increased number of deficits on all subscales in mothers with postpartum psychiatric disorders as compared to healthy mothers. Depressive mothers with a single diagnosis had lower scores in responsiveness, promptness, and appropriateness and higher scores on intrusiveness as compared to those in healthy mothers. Here, maternal behavior appears more parent-centered, whereas affect seemed to be relatively unharmed. Moreover, as compared to healthy mothers, mothers with comorbid depression and anxiety symptomatology achieved lower scores on responsiveness, appropriateness, and positive affect and higher scores on intrusiveness and negative affect. It is suggested, that increased deficits are related to the severity of illness in mothers with comorbidities. Results on promptness indicate that these mothers are still capable of maintaining higher vigilance to infant cues. Variance in maternal behavior was relatively high in clinical mothers, showing that some of them are well capable of behaving in a sensitive manner toward their child. One strength of our adapted method is that particular aspects of sensitive parent–child interactions are assessed separately. This may shed light on specific behavior patterns of different postpartum psychiatric disorders, which may in turn relate to specific child outcomes. The manual is open for usage, while reliability testing is required.
Theoretical Background
Postpartum Mood Swings and Psychiatric Disorders
The birth of a child is typically represented as a fascinating and happy event. In reality though, a few days after child birth, about 40–80% of mothers experience symptoms of depression and emotional lability (1–3). This phenomenon, commonly known as “baby blues,” usually declines after a couple of days without psychiatric treatment. Tremendous changes in hormonal levels and psychological difficulties in adapting to the new situation after childbirth are supposed to be responsible for this emotional status (4–7). However, when these symptoms manifest in a mental disorder during pregnancy or postpartum, as it does in 10–15%, treatment is mandatory (8, 9). Maternal risk factors are a history of (familial) psychiatric disorders, sociodemographic variables, such as early motherhood, low income, low educational level, and low social support, as well as experiences of maltreatment during childhood or later life (10–13).
The most common and significant diagnoses of postpartum psychiatric disorders are postpartum depression (14), followed by postpartum anxiety (15, 16), postpartum obsessive–compulsive disorder (OCD) (17), and postpartum psychosis (18). Additional compulsive infant-focused thoughts are common in perinatal mental illness (19). Postpartum diagnoses often appear comorbid [e.g., Refs. (20, 21). In sum, they are comparable to disorders outside the postpartum period that refer to alterations in affect and cognition. However, additional peculiarities are that fears, obsessive thoughts, and sense of guilt focus on the child [e.g., Refs. (22–24)].
Maternal Sensitivity in Mentally Ill Mothers
Various symptoms with postpartum onset interfere with the demands of caring for a child and handling motherhood. Therefore, mothers with postpartum disorders often exhibit specific behavioral restraints during interaction with their infant. More specifically, postnatally depressed mothers, as compared to healthy mothers, show fewer positive caregiving behaviors, less emotional involvement, and less responsiveness when interacting with their children (25). In contrast, anxious mothers show more exaggerated behaviors and increased arousal when interacting with their children (26). Some mothers suffering from compulsive thoughts in terms of harming their child tend to withdraw from interactions as they are afraid to hurt their child (27, 28). In postpartum psychosis, Hornstein and colleagues (29) describe affected mothers as quickly overstrained, emotionally tense, uncoordinated, and sometimes awkwardly moving their infant.
In sum, postpartum psychiatric disorders compromise a mother’s ability to interact with her child in a sensitive way, which decreases the quality of the mother–child interaction [e.g., Refs. (25, 26, 30)]. Sensitive parenting behavior means to consider the child’s perspective, adequately infer and respond to emotional needs, and provoke positive reciprocity during interaction. Sensitivity itself is defined by the perception, correct interpretation, and a prompt and adequate reaction to a child’s signals and communication attempts (31). There is evidence that sensitivity is affected in mothers with postpartum disorders. As prior work suggests, there seem to be symptom-specific patterns regarding alterations on different subscales of sensitivity, which are described below.
Responsiveness. The perception and reaction toward the child’s signal was found to be lowered and less contingent in mothers with postpartum depression (25, 32–35). Also, maternal trait anxiety reduces responsiveness in healthy mothers (36, 37), whereas, in contrast, clinically anxious mothers show some overactivity (38).
Appropriateness of maternal behavior can be observed if an interaction sequence is “well-rounded” by being supportive and child-centered in an adequate way. Such supportive behavior is reduced in mothers with depressive symptoms (33). Anxious mothers behave less appropriately (39) and are more open to misinterpretations of children’s cries, which may then lead to inappropriate reactions (40). Also, repeating sorrowful thoughts can lead to lower structuring during mother–child interactions (26, 41–43). For postpartum psychosis, results regarding the appropriateness of maternal behavior are ambiguous. A recent review postulates that mothers with postpartum psychosis are as likely as postnatally depressed mothers to harm their children (44), whereas Riordan et al. (45) reported observations of greater interaction deficits than those with affective disorders, namely being more remote, insensitive, intrusive and self-absorbed.
Another important component closely related to the concept of sensitivity is intrusiveness. Higher scores on this scale are used when the caregiver denies the child’s autonomy and acts in a self-centered controlling way. On the other hand, a nonintrusive caregiver considers the child’s perspective an important part of its individuality and respects it. Mothers with postpartum depression were found to exhibit behaviors of intrusiveness and withdrawal inconsistently [e.g., Refs. (16, 25)]. Highly anxious mothers show more intrusive behaviors compared to mothers with low anxiety levels [e.g., Refs. (36, 37, 43)] as less support of the infants’ autonomy (46). Similarly, at an older age, teenagers with parents suffering from OCD report to be confronted with more controlling behavior and boundaries from their parents (47). Finally, reactions of psychotic mothers toward their children are assumed to be more intense in their intrusive behavior (48).
Several methods used to assess parental interactional behavior emphasize the importance of warmth and positive climate, although these aspects are not included in the original definition of sensitivity. Key aspects of depression are depressed mood and loss of interest. Thus, mothers with this diagnosis often experience blunted emotionality or an increase in negative affect. These emotional characteristics compromise the affective climate during mother–child interactions. More precisely, depression lowers the mothers’ capability to flexibly switch between affective states and adjust to their child’s altering affective states and needs sensitively (49, 50). Also, increases in hostility and negativity could even be observed in mothers who only exhibit subclinical levels of depression (34, 51). Finally, depressed mothers are described as less warm, more irritable, and lack joy in interacting with their child (35, 52).
Negative affect in mothers with postpartum anxiety disorder reveals itself in stressful and sorrowful behavior (53), increased criticism, and less satisfaction regarding the child’s behavior (54, 55). Some studies also describe mothers with postpartum anxiety disorders as less warm and positive in contact with their children, indicated by fewer smiles or positive gestures (46, 54, 56, 57). However, other studies suggest that maternal anxiety may also yield more positive interactions (26) or that maternal affect is at least comparable to healthy mothers (58–60).
The relevance of maternal sensitivity is evidenced by numerous studies that identify this domain of caregiving behavior as an important predictor of the child’s attachment (61–66). Indeed, the quality of attachment is highly sensitive to the appropriateness of early experiences (67, 68). In this line, insecure attachment strategies can be viewed as adaptions to less emotionally available or reliable caregivers, which means that they are functional in a given environment (69). Secure attachment relationships, however, provide the child with a range of competencies and have a positive impact on its social and language development (66, 70–72). With regard to maternal depression, a lack of sensitivity can yield insecure attachment, whereas maternal sensitive behavior can buffer negative effects of depression and increase the likelihood of establishing a secure attachment relationship (73, 74). Interventions focusing on improving maternal sensitivity have the potential to increase the offspring’s attachment security (75). However, specific associations between certain aspects of sensitivity and child outcome variables are still unknown, which is why more fine-grained analyses on a subscale level are needed. Finally, this may be especially important with regard to behavioral impairments exhibited by mentally ill mothers.
Previous Measures of Maternal Sensitivity
Observational tools to assess maternal behavior in mother–child interactions are numerous (76–79). Most combine scales measuring sensitivity with other observable behaviors like affect or even play and generate an overall score. In the following, we describe the four most influential methods that a) assess parenting behavior in terms of maternal sensitivity and b) have successfully been used to assess predictors of children’s attachment security.
First, the Ainsworth Maternal Sensitivity Scale is one of four scales assessing parental behavior (31): Sensitivity versus Insensitivity to the baby’s signals, Cooperation versus Interference with baby’s ongoing behavior, Physical and Psychological availability versus Ignoring and Neglecting, and Acceptance versus Rejection of the baby’s needs. Here, the scale sensitivity turned out to be a key variable because it was found to be correlated to acceptance, cooperation, and availability and to be a reliable predictor of attachment security (61). Affect is considered in the Acceptance versus Rejection Scale because it deals with the balance between the mother’s positive and negative feelings about the baby. The Ainsworth Maternal Sensitivity Scale requires the observer to make one global assessment of sensitivity. In further analyses, it has been related to attachment quality and a range of child behavior. It is the origin of other developing measurement tools like the NICHD–Study of Early Child Care Mother–Child Interaction (ECCN) Scale.
Second, the NICHD-ECCN Scale for mothers of children from 6 up to 24 months quantifies different aspects of maternal behavior rated from videotaped dyadic semistructured play interactions. It assesses the following aspects of parenting behavior: Sensitivity/Responsivity to distress (adapted from the original Ainsworth Maternal Sensitivity Scale), Sensitivity/Responsivity to nondistress, Intrusiveness, Detachment, Stimulation of development, Positive regard for the child, Negative regard for the child, and Flatness of affect (80). Even though there are two separate global rating scales measuring maternal sensitivity/responsivity, most studies use a composite measure of overall maternal sensitivity as an indicator of mothers’ sensitive behavior [e.g., Ref. (81)]. The NICHD-ECCN sensitivity scales are one of eight widely used observational measures; however, there are indeed a total of 50 measures related to the construct of maternal sensitivity (79). A number of studies have shown that maternal sensitivity measured by the NICHD-ECCN Scale is predictive of different child outcomes, for example, attachment security (82, 83) or cognitive competence (84).
Third, Biringen and colleagues (85–87) developed the emotional availability (EA) Scales. The EA Scales describe the caregiver’s ability to perceive and react to both positive and negative emotions, as well as the child’s reaction to the caregiver’s behavior. It includes a multidimensional set of features (e.g., caregiver’s sensitivity, nonhostility, structuring, nonintrusiveness). Moreover, the child’s behavior is observed, too. This leads to the evaluation of the affective quality of parent–child relationships from the first weeks of life to adolescence. There is no given structure for the observational situation, and it has been applied in separation–reunion situations (62), still face procedure (88), and structured and semistructured play situations (89, 90).
Fourth, the CARE-Index is a screening tool intended to enable trained professionals to make judgments about the necessity of a family intervention (91). Similar to the EA Scales, the method evaluates the quality of caregiver–infant interaction. Observational situations are 3 min of play interaction recorded on video under nonthreatening conditions. It is applicable from birth to 15 months and up to 2.5 years when using the toddler form. The coding procedure focuses the observer’s attention on seven aspects of the caregiver’s and the infant’s behaviors, including affect and cognition. For caregivers, these are sensitivity, control, and unresponsiveness. These codes define four patterns of caregivers’ interactional behavior. The “sensitive pattern” involves how the caregiver accommodates to the infant’s behavior and shares the most commonalities to the concept of sensitivity. The “controlling pattern” identifies behaviors that are either overtly hostile or covertly hostile comparable to intrusiveness and hostility in other scales, whereas the “unresponsive pattern” consists of items describing forms of withdrawal.
Limitations of Existing Methods for Mentally Ill Mothers
With many other methods, but the four named as influential in attachment research, it should be just a matter of choice to evaluate maternal sensitivity in postpartum psychiatric disorders. Indeed, all of them have been in use for clinical research [e.g., Refs. (76, 79] with their strengths and weaknesses. However, to integrate sensitivity research and specific parenting characteristics with postpartum psychiatric disorders, each of the named methods has its own limitations.
First, the onset of postpartum depression starts either already during pregnancy with signs for mental health problems or manifestations of depression and anxiety or immediately after birth or at least very few weeks or months after delivery. In practice, the diagnosis is given with diagnostic criteria until children reach the age of 1, in some hospitals even 2. Here, it is important to note that sensitivity measures vary regarding recommendations on the child’s age range: Whereas the scales of Ainsworth, EA, and CARE-Index allow observation from birth on, the NICHD Scale starts from 6 months of age and was not specifically intentionally developed for newborns or younger infants. Moreover, the CARE-Index and the EA Scales measure dyadic interaction, which increases in older infants. This might account for the number of null findings in studies using the EA Scales in depressed and nondepressed mothers (86).
Second, the development from and application with regard to attachment theory and research are different. The CARE-Index and the EA Scales can be regarded as further developments of the Ainsworth sensitivity scales and are both very promising in evaluating the dyadic interaction within the developing attachment relationship because sensitive maternal behavior is related to secure attachment. According to Bowlby (92), attachment to the primary caregiver develops not earlier than after 8 weeks, with increasing differentiation in the second half of the infant’s first year and attachment measures are applied with 12–18 months. Because maternal postpartum psychiatric disorders occur within the infant’s first year of life, with an onset immediately until 4 weeks after birth, observational measures of attachment security need to be assessed at follow-up. The Ainsworth sensitivity and the NICHD-ECCN scales have been shown to be good predictors for measures of attachment security. Moreover, the latter two are freely available and open to use for everyone. For research, reliability testing is mandatory. Training to learn the manual of the CARE-Index takes about 8 days plus practice and reliability testing. Also, the EA Scales require 1 week with additional training by Biringen, too. Whereas the Ainsworth sensitivity and the NICHD scales are free for usage, the other two are subject to charges.
Another limitation is that the NICHD ECCN sample mostly stems from the middle class. For samples who are at specific risk to show highly dysfunctional parenting behaviors, however, it is necessary to use scales that particularly differentiate behavioral nuances at low levels of parenting competence and that allow to measure distinct impairments of specific aspects of parenting behaviors.
Furthermore, all methods vary with regard to the observational situation. Whereas the Ainsworth Maternal Sensitivity Scale and the EA Scales can be applied in different settings, the CARE-Index favors free-play situations, and the NICHD-ECCN Scale requires semistructured situations like diaper change or feeding situation or in the toddler form a manualized procedure. Also, the required recording length ranges from 3 min (CARE-Index) to 30 min (EA Scales). Regarding the special group of mentally ill mothers, the observational situation must be carefully chosen. It should be easy to implement during daily routine of several treatment institutions. Because those mothers are limited in their capacity to play freely with their children, it must not enforce the feeling of insufficiency.
Next, a crucial diagnostic criterion of postpartum depression is depressed mood and loss of interest, whereas arousal is increased in mothers with postpartum anxiety. Affect measures have been considered in all scales but only to a limited degree: Hostility or warmth is measured in the Ainsworth Maternal Sensitivity and EA scales. The NICHD-ECCN sensitivity composite score includes positive and negative regard of the child for youngest children, with changes in the negative affect scale in the toddler form.
Further considerations refer to how differentiated maternal behavior is measured, which is especially important with regard to mothers’ symptom comorbidity. Recent research finds that depression and anxiety during the first 8 weeks postpartum occur simultaneously in 13% of mothers (20). Symptoms of anxiety often come along with symptoms of compulsive behavior (93). Triple comorbidity of depression, anxiety, and posttraumatric stress disorder (PTSD) is relatively rare with a prevalence of 2% to 3% (94). Other comorbidities are not well studied, although they appear in clinical practice. Next to comorbid symptoms, stresses and strains as parenting or childhood stress, immigration history, and maternal vulnerable personality predict higher rates or symptoms (20). A main concern with the recent methods is that behavioral variance caused by comorbidity may not be represented sufficiently because all ratings use sum scores or general ratings. For instance, a mother with depression can partly be responsive and adequate but not prompt, whereas a psychotic mother might act responsive, prompt but not adequate. By using a sum scale of sensitivity, both mothers would receive low scores, but how can one differentiate behavior between these mothers regarding sensitivity? And how can such differences then be related to later child outcome? With the future goal, that is to describe the mother–child interaction in postpartum disorders with the full spectrum of comorbidities and risk factors, a separation of the concept of sensitivity into its original components described by Ainsworth is valuable.
To sum up, we propose an adaptation of the described methods to measure sensitivity to fully represent the spectrum of altered behavior in postpartum psychiatric disorders with all its comorbidities. Our intention was to develop a method that is applicable in a clinical routine setting (e.g., mother–baby unit) with reasonable effort for patients and the therapeutic team. At the same time, it should be usable for scientific purposes. Future scientific questions can then focus on how maternal caregiving behavior differs with regard to different diagnoses while taking into account the high number of comorbidities. It is also of special interest if other risk factors associated with postpartum psychiatric disorders are related to specific deficits, for example, parenting stress, traumatic experiences, or lack of social support. And finally, we aim to relate our findings to specific child outcomes to increase our understanding on symptom-specific effects of alterations in parenting behavior that are related to maternal mental illness.
The present paper describes the development of an adapted measure of maternal caregiving behavior for scientific and clinical use in mothers with postpartum psychiatric disorder. The adapted measure specifically considers the clinical setting, peculiarities of postpartum disorders, and a fine-grained description of maternal behavior. We then present a preliminary pilot implementing the adapted measure on 38 mothers admitted to a mother–baby unit and 35 healthy mothers.
Method
Ethics
This study was carried out in accordance with the Declaration of Helsinki and the permission and recommendations of the Ethics Committee of the Friedrich-Alexander University Erlangen Nuremberg and the Ethics Committee of Technical University Dresden (Ethics committee of the FA: 320_15 B, Ethics committee of the TU: EK450 22013). All participants gave written and informed consent. For all data concerning children, written informed consent was obtained from the parents.
The Pilot Project: Video Screening for the Development of the Adapted Sensitivity Scale
Sample
Mentally ill mothers currently attending a video-based interaction therapy in a mother–baby day unit were asked to participate in the study. Video recordings were made on a voluntary basis. Treatment institutions were the Mother-Baby-Day-Unit of the Clinic of Psychiatry and Psychotherapy of the Paracelsus University Clinic Nuremberg Psychiatry in Nuremberg and the Mother-Baby-Day-Unit of the Clinic for Psychotherapy and Psychosomatics of the University Clinic Carl Gustav Carus at the Technical University in Dresden. In these units, mothers spent time from 8 to 16 o’clock each day for an average of 8 weeks, during which they receive a variety of interventions (e.g., group therapy, psychoeducation, personal counseling, and art therapy). A special focus lies in the improvement of mother–child interaction by providing sensitivity training, baby massage, and mother–baby bonding therapy. Video interaction therapy starts soon after the initial assessment with numerous sessions during the whole stay in treatment. In these sessions, mothers watch videotapes of themselves interacting with their infant and get feedback about positive sequences from their therapist. They are then supported by their therapist to enhance such behaviors and integrate them into daily life situations.
The total sample of mothers who agreed to participate in the current study consisted of 102 mothers with postpartum disorders (67 stemming from the Dresden Unit and 35 from the Nuremberg Unit) and of 38 healthy/nonclinical mothers. For mentally ill mothers, the diagnoses were depression, anxiety, compulsive disorder, PTSD, substance abuse {of medium extent [alcohol, tetrahydrocannabinol (THC), or nicotine during pregnancy and continuing]}, bipolar disorder, personality pathology, and/or psychosis (order according to frequency). More than half of the patients had more than one diagnosis.
Clincial diagnoses were based on clinical assessment according to International Statistical Classification of Diseases and Related Health Problems (ICD-10) criteria, video recordings were made by an interaction therapist, and questionnaires were assessed as self-ratings.
Observation of Mother–Child Interaction
Observation and analysis of mother–child interaction were used for the development of the adapted sensitivity scales. Videos were recorded in clinical routine for therapeutic use at the beginning of their therapy. Mothers were instructed to act as normal as during daily routine.
Description of the Adapted Sensitivity Scales for Observation
The method is based on the Ainsworth Maternal Sensitivity Scale (31) and the NICHD-ECCN Scale (80, 84, 95) and was adapted to the survey situation, children’s age, and peculiarities of interaction behavior in mothers with postpartum psychiatric disorders. Analysis of video-recorded interactions was done according to the manual attached (see Supplementary Material).
With respect to behavioral deficits in mentally ill mothers (as described above), the following scales were defined: caregiver’s responsiveness, promptness of reaction, appropriateness of the caregiver’s reaction, intrusiveness of the caregiver, and negative affect and positive affect toward the child.
The scale responsiveness refers to whether the mother reacts to the child’s signals. Here, given that the child sends a signal, overtly or subtle, the mother needs to signal back that she recognized it. For example, during diaper change, this can be the exchange of a look or comments on what is happening, when the child displays discomfort. Promptness is defined whether the response occurs immediately, not exceeding 3 s. Otherwise, the child may not relate its own action to the maternal reaction and experience himself as agent of this interaction.
The scale appropriateness measures whether the mother’s reaction fulfills or at least adequately attempts to fulfill the baby’s needs presented in the sequence. Generally spoken, this refers to security, warmth, and comfort. An appropriate reaction is well-rounded and children experiencing appropriate behavior are usually less stressed.
These three scales were chosen based on Ainsworth’s definition of sensitivity and the NICHD descriptions, whereas both of them use an overall score for all three types of behaviors referred to as “sensitivity.”
Intrusiveness measures to what extent the caregiver respects the child’s autonomy and accepts its individuality. High intrusiveness indicates low respect of autonomy. Practically, this can often be observed when mothers unclothe their children in an uncomfortable but quick manner, instead of doing so with respect to the child’s reaction and by providing guidance through, for example, verbalization. Mothers with postpartum psychiatric disorders have difficulties here because they often seem to follow an adult-centered script and do not seem to be able to take over the child’s perspective.
Negative affect is defined as the presence of active expressions of negative affect either verbally, facial, or by hostile actions. Because infants cannot differentiate whether they are the cause for maternal bad mood or whether there are other causes, all kinds of negative affect and hostility are rated. Positive affect, in contrast, is mirrored in the caregiver’s joy within the interaction. These scales already existed in the NICHD-ECCN Scale and were modified with special regard to the altered affectivity in psychiatric disorders.
The method and the rating scheme are described at length in the manual at the appendix (compare Supplementary Material). We added examples that were found in the videos to the descriptions.
Scales and blinded videos were repeatedly discussed on lab meetings and with trained sensitivity observers. Other scales, as measuring maternal speech or body contact, were rejected during adaptation because they were not directly related to the concept of sensitivity, although many mothers also show deficits here.
In total, six scales were rated on a 9-point scale ranging from one to five with semisteps in between. Defined anchor points are 1, 2, 3, 4, and 5. Low values indicated low characteristics of the regarding scale, whereas high values go along with frequent observation of the behavior in the scale.
Coding of Mother–Child Interaction
Analyses were conducted by five postgraduate psychology students who participated in a seminar on “observational tools to assess baby’s signals” and underwent intense reliability training by experienced researchers. Reliability training included reading literature on sensitivity, discussing videos with mother–child interaction and doing pre-ratings to find misperceptions or positive or negative observation bias on a weekly basis for 6 months. They were trained with the help of the manual and an assessment sheet (see the Manual) analyzing the categories: Responsivity, promptness, appropriateness, intrusiveness, and negative and positive affect. Note: Observers who are familiar and reliable with other sensitivity scales should be able to use the method with less intense training.
Raters were blind to diagnoses. All five students were required to become highly reliable, with all κ > 0.85 before they were allowed to score the videos included in the study. According to McHugh (96), this indicates that interrater reliability is strong to perfect. Post hoc calculated interrater reliability (weighted kappa) was based on 17 double-coded video tapes after 6 months. Here, mean reliability was moderate, with κ = 0.73. All raters showed strong reliability on the scale intrusiveness, κ = 0.85, whereas on the scale, promptness reliability was lowest and just weak, with κ = 0.59. Reliability for the other scales were moderate with responsiveness, κ = 0.66; appropriateness, κ = 0.73; negative affect; κ = 0.76; and positive affect, κ = 0.80.
First Statistical Analyses Comparing Data on Depressed and Anxious Mothers to a Healthy Group
Sample
For the present study, we examined a subset of the clinical sample including 31 mothers from the Nuremberg Unit and seven mothers from the Dresden Unit with postpartum depression and/or anxiety disorder. The clinical sample was recruited consecutively from 2016 to 2018. Infants were healthy as seen by Pediatrics from the hospital. There was a massive reduction of usable videos because during the pilot phase, criteria for the recordings of the videos for scientific usage have been developed.
Videos were excluded if they were <3 min in length (according to the standard CARE-Index procedure), recorded after the third week of admission, the patient presented with three clinical diagnoses on the basis that the underlying disorder was unclear (e.g., depression and anxiety and personality disorder and substance abuse), invisibility of important parts of the interaction, strong sound problems, or lack of questionnaire data.
In contrast, inclusion criteria were a good quality of the video, recording at the beginning of the therapy, and at least one of the diagnoses from the spectrum of depression, anxiety, or compulsive disorder.
The control group was acquired in the area of Erlangen Nuremberg, Germany, and videos were recorded during home visits. The control mothers were recruited via flyer or word of mouth and agreed to participate in a home visit, including the recording of a video and assessment of questionnaires. They were paid 20€ and received a small toy for the child.
All mothers were instructed to act as usual during daily routine. All videos included a semistandardized situation, where they changed the diapers of their infant or fed him or her. In addition, parents were asked to play with their infant without instruction.
Questionnaires
Brief Symptom Inventory
The Brief Symptom Inventory (BSI) (97) is a short form of the Symptom Checklist SCL-90-R (98) and aims to assess mental stress of participants within the last 7 days. Participants respond on a 5-step Likert Scale, ranging from 0 (“not at all”) to 4 (very heavy) how much they agree to a total of 53 items. The BSI includes nine scales assessing, for example, depression, anxiety, or psychotic experiences. Finally, the global score [Global Severity Index (GSI)] is calculated to assess general mental stress.
In addition, there are three global scores for general mental stress: GSI, intensity [(Positive Symptom Distress Index (PSDI)], and number of reported symptoms [positive symptom total (PST)].
Scores can be transformed into T scores with different norms for academic students or adults in general, as well as men and women. Here, we used T scores for women (nonstudent) to assess the global severity of mental illness. Clinically relevant GSIT scores are above ≥63 (99).
Edinburgh Postnatal Depression Scale
To assess postpartum symptoms of depression, we used the Edinburgh Postnatal Depression Scale (EPDS) (22). The screening instrument includes 10 items asking for the mood of the last 7 days of young mothers. Mothers had to answer on a 4-point Likert (0–3) Scale how much they agreed with each item. Scores were summed up, with 30 as the highest possible value. High values indicate strong symptoms. Mothers with scores of 13 or higher are regarded as likely to suffer from depression. Validation studies (100) reported good sensitivity (79%) and specificity (85%).
Statistics
We used SPSS 25.0 for analysis. To examine differences between group variables, we used t-test. Intercorrelation analysis was done by Pearson correlation. Potentially influencing factors, as age of the child or mother, were also controlled by using Pearson correlation. Group comparisons regarding sensitivity were done with multivariate analysis of variance (ANOVA). All post hoc pairwise comparisons were performed using LSD. Significance level followed p ≤ 05*, p ≤ 0.01**, p ≤ 0.001***. Tables show means and standard deviations.
Results
Sample Descriptives
Mothers of both groups were at the same age in the beginning of the thirties and had the same, relatively high, educational background (Table 1). The sex of the children had a similar ratio in both groups. Children of mentally ill mothers were significantly younger than children of the control group. In the clinical group, the number of participants with at least one close relative (parents or grandparents) who suffered from mental disorders was twice as high as in the control group.
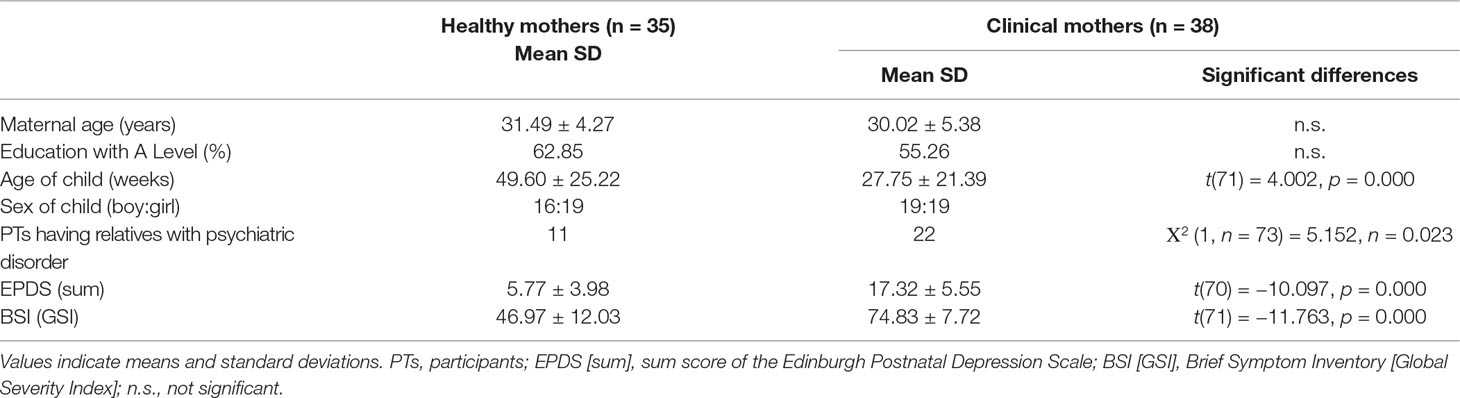
Table 1 Demographic data for healthy and clinical mothers.
Psychopathology was significantly higher in the clinical group as indicated by measures of the BSI (GSI) and EPDS. In the control group most participants (27 of 35) had scores below 10, while 5 participants had an EPDS score between 10 and 12, indicating a medium degree of postpartum depressive symptoms, and 3 of them had scores above 12 (clinical relevance). In contrast, in the clinical group, almost all mothers (36 of 38) had scores above 12, whereas 2 of them scored between 10 and 12.
Group Comparisons
We used multivariate ANOVA to test if the group of healthy mothers differs in maternal sensitivity significantly from the clinical group. Although not significant (F(6,66) = 1.690; p = 0.137), results indicate that the clinical group performs poorer in all subscales compared to the healthy control group (Table 2). Nonsignificance is typical when the dependent variables are highly correlated (Table 4). Further analysis underlines it: extracting promptness as a dependent factor from analysis leads to approaches of significance (F(5,67) = 2.042; p = 0.084). However, univariate comparisons result in significant effects for each of the dependent measures. Healthy mothers are more responsive, more prompt, and more appropriate than mentally ill mothers. They respect more of the child’s autonomy, whereas clinical mothers are more intrusive. Negative affect is lower and positive affect is higher in the healthy group than in the clinical group. Whereas the group of healthy mothers perform in the upper range of the scale (range 3.87–4.33), clinical mothers perform still in a mediocre to upper range (range 3.12–3.88).
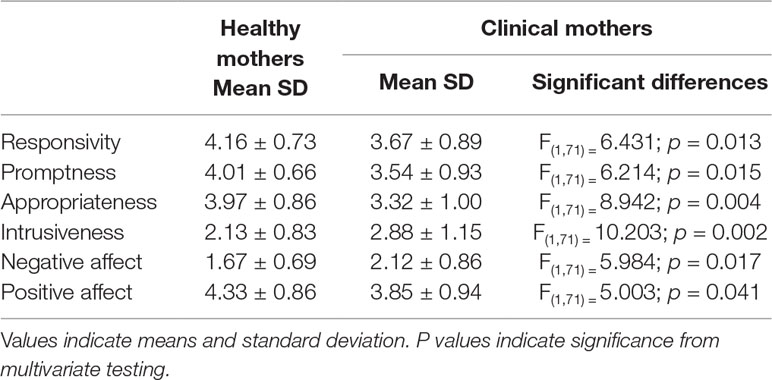
Table 2 Comparison of the sensitivity subscales for healthy and clinical mothers.
Factors Influencing Maternal Sensitivity
We tested for maternal and child age as possible parameters influencing sensitivity. Spearman correlation revealed no significance with these factors for none of the scales neither in the group of healthy nor clinical mothers (compare Table 3). For further testing if the difference of child age between the group still affected the results, we included it as a covariate into the analysis. Here, significance was reduced to a trend level in three scales, namely, responsivity (F(1,70) = 2.820, p = 0.098), promptness (F(1,70) = 3.594, p = 0.062), and negative affect (F(1,70) = 3.816, p = 0.055).
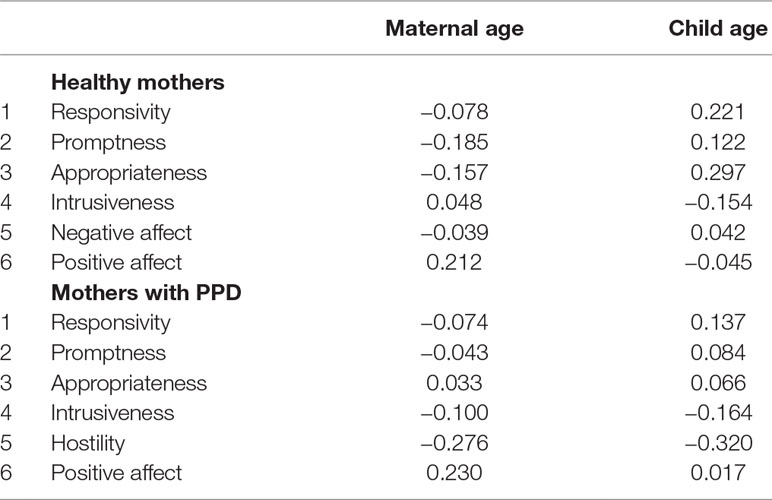
Table 3 No correlation of maternal behavior with maternal or child age.
Intercorrelations Between the Scales of Sensitivity
As visible in Table 4, all scales correlate significantly with each other in the healthy control group (range from r = 0.934 to r = 0.446) and the clinical group (range from r = 0.955 to r = 0.620).
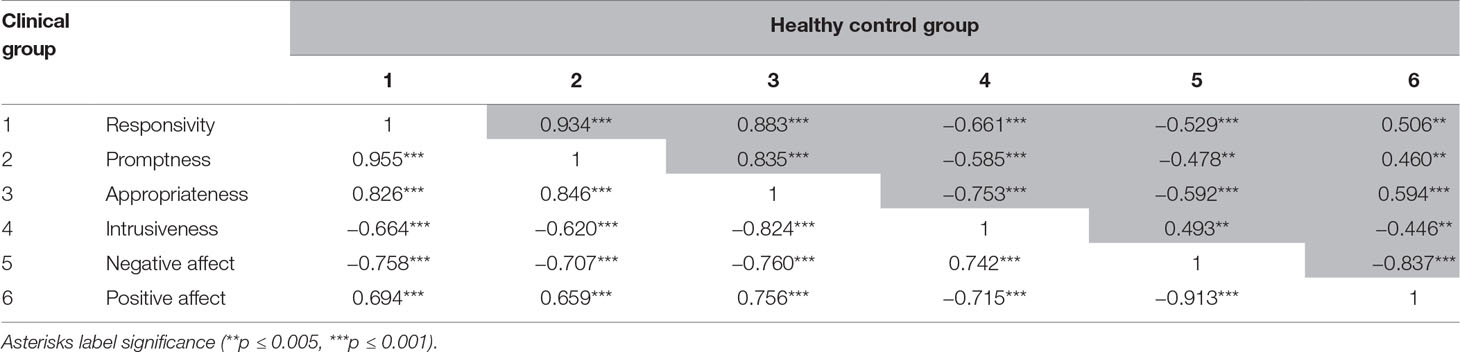
Table 4 Intercorrelations of maternal sensitivity in the control group (n = 35) (upper values, gray background) and the clinical group (n = 38) (lower values).
Influence of Severity of Symptoms in Mental Illness on Sensitivity
One goal of the development of the adapted method is to analyze sensitivity with respect to specific symptoms of depression to better differentiate between groups of different mental disorders. In the group of healthy mothers, we found mothers who scored subclinical to moderate on depression or EPDS and/or BSI and were clinically conspicuous. We decided not to exclude them from earlier analysis because they were “healthy enough” not to be in treatment. However, in an additional analysis, we put them in a separate group, named “healthy with mild depressive symptoms” (n = 8). Moreover, we separated the group of clinical mothers. Whereas 16 mothers were diagnosed with depression only, 19 mothers had depression and anxiety disorder or compulsive thoughts comorbid. We excluded three mothers because their comorbid diagnosis appeared to raise a personality disorder. The healthy group without depressive symptoms consists of 27 mothers. It is obvious that, with increasing symptoms, EPDS and BSI scores rise (Table 5).
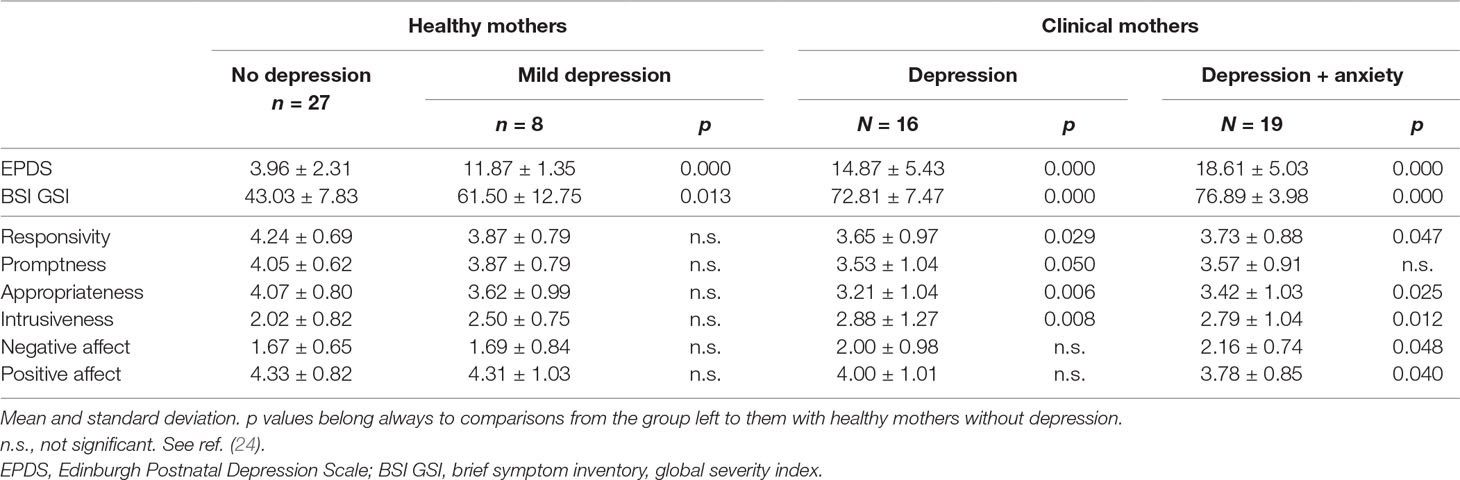
Table 5 Comparisons of the sensitivity subscales for groups with different degrees of depressive symptoms, ranging from no symptoms to comorbidities.
We used multivariate analysis to test whether the sensitivity scales differ significantly between the four groups (healthy vs. mild symptoms vs. clinical with depression vs. clinical with depression and comorbidities). Not significantly, but descriptively, with increasing severity, sensitivity gets worse. Healthy but mildly depressed mothers have lower values in sensitivity but not in their affect. Clinically burdened mothers differ significantly in their sensitivity pattern from that of healthy mothers. Whereas mothers with depression respond less, are less prompt, less appropriate, and more intrusive, their affect does not differ significantly from that of healthy mothers. Mothers with additional diagnoses of anxiety are less responsive, less appropriate, and more intrusive and show more negative and less positive affect but are not significantly less prompt.
Discussion
General Discussion
The present study aimed at adapting observational methods assessing sensitivity in caregivers to a group of mothers with postpartum mental disorders. Therefore, we screened 102 videos of mentally ill mothers interacting with their infants to identify specific parenting behaviors associated with different postpartum mental disorders. These specific behaviors are described in the manual, which can be found in the supplements. With respect to the main deficits of maternal caregiving behavior, we combined different measurement scales for sensitivity. More precisely, with special regard to attachment research, the Ainsworth’s Maternal Sensitivity Scale (31) and the NICHD Scale were chosen as a basis for the present method while integrating aspects taken from the EA Scales, the CARE-Index, and from a range of other observational tools focusing on parental behavior (76, 79). This procedure resulted in the examination of responsiveness, promptness, appropriateness, intrusiveness, negative affect, and positive affect. The compilation of these final scales is adapted to the special group of mothers with postpartum disorders because it considers peculiarities regarding the onset of illness, child age, and disorder-related behavior.
In a second step, we used the adapted scales for a preliminary analysis aiming to investigate whether the method is applicable in a clinical group. Therefore, we compared caregiving behavior in a group of mothers at the beginning of treatment in a psychiatric mother–baby unit to that of a group of healthy mothers. Results revealed that mentally ill mothers have difficulties in all aspects of sensitivity, intrusiveness, and affect. Mothers with postpartum psychiatric disorders were found to be less responsive, respond slower, less adequate and to be more intrusive and show more negative and less positive affect toward their children. These findings are not surprising because it has been repeatedly described that postpartum depression can result in tremendous problems regarding mother–child interactions [e.g., Refs. (25, 26, 30, 55, 98)].
A second aim was to see whether assessing different aspects of sensitivity separately would help identify typical behavior patterns of mothers with mental disorders dependent on their diagnosis or other risk factors for altered mother–child interaction. Here, we found that the severity of symptoms is an important factor influencing maternal sensitivity in the present sample. Even in the healthy group, we observed that mild depressive symptoms already reduce sensitivity, however, the effect was rather small. This is in line with recent research showing that subclinical depressive symptoms may increase hostility and negative affect (51) and reduce maternal sensitivity (101). Moreover, we separated the clinical group into those with depression only and those who have an additional diagnosis for anxiety disorder because postpartum depression and postpartum anxiety are frequently comorbid (102, 103). Comparing results to the healthy control group revealed deficits in both groups of mothers with mental illness, but we found different behavioral patterns: In contrast to healthy mothers, those with depression only scored significantly lower on all scales of sensitivity (responsiveness, promptness, appropriateness) and intrusiveness; they did not differ significantly on the affect scales, although values are lower than those in the healthy group. In comparison, mothers with comorbidities of depression and anxiety scored, apart from promptness, significantly lower on all subscales, indicating general deficits in mother–child interaction including own emotion regulation.
The difficulties with sensitivity and intrusiveness in depressive-only mothers have repeatedly been found in earlier studies. Responsiveness, the perception and reaction to a child’s signal, has repeatedly been shown to be lower in postpartum depression (25, 32–35). Moreover, maternal responses are less contingent (25) and less appropriate (33). Intrusiveness and withdrawal are reported to appear inconsistently (16, 25), whereas in our study, depressed mothers generally tend to show less respect for child autonomy. Without the investigation of a behavioral pattern, the lack of responsiveness alone may lead to the assumption that signals are not perceived, likely as a result from a cognitive deficit. In combination with measures of lower appropriateness and higher intrusiveness, it can be assumed that mothers ignore their children purposely, followed by a parent-centered response inappropriate to the child’s needs. The underlying cognitive process behind this behavior remains unmeasurable, but it seems as if intuitive behavior is disturbed in depressed mothers (97) and that they rather follow a script or external recommendations during interaction. Also, depression worsens the ability to manage changes between affective states, and it is more difficult to adjust to their child’s affective states and needs sensitively (49, 50). Interestingly, in our study, maternal depression did not significantly alter affect during mother–child interactions in mothers with depression only, although depressive mood is central in depression. In contrast, Cohn and colleagues (104) argue that negative affect is increased four times in depressed mothers. Also, prior work found mothers with former or postpartum depression to show more negative behaviors as criticizing or destructive reactions and fewer positive behaviors, such as praise or constructive guidance during interaction sequences (105, 106). One reason why we did not find this could be that, in the present sample, the variance in the affect scale is relatively increased in clinical mothers as compared to healthy mothers. This indicates that some of them are well capable of positive interaction with their infants, whereas others are not. Laucht et al. (107) suggest, that, because of some well-functioning, self-control mechanisms, many depressive mothers are capable of acting as nondepressed in contact with their children, warranting a positive child development (107).
As general explanation, the disturbances in altered mother–child interaction are caused or accompanied by altered brain activation. Mothers with postpartum depression have shown weaker activation of reward and motivation areas, such as the thalamus, nucleus accumbens, caudate, and key emotion regulation areas, such as the lateral orbitofrontal cortex (108). Lower responsiveness may be the result when motivation is lowered to increase contentment and infant stimuli do not feel as rewarding for some of them as for healthy mothers.
In our subsample, mothers with depression and anxiety comorbid presented another behavioral pattern. This group showed deficits in all scales, except promptness, which may represent the increase of impairment caused by the double diagnosis.
Earlier findings on maternal anxiety describe mothers as less responsive and withdrawing from interaction, also in trait anxiety of healthy mothers after birth [e.g., Refs. (36, 37)]. More precisely, anxious mothers behave less appropriate (39) and are more exaggerating or overprotective (26, 38). This exaggeration or overprotection, probably caused by the typical higher arousal in anxiety, is mirrored in the “promptness” scale. In our study, we found mothers with comorbid anxiety to have somewhat lowered scores on this scale; however, they did not significantly differ from those of the healthy group. In the face of comorbid anxiety, promptness may be a sign of higher alertness to threatening keys (such as unfamiliar baby signals combined with low maternal self-efficacy). In our, as well as in recent, studies, highly anxious mothers present more intrusive behaviors compared to mothers with low anxiety levels [e.g., Refs. (36, 37, 43)] and support less autonomy (46). They interfere with and try to control the child’s behavior (37, 38, 41), often with the objective to be overprotective (53, 109).
The finding that responsiveness, appropriateness, and intrusiveness are worsened in comorbidly ill mothers may reflect a commonality with depressed mothers’ behavior, namely, that they act more parent-centered and less intuitive. The constant alertness reflected in the promptness scale could give a hint to their inner conflict between “waiting for signals” and “not being able to react flexible.” This conflict is also visible on the affect scale because they show less cheerful play and more negative affect mimically and verbally, more distressed behavior, or emotional flattening. Negative affect in maternal anxiety has been observed through stress and sorrowful behavior (53), increased criticism, and less satisfaction of the child’s behavior (54, 55). In our study, we observed lowering of positive affect in depressed and anxious mothers in contrast to some other studies (26, 58–60). Our finding is in line with those studies describing depressed and anxious mothers as generally less warm and positive in contact with their children, indicated by less smiling and positive gestures (46, 54, 56, 57). The lack of joy in the postpartum phase might also have its cause in altered brain processes, namely, that higher levels of anxiety in relation to parenting correlated with reduced activation in the substantia nigra, a region implicated in reward prediction and processing (110). When a child’s smile feels less rewarding, experience of joy is probably reduced, too. Consequently, intentions to make the child laugh may be lacking.
In sum, the presented scales successfully identify specific deficits in mother–child interaction of mothers with postpartum psychiatric disorders. It further shows that these deficits differ depending on the diagnosis or comorbidity of mothers and thus provide simplifications for tailored therapeutic intervention. Although for depressed-only mothers, a training on improving appropriate reactions and on understanding of infant’s signals and needs might be sufficient, mothers with depression and anxiety comorbidity may need further support in their own emotion regulation. Our method is very detailed, but it is still closely related to the concept of sensitivity. Therefore, it is suited for the investigation of maternal behavior as a predictor of later attachment security.
Limitations
Results of our study are based on a group of healthy mothers and a subgroup of mothers admitted in a psychiatric/psychosomatic Mother-Baby-Day-Unit Nuremberg or Dresden. Healthy and nonhealthy mothers did not differ in their educational degree or age. One limitation was that the children of clinical mothers were younger than those of the control group because of a change of admission requirements in the hospital while the study was still ongoing. However, there was no correlation of the scales with child’s age.
Behavioral assessment was located differently for clinical and healthy mothers that may have caused different levels of stress or comfort during observation.
Another limitation of the study is the rather small sample size in the group with comorbidities with respect to the fact that they are diagnosed with different and/or several anxiety disorders. Anxiety disorders manifest in a wide range: generalized anxiety disorder, OCD, panic disorder, and birth-related PTSD. In the postpartum period, sometimes the severity and symptoms do not rise to the level of an anxiety disorder diagnosis (e.g., hypervigilant concerns and attention for the baby, extreme lability, constant worry) but nevertheless can cause significant distress and disturb mother–child interactions (93, 111). Creating further, more clearly defined subgroups would have yielded in too small sample sizes. So, conclusions for different diagnoses of anxiety on sensitivity must be postponed to future studies. Still, the investigation of subgroups and comorbidities remains an important goal for the present method.
Further Thoughts on the Use of the Method in Postpartum Psychiatric Disorders
Intercorrelations
During development of the method, it was noted repeatedly that “responsiveness” and “promptness” correlate highly significantly and were difficult to separate. We thought about combining these two scales again as the NICHD-ECCN Scale does but decided to keep them separate. First, we found “promptness” to differentiate between depressed-only and depressed-anxious mothers, as presented above. Second, during scale adaptation, we often found single videos (psychosis or very severe depression), where the difference was more obvious as responsiveness was very delayed. Third, all scales correlate with each other what is typical in this research sector. All EA Scales (86) correlate with each other, and in the Ainsworth Maternal Sensitivity Scale, the author describes the scale “sensitivity” as a key variable correlating with the other scales. The positive and negative affect scales correlated very high, too, especially in the group of mothers with mental illness. This is likely to represent the emotional flattening of mothers with depression.
Scaling
A related discussion concerns the scaling of the subunits. A rank of 3 (the mean) relates to a mother who behaves a bit more often with good caregiving skills than bad. Healthy mothers rank relatively high (around 4 from 5). Our present clinical subsample ranges from 5 to 2; only in training videos did we find ratings of 1. Why is this so and should we have adapted the scaling? The scale is not conceptualized to separate very good from perfect maternal behavior. With a rank of 4 or 5, we can assume that the behavior in the observed sequence was ideal. It must be noted that the situation was short had only little instruction. A healthy mother often knows how to perform ideally and can act so for a certain amount of time in stress-free situations. Mentally ill mothers are not necessarily “disturbed” in their sensitivity but limited in their capacities (107) and can partly behave normal. Moreover, although the group presented here is severely impaired, the therapeutic staff decided that the child’s well-being is not critically endangered. Otherwise, they must have separated mother and child and decided to treat the mother as inpatient first. We believe that, with more demanding observational settings or other types of mental disorder as psychosis, scores will be lower. Methods of stress reduction or increase can change maternal performance, leading to higher variance between mothers.
Suggested Video Length and Observational Situation
In hospital routine, we implemented video observations with a length of 10 min displaying diaper-changing situations and free play. Especially in the group of mentally ill mothers, videos from the beginning of our studies were strikingly shorter. Whereas the CARE-index requires 3 min of observation of mother–child interaction only, the EA Scales (86) recommend analyzing much longer observations, up to 2 h. Both observations pursue different goals, namely, to decide about intervention with the CARE-Index (91) while extracting information about attachment measures with the EA Scales. Therefore, different recording times are reasonable. In our study, we recommend recording times around 10 min and include a semistructured situation and free play. Because attention span is reduced in depression, video observations should reveal deficits in maternal behavior quickly (112, 113), although many are also capable of sustaining normal behavior for a while. To increase motivation for participation and compliance for therapy and science, stress should be as low as possible during recording.
According to our clinical observations, mentally ill mothers seem to lack ideas for interactive play that may evoke feelings of insufficiency in the face of a given play task. If in future studies, higher differences between the groups are favored, stress in observation situation can be increased by using more difficult tasks or observe mothers with siblings (114). Not only attention itself but also divided attention is reduced in depression (112), what should also affect mother–child interaction in more demanding situations. In this sense, it has been shown that contact to a stranger reduces responsivity to child’s signals in mothers with social phobia (115).
Future Directions
The present adapted method is useful to measure sensitivity in postpartum psychiatric disorders. Moreover, it should allow testing for relationships to attachment qualities with later strange situation procedures. Still, the next phase of research includes validation work with other observational tools and measures of attachment. Moreover, an extension of the sample with other diagnoses as psychosis and OCDs is planned. Analyses for further understanding of the disorder and its relation to maternal behavior and then child outcome are prospects. Of further importance in the group of mothers with postpartum psychiatric disorders is the interplay of genetic and caregiving influences in the prediction of attachment and further development of the child. It could be shown that higher maternal sensitivity can be a buffer for disorganized attachment in cases of genetic risk (116).
To describe the full spectrum of deficits in mother–child interaction, risk and protection factors for altered sensitivity postpartum psychiatric disorders should be assessed. Own childhood experiences are a crucial factor for the quality of sensitivity, with adverse experiences leading to less sensitivity, whereas positive experiences make warm and sensitive parenting more likely (117, 118). Moreover, experiences of emotional or physical abuse during childhood are predictors for hostile behavior toward her own child (119), as well as for postpartum maternal depression (120). Lack of social support is related to lower sensitivity and responsiveness toward her own children (121, 122) and a key factor for the development of depression (12). Socioeconomic pressure, as low income or unemployment, leads to lower quality in interaction (123) and increases depressive symptoms (12). In contrast, higher education and maternal employment are related to more sensitivity and less control of children (124). For future studies it may be interesting to study those risk and protection factors that play a role in the development of mental health for both parent and child.
Ethics Statement
This study was carried out in accordance with the Declaration of Helsinki and the permission and recommendations of the Ethics Committee of the Friedrich-Alexander University Erlangen Nuremberg and the Ethics Committee of Technical University Dresden (Ethics committee of the FA: 320_15 B, Ethics committee of the TU: EK450 22013). All participants gave written and informed consent. For all data concerning children, written informed consent was obtained from the parents.
Author Contributions
CH and MG designed and conducted the study, created the manual, and wrote the manuscript. SG was involved in study design, setup of the manual, assessment of control group, and editing the manuscript. JJ-H and SS were involved in study design and assessment of the clinical group and editing the manuscript. JF worked on the manual and the introduction. GS was involved in study design, edits on the manual, statistics and edits on the manuscript.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We thank Melanie Tamara Kungl and Jennifer Schneider for editing the manuscript, and Julia Fenkl, Melanie Lindner, Tina Riedl, Sonja Rapp, and Sarah Schwab for observation of mother–child interaction, and Martin Schmucker for help regarding statistics.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2019.00471/full#supplementary-material
References
1. Reck C, Stehle E, Reinig K, Mundt C. Maternity blues as a predictor of DSM-IV depression and anxiety disorders in the first three months postpartum. J Affect Disord (2009) 113:77–87. doi: 10.1016/j.jad.2008.05.003
2. Oakley A, Chamberlain G. Medical and social factors in postpartum depression. J Obstet Gynaecol (Lahore) (1981) 1:182–7. doi: 10.3109/01443618109067376
3. Gonidakis F, Rabavilas AD, Varsou E, Kreatsas G, Christodoulou GN. Maternity blues in Athens, Greece: a study during the first 3 days after delivery. J Affect Disord (2007) 99:107–15. doi: 10.1016/j.jad.2006.08.028
4. Seyfried LS, Marcus SM. Postpartum mood disorders. Int Rev Psychiatry (2003) 15:231–42. doi: 10.1080/0954026031000136857
5. O’Keane V, Lightman S, Patrick K, Marsh M, Papadopoulos AS, Pawlby S, et al. Changes in the maternal hypothalamic-pituitary-adrenal axis during the early puerperium may be related to the postpartum “blues.” J Neuroendocrinol (2011) 23:1149–55. doi: 10.1111/j.1365-2826.2011.02139.x
6. Oddo S, Thiel A, Klinger D, Würzburg J, Steetskamp J, Grabmair C, et al. Postpartale depression: Ein interdisziplinärer Therapie-und Forschungsansatz. J Gynakol Endokrinol(2009) 2(3):15–21.
7. Harris B, Lovett L, Newcombe RG, Read GF, Walker R, Riad-Fahmy D. Maternity blues and major endocrine changes: cardiff puerperal mood and hormone study II. BMJ (1994) 308:949–53. doi: 10.1136/bmj.308.6934.949
8. Munk-Olsen T, Laursen TM, Pedersen CB, Mors O, Mortensen PB. New parents and mental disorders: a population-based register study. J Am Med Assoc (2006) 296:2582–9. doi: 10.1001/jama.296.21.2582
9. O’Hara MW, McCabe JE. Postpartum depression: current status and future directions. Annu Rev Clin Psychol (2013) 9:379–407. doi: 10.1146/annurev-clinpsy-050212-185612
10. Goyal D, Gay C, Issues KL-WH. How much does low socioeconomic status increase the risk of prenatal and postpartum depressive symptoms in first-time mothers? Women's Health Issues (2010) 20(2):96–104. Available at: https://www.sciencedirect.com/science/article/pii/S1049386709001364 [Accessed October 30, 2018]. doi: 10.1016/j.whi.2009.11.003
11. Jones I, Craddock N. Familiality of the puerperal trigger in bipolar disorder: results of a family study. Am J Psychiatry (2001) 158:913–7. doi: 10.1176/appi.ajp.158.6.913
12. Martini J, Petzoldt J, Einsle F, Beesdo-Baum K, Höfler M, Wittchen HU. Risk factors and course patterns of anxiety and depressive disorders during pregnancy and after delivery: a prospective-longitudinal study. J Affect Disord (2015) 175:385–95. doi: 10.1016/j.jad.2015.01.012
13. Moehler E, Resch F. Infant development and postnatal psychopathology after maternal history of childhood abuse. Ment Heal (2017) 13:615–9.
14. Shorey S, Chee CYI, Ng ED, Chan YH, Tam WWS, Chong YS. Prevalence and incidence of postpartum depression among healthy mothers: a systematic review and meta-analysis. J Psychiatr Res (2018) 104:235–48. doi: 10.1016/j.jpsychires.2018.08.001
15. Goodman JH, Watson GR, Stubbs B. Anxiety disorders in postpartum women: a systematic review and meta-analysis. J Affect Disord (2016) 203:292–331. doi: 10.1016/j.jad.2016.05.033
16. Reck C, Hunt A, Fuchs T, Weiss R, Noon A, Moehler E, et al. Interactive regulation of affect in postpartum depressed mothers and their infants: an overview. Psychopathology (2004) 37:272–80. doi: 10.1159/000081983
17. Zambaldi CF, Cantilino A, Montenegro AC, Paes JA, de Albuquerque TLC, Sougey EB. Postpartum obsessive-compulsive disorder: prevalence and clinical characteristics. Compr Psychiatry (2009) 50(6):503–9 doi: 10.1016/j.comppsych.2008.11.014
18. VanderKruik R, Barreix M, Chou D, Allen T, Say L, Cohen LS. The global prevalence of postpartum psychosis: a systematic review. BMC Psychiatry (2017) 17:272. doi: 10.1186/s12888-017-1427-7
19. Riecher-Rössler A. Was ist postpartale Depression? in Postpartale Depression. Vienna: Springer (2006) pp. 11–20.Available at: https://link.springer.com/content/pdf/10.1007/3-211-29956-4_2.pdf [Accessed October 31, 2018].
20. Falah-Hassani K, Shiri R, Dennis CL. Prevalence and risk factors for comorbid postpartum depressive symptomatology and anxiety. J Affect Disord (2016) 198:142–7. doi: 10.1016/j.jad.2016.03.010
21. Sharma V, Khan M, Corpse C, Sharma P. Missed bipolarity and psychiatric comorbidity in women with postpartum depression. Bipolar Disord (2008) 10:742–7. doi: 10.1111/j.1399-5618.2008.00606.x
22. Abramowitz JS, Schwartz SA, Moore KM. Obsessional thoughts in postpartum females and their partners: content, severity, and relationship with depression. J Clin Psychol Med Settings (2003) 10:157–64. doi: 10.1023/A:1025454627242
23. Brockington IF, Macdonald E, Wainscott G. Anxiety, obsessions and morbid preoccupations in pregnancy and the puerperium. Arch Womens Ment Health (2006) 9:253–63. doi: 10.1007/s00737-006-0134-z
24. Wimmer-Puchinger B, Riecher-Rössler A, editors. (2006). Postpartale Depression. Springer Science & Business Media. Available at: https://books.google.de/books?hl=de&lr=&id=VpqWqSLoIlQC&oi=fnd&pg=PA1&dq=Riecher-Rössler,+A.+(2006).+Was+ist+postpartale+Depression%3F+In+Wimmer-Puchinger,+B.+%26++Riecher-Rössler,+A.+Postpartale+Depression.+Von+der+Forschung+zur+Praxis.+(S.11-20).Wien:+S [Accessed October 31, 2018]. doi: 10.1007/3-211-29956-4_2
25. Hoffman Y, Drotar D. The impact of postpartum depressed mood on mother-infant interaction: like mother like baby? Infant Ment Health J (1991) 12:65–80. doi: 10.1002/1097-0355(199121)12:1<65::AID-IMHJ2280120107>3.0.CO;2-T
26. Kaitz M, Maytal H, Devor N, Bergman L, Mankuta D. Maternal anxiety, mother–infant interactions, and infants’ response to challenge. Infant Behav Dev (2010) 33(2):134–48. doi: 10.1016/j.infbeh.2009.12.003
27. Jennings KD, Ross S, Popper S, Elmore M. Thoughts of harming infants in depressed and nondepressed mothers. J Affect Disord (1999) 54:21–8. doi: 10.1016/S0165-0327(98)00185-2
28. Sichel DA, Cohen LS, Dimmock JA, Rosenbaum JF. Postpartum obsessive compulsive disorder: a case series. J Clin Psychiatry (1993) 54:156–9.
29. Hornstein C, Trautmann-Villalba P, Hohm E, Rave E, Wortmann-Fleischer S, Schwarz M. Maternal bond and mother-child interaction in severe postpartum psychiatric disorders: is there a link? Arch Womens Ment Health (2006) 9:279–84. doi: 10.1007/s00737-006-0148-6
30. Persson-Blennow I, Näslund B, McNeil TF, Kaij L, Malmquist-Larsson A. Offspring of women with nonorganic psychosis: mother-infant interaction at three days of age. Acta Psychiatr Scand (1984) 70:149–59. doi: 10.1111/j.1600-0447.1986.tb10589.x
31. Ainsworth M. Maternal sensitivity scales: the baltimore longitudinal project. Power (1969) 6:1379–88.
32. Forman DR, O’Hara MW, Stuart S, Gorman LL, Larsen KE, Coy KC. Effective treatment for postpartum depression is not sufficient to improve the developing mother–child relationship. Dev Psychopathol (2007) 19(2):585–602. doi: 10.1017/S0954579407070289
33. Dix T, Gershoff ET, Meunier LN, Miller PC. The affective structure of supportive parenting: depressive symptoms, immediate emotions, and child-oriented motivation. Dev Psychol (2004) 40:1212–27. doi: 10.1037/0012-1649.40.6.1212
34. Murray L, Cooper P, Hipwell A. Mental health of parents caring for infants. Arch Womens Ment Health (2003) 6:s71–7. doi: 10.1007/s00737-003-0007-7
35. Lovejoy MC, Graczyk PA, O’Hare E, Neuman G. Maternal depression and parenting behavior. Clin Psychol Rev (2000) 20:561–92. doi: 10.1016/S0272-7358(98)00100-7
36. Nicol-Harper R, Harvey AG, Stein A. Interactions between mothers and infants: impact of maternal anxiety. Infant Behav Dev (2007) 30:161–7. doi: 10.1016/j.infbeh.2006.08.005
37. Wijnroks L. Maternal recollected anxiety and mother-infant interaction in preterm infants. Infant Ment Health J (1999) 20:393–409. doi: 10.1002/(SICI)1097-0355(199924)20:4<393::AID-IMHJ3>3.0.CO;2-I
38. Kaitz M, Maytal H. Interactions between anxious mothers and their infants: an integration of theory and research findings. Infant Ment Health J (2005) 26:570–97. doi: 10.1002/imhj.20069
39. Samuel S, Hayton B, Gold I, Feeley N, Carter CS, Zelkowitz P. Maternal mental health moderates the relationship between oxytocin and interactive behavior. Infant Ment Health J (2015) 36:415–26. doi: 10.1002/imhj.21521
40. Petzoldt J, Wittchen H-U, Einsle F, Martini J. Maternal anxiety versus depressive disorders: specific relations to infants’ crying, feeding and sleeping problems. Child Care Health Dev (2016) 42:231–45. doi: 10.1111/cch.12292
41. Künster a. K, Ziegenhain U, Schulze U, Buchheim A, Wietersheim H, Vicari A, et al. Transgenerationale Effekte mütterlicher Angst. Monatsschrift Kinderheilkd (2012) 160:982–7. doi: 10.1007/s00112-012-2661-1
42. Stein A, Craske MG, Lehtonen A, Harvey A, Savage-McGlynn E, Davies B, et al. Maternal cognitions and mother-infant interaction in postnatal depression and generalized anxiety disorder. J Abnorm Psychol (2012) 121:795–809. doi: 10.1037/a0026847
43. Zelkowitz P, Papageorgiou A, Bardin C, Wang T. Persistent maternal anxiety affects the interaction between mothers and their very low birthweight children at 24 months. Early Hum Dev (2009) 85:51–8. doi: 10.1016/j.earlhumdev.2008.06.010
44. Ramsauer B, Achtergarde S. Mothers with acute and chronic postpartum psychoses and impact on the mother-infant interaction. Schizophr Res (2018) 197:45–58. doi: 10.1016/j.schres.2018.02.032
45. Riordan D, Appleby L, Faragher B. Mother–infant interaction in postpartum women with schizophrenia and affective disorders. Psychol Med (1999) 29(4):991–5. doi: 10.1017/S0033291798007727
46. Whaley SE, Pinto A, Sigman M. Characterizing interactions between anxious mothers and their children. J Consult Clin Psychol (1999) 67:826–36. doi: 10.1037/0022-006X.67.6.826
47. Griffiths J, Norris E, Stallard P, Matthews S. Living with parents with obsessive-compulsive disorder: children’s lives and experiences. Psychol Psychother Theory Res Pract (2012) 85:68–82. doi: 10.1111/j.2044-8341.2011.02016.x
48. Riordan D, Appleby L, Faragher B. Mother–infant interaction in post-partum women with schizophrenia and affective disorders. Psychol Med (1999) 29:991–5. doi: 10.1017/S0033291798007727
49. Lunkenheimer ES, Albrecht EC, Kemp CJ. Dyadic flexibility in early parent-child interactions: relations with maternal depressive symptoms and child negativity and behaviour problems. Infant Child Dev (2013) 22:250–69. doi: 10.1002/icd.1783
50. Murray L, Fiori-Cowley A, Hooper R, Cooper P. The impact of postnatal depression and associated adversity on early mother-infant interactions and later infant outcome. Child Dev (1996) 67:2512–26. doi: 10.1111/j.1467-8624.1996.tb01871.x
51. Behrendt HF, Konrad K, Goecke TW, Fakhrabadi R, Herpertz-Dahlmann B, Firk C. Postnatal mother-to-infant attachment in subclinically depressed mothers: dyads at risk? Psychopathology (2016) 49:269–76. doi: 10.1159/000447597
52. Letourneau N, Salmani M, Duffett-Leger L. Maternal depressive symptoms and parenting of children from birth to 12 years. West J Nurs Res (2010) 32:662–85. doi: 10.1177/0193945909359409
53. Turner SM, Beidel DC, Roberson-Nay R, Tervo K. Parenting behaviors in parents with anxiety disorders. Behav Res Ther (2003) 41:541–54. doi: 10.1016/S0005-7967(02)00028-1
54. Crosby Budinger M, Drazdowski TK, Ginsburg GS. Anxiety-promoting parenting behaviors: a comparison of anxious parents with and without social anxiety disorder. Child Psychiatry Hum Dev (2013) 44:412–8. doi: 10.1007/s10578-012-0335-9
55. Hirshfeld D, Biederman J, Brody L, Faraone S, Rosenbaum J. Associations between expressed emotion and child behavioral inhibition and psychopathology - a pilot study. J Am Acad Child Adolesc Psychiatry (1997) 36(2):205–13. doi: 10.1097/00004583-199702000-00011
56. Challacombe F, Salkovskis P. A preliminary investigation of the impact of maternal obsessive-compulsive disorder and panic disorder on parenting and children. J Anxiety Disord (2009) 23:848–57. doi: 10.1016/j.janxdis.2009.04.002
57. DiBartolo PM, Helt M. Theoretical models of affectionate versus affectionless control in anxious families: a critical examination based on observations of parent–child interactions. Clin Child Fam Psychol Rev (2007) 10:253–74. doi: 10.1007/s10567-007-0017-5
58. Aktar E, Bögels SM. Exposure to parents’ negative emotions as a developmental pathway to the family aggregation of depression and anxiety in the first year of life. Clin Child Fam Psychol Rev (2017) 20:369–90. doi: 10.1007/s10567-017-0240-7
59. Aktar E, Colonnesi C, De Vente W, Majdandžić M, Bögels SM. How do parents’ depression and anxiety, and infants’ negative temperament relate to parent-infant face-to-face interactions? Dev Psychopathol (2017) 29:697–710. doi: 10.1017/S0954579416000390
60. Weinberg MK, Beeghly M, Olson KL, Tronick E. Effects of maternal depression and panic disorder on mother-infant interactive behavior in the face-to-face still-face paradigm. Infant Ment Health J (2008) 29:472–91. doi: 10.1002/imhj.20193
61. Ainsworth Mary D, Salter Bell SM, Stayton DF. Infant-mother attachment and social development: socialization as a product of reciprocal responsiveness to signals. In: The integration of a child into a social world. p. 99–135. doi: 10.1007/978-0-387-89959-6_2
62. Easterbrooks M, Bureau J, Lyons-Ruth K. Developmental correlates and predictors of emotional availability in mother–child interaction: a longitudinal study from infancy to middle childhood. Dev Psychopathol (2012) 24(1):65–78. doi: 10.1017/S0954579411000666
63. Bost KK, Shin N, Mcbride BA, Brown GL, Vaughn BE, Coppola G, et al. Maternal secure base scripts, children’s attachment security, and mother - child narrative styles. In: Attachment and Human Development. p. 241–60. doi: 10.1080/14616730600856131
64. Spieker SJ, Oxford ML, Fleming CB, Lohr MJ. Parental childhood adversity, depressive symptoms, and parenting quality: effects on toddler self-regulation in child welfare services in involved families. Infant Ment Health J (2018) 39:5–16. doi: 10.1002/imhj.21685
65. Grossmann K, Grossmann KE, Spangler G, Suess G, Unzner L. Maternal sensitivity and newborns’ orientation responses as related to quality of attachment in Northern Germany. Monogr Soc Res Child Dev (1985) 50:233. doi: 10.2307/3333836
66. De Wolff MH, van Ijzendoorn M. Sensitivity and attachment: a meta-analysis on parental antecedents of infant attachment. Child Dev(1997) 68(4):571–91. doi: 10.1111/j.1467-8624.1997.tb04218.x
67. Cicchetti D, Barnett D. Attachment organization in maltreated preschoolers. Dev Psychopathol (1991) 3:397–411. doi: 10.1017/S0954579400007598
68. Fenichel E. Relationships at risk. Infants Young Child (2002) 15:49–56. doi: 10.1097/00001163-200210000-00007
69. Main M, Hesse E. Parents' unresolved traumatic experiences are related to infant disorganized attachment status: Is frightened and/or frightening parental behavior the linking mechanism? In: Greenberg MT, Cicchetti D, Cummings EM, (Eds.), The John D. and Catherine T. MacArthur Foundation series on mental health and development. Attachment in the preschool years: theory, research, and intervention. Chicago, IL, US: University of Chicago Press. (1990) pp. 161-182. doi: 10.1016/j.ncl.2015.11.007
70. Belsky J, Pasco Fearon RM. Early attachment security, subsequent maternal sensitivity, and later child development: does continuity in development depend upon continuity of caregiving? Attach Hum Dev (2002) 4:361–87. doi: 10.1080/14616730210167267
71. Sroufe LA. Attachment and development: a prospective, longitudinal study from birth to adulthood. Attach Hum Dev (2005) 7:349–67. doi: 10.1080/14616730500365928
72. Wartner UG, Grossmann K, Fremmer-Bombik E, Suess G. Attachment patterns at age six in South Germany: predictability from infancy and implications for preschool behavior. Child Dev (1994) 65(4):1014–27. doi: 10.1111/j.1467-8624.1994.tb00799.x
73. Campbell SB, Brownell CA, Hungerford A, Spieker SJ, Mohan R, Blessing JS. The course of maternal depressive symptoms and maternal sensitivity as predictors of attachment security at 36 months. Dev Psychopathol (2004) 16:231–52. doi: 10.1017/S0954579404044499
74. Carter AS, Garrity-Rokous FE, Chazan-Cohen R, Little C, Briggs-Gowan MJ. Maternal depression and comorbidity: predicting early parenting, attachment security, and toddler social-emotional problems and competencies. J Am Acad Child Adolesc Psychiatry (2001) 40:18–26. doi: 10.1097/00004583-200101000-00012
75. Bakermans-Kranenburg MJ, Van IJzendoorn MH, Juffer F. Less is more: meta-analyses of sensitivity and attachment interventions in early childhood. Psychol Bull (2003) 129:195–215. doi: 10.1037/0033-2909.129.2.195
76. Lotzin A, Lu X, Kriston L, Schiborr J, Musal T, Romer G, et al. Observational tools for measuring parent–infant interaction: a systematic review. Clin Child Fam Psychol Rev (2015) 18(2):99–132.
77. Bretherton I. Emotional availability: an attachment perspective. Attach Hum Dev (2000) 2:233–41. doi: 10.1080/14616730050085581
78. Bretherton I. Revisiting Mary Ainsworth’s conceptualization and assessments of maternal sensitivity-insensitivity. Attach Hum Dev (2013) 15:460–84. doi: 10.1080/14616734.2013.835128
79. Mesman J, Emmen RAG. Mary Ainsworth’s legacy: a systematic review of observational instruments measuring parental sensitivity. Attach Hum Dev (2013) 15:485–506. doi: 10.1080/14616734.2013.820900
80. Owen MT. The NICHD study of early child care mother-infant interaction scales. Unpubl manuscript, Timberlawn Psychiatr Res Found Dallas, TX (1992)
81. Bradley Bradley RH, Corwyn RF. Infant temperament, parenting, and externalizing behavior in first grade: a test of the differential susceptibility hypothesis. J Child Psychol Psychiatry (2008) 49:124–31. doi: 10.1111/j.1469-7610.2007.01829.x
82. NICHD Early Child Care Research Network. Child-care and family predictors of preschool attachment and stability from infancy. Dev Psychol (2001) 37:847–62. doi: 10.1037//0012-1649.37.6.847
83. Bakermans-Kranenburg MJ, Van IJzendoorn MH, Kroonenberg PM. Differences in attachment security between African-American and white children: ethnicity or socio-economic status? Infant Behav Dev (2004) 27:417–33. doi: 10.1016/j.infbeh.2004.02.002
84. NICHD Early Child Care Research Network. Child-care structure→ process→ outcome: direct and indirect effects of child-care quality on young children’s development. Psychol Sci (2002) 13:199–206. doi: 10.1111/1467-9280.00438
85. Biringen Z. The emotional availability (EA) scales and the emotional attachment and emotional availability (EA2) clinical screener: Infancy/early childhood version; middle childhood/youth version; therapist/interventionist manual; couple relationship manual. Boulder (2008). Available at: www.emotionalavailability.com.
86. Biringen Z, Derscheid D, Vliegen N, Closson L, Easterbrooks MA. Emotional availability (EA): theoretical background, empirical research using the EA Scales, and clinical applications. Dev Rev (2014) 34:114–67. doi: 10.1016/j.dr.2014.01.002
87. Easterbrooks MA, Biringen Z. The emotional availability scales: methodological refinements of the construct and clinical implications related to gender and at-risk interactions. Infant Ment Health J (2005) 26:291–4. doi: 10.1002/imhj.20053
88. Kogan N, Carter AS. Mother-infant reengagement foilowing the still-face: the role of maternal emotional availability in infant affect regulation. Infant Behav Dev (1996) 19:359–70. doi: 10.1016/S0163-6383(96)90034-X
89. Biringen Z, Damon J, Grigg W, Mone J, Pipp-Siegel S, Skillern S, et al. Emotional availability: differential predictions to infant attachment and kindergarten adjustment based on observation time and context. Infant Ment Health J (2005) 26:295–308. doi: 10.1002/imhj.20054
90. Dolev S, Oppenheim D, Koren-Karie N, Yirmiya N. Emotional availability in mother-child interaction: the case of children with autism spectrum disorders. Parenting (2009) 9:183–97. doi: 10.1080/15295190902844332
91. Crittenden PM. CARE-Index: coding manual. Unpubl manuscript. Miami:Family Relations Institute (2003).
92. Attachment Behaviors Scale, Available at: https://lifepathsresearch.org/wp-content/uploads/Attachment-Behaviors-Scale.pdf [Accessed November 16, 2018].
93. Ross LE, McLean LM. Anxiety disorders during pregnancy and the postpartum period: a systematic review. J Clin Psychiatry (2006) 67:1285–98. doi: 10.4088/JCP.v67n0818
94. Agius A, Xuereb RB, Carrick-Sen D, Sultana R, Rankin J. The co-existence of depression, anxiety and post-traumatic stress symptoms in the perinatal period: a systematic review. Midwifery (2016) 36:70–9. doi: 10.1016/j.midw.2016.02.013
95. Network NECCR. Child care and mother-child interaction in the first 3 years of life. Dev Psychol (1999) 35:1399–413. doi: 10.1037//0012-1649.35.6.1399
96. McHugh ML. Interrater reliability: the kappa statistic. Biochem Med (Zagreb) (2012) 22(3):276–82.
97. Parsons CE, Young KS, Stein A, Kringelbach ML. Intuitive parenting: understanding the neural mechanisms of parents’ adaptive responses to infants. Curr Opin Psychol (2017) 15:40–4. doi: 10.1016/j.copsyc.2017.02.010
98. Derogatis LR. Symptom Checklist-90-R (SCL-90-R). In: Administration, scoring, and procedures manual., 3rd. Minneapolis: National Computer Systems (1994).
100. Cox J, Chapman G, Murray D, Jones P. Validation of the Edinburgh Postnatal Depression Scale (EPDS) in non-postnatal women. J Affect Disord (1996) 39(3):185–9. doi: 10.1016/0165-0327(96)00008-0
101. Tietz A, Zietlow AL, Reck C. Maternal bonding in mothers with postpartum anxiety disorder: the crucial role of subclinical depressive symptoms and maternal avoidance behaviour. Arch Womens Ment Health (2014) 17:433–42. doi: 10.1007/s00737-014-0423-x
102. O’Hara M, Wisner K. Perinatal mental illness: definition, description and aetiology. Elsevier Best Pract Res Clin Obstet Gynaecol (2014) 28:3–12. doi: 10.1016/j.bpobgyn.2013.09.002
103. Reck C, Struben K, Backenstrass M, Stefenelli U, Reinig K, Fuchs T, et al. Prevalence, onset and comorbidity of postpartum anxiety and depressive disorders. Acta Psychiatr Scand (2008) 118:459–68. doi: 10.1111/j.1600-0447.2008.01264.x
104. Cohn JF, Campbell SB, Matias R, Hopkins J. Face-to-face interactions of postpartum depressed and nondepressed mother-infant pairs at 2 Months. Dev Psychol (1990) 26:15–23. doi: 10.1037/0012-1649.26.1.15
105. Ewell Foster CJ, Garber J, Durlak JA. Current and past maternal depression, maternal interaction behaviors, and children’s externalizing and internalizing symptoms. J Abnorm Child Psychol (2008) 36:527–37. doi: 10.1007/s10802-007-9197-1
106. Caughy MO, Huang K-Y, Lima J. Patterns of conflict interaction in mother–toddler dyads: differences between depressed and non-depressed mothers. J Child Fam Stud (2009) 18:10–20. doi: 10.1007/s10826-008-9201-6
107. Laucht M, Esser G, Schmidt MH. Heterogene entwicklung von kindern postpartal depressiver mütter. Z Klin Psychol Psychother (2002) 31:127–34. doi: 10.1026//1616-3443.31.2.127
108. Laurent HK, Ablow JC. The missing link: mothers’ neural response to infant cry related to infant attachment behaviors. Infant Behav Dev (2012) 35:761–72. doi: 10.1016/j.infbeh.2012.07.007
109. Bögels SM, Van Melick M. The relationship between child-report, parent self-report, and partner report of perceived parental rearing behaviors and anxiety in children and parents. Pers Individ Dif (2004) 37:1583–96. doi: 10.1016/j.paid.2004.02.014
110. Kim P, Rigo P, Leckman JF, Mayes LC, Cole PM, Feldman R, et al. A prospective longitudinal study of perceived infant outcomes at 18-24 months: neural and psychological correlates of parental thoughts and actions assessed during the first month postpartum. Front Psychol (2015) 6:1772. doi: 10.3389/fpsyg.2015.01772
111. Lok P, Pop-Purceleanu M, Tendolkar I. Anxiety disorders during pregnancy and the post-partum period. Tijdschr Psychiatr (2015) 57(6):415–23.
112. Majer M, Ising M, Künzel H, Binder EB, Holsboer F, Modell S, et al. Impaired divided attention predicts delayed response and risk to relapse in subjects with depressive disorders. Psychol Med (2004) 34:1453–63. doi: 10.1017/S0033291704002697
113. Lee RSC, Hermens DF, Porter MA, Redoblado-Hodge MA. A meta-analysis of cognitive deficits in first-episode major depressive disorder. J Affect Disord (2012) 140:113–24. doi: 10.1016/j.jad.2011.10.023
114. Madigan S, Plamondon A, Browne D, Jenkins J. Stability of observed maternal behavior across tasks, time, and siblings. Parenting (2016) 16:108–24. doi: 10.1080/15295192.2016.1134990
115. Murray L, Cooper P, Creswell C, Schofield E, Sack C. The effects of maternal social phobia on mother-infant interactions and infant social responsiveness. J Child Psychol Psychiatry (2007) 48:45–52. doi: 10.1111/j.1469-7610.2006.01657.x
116. Spangler G. Individual dispositions as precursors of differences in attachment quality: why maternal sensitivity is nevertheless important. Attach Hum Dev (2013) 15:657–72. doi: 10.1080/14616734.2013.842065
117. Simons RL, Beaman J, Conger RD, Chao W. Childhood experience, conceptions of parenting, and attitudes of spouse as determinants of parental behavior. J Marriage Fam (1993) 55:91–106. doi: 10.2307/352961
118. Belsky J, Sligo J, Jaffee SR, Woodward L, Silva PA. Intergenerational transmission of warm-sensitive-stimulating parenting: a prospective study of mothers and fathers of 3-year-olds. Child Dev (2005) 76:384–96. doi: 10.1111/j.1467-8624.2005.00852.x
119. Bailey H, DeOliveira C, Wolfe V, Evans E, Hartwick C. The impact of childhood maltreatment history on parenting_A comparison of maltreatment types & assessment methods. Child Abuse Neg (2012) 36(3):236–46. doi: 10.1016/j.chiabu.2011.11.005
120. Gaillard A, Le Strat Y, Mandelbrot L, Keïta H, Dubertret C. Predictors of postpartum depression: prospective study of 264 women followed during pregnancy and postpartum. Psychiatry Res (2014) 215:341–6. doi: 10.1016/j.psychres.2013.10.003
121. Kivijarvi M, Raiha H, Virtanen S, Lertola K, Piha J. Maternal sensitivity behavior and infant crying, fussing and contented behavior: the effects of mother’s experienced social support. Scand J Psychol (2004) 45:239–46. doi: 10.1111/j.1467-9450.2004.00400.x
122. Mertesacker B, Bade U, Haverkock A, Pauli-Pott U. Predicting maternal reactivity/sensitivity: the role of infant emotionality, maternal depressiveness/anxiety, and social support. Infant Ment Health J (2004) 25:47–61. doi: 10.1002/imhj.10085
123. Sidor A, Köhler H, Cierpka M. Einfluss der sozioökonomischen Risikobelastung auf mütterliche Feinfühligkeit, Stressbelastung und Familienfunktionalität. Prax Kinderpsychol Kinderpsychiatr (2018) 67:257–3. doi: 10.13109/prkk.2018.67.3.257
Keywords: maternal sensitivity, postpartum depression (PPD), postpartum anxiety, mother–child interaction, AINSWORTH
Citation: Heinisch C, Galeris M-G, Gabler S, Simen S, Junge-Hoffmeister J, Fößel J and Spangler G (2019) Mothers With Postpartum Psychiatric Disorders: Proposal for an Adapted Method to Assess Maternal Sensitivity in Interaction With the Child. Front. Psychiatry 10:471. doi: 10.3389/fpsyt.2019.00471
Received: 24 January 2019; Accepted: 13 June 2019;
Published: 22 July 2019.
Edited by:
Giovanni De Girolamo, Centro San Giovanni di Dio Fatebenefratelli (IRCCS), ItalyReviewed by:
Ming Wai Wan, University of Manchester, United KingdomHiroaki Hori, National Center of Neurology and Psychiatry (Japan), Japan
Copyright © 2019 Heinisch, Galeris, Gabler, Simen, Junge-Hoffmeister, Fößel and Spangler. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Christine Heinisch, christine.heinisch@fau.de
†These authors have contributed equally to this work.