 Jessica Schoch-Ruppen1,2
Jessica Schoch-Ruppen1,2 Ulrike Ehlert1,2
Ulrike Ehlert1,2 Franziska Uggowitzer1,3Nadine Weymerskirch1
Franziska Uggowitzer1,3Nadine Weymerskirch1 Pearl La Marca-Ghaemmaghami1*
Pearl La Marca-Ghaemmaghami1*- 1Department of Clinical Psychology and Psychotherapy, University of Zurich, Zurich, Switzerland
- 2University Research Priority Program – Dynamics of Healthy Aging, University of Zurich, Zurich, Switzerland
- 3School of Social Work, Institute for Integration and Participation, University of Applied Sciences and Arts Northwestern Switzerland, Olten, Switzerland
Background: Experiencing high levels of stress during pregnancy can impair maternal well-being and fetal development. Consequently, unbiased assessment of maternal psychological state is crucial. Self-report measures are vulnerable to social desirability effects. Thus, implicit measures, such as word choice analysis, may offer an alternative.
Methods: In this longitudinal online-study, 427 pregnant women described their emotional experiences in writing and additionally responded to self-report questionnaires assessing symptoms of prenatal stress and depression. The written texts were analyzed with a computerized text analysis program. After birth, 253 women provided information on birth outcome.
Results: Word use differed significantly depending on maternal socioeconomic (e.g., marital status) and pregnancy-related characteristics (e.g., parity). Prenatal stress and depressive symptoms were associated with more frequent use of negative emotion words and words of anxiety, as well as with less first-person plural, but not singular pronoun use. Negative emotion and cognitive mechanism words predicted birth outcome, while self-report measures did not.
Conclusion: In addition to self-report measures, word choice may serve as a useful screening tool for symptoms of depression and stress in pregnant women. The findings on pronoun use may reflect women’s changing experience of self-identity during the transition to motherhood.
Introduction
Pregnancy and the transition to motherhood is characterized by physiological, psychological, and social changes (Hobbs and Cole, 1976; Yali and Lobel, 1999). The attempt to adapt to these multifaceted changes may result in prenatal stress (La Marca-Ghaemmaghami and Ehlert, 2015). In fact, a majority of women report experiencing psychosocial stress during pregnancy(Woods et al., 2010). Some women may go on to develop negative affect states such as anxiety or depressive symptoms. Prevalence rates for mental health problems during pregnancy vary between studies. Prenatal depressive symptoms are present in approximately 16–37% of all pregnant women and about 5–12% fulfill the criteria for major depression (Lee et al., 2007; Melville et al., 2010; Fall et al., 2013; Lara et al., 2015). Feelings of anxiety seem to occur even more frequently ranging from 14 to 54% (Heron et al., 2004; Lee et al., 2007; Rubertsson et al., 2014). The prevalence rate for anxiety disorders during pregnancy is 13% (Vesga-López et al., 2008). If not adequately treated, prenatal psychological problems may persist throughout pregnancy and into the postpartum period (Grant et al., 2008).
Prenatal stress may not only decrease pregnant women’s well-being, but also can negatively affect fetal development and neonatal birth outcome. For instance, maternal depressive symptoms have been found to be associated with lower neonatal birth weight (Goedhart et al., 2010; Dunkel Schetter and Lobel, 2012) and preterm delivery (i.e., birth before 37 completed week’s gestation) (Grote et al., 2010). Pregnancy anxiety is a specific form of anxiety, which reflects a pregnant woman’s extensive worries about the well-being of her unborn child and fears associated with prenatal medical care, birth, and motherhood. This type of anxiety shows strong links to shorter gestational length (Roesch et al., 2004; Dunkel Schetter and Glynn, 2011) and was found to be a risk factor for preterm birth (Dole et al., 2003; Mancuso et al., 2004; Kramer et al., 2009). However, contradictory findings on the effect of psychological symptoms on birth outcome have been reported as well. For instance, two large population-based studies found no associations between mental health symptoms and neonatal birth outcome (Andersson et al., 2004; Bödecs et al., 2010). Grote et al. (2010) argue that these divergences are likely due to methodological issues such as choice of assessment method or confounding factors. Most studies investigating the consequences of prenatal stress rely on self-report measures by pregnant women as indicators of their mental health status (Lobel, 1994). Yet, self-report questionnaires can elicit socially desirable response behavior, particularly with regard to sensitive topics (King and Bruner, 2000). Consequently, results may be biased with respect to accuracy and completeness of answers (Deshields et al., 1995; Taylor et al., 2006). Thus, self-report measures tend to impair research validity and are often considered a research limitation (Fisher, 1993; Skouteris et al., 2009). Pregnant women oftentimes mention fear of judgment and other negative consequences as barriers to fully disclose their mental health issues to their health care provider (Byatt et al., 2013; Kingston et al., 2015). If pregnant women’s subjective experiences differ substantially from society’s mainly positive view of pregnancy or their own self-image, they might experience feelings of guilt and shame. They could then withhold their problems, and present an image of themselves and of their pregnancy that is more consistent with their own as well as societal expectations (Johnson and Fendrich, 2005). This is in line with findings showing that most psychological difficulties experienced by pregnant women remain unspoken and therefore, untreated (Hatton et al., 2007; Vesga-López et al., 2008; World Health Organization the United Nations Population Fund [WHO], 2008). However, early detection and treatment of mental health problems and stress overexposure are essential to ensure pregnant women’s well-being as well as the healthy development of the child in utero.
In order to bypass social desirability or self-presentation biases when assessing sensitive topics, researchers in other fields of psychology and social sciences have turned to implicit measures (Pressman and Cohen, 2007; Hussy et al., 2010; Brönnimann et al., 2013). Particularly, analyzing word use is a promising way to gain insight into psychosocial processes while avoiding response bias in self-reports (Mehl and Pennebaker, 2003; Pennebaker, 2011). The majority of our language is made up of content words such as nouns and verbs which we use to communicate what we think (Chung and Pennebaker, 2011). Function words, such as pronouns, form the second group of linguistic characteristics. Even though they only make up about 1% of our natural language, they are closely related to psychosocial processes and describe how we think about ourselves and our surroundings (Miller, 1995; Tausczik and Pennebaker, 2010). Accordingly, studies have found individual differences in word use depending on age (Pennebaker and Stone, 2003), gender (Mehl and Pennebaker, 2003), or personality (Hirsh and Peterson, 2009). Moreover, word choice is correlated with an individual’s mental health status (Rude et al., 2004). Studies have consistently confirmed depressive patients’ increased use of first-person singular pronouns reflecting a stronger self-focus compared to non-depressed individuals (Weintraub, 1981; Rude et al., 2004). Depression is further characterized by a more frequent use of negative emotion words (Rude et al., 2004; Ramirez-Esparza et al., 2008). Similarly, the experience of acute stress is reflected in higher use of negative emotion words (Liehr et al., 2004). Unlike the greater self-focus in depression, acute stress results in increased collective orientation, marked by a higher use of first-person plural pronouns (Stone and Pennebaker, 2002; Liehr et al., 2004). Apart from reflecting mental health status, word use has also been found to be a predictor for psychotherapy outcome. Lower post-therapy depressive symptoms were related to a decrease in first-person singular pronouns and an increase in positive emotion words during therapy (Pulverman et al., 2015). Studies have provided further evidence for the predictive value of word choice for physical health outcomes. For example, negative emotion words were identified as risk factors for heart disease mortality whilst positive emotion words were found to be protective (Eichstaedt et al., 2015).
Analysis of word use in pregnant women could provide a unique perspective into their emotional experience of pregnancy. Surprisingly, only one study to date has investigated the association between linguistic characteristics and pregnancy in the broader sense: In this retrospective study, parents completed an online questionnaire after the birth of their child and were asked to write about their experience of trying to conceive (Sweeny et al., 2015). The parents’ use of negative emotion words was positively associated with the level of self-reported anxiety during that period. Parents using more first-person plural pronouns reported less anxiety and rumination, while first-person singular pronouns were positively associated with rumination. Moreover, mentioning words targeted at cognitive processes (e.g., because, think) were negatively correlated with both anxiety and rumination (Sweeny et al., 2015). Having previously experienced a miscarriage was significantly related to a more frequent use of negative emotions including anxiety and sad words, but in women only (Nelson et al., 2015). Despite these interesting findings, it has to be kept in mind that the study used a retrospective design which could yield memory bias in parents’ recollections (Sweeny et al., 2015). Furthermore, participants described the time during which they were trying to conceive and not their emotional experiences associated with the pregnancy itself. Ensuring mother’s well-being in pregnancy is important for herself and her child. However, both researchers and health care providers face barriers in the assessment of potential psychological problems and stress overload. Therefore, research on linguistic characteristics in pregnancy is required.
Present Research
The present study was guided by three main research questions. Since word choice has been found to differ between sociodemographic groups or in terms of health conditions (Mehl and Pennebaker, 2003; Lorenz and Meston, 2012), we first investigated associations between pregnant women’s word use and maternal socioeconomic (e.g., educational qualification) and pregnancy-related characteristics (e.g., gestational age). We expected factors such as parity (nulliparous vs. primiparous/multiparous), gestational age, or the experience of complications during pregnancy to influence a woman’s state of mind and therefore, also her choice of words. In self-report studies, nulliparous women, for example, indicated higher fear of childbirth compared to women who already have given birth to a child (Rouhe et al., 2009). Also, pregnant women’s perception of stress seems to decrease with advancing gestation (Glynn et al., 2004). Analyses for this first research question were mainly exploratory in nature since there are hardly any studies on associations between word use and maternal socioeconomic and pregnancy-related characteristics to base our hypotheses on.
Second, this study set out to replicate findings on the relationship between self-reported psychological well-being and word use obtained from other study populations in a sample of pregnant women. We hypothesized prenatal depressive symptoms to be positively associated with the use of first-person singular pronouns and negative emotion words (Rude et al., 2004). We formulated a second analogous hypothesis for prenatal stress, i.e., prenatal stress is related to higher use of first-person singular pronouns and negative emotion words.
Third, we explored the relationship between word use and neonatal birth outcome above and beyond common control variables and self-report measures of the experience of stress and depressive symptoms. Following results from other studies, we expected greater self-focus and negative emotionality – as indicators of stress and depressive symptomatology and therefore, decreased psychological well-being – to be related to poorer birth outcome (i.e., a shorter duration of gestation, and lower neonatal birth weight and size) (Dunkel Schetter and Glynn, 2011; Dunkel Schetter and Lobel, 2012). Deriving from studies on expressive writing, we predicted a positive association between a more frequent use of words that reflect cognitive processing (e.g., think, know) on birth outcome (Pennebaker et al., 1997).
Materials and Methods
Participants and Procedure
The present data stemmed from a larger online research study on the psychological well-being of pregnant women, which was conducted between April 2012 and October 2013. The study was divided into two parts and addressed pregnant women from German-speaking countries of Central Europe (Switzerland, Germany, Austria, the Principality of Liechtenstein, and Luxembourg). Participants were recruited by placing online advertisement (e.g., in pregnancy forums) as well as displaying flyers in gynecologists’ practices and shops selling baby products. The participants were informed about the study’s objectives and their right to withdraw their participation at any time, without any consequences. The women provided informed consent prior to responding to the online questionnaire. The study was conducted in adherence to the regulations of the Ethics Committee of the Faculty of Arts and Sciences of the University of Zurich. The first online assessment (T1) included information on sociodemographic characteristics (e.g., age, marital status) and pregnancy (e.g., whether the pregnancy was planned or not) as well as several psychometric questionnaires related to the women’s psychological well-being (e.g., the experience of prenatal stress and presence of depressive symptoms). Pregnancy-related variables were assessed by single questions, e.g., “Have you experienced any complications in the present pregnancy?” with two response options (yes/no). Category options for sociodemographic variables in the questionnaire are shown in Table 1. At the same time, the women were asked to describe their experiences of pregnancy in writing. Upon agreement, we invited the women to a second online assessment approximately 1 month after the expected delivery date (T2) during which they provided information on birth outcome (e.g., gestational length, neonatal weight, and size at birth). From the original sample of 725 pregnant women, we excluded the texts of 294 women, as they used fewer than 40 words. This minimum of 40 words was required to increase the reliability of the results1. Another 4 women were excluded due to multifetal pregnancy which could influence their children’s birth outcome (e.g., with regard to gestational length and birth weight). Even though it would be important to investigate these women’s experiences in pregnancy, the small number of cases did not allow us to test corresponding hypotheses and conduct statistical analyses. This resulted in a sample size of N = 427 for T1, of which n = 253 women responded to T2 as well.
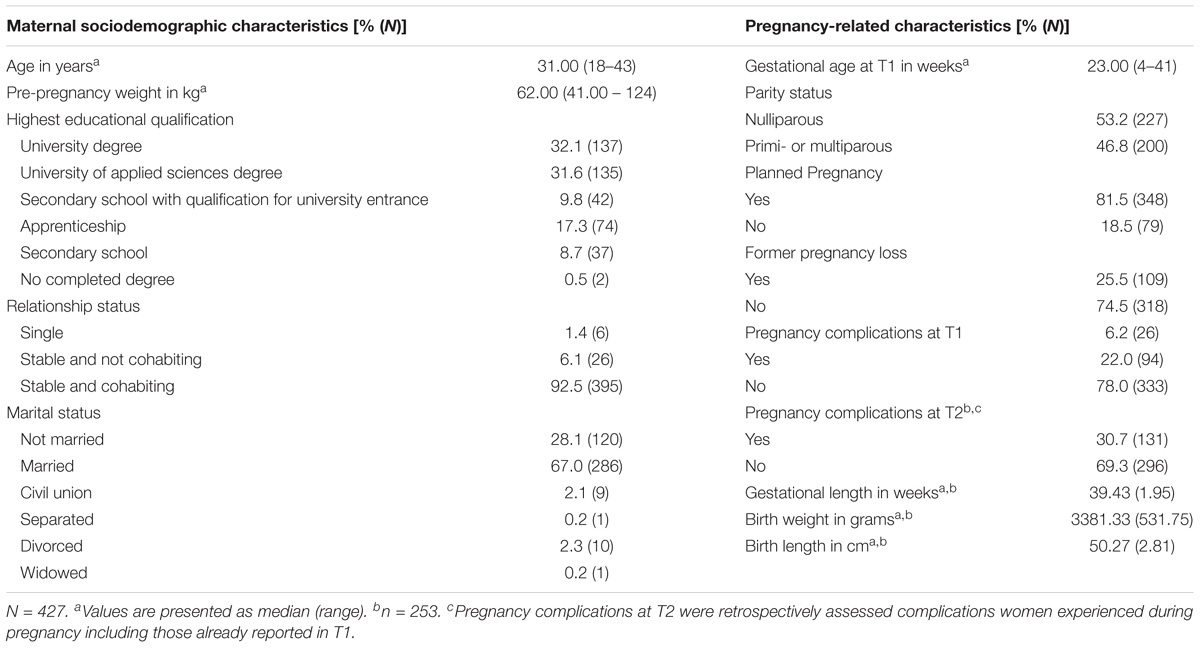
TABLE 1. Descriptive statistics of sample.
Measures
The Psychological Experience of Stress During Pregnancy
Pregnancy-specific stress was assessed with the German version of the Prenatal Distress Questionnaire (Yali and Lobel, 1999; Pluess et al., 2010). The scale consists of 12 items, which measure the concerns and worries of women regarding pregnancy and birth, e.g., “I am worried about eating healthy foods and a balanced diet for the infant.” Items are rated on a five-point Likert scale from 1 (not at all worried) to 5 (extremely worried). A Cronbach’s alpha of 0.808 for the present study indicates a good internal consistency of the measure.
Symptoms of Depression
The German version of the Edinburgh Postnatal Depression Scale (EPDS) was used to measure depressive symptoms (Cox et al., 1987; Bergant et al., 1998). This is a well-validated self-report questionnaire, often used to evaluate women’s psychological state during pregnancy and the postpartum period (Nast et al., 2013). The women responded to ten items assessing how they felt in the past week using a scale from 1 (most of the time) to 4 (not at all), e.g., “I have felt sad or miserable”. In this study, the scale’s internal consistency was good (α = 0.851).
Word Use
Following recommendations by other authors (Pennebaker, 1989; Horn and Mehl, 2004), participants were presented with the following instructions: “For this study, could you please take some time (about 5 min) to describe your feelings and thoughts regarding this pregnancy? You do not need to worry about spelling, sentence structure, or grammar.” The resulting texts were analyzed with the Linguistic Inquiry and Word Count (LIWC; Pennebaker et al., 2007). LIWC is a software that uses a word count approach to analyze a written text. The software has an internal dictionary which consists of more than 4500 words and word stems that are presorted into linguistic and psychological categories (Pennebaker et al., 2007). LIWC calculates the frequency of words from the written sample that fall into a given category by comparing each word against its internal dictionary. We applied the German LIWC dictionary which was shown to have equivalently good psychometric properties compared to the original English version (Wolf et al., 2008). Before data analysis, we corrected the texts for spelling errors. On average, women wrote 91.08 words (SD = 55.33). Almost 78% (SD = 5.43) of all words were recognized by the LIWC dictionary.
Quantity of word categories were computed as the percentage of words in the specific categories related to the total length of the text. Multiple linguistic categories were used for the current study: first-person singular (e.g., I, me) (M = 8.97%, SD = 4.64) and first-person plural pronouns (e.g., we, us) (M = 1.29%, SD = 2.24), positive emotion words (e.g., love, nice) (M = 4.84%, SD = 2.61), negative emotion words (e.g., hate, hurt) (M = 3.25%, SD = 2.54) including anxiety (e.g., nervous, tense) (M = 1.60%, SD = 1.71), and sad words (e.g., cry, grief) (M = 0.50%, SD = 0.92). Additionally, we were interested in the word category cognitive mechanisms (e.g., think, understand) (M = 12.04%, SD = 3.97), including words of cause (e.g., because, effect), (M = 2.09%, SD = 1.78), discrepancy (e.g., should, would) (M = 2.05%, SD = 1.72), insight (e.g., consider, know) (M = 2.75%, SD = 2.00), inhibition (e.g., constrain, stop) (M = 0.35%, SD = 0.73), and certainty (e.g., absolutely, sure, always, never) (M = 3.37%, SD = 2.18).
Birth Outcome Measures
The women responded to questions regarding birth outcome (i.e., gestational length, weight and size of the neonate) at T2 and were subsequently asked about the source of this information. Most women (82.2%, n = 208) reported that they had obtained the information from medical records and birth certificates. A further 7.91% (n = 20 women) described that they had received the information orally from their obstetrician, pediatrician, and/or midwife, 5.93% (n = 15) indicated that they remembered it (e.g., “I know it by heart”), and 3.95% (n = 10) did not indicate the source of information. Validation studies show excellent agreement between maternal reports in the months after delivery and medical records regarding gestational age at delivery, neonatal birth weight and size (Troude et al., 2008; Bat-Erdene et al., 2013).
Statistical Analyses
Statistical analyses were performed using the IBM Statistical Package for the Social Sciences (SPSS Version 22 for Windows). Since several linguistic categories were positively skewed, we applied log transformation using the formula ln (score + 1) (Field, 2013; Schultheiss, 2013). Visual inspections and Kolmogorov–Smirnov tests showed that most variables were still not normally distributed, even though the skewness of the data could be improved. Therefore, we further used non-parametric tests for all analyses, e.g., Spearman correlations (Delucchi and Bostrom, 2004). For education, a dichotomized variable was created with women with a University degree classified as 1 for highest educational qualification. Relationship status was dichotomized by assigning the value 1 for all women in a relationship (cohabiting or not). For marital status, two categories were computed with 1 indicating being married at the moment.
Prior to investigating the research questions, we examined potential differences in sociodemographic, and pregnancy-related variables, as well as psychological measure (i.e., experience of stress and depressive symptoms) between women participating at T1 and those participating at both T1 and T2 using Mann–Whitney U tests. Pregnant women who participated at both T1 and T2 were later in gestation (Mdn = 25.00) compared to women who did not provide data at T2 (Mdn = 21.50; U = 17633.50, p < 0.001) and experienced less prenatal stress (Mdn = 6.00) and depressive symptoms (Mdn = 12) compared to those who did not respond to T2 (Mdn for prenatal stress = 7.00; U = 17326.50, p = 0.003; Mdn for depressive symptoms = 14.00; U = 16583.00, p = 0.016).
For the first research question, potential associations between maternal sociodemographic and pregnancy-related characteristics and word choice were explored with Spearman correlations. Group differences in word choice were analyzed with Mann–Whitney U tests (i.e., group differences in word choice regarding maternal educational qualification, marital status, (un-)planned pregnancy, (nulli-)parity, prior pregnancy loss, and current pregnancy complications). Effect sizes were calculated according to the formula r = z / √N and interpreted as small (r = 0.1), medium (r = 0.3), or large (r = 0.5) (Cohen, 1990; Rosenthal, 1991).
With regard to the second research question, the relationship between word choice and maternal psychological state was investigated with partial Spearman correlations. To determine relevant control variables prior to the main statistical analyses, point-biserial correlations between maternal psychological state (i.e., the experience of stress and depressive symptoms during pregnancy) and the following variables were computed: maternal age, education, marital status, relationship status, parity, unplanned pregnancy, pregnancy complications at T1, and gestational week at T1. For prenatal stress, the following variables were significant and therefore, controlled for: maternal age (rs = −0.272, p < 0.001), education (rs = −0.105, p = 0.035), marital status (rs = −0.142, p = 0.004), relationship status (rs = −0.137, p = 0.006), parity (rs = 0.147, p = 0.003), unplanned pregnancy (rs = 0.124, p = 0.13), and gestational week at T1 (rs = −0.200, p < 0.001). With regard to depressive symptoms, maternal age (rs = −0.153, p = 0.002), marital status (rs = −0.120, p = 0.016), unplanned pregnancy (rs = 0.229, p < 0.001), relationship status (rs = −0.177, p < 0.001), and pregnancy complications at T1 (rs = 0.203, p < 0.001) were significant and added as control variables in the relevant analyses.
For the final research question, we ran block-wise multiple regressions to determine the influence of prenatal stress, depressive symptoms, and word choice on birth outcome. In the first block, we entered control variables from sociodemographic and pregnancy-related domains. Again, control variables were determined beforehand with correlation analyses. In addition to the variables described in the previous paragraph, pregnancy complications at T2, maternal pre-pregnancy weight, the newborn’s gender, and gestational length were tested for their potential influence on birth outcome. For gestational length, only gestational age at T1 was significant and chosen as a control variable. For neonatal birth weight and size, gestational length, maternal pre-pregnancy weight, and newborn’s gender were significantly correlated and entered into the respective models as control variables. The second block was composed of self-reported psychometric measures, namely prenatal stress and depressive symptoms. In a third step, word choice was entered into the analyses. Word categories included first-person singular and plural pronouns, positive emotions, negative emotions (including words of anxiety and sadness), and cognitive mechanisms (including words of certainty, insight, discrepancy, and inhibition). A step-wise selection method was applied to the second and third block so that at each step only the variable with the largest significant contribution was entered into the model (Field, 2013). For the results presented here, non-significant variables were dropped and a final block-wise regression was run in which all significant predictors established in the first regression were entered simultaneously.
Statistical significance was defined as p < 0.05, and all analyses were two-tailed.
Results
Sample Characteristics
The descriptive statistics of the study sample are presented in Table 1.
Is Word Choice Associated With Maternal Sociodemographic and Pregnancy-Related Characteristics?
Concerning maternal sociodemographic characteristics, Spearman correlations indicated that maternal age was associated with fewer anxiety words (rs = −0.120, p = 0.013). Women who had attained a higher educational qualification (n = 137) wrote fewer first-person plural pronouns (U = 17447.50, p = 0.022, r = 0.11), but more words of inhibition (U = 17831.50, p = 0.026, r = 0.11) in their texts than women with a lower educational qualification (n = 290). Pregnant women who were not in a stable relationship (n = 6) used less anxiety words compared to women with a partner (U = 656.50, p = 0.040, r = 0.10; n = 421). Married women (n = 286) compared to non-married women (n = 141) used more words indicating certainty (U = 17579.50, p = 0.031, r = 0.10).
With regard to pregnancy-related characteristics, gestational age was negatively correlated with the use of first-person singular pronouns (rs = −0.123, p = 0.011) and words of insight (rs = −0.119, p = 0.014). Then, the frequency of negative emotion and sad words was significantly higher in nulliparous women (n = 227) compared to women who had given birth before (U = 20014.50, p = 0.035, r = 0.10 and U = 19942.50, p = 0.008, r = 0.13; n = 200). Women used significantly fewer words of certainty, if the pregnancy was unplanned (U = 11502.50, p = 0.023, r = 0.11; planned pregnancy: n = 348; unplanned pregnancy: n = 79). The use of anxiety words was elevated in women who had experienced at least one pregnancy loss in the past (U = 15151.50, p = 0.047, r = 0.10; n = 109), while their use of first-person plural pronouns was decreased compared to women who had never had a pregnancy loss before (U = 14793.50, p = 0.010, r = 0.13; n = 318). Women experiencing complications in the present pregnancy (n = 94) used significantly less first-person singular pronouns (U = 13092.00, p = 0.015, r = 0.12), more negative emotion words (U = 13539.00, p = 0.045, r = 0.21), and fewer words of certainty (U = 12886.50, p = 0.009, r = 0.13) compared to women who did not experiency any pregnancy complications (n = 333).
Does Word Use Reflect Pregnant Women’s Self-Reported Psychological State?
Findings on the analyses of the relationship between maternal psychological symptoms as measured by self-report questionnaires and word choice are reported in Table 2.

TABLE 2. Partial Spearman correlation coefficients for the associations between maternal psychological state and word choice.
Is Maternal Word Use During Pregnancy Associated With Neonatal Birth Outcome?
The association between maternal psychological state, word choice and birth outcome was analyzed separately for gestational length, neonatal birth weight, and birth size. Prenatal stress and depressive symptoms assessed using self-report questionnaires did not show any relationship with pregnancy duration and were therefore dropped from the final analysis. For gestational length, including word choice resulted in a significant increase in ΔR2 = 0.04, F(3,249) = 6.66, p < 0.001. First-person plural pronoun use (β = −0.18, p = 0.005) as well as negative emotion words (β = −0.14, p = 0.024) predicted gestational length (see Table 3). Hence, women using more first-person plural pronouns (e.g., we) and negative emotion words (e.g., hurt) delivered their babies earlier. In total, the predictors could explain 6% of variance in gestational length.
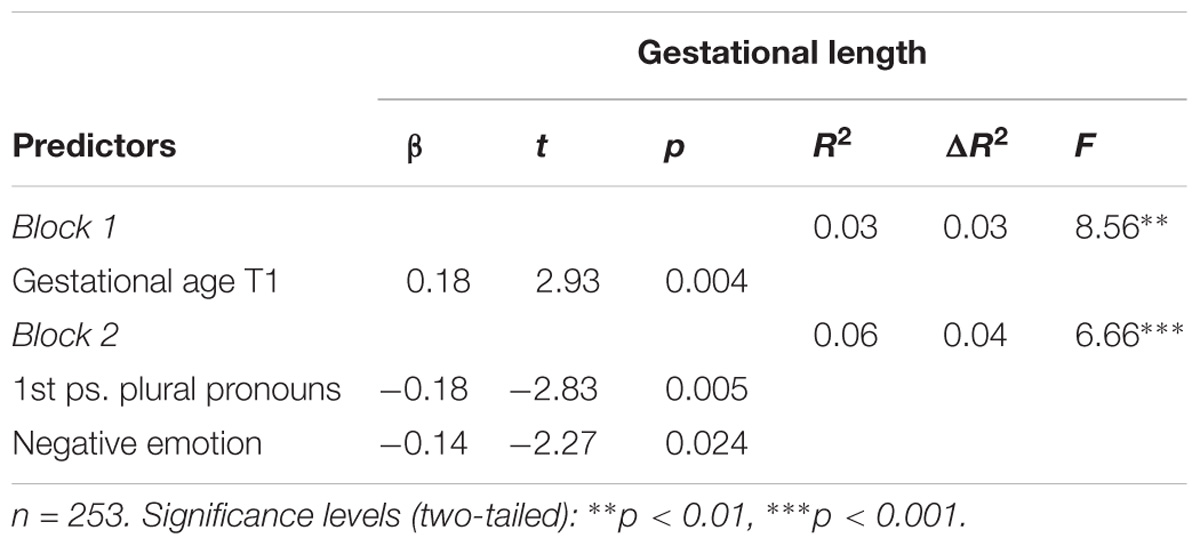
TABLE 3. Block-wise regression analysis for gestational length.
Results of the regression analysis for birth weight are presented in Table 4. Self-reported measures of maternal psychological state did not predict birth weight. Entering word choice in the second block led to a significant increase in ΔR2 = 0.01, F(5,245) = 40.88, p < 0.001. Using more first-person plural pronouns predicted lower birth weight (β = −0.11, p = 0.035). The final model was able to explain 39% of variance in birth weight.
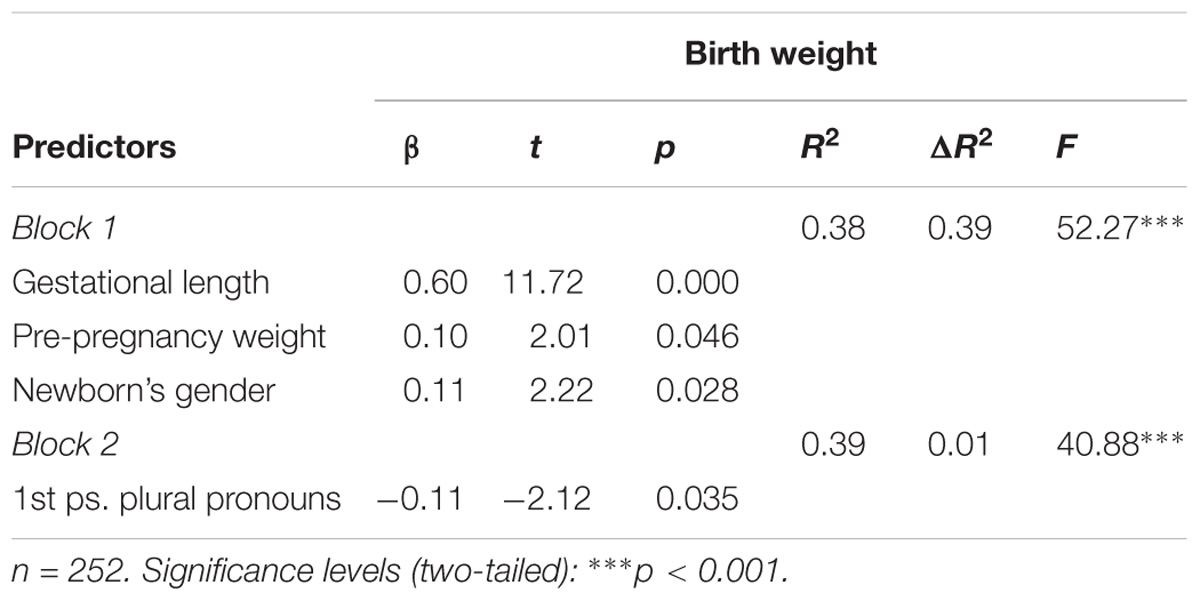
TABLE 4. Block-wise regression analysis for neonatal birth weight.
Neonatal size at birth was not predicted by depressive symptoms and prenatal stress, as assessed by self-report. Adding word choice explained significantly more variance, ΔR2 = 0.01, F(4,243) = 36.04, p < 0.001. Cognitive mechanisms predicted larger birth size (β = 0.12, p = 0.024). Overall, the predictors explained 36% of variance in birth size. Results are shown in Table 5.
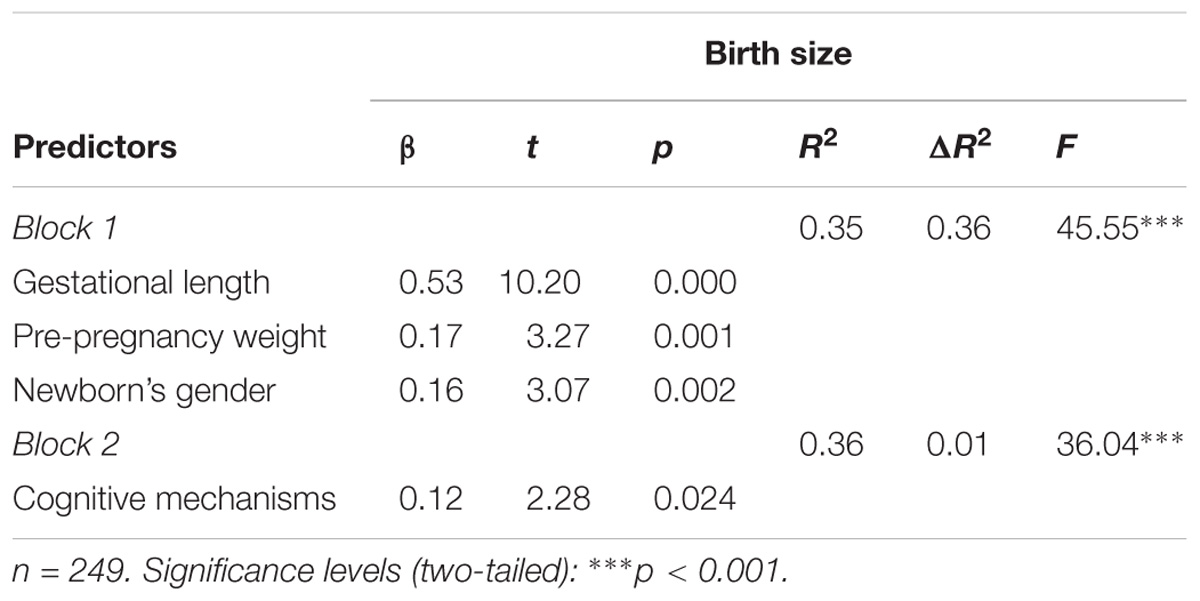
TABLE 5. Block-wise regression analysis for neonatal birth size.
Discussion
Summary and Discussion of Results
The goal of this study was to explore pregnant women’s word choice, its association with maternal socioeconomic and pregnancy-related characteristics, self-report measures of prenatal stress and depressive symptoms, and its predictive value for pregnancy duration and neonatal birth outcome. Analyses for the first research question yielded that married women used words of certainty more frequently than unmarried women, while single women wrote fewer anxiety words compared to women in a stable relationship. Higher maternal age was associated with fewer anxiety words as well. Word choice also differed depending on pregnancy-related factors, such as nulliparity, former pregnancy loss, or the experience of pregnancy complications. In these cases, women’s texts contained more negative emotion or anxiety words, respectively. Frequency of certainty words was decreased in women with an unplanned pregnancy and in those experiencing pregnancy complications. In the latter, the use of first-person singular pronouns was reduced as well, while women who had experienced a former pregnancy loss used less first-person plural pronouns. If pregnancy was more advanced, pregnant women mentioned fewer first person singular pronouns and words of insight.
For the second research question, we analyzed the relationship between maternal psychological state and word choice. Women reporting increased prenatal stress used more negative emotion words and anxiety words. Similarly, women reporting higher depressive symptoms used fewer positive emotion words, more negative emotion words, including words of anxiety and sadness. In line with the literature, we had expected depressive symptoms in pregnant women to be associated with increased use of first-person singular pronouns. This, however, was not the case. Instead, higher depressive symptomatology and likewise increased prenatal stress were associated with fewer first-person plural pronouns.
Finally, when investigating the association between word use and birth outcome, we found women’s more frequent use of negative emotion words, but surprisingly also more frequent use of first-person plural pronouns to predict shorter gestational length. Likewise, lower neonatal birth weight was predicted by writing more words such as we or our. Increased birth size, though, was associated with pregnant women’s more frequent use of words relating to cognitive mechanisms.
To date, hardly any study has investigated word use in pregnant women. Thus, the present findings contribute to our advancement of understanding maternal psychological processes during pregnancy and their impact on fetal development. In the following, we will discuss the results based on the literature on lexical choice in other non-pregnant study samples.
The first research question addressed associations between linguistic and maternal sociodemographic as well as pregnancy-related characteristics. Our finding of a higher usage of certainty words in married compared to unmarried women corresponds to results indicating higher pregnancy wantedness in married compared to cohabitating and single women (Santelli et al., 2003; Maxson and Miranda, 2011) and a higher prevalence of a planned pregnancy in married compared to non-cohabitating pregnant women (Wellings et al., 2013). Then, we found higher maternal age to be associated with fewer anxiety words. This is in line with a study by McMahon et al. (2011), in which older pregnant women (>37 years) reported lower symptoms of anxiety and depression and seemed to be more resilient than their younger counterparts. However, this advantage of advanced maternal age may be annuled in older pregnant women who conceive via assisted reproductive technology (McMahon et al., 2011). Surprisingly, in our sample, single pregnant women used fewer anxiety words than the women in a stable relationship. This result should, however, be considered with caution due to the small sample size (n = 6) in the group of single pregnant women. Few studies have systematically compared the effect of singlehood, cohabitation, and marriage on maternal psychological wellbeing in pregnancy – even less so with regard to word use. Maternal singlehood in pregnancy has been linked with an increased risk for the experience of postpartum depressive symptoms (Lara et al., 2016). Moreover, the prevalence of mental health problems seems to be increased in single mothers compared to mothers who have a partner (Crosier et al., 2007). This difference was explained by higher financial problems and decreased social support in single mothers.
With regard to pregnancy-related characteristics, the positive associations between negative emotion words and negative experiences such as pregnancy complications were to be expected, since negative experiences or states (e.g., psychiatric disorders) tend to be reflected in a more negative word use in non-pregnant participants (Rude et al., 2004; Orsillo et al., 2004; Minor et al., 2015). Furthermore, similar to marital status, women facing greater insecurity in pregnancy, such as when they had not planned their current pregnancy, or when they were confronted with obstetrical risks, expressed these concerns in their written texts by using less words indicating certainty such as absolutely, sure, always, or never. Similarly, in a study with breast-cancer patients, higher use of linguistic uncertainty was related to lower well-being and greater depression (Cordova et al., 2001).
The results for first-person singular and plural pronouns are somewhat contradictory to the literature. A more frequent use of first-person singular pronouns (e.g., I, me) has been associated with impaired mental health, such as increased depressive symptoms (Stirman and Pennebaker, 2001; Rude et al., 2004). Accordingly, one would assume that the experience of obstetric complications, which are known to increase the risk of depressive symptoms (Brandon et al., 2008; Byatt et al., 2013), is linked with a more frequent use of first-person singular pronouns. However, in our study, women with pregnancy complications wrote less first-person singular pronouns compared to women without obstetric complications. This might possibly indicate that when women worried about the health of their unborn child, their focus shifted away from themselves. A lower usage of first-person singular pronouns, however, was associated with a more advanced pregnancy, indicating a decrease in self-focus with impending birth.
Plural pronouns, under certain circumstances, appear to be a marker of shared identity, closeness, and affiliative motivation (Slatcher, 2009; Chung and Pennebaker, 2011). After the terror attack on the World Trade Center Towers on September 11th 2001, researchers noted increases in plural pronoun use suggesting increased collective orientation in this time of stress (Mehl and Pennebaker, 2003; Liehr et al., 2004). Some researchers suggest that referring to ourselves as a dyad or group has adaptive psychological consequences (Kelley and Thibaut, 1978; Zimmermann et al., 2013). Therefore, acute stress seems to increase social connectedness and the use of plural pronouns. In the long term, this collective orientation may improve mental health and well-being. Accordingly, Frost (2013) found participants using more first-person plural pronouns to report fewer depressive symptoms and higher psychological well-being. Similarly, in the texts of parents who retrospectively described their thoughts and feelings about the time when they were trying to conceive, more first-person plural pronouns were associated with less anxiety and rumination (Sweeny et al., 2015). In the present study though, women who had experienced a former pregnancy loss, wrote fewer first-person plural pronouns. This could indicate a lack of social connectedness. Several qualitative interview studies show that women experiencing a miscarriage tend to suffer in silence and feel disconnected (Adolfsson et al., 2004; MacWilliams et al., 2016). Furthermore, they may regard their pregnancy loss as a personal failure accompanied by feelings of their own guilt (Wong et al., 2003; Adolfsson et al., 2004). It could also be argued that women who have had to deal with a pregnancy loss in their past are emotionally distancing themselves from their unborn child due to fears of another pregnancy loss (Adolfsson et al., 2012). However, studies on the impairment of prenatal attachment in subsequent pregnancies after a pregnancy loss provided mixed results (Tsartsara and Johnson, 2006; Alhusen, 2008). In sum, pregnant women differ from other samples in regard to their use of singular and plural pronouns. Future research is needed to understand the mechanisms of these associations more clearly.
For the second research question on word use and maternal psychological state, we expected to replicate consistent findings from previous research in our sample of pregnant women. However, our hypotheses were only partially supported. We found worse self-reported maternal psychological state, that is higher prenatal stress and depressive symptoms, to be reflected in a higher frequency of negative emotion words including words of anxiety and sadness. This is similar to other studies, in which negative emotion words were positively related to depression or the experience of sexual abuse (Ramirez-Esparza et al., 2008; Lorenz and Meston, 2012). Yet unexpectedly, we did not find the negative relationship between maternal psychological state and first-person singular pronouns (Stirman and Pennebaker, 2001; Rude et al., 2004). In the present study, instead, women experiencing increased prenatal stress and depressive symptoms used first-person plural pronouns less frequently. Comparable results have been obtained in a study by Frost (2013) in which lower psychological well-being was associated with lower use of first-person plural pronouns. Even though acute stress is supposed to increase collective orientation and have benefits for well-being (Mehl and Pennebaker, 2003; Zimmermann et al., 2013), the experience of prolonged stress and depressive symptoms seems to have the opposite effect by narrowing our focus on the self. However, instead of an increase in single pronouns as in other studies (Rude et al., 2004), we observed a decrease in plural pronouns in pregnant women with lower psychological well-being. Possibly, and under certain circumstance, decreased psychological well-being in pregnant women is not reflected by a stronger focus on the single self (I, mine), but by decreased attention to a shared self (us, our). Pregnancy can evoke changes in women’s identity and the transition to motherhood expands women’s self (Laney et al., 2014, 2015). Therefore, women referring to themselves as a family instead of an individual could be interpreted as a sign of collective orientation, which may have beneficial, adaptive psychological consequences. Hence, women’s increased or decreased use of first-person plural pronouns might be more indicative of pregnant women’s psychological state than their choice of singular pronouns.
Our results suggest that word use is indeed associated with self-reported psychological symptoms in pregnancy. Nevertheless, we could also show that findings from previous studies cannot easily be generalized to pregnant women. They might differ in word choice from other participants because they experience changes in the representation of their self during pregnancy, which is reflected in changes in their word use. Therefore, future studies should investigate pregnant women’s word use and its associations with their psychological state in more depth, particularly with regard to the use of first-person singular and plural pronouns.
For the final research question, we explored the relationship between word use and birth outcome variables above and beyond that of self-reported prenatal stress and depressive symptoms and common control variables. Interestingly in this study, maternal self-reported psychological state was not related to any birth outcome measure in the first place. Therefore, this hypothesis could not be tested as originally planned. The lacking association, however, corresponds to studies reporting no significant associations between women’s psychological symptoms or psychiatric disorders and children’s birth outcome (Andersson et al., 2004; Bödecs et al., 2010). Still, several studies found evidence for the influence of self-reported depressive symptoms or prenatal anxiety on adverse birth outcome (Grote et al., 2010; Dunkel Schetter and Lobel, 2012). This divergence may be explained by socially desirable response behavior that biased the self-reported measures of women’s mental health. Alternatively, pregnant women might want to see themselves in a different way compared to their true feelings. Therefore, in self-reports, they might present an image of themselves that is consistent with their own, more positive self-image in order to protect their self. Relying on self-report measures bears the risk of under-identification and under-treatment of psychological problems in pregnancy due to feelings of guilt or shame pregnant women might experience (World Health Organization the United Nations Population Fund [WHO], 2008). Implicit measures allow for an additional, less biased perspective and insight into women’s psychological state during pregnancy. In the present study, this assumption is supported by several linguistic categories that were indeed found to be significant predictors of birth outcome. Negative emotion words predicted shorter gestational length, suggesting that a negative emotional state could have a negative influence on the course of pregnancy and on fetal development. Since this relationship could not be found for women’s self-reported psychological state, the analysis of word choice such as higher use of negative emotion words could be an effective screening tool for lower well-being in pregnancy. Experiencing frequent negative emotional states and excessive stress during pregnancy has been associated with a dysregulated maternal hypothalamic-pituitary-adrenal (HPA) axis and increased circulating cortisol levels in the maternal blood (La Marca-Ghaemmaghami and Ehlert, 2015). Cortisol can pass the placental barrier more easily under maternal chronic stress conditions and exert adverse effects on the development of the fetus (Ghaemmaghami et al., 2014; La Marca-Ghaemmaghami et al., 2015, 2017).
The findings with regard to the use of first-person plural pronouns and birth outcome are again somewhat contradictive. Our second research question revealed associations between lower psychological well-being and less use of first-person plural pronouns. Based on these results, we would have expected a positive influence of first-person plural pronouns (e.g., we) on birth outcome, as it seemed to reflect higher maternal well-being. However, more frequent use of first-person plural pronouns negatively predicted gestational length and neonatal birth weight. Since studies found an increase in plural pronouns after a stressful event, we could interpret pregnant women’s increased use of first-person plural pronouns to be an indicator of experienced stress in pregnancy that could not be detected with self-report measures. Possibly, higher usage of we-pronouns may reflect an increased experience of social support in response to an increased experience of prenatal stress. From this point of view, the negative association between plural pronouns and birth outcome is more coherent. It is noteworthy, though, that studies have shown first-person plural pronouns to have other meanings besides a shared sense of identity (Tausczik and Pennebaker, 2010). Further research is needed to clarify the mechanisms behind the use of plural pronouns during pregnancy and in general, particularly how they are affected by different forms of stress or the experience of social support and their relevance for well-being and health.
The amount of cognitive mechanism words was a predictor of higher birth size. This linguistic category is a marker of cognitive activity and the active construction of meaning (Graham et al., 2009; Pennebaker et al., 2015). It has been associated with better physical health (Pennebaker et al., 1997; Low et al., 2006). For example, caregivers who wrote about their partner’s suffering showed higher heart rate reactivity when their texts contained fewer words of cognitive processing (Monin et al., 2012). Studies on writing as a therapeutic technique showed that improvement in therapy was associated with patients using more cognitive words over the course of time (Pennebaker et al., 1997; Campbell and Pennebaker, 2003). In conclusion, thinking and processing the manifold events in pregnancy could be a form of emotion regulation and could predict healthier birth outcome through a stress-protective biological pathway. More frequent use of cognitive mechanism words has been associated with decreased anxiety and rumination in couples who described their experience of trying to conceive (Sweeny et al., 2015).
In order to ensure pregnant women’s well-being and a healthy development of their child, prenatal mental health care needs to be incorporated into traditional health care services during pregnancy (World Health Organization the United Nations Population Fund [WHO], 2008). However, psychological symptoms in pregnancy often remain unspoken due to feelings of guilt and shame resulting in biased information. Our results suggest that analyzing word choice, particularly regarding the use of sad words and words of certainty might serve as a helpful tool in screening for psychological symptoms in pregnancy and reduce the problems associated with social desirability and positive self-representation.
Limitations, Strengths, and Future Research
Several limitations of this study need to be discussed. Participants were asked to spend about 5 min writing their response to the open-ended question. However, text samples were provided online without controlling for whether the women stuck to this time frame. Consequently, most participants provided relatively short text samples. Many studies using the word count approach had participants write for a certain amount of time or space, such as writing for 20 min on an A4-paper (Lorenz and Meston, 2012; Kim et al., 2015). However, there have been studies using shorter text samples, which yielded reliable results (Holtgraves, 2011; Tumasjan et al., 2011). For the current study, reliability of analysis was enhanced by only including texts with a minimum of 40 words. Nevertheless, future studies might consider setting requirements such as a minimum amount of writing time or space. Furthermore, by assessing several text samples throughout pregnancy, researchers would be able to investigate changes in word choice during this emotional period in a woman’s life. Similarly, maternal psychological well-being was measured only once during pregnancy. In the present study, depressive symptoms and prenatal stress had no impact on birth outcome. However, research has shown variability in these measures depending on prenatal stage (Teixeira et al., 2009). Hence, several measurement time points during pregnancy could provide a more detailed picture of women’s mental well-being and its relation to linguistic variables and birth outcome.
Participating women were of different gestational ages at the first measurement time point, resulting in a large variability. However, this circumstance was purposely taken into account in order to explore whether maternal well-being and word use might differ depending on the time point of pregnancy. Indeed, maternal prenatal stress at T1 was negatively associated with gestational age, suggestive of decreased stress with advancing pregnancy – a finding which is in line with results from previous studies (e.g., Glynn et al., 2004; Lübke et al., 2017). And, more frequent use of first-person singular pronouns was associated with a less advanced pregnancy which may indicate changes in women’s representation of self with advancing pregnancy in such a way that their focus on themselves decreases with approaching birth.
Another limitation concerns the high drop-off rate observed at T2. Women dropping out of the study after T1 were earlier in their pregnancy at T1 and seemed to be experiencing more stress and depressive symptoms. These women may have been less motivated to respond to our questions at T2 and might have decided to discontinue their participation.
Also, we did obtain a relatively healthy birth sample. Most pregnancies were of average gestational length and most newborns were of normal birth weight and size. Only 7.9% (20) of the infants were born preterm and only 4.8% (12) had low birth weight below 2500 g. Therefore, there might not have been enough variability in the outcome variables for our analyses. However, even in the normal range, lower birth weight is a risk factor for the development of diseases in adulthood (Harris and Seckl, 2011). Also, the prevalence rates of preterm birth in European countries range between 5.3 and 11.4 per 100 life births (Lisonkova et al., 2012), and according to estimations by the United Nations Children’s Fund and World Health Organization (2004) 6.4% of all infants are affected by low birth weight (<2500 g).
The effect sizes in the present study were small and may limit the clinical importance of the results, such as the predictive value of word choice for birth outcome. However, the present effect sizes are comparable to other studies on word choice (Pennebaker and King, 1999; Newman et al., 2003, 2008; Yarkoni, 2010). Nevertheless, more research on this topic is needed to further confirm our results.
Despite these shortcomings, the present study is strengthened by its study design. A major advantage is the application of a multi-method approach to answer our research questions. By combining a cross-sectional and longitudinal study design, we were able to analyze relationships between word choice and variables in pregnancy as well as to determine the predictive value of word choice for birth outcome. Moreover, we combined different assessment methods including self-reported and objective data as well as implicit measures. This offered a unique perspective on women’s psychological state of mind. Our approach allowed us to investigate the independent contribution of word choice to birth outcome while controlling for self-reported maternal psychological state. The study is further strengthened by the inclusion of several control variables such as pregnancy complications.
Conclusion
It is essential for both research and clinical practice to be able to accurately assess pregnant women’s psychological well-being in order to identify those women at risk for prenatal stress overexposure. Explicit assessment methods are often limited by social desirability or self-presentation bias. The additional use of implicit measures such as word choice may increase measurement accuracy and ensure with greater reliability that pregnant women in distress receive psychological care rapidly. Research efforts have to be intensified in order to gain a better understanding of the psychological dimensions of women’s word use during pregnancy and assess the advantages of word choice analyses as an additional screening tool for impaired psychological well-being.
Availability of Data and Material
The datasets analyzed during the current study are not publicly available due to terms of consent to which the participants agreed, but are available from the corresponding author upon reasonable request.
Ethics Statement
The study was carried out in accordance with the regulations of the Ethics Committee of the Faculty of Arts and Sciences of the University of Zurich. All participants provided informed consent.
Author Contributions
UE and PLM-G designed the study and were involved in the interpretation of the data. PLM-G oversaw the recruitment process and the statistical analyses. FU and NW helped in the recruitment of the participants. JS-R prepared the LIWC text samples, was responsible for data analysis, and drafted the manuscript. All authors reviewed, revised, and provided approval of the final version of the manuscript.
Funding
This study was supported by the Sophie von Liechtenstein Foundation for Woman and Child and the Foundation Propter Homines (to UE).
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors would like to thank Stefan Hofmann, Jutta Joormann, Antonio Pascual-Leone, and Oliver Schultheiss who during a summer school encouraged the last author to include implicit measures in this study on the psychological well-being of pregnant women. The authors also wish to acknowledge the efforts of Jana Roos in her support in the recruitment process of the study. And last but not least, the authors wish to express their gratitude to the pregnant women who volunteered to participate in this study.
Abbreviations
APA, American Psychological Association; EPDS, Edinburgh Postnatal Depression Sale; LIWC, Linguistic Inquiry and Word Count; SPSS, Statistical Package for the Social Sciences.
Footnotes
- ^ In order to determine the best threshold for the present linguistic analyses, we contacted Professor James Pennebaker, co-developer of the LIWC analysis program which was applied in this study. According to Professor Pennebaker (personal communication, May 28, 2013), the threshold depends on the number of texts available. He suggested a 40-word threshold for a total number of 100 texts, a larger threshold if fewer texts had been available.
References
Adolfsson, A., Johansson, C., and Nilsson, E. (2012). Swedish women’s emotional experience of the first trimester in a new pregnancy after one or more miscarriages: a qualitative interview study. Adv. Sex. Med. 2, 38–45. doi: 10.4236/asm.2012.23007
Adolfsson, A., Larsson, P. G., Wijma, B., and Bertero, C. (2004). Guilt and emptiness: women’s experiences of miscarriage. Health Care Women Int. 25, 543–560. doi: 10.1080/07399330490444821
Alhusen, J. L. (2008). A literature update on maternal-fetal attachment. J. Obstet. Gynecol. Neonatal Nurs. 37, 315–328. doi: 10.1111/j.1552-6909.2008.00241.x
Andersson, L., Sundström-Poromaa, I., Wulff, M., Aström, M., and Bixo, M. (2004). Neonatal outcome following maternal antenatal depression and anxiety: a population-based study. Am. J. Epidomol. 159, 872–881. doi: 10.1093/aje/kwh122
Bat-Erdene, U., Metcalfe, A., McDonald, S. W., and Tough, S. C. (2013). Validation of Canadian mothers’ recall of events in labour and delivery with electronic health records. BMC Pregnancy Childbirth 13:S3. doi: 10.1186/1471-2393-13-S1-S3
Bergant, A. M., Nguyen, T., Heim, K., Ulmer, H., and Dapunt, O. (1998). German language version and validation of the Edinburgh postnatal depression scale. Dtsch. Med. Wochenschr. 123, 35–40. doi: 10.1055/s-2007-1023895
Bödecs, T., Horváth, B., Szilágyi, E., Gonda, X., Rihmer, Z., and Sándor, J. (2010). Effects of depression, anxiety, self-esteem, and health behavior on neonatal outcomes in a population-based Hungarian sample. Eur. J. Obstet. Gynecol. Reprod. Biol. 154, 45–50. doi: 10.1016/j.ejogrb.2010.08.021
Brandon, A. R., Trivedi, M. H., Hynan, L. S., Miltenberger, P. D., Labat, D. B., Rifkin, J. B., et al. (2008). Prenatal depression in women hospitalized for obstetric risk. J. Clin. Psychiatry 69, 635–643. doi: 10.4088/JCP.v69n0417
Brönnimann, R., Herlihy, J., Müller, J., and Ehlert, U. (2013). Do testimonies of traumatic events differ depending on the interviewer? Eur. J. Psychol. Appl. Leg. Context 5, 97–121. doi: 10.5167/uzh-109365
Byatt, N., Biebel, K., Friedman, L., Debordes-Jackson, G., Ziedonis, D., and Pbert, L. (2013). Patient’s views on depression care in obstetric settings: how do they compare to the views of perinatal health care professionals? Gen. Hosp. Psychiatry 35, 598–604. doi: 10.1016/j.genhosppsych.2013.07.011
Campbell, R. S., and Pennebaker, J. W. (2003). The secret life of pronouns: flexibility in writing style and physical health. Psychol. Sci. 14, 60–65. doi: 10.1111/1467-9280.01419
Chung, C., and Pennebaker, J. W. (2011). “The psychological functions of function words,” in Social Communication, ed. K. Fiedler (New York, NY: Psychology Press), 343–359.
Cohen, J. (1990). Things I have learned (so far). Am. Psychol. 45, 1304–1312. doi: 10.1037/0003-066X.45.12.1304
Cordova, M. J., Cunningham, L. C., Carlson, C. R., and Andrykowski, M. A. (2001). Social constraints, cognitive processing, and adjustment to breast cancer. J. Consult. Clin. Psychol. 69, 706–711. doi: 10.1037/0022-006X.69.4.706
Cox, J. L., Holden, J. M., and Sagovsky, R. (1987). Detection of postnatal depression. Development of the 10-item Edinburgh postnatal depression scale. Br. J. Psychiatry 150, 782–786. doi: 10.1192/bjp.150.6.782
Crosier, T., Butterworth, P., and Rodgers, B. (2007). Mental health problems among single and partnered mothers. The role of financial hardship and social support. Soc. Psychiatry Psychiatr. Epidemiol. 42, 6–13.
Delucchi, K. L., and Bostrom, A. (2004). Methods for analysis of skewed data distributions in psychiatric clinical studies: working with many zero values. Am. J. Psychiatry 171, 1159–1168. doi: 10.1176/appi.ajp.161.7.1159
Deshields, T. L., Tait, R. C., Gfeller, J. D., and Chibnall, J. T. (1995). Relationship between social desirability and self-report in chronic pain patients. Clin. J. Pain 11, 189–193. doi: 10.1097/00002508-199509000-00005
Dole, N., Savitz, D. A., Hertz-Picciotto, I., Siega-Riz, A. M., McMahon, M. J., and Buekens, P. (2003). Maternal stress and preterm birth. Am. J. Epidemiol. 157, 14–24. doi: 10.1093/aje/kwf176
Dunkel Schetter, C., and Glynn, L. M. (2011). “Stress in pregnancy: empirical evidence and theoretical issues to guide interdisciplinary research,” in The Handbook of Stress Science Biology, Psychology and Health, eds A. Baum and R. Contrada (New York, NY: Springer Publishing Company), 321–343.
Dunkel Schetter, C., and Lobel, M. (2012). “Pregnancy and birth outcomes: a multilevel analysis of prenatal maternal stress and birth weight,” in Handbook of Health Psychology, 2nd Edn, eds A. Baum, T. A. Revenson, and J. Singer (New York, NY: Taylor & Francis), 431–463.
Eichstaedt, J. C., Schwartz, H. A., Kern, M. L., Park, G., Labarthe, D. R., Merchant, R. M., et al. (2015). Psychological language on Twitter predicts county-level heart disease mortality. Psychol. Sci. 26, 159–169. doi: 10.1177/0956797614557867
Fall, A., Goulet, L., and Vézina, M. (2013). Comparative study of major depressive symptoms among pregnant women by employment status. Springerplus 2:201. doi: 10.1186/2193-1801-2-201
Field, A. (2013). Discovering Statistics using IBM SPSS Statistics, 4th Edn. London: SAGE Publications Ltd.
Fisher, R. J. (1993). Social desirability bias and the validity of indirect questioning. J. Consum. Res. 20, 303–315. doi: 10.1086/209351
Frost, D. M. (2013). The narrative construction of intimacy and affect in relationship stories: implications for relationship quality, stability, and mental health. J. Soc. Pers. Relatsh. 30, 247–269. doi: 10.1177/0265407512454463
Ghaemmaghami, P., Dainese, S. M., La Marca, R., Zimmermann, R., and Ehlert, U. (2014). The association between the acute psychobiological stress response in second trimester pregnant women, amniotic fluid glucocorticoids, and neonatal birth outcome. Dev. Psychobiol. 56, 734–747. doi: 10.1002/dev.21142
Glynn, L. M., Schetter, C. D., Wadhwa, P. D., and Sandman, C. A. (2004). Pregnancy affects appraisal of negative life events. J. Psychosom. Res. 56, 47–52.
Goedhart, G., Snijders, A. C., Hesselink, A. E., van Poppel, M. N., Bonsel, G. J., and Vrijkotte, T. G. M. (2010). Maternal depressive symptoms in relation to perinatal mortality and morbidity: results from a large multiethnic cohort study. Psychosom. Med. 72, 769–776. doi: 10.1097/PSY.0b013e3181ee4a62
Graham, J. E., Glaser, R., Loving, T. J., Malrakey, W. B., Stowell, J. R., and Kiecolt-Glaser, J. K. (2009). Cognitive word use during marital conflict and increases in proinflammatory cytokines. Health Psychol. 28, 621–630. doi: 10.1037/a0015208
Grant, K.-A., McMahon, C., and Austin, M.-P. (2008). Maternal anxiety during the transition to parenthood: a prospective study. J. Affect. Disord. 108, 101–111. doi: 10.1016/j.jad.2007.10.002
Grote, N. K., Bridge, J. A., Gavin, A. R., Melville, J. L., Iyengar, S., and Katon, W. J. (2010). A meta-analysis of depression during pregnancy and the risk of preterm birth, low birth weight, and intrauterine growth restriction. Arch. Gen. Psychiatry 67, 1012–1024. doi: 10.1001/archgenpsychiatry.2010.111
Harris, A., and Seckl, J. (2011). Glucocorticoids, prenatal stress and the programming of disease. Horm. Behav. 59, 279–289. doi: 10.1016/j.yhbeh.2010.06.007
Hatton, D. C., Harrison-Hohner, J., Matarazzo, J., Edwards, P., Lewy, A., and Davis, L. (2007). Missed antenatal depression among high risk women: a secondary analysis. Arch. Womens Ment. Health 10, 121–123. doi: 10.1007/s00737-007-0180-1
Heron, J., O’Connor, T. G., Evans, J., Golding, J., and Glover, V. (2004). The course of anxiety and depression through pregnancy and the postpartum in a community sample. J. Affect. Disord. 80, 65–73. doi: 10.1016/j.jad.2003.08.004
Hirsh, J. B., and Peterson, J. B. (2009). Personality and language use in self-narratives. J. Res. Pers. 43, 524–527. doi: 10.1016/j.jrp.2009.01.006
Hobbs, D. F., and Cole, S. P. (1976). Transition to parenthood: a decade replication. J. Marriage Fam. 38, 723–731. doi: 10.2307/350691
Holtgraves, T. (2011). Text messaging, personality, and the social context. J. Res. Pers. 45, 92–99. doi: 10.1016/j.jrp.2010.11.015
Horn, A. B., and Mehl, M. R. (2004). Expressives schreiben als copingtechnik: ein überblick über den stand der forschung. Verhaltenstherapie 14, 274–283. doi: 10.1159/000082837
Hussy, W., Schreier, M., and Echterhoff, G. (2010). Forschungsmethoden in Psychologie und Sozialwissenschaften - für Bachelor. Berlin: Springer.
Johnson, T., and Fendrich, M. (2005). Modeling sources of self-report bias in a survey of drug use epidemiology. Ann. Epidemiol. 15, 381–389. doi: 10.1016/j.annepidem.2004.09.004
Kelley, H. H., and Thibaut, J. W. (1978). Interpersonal Relations: A theory of Interdependence. New York, NY: Wiley.
Kim, K., Lee, S., and Lee, C. (2015). College students with ADHD traits and their language styles. J. Atten. Disord. 19, 687–693. doi: 10.1177/1087054713484512
King, M. F., and Bruner, G. C. (2000). Social desirability bias: a neglected aspect of validity testing. Psychol. Mark. 17, 79–103. doi: 10.1002/(SICI)1520-6793
Kingston, D. E., Biringer, A., Toosi, A., Heaman, M. I., Lasiuk, G. C., McDonald, S. W., et al. (2015). Disclosure during prenatal mental health screening. J. Affect. Disord. 186, 90–94. doi: 10.1016/j.jad.2015.07.003
Kramer, M. S., Lydon, J., Séguin, L., Goulet, L., Kahn, S. R., McNamara, H., et al. (2009). Stress pathways to spontaneous preterm birth: the role of stressors, psychological distress, and stress hormones. Am. J. Epidemiol. 169, 1319–1326. doi: 10.1093/aje/kwp061
La Marca-Ghaemmaghami, P., Dainese, S. M., La Marca, R., Zimmermann, R., and Ehlert, U. (2015). The acute autonomic stress response and amniotic fluid glucocorticoids in second-trimester pregnant women. Psychosom. Med. 77, 41–49. doi: 10.1097/PSY.0000000000000130
La Marca-Ghaemmaghami, P., Dainese, S. M., Stalla, G., Haller, M., Zimmermann, R., and Ehlert, U. (2017). Second-trimester amniotic fluid corticotropin-releasing hormone and urocortin in relation to maternal stress and fetal growth in human pregnancy. Stress 20, 231–240. doi: 10.1080/10253890.2017.1312336
La Marca-Ghaemmaghami, P., and Ehlert, U. (2015). Stress during pregnancy: experienced stress, stress hormones, and protective factors. Eur. Psychol. 20, 102–119. doi: 10.1027/1016-9040/a000195
Laney, E. K., Carruthers, L., Hall, M. E. L., and Anderson, T. (2014). Expanding the self: motherhood and identity development in faculty women. J. Fam. Issues 35, 1227–1251. doi: 10.1177/0192513X13479573
Laney, E. K., Hall, M. E. L., Anderson, T. L., and Willingham, M. M. (2015). Becoming a mother: the influence of motherhood on women’s identity development. Identity 15, 126–145. doi: 10.1080/15283488.2015.1023440
Lara, M. A., Navarrete, L., and Nieto, L. (2016). Prenatal predictors of postpartum depression and postpartum depressive symptoms in Mexican mothers: a longitudinal study. Arch. Womens Ment. Health 19, 825–834. doi: 10.1007/s00737-016-0623-7
Lara, M. A., Navarrete, L., Nieto, L., Martín, J. P. B., Navarro, J. L., and Lara-Tapia, H. (2015). Prevalence and incidence of perinatal depression and depressive symptoms among Mexican women. J. Affect. Disord. 175, 18–24. doi: 10.1016/j.jad.2014.12.035
Lee, A. M., Lam, S. K., Sze Mun Lau, S. M., Chong, C. S., Chui, H. W., and Fong, D. Y. (2007). Prevalence, course, and risk factors for antenatal anxiety and depression. Obstet. Gynecol. 110, 1102–1112. doi: 10.1001/archpsyc.65.7.805
Liehr, P., Mehl, M. R., Summers, L. C., and Pennebaker, J. W. (2004). Connecting with others in the midst of stressful upheaval on September 11, 2001. Appl. Nurs. Res. 17, 2–9. doi: 10.1016/j.apnr.2003.10.010
Lisonkova, S., Sabr, Y., Butler, B., and Joseph, K. S. (2012). International comparisons of preterm birth: higher rates of late preterm birth are associated with lower rates of stillbirth and neonatal death. BJOG 119, 1630–1639. doi: 10.1111/j.1471-0528.2012.03403.x
Lobel, M. (1994). Conceptualizations, measurement, and effects of prenatal maternal stress on birth outcomes. J. Behav. Med. 17, 225–272. doi: 10.1007/BF01857952desi
Lorenz, T. A., and Meston, C. M. (2012). Associations among childhood sexual abuse, language use, and adult sexual functioning and satisfaction. Child Abuse Negl. 36, 190–199. doi: 10.1016/j.chiabu.2011.09.014
Low, C. A., Stanton, A. L., and Danoff-Burg, S. (2006). Expressive disclosure and benefit finding among breast cancer patients: mechanisms for positive health effects. Health Psychol. 25, 181–189. doi: 10.1037/0278-6133.25.2.181
Lübke, K. T., Busch, A., Hoenen, M., Schaal, B., and Pause, B. M. (2017). Pregnancy reduces the perception of anxiety. Sci. Rep. 7:9213. doi: 10.1038/s41598-017-07985-0
MacWilliams, K., Hughes, J., Aston, M., Field, S., and Moffatt, F. W. (2016). Understanding the experience of miscarriage in the emergency department. J. Emerg. Nurs. 42, 504–512. doi: 10.1016/j.jen.2016.05.011
Mancuso, R. A., Schetter, C. D., Rini, C. M., Roesch, S. C., and Hobel, C. J. (2004). Maternal prenatal anxiety and corticotropin-releasing hormone associated with timing of delivery. Psychosom. Med. 66, 762–769. doi: 10.1097/01.psy.0000138284.70670.d5
Maxson, P., and Miranda, M. L. (2011). Pregnancy intention, demographic differences, and psychosocial health. J. Womens Health 20, 1215–1223. doi: 10.1089/jwh.2010.2379
McMahon, C. A., Boivin, J., Gibson, F. L., Hammarberg, K., Wynter, K., Saunders, D., et al. (2011). Age at first birth, mode of conception and psychological wellbeing in pregnancy: findings from the parental age and transition to parenthood Australia (PATPA) study. Hum. Reprod. 26, 1389–1398. doi: 10.1093/humrep/der076
Mehl, M. R., and Pennebaker, J. W. (2003). The sounds of social life: a psychometric analysis of students’ daily social environments and natural conversations. J. Pers. Soc. Psychol. 84, 857–870. doi: 10.1037/0022-3514.84.4.857
Melville, J. L., Gavin, A., Guo, Y., Fan, M.-Y., and Katon, W. J. (2010). Depressive disorders during pregnancy: prevalence and risk factors in a large urban sample. Obstet. Gynecol. 116, 1064–1070. doi: 10.1097/AOG.0b013e3181f60b0a
Miller, G. A. (1995). WordNet: a lexical database for English. Commun. ACM 38, 39–41. doi: 10.1145/219717.219748
Minor, K. S., Bonfils, K. A., Luther, L., Firmin, R. L., Kukla, M., MacLain, V. R., et al. (2015). Lexical analysis in schizophrenia: how emotion and social word use informs our understanding of clinical presentation. J. Psychiatr. Res. 64, 74–78. doi: 10.1016/j.jpsychires.2015.02.024
Monin, J. K., Schulz, R., Lemay, E. P. Jr., and Cook, T. B. (2012). Linguistic markers of emotion regulation and cardiovascular reactivity among older caregiving spouses. Psychol. Aging 27, 903–911. doi: 10.1037/a0027418
Nast, I., Bolten, M., Meinlschmidt, G., and Hellhammer, D. H. (2013). How to measure prenatal stress? A systematic review of psychometric instruments to assess psychosocial stress during pregnancy. Paediatr. Perinat. Epidemiol. 27, 313–322. doi: 10.1111/ppe.12051
Nelson, S. K., Robbins, M. L., Andrews, S. E., and Sweeny, K. (2015). Disrupted transition to parenthood: gender moderates the association between miscarriage and uncertainty about conception. Sex Roles 76, 380–392. doi: 10.1007/s11199-015-0564-z
Newman, M. L., Groom, C. J., Handelman, L. D., and Pennebaker, J. W. (2008). Gender differences in language use: an analysis of 14,000 text samples. Discourse Process. 45, 211–236. doi: 10.1080/01638530802073712
Newman, M. L., Pennebaker, J. W., Berry, D. S., and Richards, J. M. (2003). Lying words: predicting deception from linguistic styles. Pers. Soc. Psychol. Bull. 29, 665–675. doi: 10.1177/0146167203029005010
Orsillo, S. M., Batten, S. V., Plumb, J. C., Luterek, J. A., and Roessner, B. M. (2004). An experimental study of emotional responding in women with posttraumatic stress disorder related to interpersonal violence. J. Trauma Stress 17, 241–248. doi: 10.1023/B:JOTS.0000029267.61240.94
Pennebaker, J. W. (1989). “Confession, inhibition, and disease,” in Advances in Experimental Social Psychology, ed. L. Berkowitz (New York, NY: Academic Press. ), 211–244. doi: 10.1016/S0065-2601(08)60309-3
Pennebaker, J. W. (2011). Using computer analyses to identify language style and aggressive intent: the secret life of function words. Dyn. Asymmetric Confl. 4, 92–102. doi: 10.1080/17467586.2011.627932
Pennebaker, J. W., Booth, R. J., and Francis, M. E. (2007). Linguistic Inquiry and Word Count: LIWC [Computer Software]. Austin, TX: LIWC.net.
Pennebaker, J. W., Boyd, R. L., Jordan, K., and Blackburn, K. (2015). The Development and Psychometric Properties of LIWC2015. Austin, TX: University of Texas at Austin.
Pennebaker, J. W., and King, L. A. (1999). Linguistic styles: language use as an individual difference. J. Pers. Soc. Psychol. 77, 1296–1312. doi: 10.1037/0022-3514.77.6.1296
Pennebaker, J. W., Mayne, T. J., and Francis, M. E. (1997). Linguistic predictors of adaptive bereavement. J. Psychosom. Obstet. Gynecol. 72, 863–871. doi: 10.1037//0022-3514.72.4.863
Pennebaker, J. W., and Stone, L. D. (2003). Words of wisdom: language use over the life span. J. Pers. Soc. Psychol. 85, 291–301. doi: 10.1037/0022-3514.85.2.291
Pluess, M., Bolten, M., Pirke, K.-M., and Hellhammer, D. (2010). Maternal trait anxiety, emotional distress, and salivary cortisol in pregnancy. Biol. Psychol. 83, 169–175. doi: 10.1016/j.biopsycho.2009.12.005
Pressman, S. D., and Cohen, S. (2007). Use of social words in autobiographies and longevity. Psychosom. Med. 69, 262–269. doi: 10.1097/PSY.0b013e31803cb919
Pulverman, C. S., Lorenz, T. A., and Meston, C. M. (2015). Linguistic changes in expressive writing predict psychological outcomes in women with history of childhood sexual abuse and adult sexual dysfunction. Psychol. Trauma 7, 50–57. doi: 10.1037/a0036462
Ramirez-Esparza, N., Chung, C. K., Kacewicz, E., and Pennebaker, J. W. (2008). “The psychology of word use in depression forums in English and in Spanish: texting two text analytic approaches,” in Proceedings of the International Conference on Weblogs and Social Media, (Menlo Park, CA: AAI Press), 102–108.
Roesch, S. C., Schetter, C. D., Woo, G., and Hobel, C. J. (2004). Modeling the types and timing of stress in pregnancy. Anxiety Stress Coping 17, 87–102. doi: 10.1080/1061580031000123667
Rosenthal, R. (1991). Effect sizes: pearson’s correlation, its display via the BESD, and alternative indices. Am. Psychol. 46, 1086–1087.
Rouhe, H., Salmela-Aro, K., Halmesmaki, E., and Saisto, T. (2009). Fear of childbirth according to parity, gestational age, and obstetric history. Int. J. Obstet. Gynaecol. 116, 67–73. doi: 10.1111/j.1471-0528.2008.02002.x
Rubertsson, C., Hellström, J., Cross, M., and Sydsjö, G. (2014). Anxiety in early pregnancy: prevalence and contributing factors. Arch. Womens Ment. Health 17, 221–228. doi: 10.1007/s00737-013-0409-0
Rude, S., Gortner, E.-M., and Pennebaker, J. (2004). Language use of depressed and depression-vulnerable college students. Cogn. Emot. 18, 1121–1133. doi: 10.1080/02699930441000030
Santelli, J., Rochat, R., Hatfield-Timajchy, K., Gilbert, B. C., Curtis, K., Cabral, R., et al. (2003). The measurement and meaning of unintended pregnancy. Perspect. Sex. Reprod. Health 35, 94–101.
Schultheiss, O. C. (2013). Are implicit motives revealed in mere words? Testing the marker-word hypothesis with computer-based text analysis. Front. Psychol. 4:748. doi: 10.3389/fpsyg.2013.00748
Skouteris, H., Wertheim, E. H., Rallis, S., Milgrom, J., and Paxton, S. J. (2009). Depression and anxiety through pregnancy and the early postpartum: an examination of prospective relationships. J. Affect. Disord. 113, 303–308. doi: 10.1016/j.jad.2008.06.002
Slatcher, R. B. (2009). “Language usage in relationships,” in Encyclopedia of Human Relationships, eds H. T. Reis and S. Sprecher (Thousand Oaks, CA: Sage), 959–962.
Stirman, S. W., and Pennebaker, J. W. (2001). Word use in the poetry of suicidal and nonsuicidal poets. Psychosom. Med. 63, 517–522. doi: 10.1097/00006842-200107000-00001
Stone, L. D., and Pennebaker, J. W. (2002). Trauma in real time: talking and avoiding online conversations about the death of Princess Diana. Basic Appl. Soc. Psychol. 24, 172–182. doi: 10.1207/153248302760179101
Sweeny, K., Andrews, S. E., Nelson, S. K., and Robbins, M. L. (2015). Waiting for a baby: navigating uncertainty in recollections of trying to conceive. Soc. Sci. Med. 141, 123–132. doi: 10.1016/j.socscimed.2015.07.031
Tausczik, Y. R., and Pennebaker, J. W. (2010). The psychological meaning of words: LIWC and computerized text analysis methods. J. Lang. Soc. Psychol. 29, 24–54. doi: 10.1177/0261927X09351676
Taylor, A. W., Grande, E. D., Gill, T. K., Chittleborough, C. R., Wilson, D. H., Adams, R. J., et al. (2006). How valid are self-reported height and weight? A comparison between CATI self-report and clinic measurements using a large cohort study. Aust. N. Z. J. Public Health 30, 238–246. doi: 10.1111/j.1467-842X.2006.tb00864.x
Teixeira, C., Figueiredo, B., Conde, A., Pacheco, A., and Costa, R. (2009). Anxiety and depression during pregnancy in women and men. J. Affect. Disord. 119, 142–148. doi: 10.1016/j.jad.2009.03.005
Troude, P., L’Hélias, L. F., Raison-Boulley, A. M., Castel, C., Pichon, C., Bouyer, J., et al. (2008). Perinatal factors reported by mothers: do they agree with medical records? Eur. J. Epidemiol. 23, 557–564. doi: 10.1007/s10654-008-9268-9
Tsartsara, E., and Johnson, M. P. (2006). The impact of miscarriage on women’s pregnancy-specific anxiety and feelings of prenatal maternal-fetal attachment during the course of a subsequent pregnancy: an exploratory follow-up study. J. Psychosom. Obstet. Gynecol. 27, 173–182. doi: 10.1080/0167482060064619
Tumasjan, A., Sprenger, T. O., Sandner, P. G., and Welpe, I. M. (2011). Election forecasts with twitter: how 140 characters reflect the political landscape. Soc. Sci. Comput. Rev. 29, 402–418. doi: 10.1177/0894439310386557
United Nations Children’s Fund and World Health Organization (2004). Low Birthweight: Country, Regional and Global Estimates. New York, NY: UNICEF.
Vesga-López, O., Blanco, C., Keyes, K., Olfson, M., Grant, B. F., and Hasin, D. S. (2008). Psychiatric disorders in pregnant and postpartum women in the United States. Arch. Gen. Psychiatry 65, 805–815. doi: 10.1001/archpsyc.65.7.805
Wellings, K., Jones, K. G., Mercer, C. H., Tanton, C., Clifton, S., Datta, J., et al. (2013). The prevalence of unplanned pregnancy and associated factors in Britain: findings from the third National Survey of Sexual Attitudes and Lifestyles (Natsal-3). Lancet 382, 1807–1816. doi: 10.1016/S0140-6736(13)62071-1
Wolf, M., Horn, A. B., Mehl, M. R., Haug, S., Pennebaker, J. W., and Kordy, H. (2008). Computergestützte quantitative Textanalyse. Diagnostica 54, 85–98. doi: 10.1026/0012-1924.54.2.85
Wong, M. K., Crawford, T. J., Gask, L., and Grinyer, A. (2003). A qualitative investigation into women’s experiences after a miscarriage: implications for the primary healthcare team. Br. J. Gen. Pract. 53, 698–702.
Woods, S. M., Melville, J. L., Guo, Y., Fan, M.-Y., and Gavin, A. (2010). Psychosocial stress during pregnancy. Am. J. Obstet. Gynecol. 202, 61.e1–61.e7. doi: 10.1016/j.ajog.2009.07.041
World Health Organization the United Nations Population Fund [WHO] (2008). Maternal Mental Health and Child Health and Development in Low and Middle Income Countries (Report of the WHO-UNFPA Meeting, Geneva, Switzerland). Available at: http://www.who.int/mental_health/prevention/suicide/mmh_jan08_meeting_report.pdf
Yali, A. M., and Lobel, M. (1999). Coping and distress in pregnancy: an investigation of medically high risk women. J. Psychosom. Obstet. Gynecol. 20, 39–52. doi: 10.3109/01674829909075575
Yarkoni, T. (2010). Personality in 100,000 Words: a large-scale analysis of personality and word use among bloggers. J. Res. Pers. 44, 363–373. doi: 10.1016/j.jrp.2010.04.001
Keywords: pregnancy, prenatal stress, psychological well-being, birth outcome, word choice, LIWC
Citation: Schoch-Ruppen J, Ehlert U, Uggowitzer F, Weymerskirch N and La Marca-Ghaemmaghami P (2018) Women’s Word Use in Pregnancy: Associations With Maternal Characteristics, Prenatal Stress, and Neonatal Birth Outcome. Front. Psychol. 9:1234. doi: 10.3389/fpsyg.2018.01234
Received: 01 March 2018; Accepted: 27 June 2018;
Published: 24 July 2018.
Edited by:
Nuno Barbosa Rocha, Politécnico do Porto, PortugalReviewed by:
Irene Messina, Università degli Studi di Padova, ItalyMaría I. Cordero, Manchester Metropolitan University, United Kingdom
Jean Marc Guile, University of Picardie Jules Verne, France
Copyright © 2018 Schoch-Ruppen, Ehlert, Uggowitzer, Weymerskirch and La Marca-Ghaemmaghami. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pearl La Marca-Ghaemmaghami, pearl.lamarca@psychologie.uzh.ch