 Annina Seiler
Annina Seiler Josef Jenewein
Josef Jenewein- 1Department of Consultation-Liaison Psychiatry and Psychosomatic Medicine, University Hospital Zurich, Zurich, Switzerland
- 2Clinic Zugersee, Center for Psychiatry and Psychotherapy, Oberwil-Zug, Switzerland
Background: Being diagnosed with cancer and undergoing its treatment are associated with substantial distress that can cause long-lasting negative psychological outcomes. Resilience is an individual’s ability to maintain or restore relatively stable psychological and physical functioning when confronted with stressful life events and adversities. Posttraumatic growth (PTG) can be defined as positive life changes that result from major life crises or stressful events.
Objectives: The aims of this study were to 1) investigate which factors can strengthen or weaken resilience and PTG in cancer patients and survivors; 2) explore the relationship between resilience and PTG, and mental health outcomes; and 3) discuss the impact and clinical implications of resilience and PTG on the process of recovery from cancer.
Methods: A literature search was conducted, restricted to PubMed from inception until May 2018, utilizing the following key words: cancer, cancer patients, cancer survivors, resilience, posttraumatic growth, coping, social support, and distress.
Results: Biological, personal, and most importantly social factors contribute to cancer patients’ resilience and, consequently, to favorable psychological and treatment-related outcomes. PTG is an important phenomenon in the adjustment to cancer. From the literature included in this review, a model of resilience and PTG in cancer patients and survivors was developed.
Conclusions: The cancer experience is associated with positive and negative life changes. Resilience and PTG are quantifiable and can be modified through psychological and pharmacological interventions. Promoting resilience and PTG should be a critical component of cancer care.
Introduction
For many cancer patients, receiving a diagnosis of cancer and undergoing its treatment together comprise an extremely stressful experience that can render individuals vulnerable to long-lasting negative psychological outcomes, including emotional distress, depression, anxiety, sleep problems, fatigue, and impaired quality of life (1–5). Cancer is commonly perceived as a life-threatening and potentially traumatic illness, perceptions exacerbated by its sudden onset and uncontrollable nature (6). Furthermore, cancer patients must deal with dramatic life changes to which they have to adapt throughout their treatment trajectory (7). Research published in recent decades has emphasized the traumatic characteristics of a life-threatening illness, like cancer, and demonstrated how cancer patients exhibit responses consistent with psychological trauma (8–11). While in the fourth edition of the American Psychiatric Association’s (12) Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) (13), life-threatening cancer was acknowledged to be a severe stressor that can trigger posttraumatic stress disorder (PTSD), in the newest edition, the DSM-5, “a non-immediate, non-catastrophic life-threatening illness,” like cancer, is no longer qualified as traumatic, irrespective of how stressful or serious it is (14).
Interestingly, despite substantial distress that is associated with a cancer diagnosis and its treatment, many cancer patients manifest remarkable resilience (15, 16). Studies have shown that overcoming cancer and its treatment can be an opportunity for personal growth, as well as for enhanced mental and emotional well-being that could potentially be linked to better coping with disease-related demands (17–19). However, not everyone reacts to adversities in the same way, with some more resilient than others (20). Understanding which factors discriminate cancer patients, as well as cancer survivors who experience psychological growth from those who do not, might have important clinical implications and guide interventions to assist cancer patients and survivors with their psychological recovery from the cancer experience.
For this article, we reviewed the literature on resilience and posttraumatic growth (PTG) in cancer patients and survivors, so as to better understand which psychosocial, disease-related, and contextual factors yield better adjustment to the disease. The overall aims of this review were to 1) investigate which factors can strengthen or weaken resilience and PTG in cancer patients and survivors; 2) explore the relationships between resilience and PTG, and mental health outcomes; and 3) discuss the impact of resilience and PTG on the process of recovery from the disease, as well as the clinical implications of this impact.
For the purposes of this review, a literature search was conducted, restricted to PubMed articles from inception (1979) until May 2018, using the following search terms in various combinations: cancer, cancer patients, cancer survivors, resilience, posttraumatic growth, coping, social support, and distress. Only studies involving patients who were adults (≥18 years) were included. To be considered for the review, articles had to be peer reviewed and written in English (Table 1). The psychometric instruments used in the eligible studies are summarized in Table 2. From the literature reviewed, a two-pathway model of resilience in cancer patients and cancer survivors was drafted (Figure 1).

Table 1 Summary of studies included in the review.
Table 2 Psychometric instruments used in eligible studies.
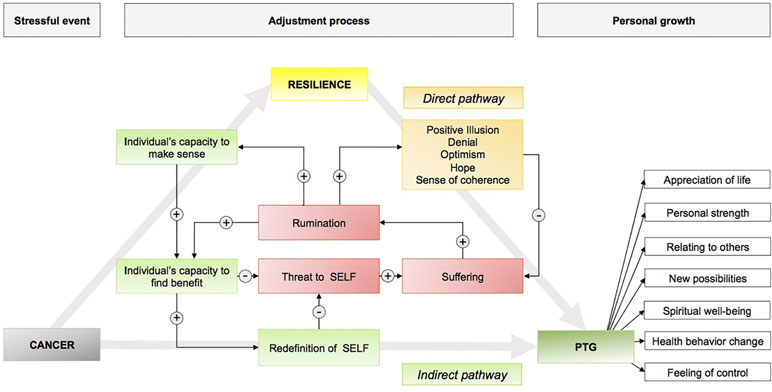
Figure 1 Conceptual framework of resilience, meaning making, and posttraumatic growth following a cancer diagnosis. Two different pathways of resilience are presented: direct pathway (orange) buffers distress and suffering via personality traits and coping abilities; the indirect pathway (75) decreases suffering by changes and redefinition of the individual’s self. Note: (+): increase; (−): decrease.
Over the last few decades, increasing evidence has been published that serious life events and life-threatening illnesses can lead not only to increased psychological distress but also to positive life changes (93, 138, 146). In this context, various research groups have established concepts pertaining to “benefit-finding” (21, 45, 135), personal growth through “constructive confrontation” (122), “stress-related growth” (109), “growth through adversity” (71), and “posttraumatic growth” (34). These concepts may be considered as indirect pathways of resilience because psychological adjustment is facilitated and accomplished by psychological processes. On the other hand, several theoretical and empirical concepts focus on the particular resistance against psychological distress that can arise in cancer patients [e.g., sense of coherence, optimism, Connor–Davidson Resilience Scale (41)] and therefore can be considered direct pathways of resilience.
Resilience can be viewed as an individual’s ability to maintain or restore relatively stable psychological and physical functioning when confronted with stressful life events and adversity (30). In the context of cancer, resilience refers to an individual’s protective attributes and/or personal characteristics, which are thought to be modifiable and to promote successful adaptation to cancer, including, among others, meaning and purpose in life, sense of coherence, optimism, positive emotions, self-esteem, self-efficacy, cognitive flexibility, coping, social support, and spirituality (51, 63). Resilience is considered a dynamic mechanism that changes over time and can be affected by life circumstances, one’s environment, and situational as well as contextual factors (92). Aversive and/or stressful experiences may cause transient perturbations, even in resilient individuals (e.g., constant mind-wandering, preoccupation, or restless sleep) (29). However, in cancer patients, there are multiple, sometimes unexpected, pathways to resilience (92). Although marked variation exists in how cancer patients cope with cancer as a disease, there is growing recognition that resilience to life-threatening situations, like cancer, is far more common than often believed (29). Many cancer patients can handle this extremely stressful experience with minimal to no effect on their daily functioning and may even experience positive emotional and personal growth (29). In addition to biological factors (e.g., gene–environment interactions) (72), individuals’ personal factors (e.g., self-efficacy, coping, optimism, and hope) (66), and environmental factors, particularly social support (129), collectively account to their resilience and psychological adaptations to the cancer experience (51).
Factors Facilitating Resilience in Cancer Patients
Meaning Making
The first several months after someone is diagnosed with cancer is a critical period, during which they are confronted with a number of physical, psychological, social, spiritual, and existential changes imposed by the disease (80). This period is characterized by existential distress, worries about health and safety, and fears about dependency, lost autonomy, and death (88). These tumor-triggered existential concerns often confuse one’s general sense that life has order and purpose and force many patients with cancer to search for new meaning in life, as they struggle to make sense of their cancer (73, 80).
Meaning making is a conceptual model that attempts to explain someone’s adjustment to his or her cancer experience (108, 110). Contrary to Antonovsky’s theory, recent literature provides evidence that conceptualizes “meaning” and “meaning making” as a behavioral process of adaptive adjustment, rather than a personality trait. Park and Folkman (111) postulated to distinguish between meaning as a coping process and a coping outcome. Meaning making as a coping process reflects attempts to balance a mismatch between situational meaning (meaning in the context of a specific event) and global meaning (global beliefs and goals) by reappraising and creating both the situational meaning and one’s global beliefs and goals. Thus, meaning can be viewed as an outcome of a successful coping process, which itself is an important element of resilience.
Theorists assume that attempts at meaning making result in better adjustment to cancer, but only under circumstances wherein meaning is derived via the process (111). For instance, in a longitudinal study of cancer survivors, meaning-making efforts were found to be related to better adaptation to stress via the successful creation of meanings generated by the cancer experience (110). In contrast, meaning-making attempts and searching for meaning are commonly associated with elevated levels of distress, poorer mental functioning, and a less positive/more negative affect (73, 139). Evidence suggests that searching for meaning is only helpful when meaning is found (73). Conversely, unsuccessful meaning-making efforts present fruitless rumination, resulting in discomfort rather than adaptive adjustment (12, 149). Some authors even recommend accepting that one’s experience has no meaning when sense cannot be made or meaning easily found and instead spend time and effort concentrating on enjoyable things and experiences and the potential for future growth (73, 127, 149).
Posttraumatic Growth
Posttraumatic growth (PTG) can be defined as subjective, positive psychological changes that arise when someone endures some major life crisis or traumatic event (137). Typically, these changes entail benefits, like increased life appreciation, renewed or altered life priorities, enhanced sense of personal strength, improved social relationships, perceived new possibilities, developing a deeper sense of spirituality and personal meaning (6, 136), increased bodily care, positive health behavior changes, and augmented feelings of personal control (137). Thus, with PTG, life becomes richer, more meaningful, and rewarding. However, it may not be implicitly associated with greater well-being or less suffering (152).
According to a theory proposed by Tedeschi and Calhoun (6, 136, 137), PTG emerges when an event is associated with a level of stress sufficient to threaten or even destroy a person’s beliefs, life expectations, or even life itself (34). For instance, being forced to cope with a potentially life-threatening disease, like cancer, can cause enough stress that someone begins to critically scrutinize his or her place in it in the world and overall worldview. This approach assumes that the disruption and distress caused by the trauma trigger cognitive processing and restructuring of the event (post-trauma processing), resulting in new insights and revised beliefs to reflect the person’s new reality (108, 125, 136). During the development of PTG, successful coping following a traumatic event occurs when the affected individual’s perception of self, others, and the meaning of the event can be reappraised and positively recreated (6, 136). In other words, deliberate rumination allows the individual to integrate the traumatic event and generate some new meaning (102).
Several authors have demonstrated that individuals who reported more stress and threat relating to a given stressful event experienced a greater degree of PTG (34, 85). The theoretic concept presumes that the more an individual reflects on the circumstances and consequences of the experience, actively tries to deal with the illness, and searches for its meaning, the more likely PTG will occur (6). Thus, PTG does not result from the trauma itself but through the struggles and efforts of dealing with the demanding situation. The literature regarding the time needed for benefit finding is inconclusive. Some authors suggest that PTG increases the longer the time interval from the traumatic event (43, 125). Contrary to these findings, in another study involving breast cancer patients, benefit-finding within the year following the diagnosis of cancer predicted better adjustment, including less distress and depression, 5 to 8 years after the initial diagnosis (36).
Connor–Davidson Resilience Scale
Resilience can be seen as a measure of an individual’s stress-coping ability (40), an outcome that might also be of high relevance when treating cancer patients. Based on Richardson’s model of biopsychospiritual balance (“homeostasis”) (116), including several theoretical concepts (e.g., Kobasa, Rutter, Lyons), Connor and Davidson developed the Connor–Davidson Resilience scale (CD-RISC) (41). It has both a long and a short version, consisting of 25 (41) and 10 items (35), respectively. Each item is scored on a 5-point Likert scale, with higher scores indicating higher levels of resilience. The CD-RISC has demonstrated considerable reliability and validity in several distinct population groups, including community samples, primary care outpatients, general psychiatric outpatients, patients in a clinical trial on generalized anxiety disorder, and PTSD patients in multiple clinical trials (41). In one study evaluating resilience in patients with PTSD, mean CD-RISC (resilience) scores ranged from 80.4 among individuals in the general population to 47.8 in patients with PTSD (41). Connor and Davidson et al. (44) found that greater resilience, as indicated by the CD-RISC scale, predicted higher recovery rates in PTSD patients. Most importantly, this same research group (41, 44) has demonstrated that either pharmacotherapy alone or combined pharmacotherapy and psychotherapy significantly promoted resilience in PTSD patients, up to a level close to that observed in the general population; such therapy also alleviated symptoms of depression and anxiety, indicating that resilience is both modifiable and treatment-responsive. These results underscore the utility of resilience, as quantified by the CD-RISC, in both clinical practice and research.
The Connor–Davidson Resilience Scale has also been administered in several studies evaluating resilience in cancer patients. Data obtained with the CD-RISC in cancer patients corroborate findings from Connor and Davidson, demonstrating that cancer patients who express greater resilience experience less psychological distress and are more well adjusted to their cancer (48, 95, 97, 118, 121, 145, 150).
Factors Determining Resilience
Each phase of the cancer experience has a profound impact on the patients’ lives (79). Many socio-contextual factors are believed to be associated with resilience in cancer patients. These characteristics refer to the strengths and positive aspects of an individual’s state of mind (40). For all phases of a cancer’s outcome trajectory, resilience is constructed from preexisting baseline characteristics, like sociodemographic and other personal attributes (e.g., social support, hope, optimism); adaptation mechanisms, like coping and medical care experience (e.g., relationships with healthcare providers); and psychosocial outcomes, like PTG and quality of life (7). Knowledge on how personal and socio-contextual resources may impede resilience to cancer is of clinical importance and may provide insights into long-term outcomes in cancer patients. The next section explores which factors promote resilience and PTG in cancer patients.
Demographic Factors
While studies on risk factors for PTSD and other psychiatric comorbidities have typically implicated female gender, minority ethnicity, less education, and, to a lesser extent, younger age (32), limited and rather inconsistent data exist on the association between sociodemographic factors and resilience in cancer patients. Some studies revealed better resilience outcomes in cancer patients who were younger, had higher levels of education and income, and were Caucasian (46, 49, 79, 87). However, studies examining the impact of gender, as well as of marital and socioeconomic status, on resilience in cancer patients have yielded ambiguous results and no consistent associations (57, 65, 79, 97). Older patients (>65 years old) account for more than 60% of cancer cases (96). Clinical data on the relationship between older age and resilience are ambiguous and conflicting. Although some authors have assumed that resilience weakens with age—due to the accumulation of risks and adversities, physical and cognitive declines, and reduced personal resources (90, 97)—some studies have uncovered increased resilience with older age (39, 65, 97). Other studies have identified a mediating effect of resilience on the relationship between age and psychological adjustment, with older individuals exhibiting better adjustment to cancer and less distress when resilience was rated high (39). These results indicate that there must be different trajectories of resilience in older individuals (90, 97).
Cancer-Related Variables
Some cancer-related variables, like disease severity and time since diagnosis, were not found to be related to cancer patients’ resilience during our review of the literature. However, disease severity and time since diagnosis do appear to impact PTG and benefit finding during patients’ experience with cancer, with higher- versus lower-stage tumors linked to reduced PTG (101). Other investigators have hypothesized that searching for meaning in life is most probably to occur in patients whose cancer is moderately life-threatening (Stage II) and prognosis somewhat uncertain, whereas benefit finding was deemed less likely to occur in individuals with Stage I (presumed curable) and Stage IV (generally incurable) disease (79). In contrast, others have postulated that time since diagnosis and treatment status are not linked to benefit finding (19), while others have concluded that time alone is sometimes sufficient to promote growth (136).
Personality-Related Variables
The literature suggests that personality-related risk and resilience factors become particularly critical when one is challenged by a serious stressor, such as a life-threatening disease like cancer (47). Personality traits that are relevant to controlling and regulating mental and emotional states are likely central in resilience pathways. Among others, a coherent self-concept, self-esteem, optimism, positive emotions, and personal control have been discussed as being important personality-related factors that aid in building resilience in cancer patients (23, 29, 47, 74), whereas neuroticism and interpersonal dependency have been linked to diminished resilience (23, 79).
The personality trait “hardiness” can buffer exposure to extreme stress and may contribute to the recovery process (61). Hardiness has three dimensions: cultivation of a sense of peace and meaning in life; sense of control over one’s experiences and outcomes; and learning and growing from life experiences, both positive and negative (74). Some evidence exists suggesting that hardiness is an important contributor to resilience and PTG in cancer survivors (22, 61). In one study of cancer survivors, hardy individuals were more likely to use active coping and social support than their less hardy peers, suggesting that hardiness helped them deal with the cancer-related distress they experienced (61). In contrast, in another study involving prostate and breast cancer patients, stressors experienced in the context of low control were more detrimental in individuals with an incoherent than coherent self-concept (47).
Several studies support the premise that the expression of positive emotions and laughter can help to reduce distress following a stressful life event and facilitate adjustments to cancer (140). In a recent study of women with newly diagnosed gynecological cancer, women who were more likely to express positive emotions (e.g., gratitude, interest, and love) reported higher resilience and better quality of life (94). Moreover, breast cancer patients who could express positive emotions during cancer treatment were more likely to reframe their cancer experience positively and feel a greater sense of peace and meaning in their lives (94).
Social Context
Social support refers to assistance provided by other people (family, friends, or others outside a professional support setting), as well as the perception that one is loved, esteemed, and valued by others (144). Evidence suggests a significant link between social support and health, with social support considered an important contributor to improving well-being and reducing distress in cancer patients (16). Family and friends may help cancer patients to process their cancer-related traumatic experiences and may be involved in meaning finding, efforts that could lead to improved interpersonal relationships (26). Patients with different types of cancer who perceive a sustainable availability of social support appear to be more likely to report high levels of resilience and lower levels of distress (49, 129). More specifically, in a study of 365 bladder cancer patients, resilience, social support, and hope accounted for 30% of the variance in patients’ quality of life (82). Similarly, among breast and head and neck cancer patients, having a partner was found to have a protective effect against anxiety and depression, relative to being single (38, 87). Furthermore, support-seeking behavior and the perception of received social support have been directly linked to PTG (48).
Coping Strategies
Coping is a critical element of resilience outcomes in cancer patients (19). Across several different studies assessing cancer survivors, those who used adaptive coping strategies (e.g., positive reappraisal, social support seeking behavior, problem-focused coping, and religious coping) reported better quality of life and indicated reduced distress (26, 28, 37, 75, 94, 107, 113), while individuals using nonadaptive coping strategies (e.g., substance use or self-blame) suffered from higher distress and impaired quality of life (62, 105). In addition, the results of several studies suggest that resilience mediates the relationship between the use of coping strategies and quality of life (94, 107, 113). These findings presume that resilient cancer patients may report higher quality of life, since they are more likely to express positive emotions, integrate their cancer experience positively, and feel a sense of peace and meaning in their lives (94). Thus, resilience and coping strategies are important in patients’ quality of life. Coping strategies have also been found to play an important role in PTG. As demonstrated in a study in adolescent cancer survivors, the use of acceptance coping strategies, as opposed to avoidant coping strategies, predicted higher levels of PTG 2 to 10 years following cancer treatment (141).
Optimism, Hope, and Spirituality
Optimism is known to have protective effects when one is dealing with cancer. In a number of studies involving cancer patients, optimism was associated with better adjustment to cancer, enhanced well-being, and reduced distress, while being predictive of treatment challenge acceptance (37, 98). Conversely, pessimism predicted avoidance, denial, and impaired quality of life (37, 112). Similarly, among long-term prostate cancer survivors, those who reported being happy, hopeful, and positive in outlook had less negative treatment outcomes than those who were negative (27).
Optimism has been positively linked to resilience in cancer patients. In one sample of colorectal cancer patients, those with high reported resilience exhibited stability in optimism or even became more optimistic, relative to those with low self-reported resilience (65). Vice versa, optimism and favorable early postoperative treatment outcomes were predictive of resilience and lower distress in women diagnosed with breast cancer (76).
Hope is considered one of the most powerful coping styles when fighting against cancer (50). Fostering hope is an existential strategy for cancer patients to adjust to, and give meaning to their cancer experience, to maintain and improve well-being, and to anticipate survival (100). Six strategies have been identified for facilitating hope during cancer treatment: building and sustaining meaningful relationships, staying positive, living in the present moment, promoting accomplishments, feeling a spiritual connection, and anticipating survival (120). One’s level of hope can change over time and depends upon internal and external factors, including personality, relationships, and social support (82). Cancer patients can develop a sense of hopelessness when distress becomes overwhelming (143), and social support may be protective against hopelessness (151). Resilience was positively correlated with hope in a study on metastatic colorectal cancer patients, indicating that resilience may improve hope, thereby emphasizing the need for resilience-fostering interventions in palliative care (128). Furthermore, among cancer survivors, optimism and hope have been linked to better adjustment and growth (115). However, optimism and hope were not associated with overall survival or with progression-free survival in another study involving metastatic colorectal cancer patients (123).
Spirituality may help cancer patients to create meaning in life, and the roles of spiritual and religious beliefs in coping with cancer and fostering resilience have been widely acknowledged (67). In addition, it has been noted that many cancer patients sense spiritual growth after they are diagnosed with cancer (56, 114).
In summary, optimism, hope, and spirituality are likely to increase with preservation of resilience and recovery from psychological distress (65). Therefore, resilience-fostering interventions to nurture optimism, hope, and spirituality during cancer treatment could assist patients trying to cope with their cancer (100, 120).
Sense of Coherence
As one of the first researchers in this field, Antonovsky (155) developed in the 1970s a theoretical construct called “sense of coherence” (13) to explain differences in the way people cope with stressful life experiences. When Antonovsky studied a group of postmenopausal women who had survived concentration camps, he discovered that one third of the women had been able to remain both mentally and physically healthy. In further research, Antonovsky developed the sense of coherence (SOC) (13) model of health. The model comprises three main components, which Antonovsky described as follows: “The sense of coherence is a global orientation that expresses the extent to which one has a pervasive, enduring, though dynamic feeling of confidence that: (1) the stimuli deriving from one’s internal and external environments in the course of living are structured, predictable and explicable; (2) the resources are available to one to meet the demands posed by these stimuli; and (3) these demands are challenges worthy of investment and engagement” (25).
Over the past several decades, increasing evidence has been gathered that supports Antonovsky’s postulation that SOC is a health-promoting factor (53, 54, 84, 132). Although Antonovsky did not develop his model by studying cancer patients, current research has evidenced a strong inverse relationship between SOC and distress (59, 103) and particularly between SOC and anxiety and depression (126, 133, 142). Furthermore, several studies found a positive correlation between quality of life and SOC in cancer patients (33, 99, 106, 134). In a more recent study, including 478 breast cancer patients and a median follow‐up time of 10 years, patients with a higher SOC score had a 63% lower risk of cancer progression, an 80% lower risk of cancer-related mortality, and an 80% lower risk of all‐cause mortality than patients with a lower SOC score (83).
Recent research revealed that SOC was a health-promoting factor also in cancer patients’ partners. In one longitudinal, quantitative study involving cancer patients and their spouses (59), a higher SOC at the time of diagnosis was significantly associated with lower levels of anxiety and depression at 14 months of follow-up. In a more recent study of 147 cancer patients and their partners, participants’ SOC was an independent and significant predictor of lower distress in both patients and their partners 6 months following cancer diagnosis (60).
In a qualitative study, our own research group used Antonovsky’s theory to analyze the experience of a diagnosis of advanced melanoma in 10 patients and their significant others (52). We found that managing their current situation; applying several coping skills, including caring for one’s relationships; and seeking social supports were the most important strategies utilized by the study participants. Of note, cancer patients and their partners reported to use these coping strategies shortly after diagnosis and at the 6-month follow-up interview. Interestingly, issues reflecting meaning and spirituality played only minor roles for patients and their partners. Distraction was one of the most important and coping mechanisms among our study participants. This finding is in accordance with previous results in the literature. For instance, a comparable study investigating patients with a brain tumor and their spouses highlighted the importance of keeping life going on as before, doing hobbies, going to work, and dealing with everyday matters in order to improve one’s sense of situational meaning and the manageability of life and eventually to reduce suffering (130).
Resilience, PTG, and Recovery From Cancer
Resilience is an important area for cancer patients because it may provide a protection against the negative effects of stress by lessening or absorbing the shock of a cancer diagnosis, the impact of aversive events, and related life changes and thus improve mental health and treatment outcomes. A growing body of literature has conclusively linked resilience, in both cancer patients and cancer survivors, with better adjustment to cancer, higher quality of life, and better mental health and treatment outcomes (49, 97, 113, 118, 124, 147, 150). More specifically, in a study investigating resilience in cancer patients undergoing allogeneic stem cell transplantation, high-resilience patients reported less anxiety and depression; higher physical, emotional, and social functioning; and a better quality of life than low-resilience patients (124). In contrast, cancer patients who reported lower levels of resilience suffered from more distress, depression (150), and cancer-related fatigue (131, 153) and exhibited poorer social adjustment 6 years following their diagnosis (77). Similar outcomes were observed for cancer survivors. For instance, low-resilience women suffering from early-stage breast cancer manifested greater distress and poorer psychosocial adjustment 6 years later (77). In another study involving older cancer survivors (≥65 years), those with high resilience scores showed higher physical functioning (49). Furthermore, in a large cross-sectional sample of 1,823 hematopoietic cell transplantation survivors, lower patient-reported resilience, as measured by the 10-item CD-RISC, was positively correlated with chronic-graft-versus-host disease of higher severity, poor performance status, more illness-related absences at work, and long-term disability (118). These results indicate that resilience is independently associated with health and psychosocial outcomes. As such, resilience should be acknowledged as a protective psychosocial factor in cancer patients.
Adjusting to cancer—while experiencing the diagnosis, treatment, adverse events, and related life changes—can lead to long-lasting negative health consequences, including distress, depression, (death-) anxieties, and adjustment disorders (4). Paradoxically, studies also have shown that overcoming cancer and its treatment may be an opportunity for personal growth, positive life changes, and improved social and emotional well-being, as a consequence of resilience (17). PTG is a process of personal change that may result from coping with a stressful event (17). It also is a complex phenomenon, with characteristics related to the type of trauma (cancer severity), context (social support and relationship with health care providers), and preexisting personal resources (self-enhancement, optimism, hope, etc)., during which positive changes and psychological distress may coexist (17). PTG is best illustrated by a curvilinear relationship, whereby stress is essential to initiate PTG, while too much stress has been found to hinder the process of PTG (29, 78).
There is a body of literature providing evidence for positives changes following cancer. In a study with breast cancer patients, most women viewed their cancer experience as more positive than negative (139). Furthermore, relative to healthy women, breast cancer survivors reported greater PTG, appreciation of life, and spiritual change (17, 101). Evidence from the literature suggests that those who perceive growth shortly after a stressful life event experience better mental health and fewer posttraumatic symptoms later (55). Furthermore, PTG has been linked to positive affect and improved life satisfaction (68). Other studies have documented relationships between PTG and improved quality of life (145), lower-level distress, greater self-esteem, and less anxiety (58).
In a qualitative study of our own (119), we investigated 31 patients with head and neck cancer and 25 female partners with regard to positive personal changes following a cancer diagnosis. Our results corroborate the concept of PTG developed by Tedeschi and Calhoun. We found that most cancer patients, as well as their female partners, reported positive changes following their cancer experience. Interestingly, the female spouses described positive changes significantly more often than patients did. Regarding quality of life and psychological distress, we found that marital satisfaction was an important moderating factor (70). In a further study of our own including 224 patients suffering from various types of cancer, we investigated responses of both patients and their partners to the PTG inventory (PTGI) (154). In this study, we aimed at investigating the contributions of gender and role (patient or partner) and the individual couples (the dyad factor: belonging to any one of the 224 couples) to variability in PTGI scores. Our data revealed that all three factors—gender, role, and dyad—contributed to PTGI total score variability, while PTGI total scores as well as all PTGI subscales were higher for patients than for partners. Furthermore, “male patient–female partner pairs” exhibited greater PTG than “female patient–male partner pairs” did. Correlations also indicated a parallel posttraumatic growth in patients and partners, irrespective of the gender and role composition.
Robust evidence supports links between resilience and PTG in cancer patients. However, the strength and direction of their correlation is less clear. In some studies, resilience was directly associated with PTG among cancer patients and survivors (48), suggesting that resilient patients experience greater PTG in reaction to a stressful event. More specifically, Dong et al. (48) found a mediating effect of resilience on perceived social support and PTG, indicating that cancer patients with high levels of perceived social support showed greater resilience and thus experienced more PTG. Contrary to this study, however, other authors have argued that resilient individuals experience PTG to a lesser extent because they are not affected profoundly enough by the stressful event; as such, they fail to experience the degree of stress and mental pressure needed to act as a catalyst for cognitive processing and meaning making (29, 145, 148).
Another explanation for these contradicting empirical findings is that there might be two different cognitive components contributing to PTG, including a constructive and an illusory aspect (The Janus-Face model of PTG) (91). The latter, specifically, may not lead to actual growth and personal change.
It is important to note that there is an ongoing debate whether the diagnosis and treatment of cancer fulfills the criteria for a traumatic event according to DSM-IV (42). Moreover, the revision of the trauma criterion from DSM-IV to DSM-5 (156) raises specific concerns regarding its applicability to cancer patients. The supporting text in DSM-5 specifically states that “A life-threatening illness or debilitating medical condition is not necessarily considered a traumatic event. Medical incidents that qualify as traumatic events involve sudden, catastrophic events.” Independently from these criteria and the fact that many cancer patients do experience severe complications or extreme adverse events, the diagnosis of cancer represents an existential threat that is experienced by patients as traumatic (24, 104). According to the concept of PTG proposed by Tedeschi and Calhoun, this stress is sufficient to trigger the process of personal change.
From a theoretical point of view, we consider two different pathways of resilience (see Figure 1). The first, a direct pathway, allows affected subjects to bounce back from adversities by different personality traits (e.g., optimism, hope, hardiness, and SOC) or coping abilities (e.g., problem-focused coping, positive reappraisal, and social support seeking). The second way, which can be viewed as an indirect pathway, leads to psychological adjustment by a process of redefinition of the self, reappraisal of beliefs, and personal growth that allows patients to feel stronger. PTG, for example, but also meaning making, reflects an indirect pathway of resilience. We postulate that the indirect pathway will be used in situations when the direct pathway was not successful or in subjects with lower individual sources of resistance (e.g., low optimism). However, further research is needed to confirm this hypothesis. It is important to note that issues of personal growth and meaning making can be specifically addressed by various psychotherapeutic approaches. Therefore, positive changes may be utilized as a foundation for the psychotherapeutic work, providing hope that the adverse experience can be successfully managed and overcome. Fostering resilience and PTG during cancer treatment may yield better psychological adjustment and psychosocial functioning during and following cancer therapy, thereby facilitating recovery from the cancer itself.
Clinical Implications
The clinical relevance of resilience has been noted for patients with life-threatening diseases like cancer. Tailoring targeted interventions to facilitate resilience in cancer patients, for instance by fostering certain baseline characteristics or improving coping and adaptation strategies, may help to foster patients’ inner strength and energy and, in turn, alleviate symptoms of psychological distress, depression, and anxiety and improve quality of life (7, 150). In fact, research has shown that resilience in cancer patients may buffer against psychological distress and improve quality of life during the disease’s trajectory (150). To date, few interventions designed to promote resilience in cancer patients have been developed and evaluated. For instance, Stress Management and Resilience Training (SMART) is a group-based cognitive behavioral therapy program developed to enhance resilience and well-being and relieve symptoms of distress and anxiety. The intervention focuses on cognitive restructuring of the stressful experience and on adjusting to it via the development of inner strength (e.g., gratitude, acceptance, purpose). Among breast cancer survivors, the SMART intervention resulted in improved resilience and quality of life and reduced symptoms of distress and anxiety, relative to the control group (89). Meaning-making interventions may indirectly promote resilience by improving dispositional and modifiable factors, like self-esteem, optimism, hope, and self-efficacy (81). More specifically, in one study, patients with advanced ovarian cancer who received a meaning-making intervention reported an improved sense of meaning and purpose in life relative to controls (64). Similar findings were observed in a study with breast and colorectal cancer patients, with improved optimism and self-efficacy demonstrated among study participants in the meaning-making intervention group (81). Another study found significant benefits of a meaning-centered psychotherapy and highlights the importance of addressing existential issues in cancer patients and survivors (31).
More recently, interest has increased in promoting resilience in palliative cancer patients: in particular, interventions to foster resilience in patients with advanced or terminal cancer who have given up hope could benefit from resilience-fostering interventions. In one study involving patients with advanced-stage cancer, resilience was directly related to higher levels of perceived social support and less hopelessness (129). Similarly, among patients with metastatic colorectal cancer, resilience and hope were positively correlated, while depression was associated with lower resilience, less hope, and higher scores for suffering (128). Given that various factors of resilience can be modified and, in turn, improve hope and quality of life, resilience-fostering interventions in the palliative care setting are of great clinical value and therefore should be initiated early during the transition to palliative care. In addition, interventions to foster resilience in caregivers of patients with advanced and incurable cancer are equally important (69, 86, 117). This being said, only few studies on resilience in family caregivers of terminally ill cancer patients exist, and further investigation is needed to understand caregivers’ support needs to develop strategies to improve coping and resilience in this population (69).
Conclusions
Resilience is an important protective factor against psychological distress and consequently is closely related to mental health. Biological (gene–environment), personal (e.g., sense of coherence, optimism, and hope), and, most notable, social (e.g., social support) factors contribute to the cancer patient’s resilience and, therefore, to favorable psychological and treatment-related outcomes.
PTG as an indirect path of resilience is an important phenomenon during adjustments to cancer, and is linked to less distress, better mental health, and improved quality of life. Its theoretical foundation within the framework of resilience is only marginally investigated and not completely understood. Some studies have demonstrated a positive relationship between resilience and PTG, while others have found high levels of resilience to be associated with low PTG scores.
Improving resilience through targeted interventions that promote positive adaptations to cancer, while improving health outcomes by strengthening personal and social resources and enabling effective coping strategies, might be an effective intervention strategy to foster PTG in cancer patients. Promoting resilience through PTG should be an essential component of cancer care, and resilience-fostering factors can be improved throughout every stage of the cancer continuum.
Author Contributions
AS and JJ wrote the manuscript. Both AS and JJ amended the manuscript.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The handling editor declared a past supervisory role with one of the authors AS.
References
1. Bergerot CD, Clark KL, Nonino A, Waliany S, Buso MM, Loscalzo M. Course of distress, anxiety, and depression in hematological cancer patients: association between gender and grade of neoplasm. Palliat Support Care (2015) 13(2):115–23. doi: 10.1017/S1478951513000849
2. Linden W, Vodermaier A, Mackenzie R, Greig D. Anxiety and depression after cancer diagnosis: prevalence rates by cancer type, gender, and age. J Affect Disord (2012) 141(2–3):343–51. doi: 10.1016/j.jad.2012.03.025
3. Saboonchi F, Petersson LM, Wennman-Larsen A, Alexanderson K, Brannstrom R, Vaez M. Changes in caseness of anxiety and depression in breast cancer patients during the first year following surgery: patterns of transiency and severity of the distress response. Eur J Oncol Nurs (2014) 18(6):598–604. doi: 10.1016/j.ejon.2014.06.007
4. Rodin G, Lo C, Mikulincer M, Donner A, Gagliese L, Zimmermann C. Pathways to distress: the multiple determinants of depression, hopelessness, and the desire for hastened death in metastatic cancer patients. Soc Sci Med (1982) (2009) 68(3):562–9. doi: 10.1016/j.socscimed.2008.10.037
5. Lo C, Hales S, Zimmermann C, Gagliese L, Rydall A, Rodin G. Measuring death-related anxiety in advanced cancer: preliminary psychometrics of the Death and Dying Distress Scale. J Pediatr Hematol Oncol (2011) 33 (Suppl 2):S140–5. doi: 10.1097/MPH.0b013e318230e1fd
6. Tedeschi RG, Calhoun LG. Trauma and transformation: growing in the aftermath of suffering. (1995). Available from: http://sk.sagepub.com/books/trauma-and-transformation.
7. Molina Y, Yi JC, Martinez-Gutierrez J, Reding KW, Yi-Frazier JP, Rosenberg AR. Resilience among patients across the cancer continuum: diverse perspectives. Clin J Oncol Nurs (2014) 18(1):93–101. doi: 10.1188/14.CJON.93-101
8. Chan CMH, Ng CG, Taib NA, Wee LH, Krupat E, Meyer F. Course and predictors of post-traumatic stress disorder in a cohort of psychologically distressed patients with cancer: a 4-year follow-up study. Cancer (2018) 124(2):406–16. doi: 10.1002/cncr.30980
9. Wu X, Wang J, Cofie R, Kaminga AC, Liu A. Prevalence of posttraumatic stress disorder among breast cancer patients: a meta-analysis. Iran J Public Health (2016) 45(12):1533–44. PMC5207094
10. Lin YH, Kao CC, Wu SF, Hung SL, Yang HY, Tung HY. Risk factors of post-traumatic stress symptoms in patients with cancer. J Clin Nurs (2017) 26(19–20):3137–43. doi: 10.1111/jocn.13662
11. Swartzman S, Booth JN, Munro A, Sani F. Posttraumatic stress disorder after cancer diagnosis in adults: a meta-analysis. Depress Anxiety (2017) 34(4):327–39. doi: 10.1002/da.22542
12. Bonanno GA, Papa A, Lalande K, Zhang N, Noll JG. Grief processing and deliberate grief avoidance: a prospective comparison of bereaved spouses and parents in the United States and the People’s Republic of China. J Consult Clin Psychol (2005) 73(1):86–98. doi: 10.1037/0022-006X.73.1.86
13. American Psychiatric Association. Diagnostic and statistical manual of mental disorders (4th ed., text rev.). Washington, DC. (2000).
14. Pai A, Suris AM, North CS. Posttraumatic stress disorder in the DSM-5: controversy, change, and conceptual considerations. Behav Sci (2017) 7(1):7. doi: 10.3390/bs7010007
15. Carver CS. Resilience and thriving: issues, models, and linkages. J Soc Issues (1998) 54(2):245–66. doi: 10.1111/j.1540-4560.1998.tb01217.x
16. Gouzman J, Cohen M, Ben-Zur H, Shacham-Shmueli E, Aderka D, Siegelmann-Danieli N, et al. Resilience and psychosocial adjustment in digestive system cancer. J Clin Psychol Med Settings (2015) 22(1):1–13. doi: 10.1007/s10880-015-9416-9
17. Ruini C, Vescovelli F, Albieri E. Post-traumatic growth in breast cancer survivors: new insights into its relationships with well-being and distress. J Clin Psychol Med Settings (2013) 20(3):383–91. doi: 10.1007/s10880-012-9340-1
18. Danhauer SC, Russell GB, Tedeschi RG, Jesse MT, Vishnevsky T, Daley K, et al. A longitudinal investigation of posttraumatic growth in adult patients undergoing treatment for acute leukemia. J Clin Psychol Med Settings (2013) 20(1):13–24. doi: 10.1007/s10880-012-9304-5
19. Lelorain S, Bonnaud-Antignac A, Florin A. Long term posttraumatic growth after breast cancer: prevalence, predictors and relationships with psychological health. J Clin Psychol Med Settings (2010) 17(1):14–22. doi: 10.1007/s10880-009-9183-6
20. Chan CL, Chan TH, Ng SM. The Strength-Focused and Meaning-Oriented Approach to Resilience and Transformation (SMART): a body-mind-spirit approach to trauma management. Soc Work Health Care (2006) 43(2–3):9–36. doi: 10.1300/J010v43n02_03
21. Affleck G, Tennen H. Construing benefits from adversity: adaptational significance and dispositional underpinnings. J Pers (1996) 64(4):899–922. doi: 10.1111/j.1467-6494.1996.tb00948.x
22. Aflakseir A, Nowroozi S, Mollazadeh J, Goodarzi MA. The role of psychological hardiness and marital satisfaction in predicting posttraumatic growth in a sample of women with breast cancer in Isfahan. Iran J Cancer Prev (2016) 9(4):e4080. doi: 10.17795/ijcp-4080
23. Amstadter AB, Moscati A, Oxon MA, Maes HH, Myers JM, Kendler KS. Personality, cognitive/psychological traits and psychiatric resilience: a multivariate twin study. Pers Individ Dif (2016) 91:74–9. doi: 10.1016/j.paid.2015.11.041
24. Andrykowski MA, Steffens RF, Bush HM, Tucker TC. Lung cancer diagnosis and treatment as a traumatic stressor in DSM-IV and DSM-5: prevalence and relationship to mental health outcomes. J Trauma Stress (2015) 28(3):206–13. doi: 10.1002/jts.22005
25. Antonovsky A. Unraveling the mystery of health: how people manage stress and stay well. San Francisco: Jossey-Bass (1987).
26. Barskova T, Oesterreich R. Post-traumatic growth in people living with a serious medical condition and its relations to physical and mental health: a systematic review. Disabil Rehabil (2009) 31(21):1709–33. doi: 10.1080/09638280902738441
27. Blank TO, Bellizzi KM. After prostate cancer: predictors of well-being among long-term prostate cancer survivors. Cancer (2006) 106(10):2128–35. doi: 10.1002/cncr.21865
28. Boehmer S, Luszczynska A, Schwarzer R. Coping and quality of life after tumor surgery: personal and social resources promote different domains of quality of life. Anxiety Stress Coping (2007) 20(1):61–75. doi: 10.1080/10615800701195439
29. Bonanno GA. Loss, trauma, and human resilience: have we underestimated the human capacity to thrive after extremely aversive events? Am Psychol (2004) 59(1):20–8. doi: 10.1037/0003-066X.59.1.20
30. Bonanno GA, Westphal M, Mancini AD. Resilience to loss and potential trauma. Annu Rev Clin Psychol (2011) 7:511–35. doi: 10.1146/annurev-clinpsy-032210-104526
31. Breitbart W, Pessin H, Rosenfeld B, Applebaum AJ, Lichtenthal WG, Li Y, et al. Individual meaning-centered psychotherapy for the treatment of psychological and existential distress: a randomized controlled trial in patients with advanced cancer. Cancer (2018) 124(15):3231–9. doi: 10.1002/cncr.31539
32. Brewin CR, Andrews B, Valentine JD. Meta-analysis of risk factors for posttraumatic stress disorder in trauma-exposed adults. J Consult Clin Psychol (2000) 68(5):748–66. doi: 10.1037/0022-006X.68.5.748
33. Bruscia K, Shultis C, Dennery K, Dileo C. Predictive factors in the quality of life of cancer inpatients. J Psychosoc Oncol (2008) 26(4):75–90. doi: 10.1080/07347330802359602
34. Calhoun LG, Tedeschi RG. Handbook of posttraumatic growth: research & practice. Mahwah, NJ, US: Lawrence Erlbaum Associates Publishers (2006).
35. Campbell-Sills L, Stein MB. Psychometric analysis and refinement of the Connor–Davidson Resilience Scale (CD-RISC): validation of a 10-item measure of resilience. J Trauma Stress (2007) 20(6):1019–28. doi: 10.1002/jts.20271
36. Carver CS, Antoni MH. Finding benefit in breast cancer during the year after diagnosis predicts better adjustment 5 to 8 years after diagnosis. Health Psychol (2004) 23(6):595–8. doi: 10.1037/0278-6133.23.6.595
37. Carver CS, Pozo C, Harris SD, Noriega V, Scheier MF, Robinson DS, et al. How coping mediates the effect of optimism on distress: a study of women with early stage breast cancer. J Pers Soc Psychol (1993) 65(2):375–90. doi: 10.1037/0022-3514.65.2.375
38. Carver CS, Smith RG, Petronis VM, Antoni MH. Quality of life among long-term survivors of breast cancer: different types of antecedents predict different classes of outcomes. Psychooncology (2006) 15(9):749–58. doi: 10.1002/pon.1006
39. Cohen M, Baziliansky S, Beny A. The association of resilience and age in individuals with colorectal cancer: an exploratory cross-sectional study. J Geriatr Oncol (2014) 5(1):33–9. doi: 10.1016/j.jgo.2013.07.009
40. Connor KM. Assessment of resilience in the aftermath of trauma. J Clin Psychiatry (2006) 67(Suppl 2):46–9.
41. Connor KM, Davidson JR. Development of a new resilience scale: the Connor–Davidson Resilience Scale (CD-RISC). Depress Anxiety (2003) 18(2):76–82. doi: 10.1002/da.10113
42. Cordova MJ, Riba MB, Spiegel D. Post-traumatic stress disorder and cancer. Lancet Psychiatry (2017) 4(4):330–8. doi: 10.1016/S2215-0366(17)30014-7
43. Cormio C, Muzzatti B, Romito F, Mattioli V, Annunziata MA. Posttraumatic growth and cancer: a study 5 years after treatment end. Support Care Cancer (2017) 25(4):1087–96. doi: 10.1007/s00520-016-3496-4
44. Davidson JR, Payne VM, Connor KM, Foa EB, Rothbaum BO, Hertzberg MA, et al. Trauma, resilience and saliostasis: effects of treatment in post-traumatic stress disorder. Int Clin Psychopharmacol (2005) 20(1):43–8. doi: 10.1097/00004850-200501000-00009
45. Davis CG, Nolen-Hoeksema S, Larson J. Making sense of loss and benefiting from the experience: two construals of meaning. J Pers Soc Psychol (1998) 75(2):561–74. doi: 10.1037/0022-3514.75.2.561
46. Di Giacomo D, Cannita L, Rainieri J, Cocciolone V, Passafiume D, Ficorella C. Breast cancer and psychological resilience among young women. J Psychopathol (2016) 22:191–5.
47. Diehl M, Hay EL. Personality-related risk and resilience factors in coping with daily stress among adult cancer patients. Res Hum Dev (2013) 10(1):47–69. doi: 10.1080/15427609.2013.760259
48. Dong X, Li G, Liu C, Kong L, Fang Y, Kang X, et al. The mediating role of resilience in the relationship between social support and posttraumatic growth among colorectal cancer survivors with permanent intestinal ostomies: a structural equation model analysis. Eur J Oncol Nurs (2017) 29:47–52. doi: 10.1016/j.ejon.2017.04.007
49. Duan-Porter W, Cohen HJ, Demark-Wahnefried W, Sloane R, Pendergast JF, Snyder DC, et al. Physical resilience of older cancer survivors: an emerging concept. J Geriatr Oncol (2016) 7(6):471–8. doi: 10.1016/j.jgo.2016.07.009
50. Ebright PR, Lyon B. Understanding hope and factors that enhance hope in women with breast cancer. Oncol Nurs Forum (2002) 29(3):561–8. doi: 10.1188/02.ONF.561-568
51. Eicher M, Matzka M, Dubey C, White K. Resilience in adult cancer care: an integrative literature review. Oncol Nurs Forum (2015) 42(1):E3–16. doi: 10.1188/15.ONF.E3-E16
52. Engeli L, Moergeli H, Binder M, Drabe N, Meier C, Buechi S, et al. Resilience in patients and spouses faced with malignant melanoma. Eur J Cancer Care (Engl) (2016) 25(1):122–31. doi: 10.1111/ecc.12220
53. Eriksson M, Lindstrom B. Antonovsky’s sense of coherence scale and the relation with health: a systematic review. J Epidemiol Community Health (2006) 60(5):376–81. doi: 10.1136/jech.2005.041616
54. Eriksson M, Lindstrom B. Validity of Antonovsky’s sense of coherence scale: a systematic review. J Epidemiol Community Health (2005) 59(6):460–6. doi: 10.1136/jech.2003.018085
55. Frazier P, Conlon A, Tashiro T, Sass S. Posttraumtic growth: finding meaning through trauma. In: Selected proceedings on searching for meaning in the new millennium. Vancouver: BC: INPM Press (2002).
56. Gall TL, Charbonneau C, Florack P. The relationship between religious/spiritual factors and perceived growth following a diagnosis of breast cancer. Psychol Health (2011) 26(3):287–305. doi: 10.1080/08870440903411013
57. Goldberg RJ, Cullen LO. Factors important to psychosocial adjustment to cancer: a review of the evidence. Soc Sci Med (1982) (1985) 20:803–7.
58. Groarke A, Curtis R, Groarke JM, Hogan MJ, Gibbons A, Kerin M. Post-traumatic growth in breast cancer: how and when do distress and stress contribute? Psychooncology (2017) 26(7):967–74. doi: 10.1002/pon.4243
59. Gustavsson-Lilius M, Julkunen J, Keskivaara P, Hietanen P. Sense of coherence and distress in cancer patients and their partners. Psychooncology (2007) 16(12):1100–10. doi: 10.1002/pon.1173
60. Gustavsson-Lilius M, Julkunen J, Keskivaara P, Lipsanen J, Hietanen P. Predictors of distress in cancer patients and their partners: the role of optimism in the sense of coherence construct. Psychol Health (2012) 27(2): 178–95. doi: 10.1080/08870446.2010.484064
61. Hamama-Raz Y. Does psychological adjustment of melanoma survivors differs between genders? Psychooncology (2012) 21(3):255–63. doi: 10.1002/pon.1889
62. Helgeson VS, Snyder P, Seltman H. Psychological and physical adjustment to breast cancer over 4 years: identifying distinct trajectories of change. Health Psychol (2004) 23(1):3–15. doi: 10.1037/0278-6133.23.1.3
63. Helmreich I, Kunzler A, Chmitorz A, König J, Binder H, Wessa M, et al. Psychological interventions for resilience enhancement in adults. Cochrane Database Syst Rev (2017) (2). doi: 10.1002/14651858.CD012527
64. Henry M, Cohen SR, Lee V, Sauthier P, Provencher D, Drouin P, et al. The Meaning-Making intervention (MMi) appears to increase meaning in life in advanced ovarian cancer: a randomized controlled pilot study. Psychooncology (2010) 19(12):1340–7. doi: 10.1002/pon.1764
65. Hou WK, Law CC, Yin J, Fu YT. Resource loss, resource gain, and psychological resilience and dysfunction following cancer diagnosis: a growth mixture modeling approach. Health Psychol (2010) 29(5):484–95. doi: 10.1037/a0020809
66. Hu T, Zhang D, Wang J. A meta-analysis of the trait resilience and mental health. Pers Individ Dif (2015) 76:18–27. doi: 10.1016/j.paid.2014.11.039
67. Hunter-Hernández M, Costas-Muñíz R, Gany F. Missed opportunity: spirituality as a bridge to resilience in Latinos with cancer. J Relig Health (2015) 54(6):2367–75. doi: 10.1007/s10943-015-0020-y
68. Husson O, Zebrack B, Block R, Embry L, Aguilar C, Hayes-Lattin B, et al. Posttraumatic growth and well-being among adolescents and young adults (AYAs) with cancer: a longitudinal study. Support Care Cancer (2017) 25(9):2881–90. doi: 10.1007/s00520-017-3707-7
69. Hwang IC, Kim YS, Lee YJ, Choi YS, Hwang SW, Kim HM, et al. Factors associated with caregivers’ resilience in a terminal cancer care setting. Am J Hospice Palliative Care (2018) 35(4):677–83. doi: 10.1177/1049909117741110
70. Jenewein J, Zwahlen RA, Zwahlen D, Drabe N, Moergeli H, Buchi S. Quality of life and dyadic adjustment in oral cancer patients and their female partners. Eur J Cancer Care (Engl) (2008) 17(2):127–35. doi: 10.1111/j.1365-2354.2007.00817.x
71. Joseph S, Linley PA, Andrews L, Harris G, Howle B, Woodward C, et al. Assessing positive and negative changes in the aftermath of adversity: psychometric evaluation of the changes in outlook questionnaire. Psychol Assess (2005) 17(1):70–80. doi: 10.1037/1040-3590.17.1.70
72. Kalisch R, Muller MB, Tuscher O. A conceptual framework for the neurobiological study of resilience. Behav Brain Sci (2015) 38:e92. doi: 10.1017/S0140525X1400082X
73. Kernan WD, Lepore SJ. Searching for and making meaning after breast cancer: prevalence, patterns, and negative affect. Soc Sci Med (1982) (2009) 68(6):1176–82. doi: 10.1016/j.socscimed.2008.12.038
74. Kobasa SC. Stressful life events, personality, and health: an inquiry into hardiness. J Pers Soc Psychol (1979) 37(1):1–11. doi: 10.1037/0022-3514.37.1.1
75. Kraemer LM, Stanton AL, Meyerowitz BE, Rowland JH, Ganz PA. A longitudinal examination of couples’ coping strategies as predictors of adjustment to breast cancer. J Fam Psychol (2011) 25(6):963–72. doi: 10.1037/a0025551
76. Lam WW, Bonanno GA, Mancini AD, Ho S, Chan M, Hung WK, et al. Trajectories of psychological distress among Chinese women diagnosed with breast cancer. Psychooncology (2010) 19(10):1044–51. doi: 10.1002/pon.1658
77. Lam WW, Shing YT, Bonanno GA, Mancini AD, Fielding R. Distress trajectories at the first year diagnosis of breast cancer in relation to 6 years survivorship. Psychooncology (2012) 21(1):90–9. doi: 10.1002/pon.1876
78. Lechner SC, Carver CS, Antoni MH, Weaver KE, Phillips KM. Curvilinear associations between benefit finding and psychosocial adjustment to breast cancer. J Consult Clin Psychol (2006) 74(5):828–40. doi: 10.1037/0022-006X.74.5.828
79. Lechner SC, Zakowski SG, Antoni MH, Greenhawt M, Block K, Block P. Do sociodemographic and disease-related variables influence benefit-finding in cancer patients? Psychooncology (2003) 12(5):491–9. doi: 10.1002/pon.671
80. Lee V. The existential plight of cancer: meaning making as a concrete approach to the intangible search for meaning. Support Care Cancer (2008) 16(7):779–85. doi: 10.1007/s00520-007-0396-7
81. Lee V, Robin Cohen S, Edgar L, Laizner AM, Gagnon AJ. Meaning-making intervention during breast or colorectal cancer treatment improves self-esteem, optimism, and self-efficacy. Soc Sci Med (1982) (2006) 62(12):3133–45. doi: 10.1016/j.socscimed.2005.11.041
82. Li M-Y, Yang Y-L, Liu L, Wang L. Effects of social support, hope and resilience on quality of life among Chinese bladder cancer patients: a cross-sectional study. Health Qual Life Outcomes (2016) 14:73. doi: 10.1186/s12955-016-0481-z
83. Lindblad C, Langius-Eklof A, Petersson LM, Sackey H, Bottai M, Sandelin K. Sense of coherence is a predictor of survival: a prospective study in women treated for breast cancer. Psychooncology (2018) 27(6):1615–21. doi: 10.1002/pon.4702
84. Lindstrom B, Eriksson M. Salutogenesis. J Epidemiol Community Health (2005) 59(6):440–2. doi: 10.1136/jech.2005.034777
85. Linley PA, Joseph S. Positive change following trauma and adversity: a review. J Trauma Stress (2004) 17(1):11–21. doi: 10.1023/B:JOTS.0000014671.27856.7e
86. Lipsman N, Skanda A, Kimmelman J, Bernstein M. The attitudes of brain cancer patients and their caregivers towards death and dying: a qualitative study. BMC Palliat Care (2007) 6:7. doi: 10.1186/1472-684X-6-7
87. Llewellyn CD, Horney DJ, McGurk M, Weinman J, Herold J, Altman K, et al. Assessing the psychological predictors of benefit finding in patients with head and neck cancer. Psychooncology (2013) 22(1):97–105. doi: 10.1002/pon.2065
88. Lo C, Hales S, Jung J, Chiu A, Panday T, Rydall A, et al. Managing Cancer and Living Meaningfully (CALM): phase 2 trial of a brief individual psychotherapy for patients with advanced cancer. Palliat Med (2014) 28(3):234–42. doi: 10.1177/0269216313507757
89. Loprinzi CE, Prasad K, Schroeder DR, Sood A. Stress Management and Resilience Training (SMART) program to decrease stress and enhance resilience among breast cancer survivors: a pilot randomized clinical trial. Clinical Breast Cancer (2011) 11(6):364–8. doi: 10.1016/j.clbc.2011.06.008
90. MacLeod S, Musich S, Hawkins K, Alsgaard K, Wicker ER. The impact of resilience among older adults. Geriatr Nurs (New York, NY) (2016) 37(4):266–72. doi: 10.1016/j.gerinurse.2016.02.014
91. Maercker A, Zoellner T. The Janus face of self-perceived growth: toward a two-component model of posttraumatic growth. Psychol Inq (2004) 15:41–8. doi: 10.1016/j.cpr.2006.01.008
92. Mancini AD, Bonanno GA. Predictors and parameters of resilience to loss: toward an individual differences model. J Pers (2009) 77(6):1805–32. doi: 10.1111/j.1467-6494.2009.00601.x
93. Manne S, Ostroff J, Winkel G, Goldstein L, Fox K, Grana G. Posttraumatic growth after breast cancer: patient, partner, and couple perspectives. Psychosom Med (2004) 66(3):442–54. doi: 10.1097/01.psy.0000127689.38525.7d
94. Manne SL, Myers-Virtue S, Kashy D, Ozga M, Kissane D, Heckman C, et al. Resilience, positive coping, and quality of life among women newly diagnosed with gynecological cancers. Cancer Nurs (2015) 38(5):375–82. doi: 10.1097/NCC.0000000000000215
95. Markovitz SE, Schrooten W, Arntz A, Peters ML. Resilience as a predictor for emotional response to the diagnosis and surgery in breast cancer patients. Psychooncology (2015) 24(12):1639–45. doi: 10.1002/pon.3834
96. Marosi C, Köller M. Challenge of cancer in the elderly. ESMO Open (2016) 1(3):e000020. doi: 10.1136/esmoopen-2015-000020
97. Matzka M, Mayer H, Köck-Hódi S, Moses-Passini C, Dubey C, Jahn P, et al. Relationship between resilience, psychological distress and physical activity in cancer patients: a cross-sectional observation study. PLoS One (2016) 11(4):e0154496. doi: 10.1371/journal.pone.0154496
98. Miller DL, Manne SL, Taylor K, Keates J, Dougherty J. Psychological distress and well-being in advanced cancer: the effects of optimism and coping. J Clin Psychol Med Settings (1996) 3(2):115–30. doi: 10.1007/BF01996132
99. Mizuno M, Asano Y, Sumi T, Inoue Y. Adaptation status and related factors at 2 time points after surgery in patients with gastrointestinal tract cancer. Cancer Nurs (2011) 34(1):41–8. doi: 10.1097/NCC.0b013e3181ef69c3
100. Moadel A, Morgan C, Fatone A, Grennan J, Carter J, Laruffa G, et al. Seeking meaning and hope: self-reported spiritual and existential needs among an ethnically-diverse cancer patient population. Psychooncology (1999) 8(5):378–85. doi: 10.1002/(SICI)1099-1611(199909/10)8:5<378::AID-PON406>3.0.CO;2-A
101. Mols F, Vingerhoets AJ, Coebergh JW, de Poll-Franse LV. Well-being, posttraumatic growth and benefit finding in long-term breast cancer survivors. Psychol Health (2009) 24(5):583–95. doi: 10.1080/08870440701671362
102. Morris BA, Shakespeare-Finch J. Rumination, post-traumatic growth, and distress: structural equation modelling with cancer survivors. Psychooncology (2011) 20(11):1176–83. doi: 10.1002/pon.1827
103. Mullen PM. Sense of coherence as a mediator of stress for cancer patients and spouses. J Psychosoc Oncol (1994) 11(3):23. doi: 10.1300/J077V11N03_02
104. Mulligan EA, Wachen JS, Naik AD, Gosian J, Moye J. Cancer as a criterion a traumatic stressor for veterans: prevalence and correlates. Psychol Trauma (2014) 6(Suppl 1):S73–S81. doi: 10.1037/a0033721
105. Nuray KA, Asli E. Variables related to stress-related growth among Turkish breast cancer patients. Stress Health (2007) 23(5):315–22. doi: 10.1002/smi.1154
106. Paika V, Almyroudi A, Tomenson B, Creed F, Kampletsas EO, Siafaka V, et al. Personality variables are associated with colorectal cancer patients’ quality of life independent of psychological distress and disease severity. Psychooncology (2010) 19(3):273–82. doi: 10.1002/pon.1563
107. Pan CJ, Liu HC, Liang SY, Liu CY, Wu WW, Cheng SF. Resilience and coping strategies influencing the quality of life in patients with brain tumor. Clin Nurs Res (2017). doi: 10.1177/1054773817714562
108. Park CL. Making sense of the meaning literature: an integrative review of meaning making and its effects on adjustment to stressful life events. Psychol Bull (2010) 136(2):257–301. doi: 10.1037/a0018301
109. Park CL, Cohen LH, Murch RL. Assessment and prediction of stress-related growth. J Pers (1996) 64:71–105. doi: 10.1111/j.1467-6494.1996.tb00815.x
110. Park CL, Edmondson D, Fenster JR, Blank TO. Meaning making and psychological adjustment following cancer: the mediating roles of growth, life meaning, and restored just-world beliefs. J Consult Clin Psychol (2008) 76(5):863–75. doi: 10.1037/a0013348
111. Park CL, Folkman S. Meaning in the context of stress and coping. Rev Gen Psychol (1997) 1(2):115–44. doi: 10.1037/1089-2680.1.2.115
112. Petersen LR, Clark MM, Novotny P, Kung S, Sloan JA, Patten CA, et al. Relationship of optimism-pessimism and health-related quality of life in breast cancer survivors. J Psychosoc Oncol (2008) 26(4):15–32. doi: 10.1080/07347330802359578
113. Popa-Velea O, Diaconescu L, Jidveian Popescu M, Trutescu C. Resilience and active coping style: effects on the self-reported quality of life in cancer patients. Int J Psychiatry Med (2017) 52(2):124–36. doi: 10.1177/0091217417720895
114. Post-White J, Ceronsky C, Kreitzer M. Hope, spirituality, sense of coherence, and quality of life in patients with cancer. Oncol Nurs Forum (1996) 23:1571–9.
115. Rajandram RK, Ho SMY, Samman N, Chan N, McGrath C, Zwahlen RA. Interaction of hope and optimism with anxiety and depression in a specific group of cancer survivors: a preliminary study. BMC Res Notes (2011) 4:519–25. doi: 10.1186/1756-0500-4-519
116. Richardson GE. The metatheory of resilience and resiliency. J Clin Psychol (2002) 58(3):307–21. doi: 10.1002/jclp.10020
117. Roen I, Stifoss-Hanssen H, Grande G, Brenne AT, Kaasa S, Sand K, et al. Resilience for family carers of advanced cancer patients-how can health care providers contribute? A qualitative interview study with carers. Palliat Med (2018). doi: 10.1177/0269216318777656
118. Rosenberg AR, Syrjala KL, Martin PJ, Flowers ME, Carpenter PA, Salit RB, et al. Resilience, health, and quality of life among long-term survivors of hematopoietic cell transplantation. Cancer (2015) 121(23):4250–7. doi: 10.1002/cncr.29651
119. Ruf M, Buchi S, Moergeli H, Zwahlen RA, Jenewein J. Positive personal changes in the aftermath of head and neck cancer diagnosis: a qualitative study in patients and their spouses. Head Neck (2009) 31(4):513–20. doi: 10.1002/hed.21000
120. Saleh US, Brockopp DY. Hope among patients with cancer hospitalized for bone marrow transplantation: a phenomenologic study. Cancer Nurs (2001) 24(4):308–14. doi: 10.1097/00002820-200108000-00012
121. Scali J, Gandubert C, Ritchie K, Soulier M, Ancelin ML, Chaudieu I. Measuring resilience in adult women using the 10-items Connor–Davidson Resilience Scale (CD-RISC). PLoS One (2012) 7(6):e39879. doi: 10.1371/journal.pone.0039879
122. Schaefer JA, Moos RH. Life crisis and personal growth. In: Carpenter BN Personal coping, theory, research and application. (1992). p. 149–70.
123. Schofield PE, Stockler MR, Zannino D, Tebbutt NC, Price TJ, Simes RJ, et al. Hope, optimism and survival in a randomised trial of chemotherapy for metastatic colorectal cancer. Support Care Cancer (2016) 24(1):401–8. doi: 10.1007/s00520-015-2792-8
124. Schumacher A, Sauerland C, Silling G, Berdel WE, Stelljes M. Resilience in patients after allogeneic stem cell transplantation. Support Care Cancer (2014) 22(2):487–93. doi: 10.1007/s00520-013-2001-6
125. Sears SR, Stanton AL, Danoff-Burg S. The yellow brick road and the emerald city: benefit finding, positive reappraisal coping and posttraumatic growth in women with early-stage breast cancer. Health Psychol (2003) 22(5):487–97. doi: 10.1037/0278-6133.22.5.487
126. Siglen E, Bjorvatn C, Engebretsen LF, Berglund G, Natvig GK. The influence of cancer-related distress and sense of coherence on anxiety and depression in patients with hereditary cancer: a study of patients’ sense of coherence 6 months after genetic counseling. J Genet Couns (2007) 16(5):607–15. doi: 10.1007/s10897-007-9095-2
127. Silver RL, Boon C, Stones MH. Searching for meaning in misfortune: making sense of incest. J Soc Issues (1983) 39(2):81–101. doi: 10.1111/j.1540-4560.1983.tb00142.x
128. Solano JP, da Silva AG, Soares IA, Ashmawi HA, Vieira JE. Resilience and hope during advanced disease: a pilot study with metastatic colorectal cancer patients. BMC Palliat Care (2016) 15:70. doi: 10.1186/s12904-016-0139-y
129. Somasundaram RO, Devamani KA. A comparative study on resilience, perceived social support and hopelessness among cancer patients treated with curative and palliative care. Indian J Palliat Care (2016) 22(2):135–40. doi: 10.4103/0973-1075.179606
130. Strang S, Strang P. Spiritual thoughts, coping and ‘sense of coherence’ in brain tumour patients and their spouses. Palliat Med (2001) 15(2):127–34. doi: 10.1191/026921601670322085
131. Strauss B, Brix C, Fischer S, Leppert K, Fuller J, Roehrig B, et al. The influence of resilience on fatigue in cancer patients undergoing radiation therapy (RT). J Cancer Res Clin Oncol (2007) 133(8):511–8. doi: 10.1007/s00432-007-0195-z
132. Surtees P, Wainwright N, Luben R, Khaw KT, Day N. Sense of coherence and mortality in men and women in the EPIC-Norfolk United Kingdom prospective cohort study. Am J Epidemiol (2003) 158(12):1202–9. doi: 10.1093/aje/kwg272
133. Tagay S, Senf W, Schopper N, Mewes R, Bockisch A, Gorges R. Protective factors for anxiety and depression in thyroid cancer patients. Z Psychosom Med Psychother (2007) 53(1):62–74. doi: 10.13109/zptm.2007.53.1.62
134. Tang ST, Li CY, Chen CC. Trajectory and determinants of the quality of life of family caregivers of terminally ill cancer patients in Taiwan. Qual Life Res (2008) 17(3):387–95. doi: 10.1007/s11136-008-9316-7
135. Taylor SE. Adjustment to threatening events: a theory of cognitive adaptation. Am Psychol (1983) 38:1161–73. doi: 10.1037/0003-066X.38.11.1161
136. Tedeschi RG, Calhoun LG. The posttraumatic growth inventory: measuring the positive legacy of trauma. J Trauma Stress (1996) 9(3):455–71. doi: 10.1002/jts.2490090305
137. Tedeschi RG, Calhoun LG. Posttraumatic growth: conceptual foundations and empirical evidence. Psychol Inq (2004) 15(1):1–18. doi: 10.1207/s15327965pli1501_01
138. Thornton AA, Perez MA. Posttraumatic growth in prostate cancer survivors and their partners. Psychooncology (2006) 15(4):285–96. doi: 10.1002/pon.953
139. Tomich PL, Helgeson VS. Five years later: a cross-sectional comparison of breast cancer survivors with healthy women. Psychooncology (2002) 11(2):154–69. doi: 10.1002/pon.570
140. Tugade MM, Fredrickson BL, Barrett LF. Psychological resilience and positive emotional granularity: examining the benefits of positive emotions on coping and health. J Pers (2004) 72(6):1161–90. doi: 10.1111/j.1467-6494.2004.00294.x
141. Turner-Sack AM, Menna R, Setchell SR, Maan C, Cataudella D. Posttraumatic growth, coping strategies, and psychological distress in adolescent survivors of cancer. J Pediatr Oncol Nurs (2012) 29(2):70–9. doi: 10.1177/1043454212439472
142. Tzuh Tang S, Li CY. The important role of sense of coherence in relation to depressive symptoms for Taiwanese family caregivers of cancer patients at the end of life. J Psychosom Res (2008) 64(2):195–203. doi: 10.1016/j.jpsychores.2007.08.013
143. Vartak J. The role of hope and social support on resilience in cancer patients. Indian J Ment Health (2015) 2(1):35–42. doi: 10.30877/IJMH.2.1.2015.35-42
144. Wallston BS, Alagna SW, DeVellis BM, DeVellis RF. Social support and physical health. Health Psychol (1983) 2(4):367–91. doi: 10.1037/0278-6133.2.4.367
145. Walsh DMJ, Morrison TG, Conway RJ, Rogers E, Sullivan FJ, Groarke A. A model to predict psychological- and health-related adjustment in men with prostate cancer: the role of post traumatic growth, physical post traumatic growth, resilience and mindfulness. Front Psychol (2018) 9:136. doi: 10.3389/fpsyg.2018.00136
146. Weiss T. Correlates of posttraumatic growth in husbands of breast cancer survivors. Psychooncology (2004) 13(4):260–8. doi: 10.1002/pon.735
147. Wenzel LB, Donnelly JP, Fowler JM, Habbal R, Taylor TH, Aziz N, et al. Resilience, reflection, and residual stress in ovarian cancer survivorship: a gynecologic oncology group study. Psychooncology (2002) 11(2):142–53. doi: 10.1002/pon.567
148. Westphal M, Bonanno GA. Posttraumatic growth and resilience to trauma: different sides of the same coin or different coins? Appl Psychol (2007) 56(3):417–27. doi: 10.1111/j.1464-0597.2007.00298.x
149. Wortman CB, Silver RC. The myths of coping with loss revisited. In: Handbook of bereavement research: consequences, coping, and care. Washington, DC: American Psychological Association (2001). p. 405–29. doi: 10.1037/10436-017
150. Ye ZJ, Qiu HZ, Li PF, Liang MZ, Zhu YF, Zeng Z, et al. Predicting changes in quality of life and emotional distress in Chinese patients with lung, gastric, and colon-rectal cancer diagnoses: the role of psychological resilience. Psychooncology (2017) 26(6):829–35. doi: 10.1002/pon.4237
151. Yesilot SB, BOztunc G, Demirci PY, Manav AI, Paydas S. The evaluation of hopelessness and perceived social support level in patients with lung cancer. Int J Health Life Sci (2017) 3(2):88–105. doi: 10.20319/lijhls.2017.32.88105
152. Zoellner T, Maercker A. Posttraumatic growth in clinical psychology—a critical review and introduction of a two component model. Clin Psychol Rev (2006) 26(5):626–53. doi: 10.1016/j.cpr.2006.01.008
153. Zou G, Li Y, Xu R, Li P. Resilience and positive affect contribute to lower cancer-related fatigue among Chinese patients with gastric cancer. J Clin Nurs (2018) 27(7–8):e1412–e8. doi: 10.1111/jocn.14245
154. Zwahlen D, Hagenbuch N, Carley MI, Jenewein J, Buchi S. Posttraumatic growth in cancer patients and partners—effects of role, gender and the dyad on couples’ posttraumatic growth experience. Psychooncology (2010) 19(1):12–20. doi: 10.1002/pon.1486
Keywords: cancer, resilience, coping, social support, distress, posttraumatic growth
Citation: Seiler A and Jenewein J (2019) Resilience in Cancer Patients. Front. Psychiatry 10:208. doi: 10.3389/fpsyt.2019.00208
Received: 20 June 2018; Accepted: 22 March 2019;
Published: 05 April 2019.
Edited by:
Chantal Martin Soelch, Université de Fribourg, SwitzerlandReviewed by:
Jutta Lindert, University of Applied Sciences Emden Leer, GermanyNatasa Jokic-Begic, University of Zagreb, Croatia
Copyright © 2019 Seiler and Jenewein. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Annina Seiler, annina.seiler@usz.ch